Embed Size (px)
Citation preview

STUDIES ON POST-ATABRINE DERMATITIS
II. PERMANENT ANHIDRosIs, ANHIDROTIC ASTHENIA AND PROLONGEDDERMATITIS FOLLOWING ATABRINE DERMATITIS *
IRA LEO SCIIAMBERG, M.D.
In a previous study (1), we observed the course of chronic or recurrent, oftenbizarre dermatitis in a group of veterans of World War II who had suffered,while overseas, from a generalized dermatitis designated at the time as atypicallichen planus. Andrews (la) in 1938, and Becker and Obermayer (ib) in 1940,listed atabrine as a cause of exfoliative dermatitis. Numerous other authors(2—14) have since incriminated atabrine as the cause of so-called atypical lichenplanus. In all of the patients in our first study, and in some of those presentedin this second study, the acute process had tapered off over a period of monthsto a chronic or remittent eczematous, lichenoid or weeping pruritic dermatitis.There has been no name for this chronic disease—it mimics many dermatoses.It appears clear to us that it follows and results from the acute atabrine derma-titis incurred overseas, and in our first paper we therefore labelled it chronicatabrine dermatitis. This term has caused confusion, in that it appears to implythat the chronic dermatitis is the result of either continued atabrine ingestionor continued action of atabrine in the patient's tissues. On the suggestion ofDr. Walter Shelley, we therefore submit the name "Post-Atabrine Dermatitis",as expressing more clearly our concept of this disease.
ETIOLOGY OF POST-ATABRINE DERMATITIS
Miller, Herrmann and Rubin (12) and Herrmann and Miller (13, 14) demon-strated intense blue white fluorescence in sweat ducts in a patient who presenteda sweat retention syndrome six years after the onset of lichenoid atabrinedermatitis. They suggest that traces of atabrine were still retained by the liningof the terminal portions of the ducts as long as six years after the last ingestionof atabrine. In patients given the drug experimentally by these workers, how-ever, fluorescence of the skin, nails and sweat ducts persisted no longer than 14weeks. Whether or not further study corroborates the persistence of atabrinein the tissues for years, it appears clear to us, from the clinical standpoint,that some permanent change occurs in the skin of some patients who sufferedfrom atabrine dermatitis, which causes a dermatitis to persist for years in achronic or remittent form. Permanent sweat retention anhidrosis due to occlu-sion of the sweat ducts has been found following atabrine dermatitis (15, 16,17). Sulzberger and his group (16, 17) have suggested that occlusion of the sweatducts, in the presence of functioning sweat glands, results in multiple and
* From the Veterans Administration Regional Office, Philadelphia, and the Departmentof Dermatology, (Donald M. Pillsbury, M.D., Director), University of PennsylvaniaSchool of Medicine, Phila.
Received for publication April 6, 1953.279

280 THE JOURNAL OF iNVESTIGATIVE DERMATOLOGY
repetitious injections of sweat into the subcutaneous tissues as a result of pene-tration through the walls of the occluded ducts. Allergens or irritants in thesweat may, they suggest further, cause pathologic changes in the tissues. It ispossible that this, plus other as yet undiscovered metabolic or structural changesin the skin, may be responsible for persistence of the dermatitis. It is worthyof note that the course of some of our patients years after the onset has beensimilar to that described in the earlier phases of the dermatitis by Livingoodand Dieuaide (2): "a considerable number of these patients have acute 'explo-sive' generalized exacerbations manifested by oozing eczematoid dermatitishaving a predilection for the fiexors, groins, axillae, extremities and neck."This we feel, identifies "post-atabrine dermatitis" even more closely with theparent disease.
CLINICAL DIAGNOSIS OF POST-ATABRINE DERMATITIS
In our first paper (1) we reported the course of post-atabrine dermatitis in agroup of veterans who presented permanent atrophic residua of the skin, hairfollicles or sweat ducts. Parenthetically, it is of interest that Sulzberger andBaer (4, 11) foresaw at an early date the possibility of permanent skin changesresulting from atabrine dermatitis. In 1945, they stated "Atrophic and poikilo-derma-like changes may be largely irreversible. There may be long-lasting orperhaps permanent atrophic changes". In 1947, they stated "Residua of ata-brine dermatitis include apparently permanent scarring, alopecias and atrophy,including that of the sweat gland orifices with consequent anhidrosis and result-ing profound systemic disturbances due to faulty dissipation of heat". Thegroup reported was selected because the presence of these atrophic residuaseemed to establish the initial diagnosis of atabrine dermatitis without question.However, it was pointed out that these patients were a highly selected group,and their course and prognosis were not representative of the fate of the hundredsof men who acquired this dermatitis during World War II. In this second paperthirteen additional veterans are presented who had atabrine dermatitis of lesssevere degree, in that only four of them now show mild atrophic residua, andonly nine of them are now suffering from post-atabrine dermatitis. Results ofatabrine patch tests in eight veterans are reported, and there is further observa-tion of two of the patients presented in our first paper.
Numerous difficulties were encountered in assembling this additional group.Through the courtesy of Dr. Eugene L. Hamilton, Chief of the Medical StatisticsDivision, Office of the Surgeon General, Department of the Army, a list of 144veterans from the Philadelphia area who had been diagnosed "lichen planus"or "reaction to malaria prophylaxis" in the Army during 1944—45 was madeavailable to us. We were able to obtain Veterans Administration claims foldersfor only 23 veterans on this list, and in only ten of these were medical recordssufficiently detailed to permit critical evaluation of the diagnosis. Of these tenonly six were available for current observation. The remaining seven patientswere encountered in the routine operation of the Veterans AdministrationRegional Office Dermatology Clinic. Thus, this group cannot be considered to

STUDIES ON POST-ATABRINE DERMATITIS 281
be a random sample of veterans who had atabrine dermatitis. Even the veteranson the list supplied by the Surgeon General's office who responded to our requestthat they be examined may well have been influenced to come in because ofpersistent dermatitis.
From the often excellent and detailed clinical descriptions of the early stagesof the disease available to us, many of these veterans appeared to combineeczematous and lichenoid features, and none presented clear-cut exfoliativedermatitis. The course of many of them was apparently similar to that describedand photographed in Goldberg's study (18). Livingood and Dieuaide (2), andSchmitt (19) have stated that the eczematous type was much more commonthan the lichenoid, and Nisbet (10) classified frequency as 80% eczematous,12% lichenoid and 8 % exfoliative. In discussion of Nisbet's paper, Novy em-phasized that it is almost impossible to diagnose (as due to atabrine) the eczema-tous type. Schmitt (19) quotes Livingood as stating "hundreds of persons nowhave various types of chronic eczematous eruptions only because they hadquinacrine dermatitis during the war". One gains the impression from Schmitt'scase reports that eczematous dermatitis of the hands and feet first appearingin the Pacific Theatre is accepted by him as ipso facto evidence for the diagnosisof atabrine dermatitis. We are unable to accept this concept. Identical lesionsare seen in many patients who have never taken atabrine and have never beenin the tropics, whereas the clinical picture of widespread lichenoid and eczema-tous dermatitis (so-called atypical lichen planus) is seeii only in patients whohave taken atabrine. Even if it were shown that the incidence of eczematousdermatitis of the hands and feet was significantly higher in troops in the Pacificthan in troops and civilians in this country, the factors of heat, humidity,fungous and pyogenic infections, poor skin hygiene and emotional stress mightwell be responsible for this difference. Dr. Harvey Blank, who saw many casesof atabrine dermatitis in the Pacific area, states that the older age groups weremore often affected and that alopecia, violaceous plaques, mucous membranelesions, and localization of lesions on the upper eyelids and at the canthi of theeyes were cardinal diagnostic features (20). We are grateful to Dr. Blank for hisassistance in the selection of our cases.
Retrospective diagnosis of atabrine dermatitis in the absence of atrophicresidua, even when medical records of the acute stage of the disease are available,is often difficult. In all of the cases presented here lichen planus or atypicallichen planus was diagnosed by one or more military physicians during the earlystage. It must be recognized, however, that after this entity became known inthe Pacific area, there was a tendency to use this diagnosis rather indiscrimi-nately, even as the designation "fungous infection" had previously coveredalmost the entire range of dermatologic diseases. A number of cases diagnosedatypical lichen planus in the service were not included in this study because wedid not feel satisfied with the accuracy of the initial diagnosis.
In Table I, the essential findings in this group of 13 veterans is presented.Twelve of these men were in the Southwest Pacific, one in the China-Burma-India Theatre. The nine patients in this group without atrophic residua were

TA
BL
E I
' D
UR
AT
ION
O
F A
TA
BE
INE
INC
ES-
Si
T
ION
(M
ON
TH
S)
Hi,
— h'
'I
l-i
<
ii H
N
H 5 H
SIT
ES
OF
DE
RM
AT
ITIS
IN
C
HR
ON
OL
OO
IC
OR
DE
R C
linic
al d
ata i
n ce
tera
ns w
ho h
ad h
ad a
tabr
ine
derm
atiti
s
INT
ER
VA
L
FRO
M O
NSE
T
TO
LA
ST E
XA
M.
____
____
____
HIS
TO
RY
OF
__
____
__
ALO
FE
CIA
D
UR
INO
A
CU
TE
ST
AG
E
Yea
rs M
onth
s Sy
mpt
oms
FIN
DIN
GS O
N L
AST
EX
AM
INA
TIO
N
J.S.
C
34
27
12
MT
. W
34
20
7
B.T
. W
25
10
4
JO.
W
20
14
9
N.M
. W
21
14
13
T.F
. W
39
4
15
13 3 2 5 4 3 7 3 93
d
Bac
k, h
ands
, tar
e an
d le
gs
Feet
, leg
s, h
ands
and
arm
s
Fing
ers,
gro
in, e
ars,
too
t an
d m
outh
Nav
el,
groi
n,
eyel
ids,
hs
nds,
thi
ghs,
trun
k an
d m
outh
G
roin
, ey
elid
s, e
ars,
srm
s an
d tr
unk
Dor
sa ha
nds,
trun
k, p
enis
an
d to
ngue
Gro
ins,
ey
elid
s,
arm
s,
hand
s, e
srs
and
mou
th
Feet
, ch
est,
groi
n, e
yes,
sc
alp,
hac
k an
d ha
nds
Dor
sa h
sndl
, ar
ms,
ear
s,
neck
, tr
unk
and
legs
H
ands
, fo
rear
ms,
ea
rs,
legs
, sau
l50
and
hutto
cks
Dor
sa ha
nds,
legs
, eye
lids,
pe
nis,
arm
s L
egs,
fs
ce,
axill
ae,
neck
an
d m
outh
Fi
nger
s,
abdo
men
, fo
re-
arm
s and
legs
L
Itchi
ng fa
ce,
0 ba
ck,
ears
, le
gs
and
groi
n 0
0
Han
ds
hlis
- 0
ter
and
itch
in su
mm
er
Itch
ing
axi1
- 0
lao
and
groi
n
Itch
ing
scro
- 0
toni
sn
d pe
nis
Itch
ing
+
trun
k lo
gs
and
feet
0
+
0 0
Itch
ing
0 tr
unk
Itch
ing g
roin
0
and
feet
Itch
ing
0
hand
s It
chin
g ne
ck
+
I It
chin
g fe
et,
0
groi
n,
hand
s an
d sc
alp
Scal
p hai
r th
inne
d
Scal
p 0
Scal
p 0 0
Scal
p hai
r th
inne
d A
rms a
nd
hsnd
s A
xilla
ry
and
pubi
c ha
ir
Scal
p an
d ax
illac
0 0
7 7 7 6 6 6 6 6 6 6 4
5,
'H
C, 0
a,.,
'H 5 0 0 0
Dor
sa
fing
ers
0
Han
ds,
fore
- ar
ms 0 0 0 0 0 0 0
3 0 0 0 11
10
10 9 7 9 4 3
7 13
26
15
11
Alo
peri
a
0 0 0 0 0 0 0 0 0
Slig
ht
axill
ae
0 0
Slig
ht
in sc
alp
A.
B.
A,
R.
P. B
.
Y.
F.
H. W
.
F. W
.
H.
M.
W
36
W
28
W
26
W
19
W
42
C
26
C
27
Act
ive L
esio
ns
Scal
ing
and
exco
riat
ions
sc
alp,
eye
brow
s and
ear
s.
Hyp
erpi
gmcn
tstio
n an
d lic
heni
fica
tion
back
T
ines
ve
rsic
olor
th
ighs
, tin
es p
edis
Scal
ing
dors
a fi
nger
s and
ha
nds,
tine
a co
rpor
is
Hyp
erid
rotic
mac
orat
ion
betw
een t
oes
and
in p
en-
anal
regi
on
Lic
heni
fica
tion
peni
s,
scal
p; s
caly
pa
tche
s on
sc
rotu
m
Mac
orat
ion
anus
0 0
Arc
uste
lic
heno
id
pla-
qu
es o
n ch
est
Lic
heno
id p
apul
es p
alln
s;
eryt
hem
a an
d lic
heni
fica
- tio
n gr
oin
Lic
hcni
fica
tion
and
red
scal
ing
of f
inge
rs
Lic
heni
fica
tion
neck
Lic
heni
fica
tion
axill
sc
6 8 22 4 8 3 142
RE
MA
RK
S
Wor
se in
sum
mer
Cle
ar
sinc
e 2
year
s af
ter
onse
t, cu
rren
t fu
ngus
lesi
ons
of r
e-
cent
ons
et
Wor
se in
sum
mer
Wor
se in
sum
mer
Wor
se in
sum
mer
Wor
se in
slI
mm
er
Cle
ar s
ince
1
year
af
ter o
nset
C
lear
sin
ce 2
ye
ars
afte
r ons
et
Cle
ar i
n w
inte
r,
re-
curr
ent i
n su
mm
er
Wor
se in
sum
mer
No
seas
onal
di
ffer
- en
ce
No
seas
onal
di
ffer
- en
ce
Wor
se in
sum
mer

STUDIES ON POST-ATABRINE DERMATITIS 283
compared with thirteen patients with atrophic residua (nine in our previouspaper, four in the current study), with respect to age at onset, race, duration ofatabrine ingestion, and duration of observation. Table II shows no significantdifference between the two groups. Also, no difference was found in respect tosite of onset, chief site of current cutaneous involvement, and sites of activelesions at the onset and at the latest examination. Therefore, Table III presentsonly the composite findings for the combined groups. It may be noted that thedermatitis began on the hands in over one-third of the cases, and that oralmucous membrane lesions were noted in only one-half of the cases during theacute stage, and in only one-seventh at last examination. The last column ofTable I reveals that of the ten patients with post-atabrine dermatitis, two notedno seasonal difference, seven had summer exacerbations and one patient experi-
TABLE IITwenty-two veterans with atabrine dermatitis
VRTERANS WITH
ATROPHIC TOTALS
RESIDUA
White 8 7 15
Colored 5 2 7
Total 13 9 22
Age at onset (mean), years 29.0 30.2 29.5Duration of atabrine ingestion (mean), months
Before onset of dermatitis 5.1 9.2 6.8After onset of dermatitis 5.2 6.2 5.6
Total 10.3 15.4 12.4
Duration of observation (mean), years 5.7 6.9 6.2
enced recurrence each summer. Perhaps the greater demands made on struc-turally or functionally damaged sweat apparatus by warm weather may explainthe baleful effect of heat in eight of the ten patients in this group.
Whether or not these veterans had persistent dermatitis consequent upontheir atabrine dermatitis was not an easy decision to make in all cases. Patients2 and 4 were considered to show no evidence of post-atabrine dermatitis. How-ever, the tinea versicolor on the thighs in patient 2 and the hyperhidrotic macera-tion of the perianal area and feet in patient 4, both of which began after militaryservice, may be the result of cutaneous changes initiated by atabrine dermatitis.Conversely, the banal dermatitis of the hands in patient 3 and the anal macera-tion in patient 6 may not be causally related to the preexisting dermatitis. Inthe remainder of the cases we feel we are on firm ground in considering the lesionsas those of post atabrine dermatitis. The lesions of patient 9 are illustrated inFigure 1.

284 THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
TABLE IIISites of active lesions in 22 veterans with atabrine dermatitis
DURING ACUTE STAGE AT LAST EXAMINATION
SITES OF LESIONSSite of Sites of Site of major Sites ofonset lesions involvement lesions
Hands 8 16 4 6Trunk 2 16 1 4Legs 2 16 3 4Arms 1 14 1 4Oral mucous membrane 0 11 1 3Neck 0 8 3 3
Face (excluding periorbital area) 1 8 0 2Groin 3 8 0 2Ears 0 8 0 1
Periorbital area 1 8 0 0Axillae 0 5 1 2Feet 3 4 1 3Penis 0 4 1 2
Scalp 0 4 1 1
Buttocks 0 3 0 0Anus 0 1 1 3Scrotum 0 1 0 1
None 0 0 4 4
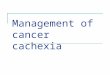
Fto. 1. Case 9. Six and three-quarters years after onset. Annular sharply outlined flatshiny lichenoid plaques, recurrent each summer. (Patient of Dr. Thomas Butterworth,through whose kindness this photograph was made available to us).
S

STUDIES ON POST-ATABRINE DERMATITIS 285
A number of these veterans had been examined and treated in the past fewyears by competent dermatologists. None had made the diagnosis of chronicpost-atabrine dermatitis. Their diagnoses included erytbema multiforme, solardermatitis, urticaria, eczematoid dermatitis, seborrheic dermatitis, neuroder-matitis, allergic dermatitis, contact dermatitis and lichen planus.
PATCH TESTS W1TH ATABRINE
Atabrine patch tests were applied to normal skin of eight patients, six ofwhom had had atabrine dermatitis, and five of whom had, at the time of testing,lesions of post-atabrine dermatitis. The intact or powdered atabrine tablet wasapplied to the normal skin of the shoulder, and left in place under a fixed dressingfor 72 hours or more. In six patients the reaction was negative, in two it waspositive. One of these was T. 0., case 3 in our first study (1), whose subsequentcourse is detailed in this paper. The other positive reaction occurred in J. S.,
FIG. 2. Case 1. Reaction to atabrioe patch test seven years and four months after onsetof dermatitis. Four plus reaction with ulceration.
patient 1 in Table I, who developed a 4 plus reaction with ulceration (Fig. 2).Figure 3 depicts this patient's eczematous lesions of post-atabrine dermatitisat the time of testing.
Livingood and Dieuaide (2) stated that it is in the eczematous type of ata-brine dermatitis that the patch test tends to be positive. Sulzberger and Baer(4) concurred that in patients with eczematous dermatitis or with exfoliativeerythroderma the patch test is often positive, but that in other clinical types itis usually negative. Bazemore (5), found no significant difference in incidenceof positive tests between patients and controls. Of seven atabrine dermatitispatients tested on normal skin by Wilson (6), one, who presented a generalizeddry patchy follicular eruption, showed at the site of the atabrine patch test"a few maculo-papular lesions". The six other patients and four controls allhad negative patch tests. Application of 1:100 atabrine ointment every threehours for three days to an area of dermatitis resulted in an acute vesicular reac-tion in three patients with universal subacute atabrine dermatitis. In other

286 THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
patients, simultaneous patch tests were positive on areas of present or pastdermatitis, and negative on normal skin. "Only that skin on which there hadpreviously been an eruption was reactive," Wilson concluded. Agress (7) foundthe atabrine patch test to be positive in 2 of 3 patients with atabrine psychosis,negative in 97 other atabrine treated malaria patients without psychosis ordermatitis. In three patients with atabrine dermatitis, and in one of twelve
FIG. 3. Case 1. Seven years and four months after onset. Red scaling and crusting ineyebrows and on cheeks and chin.
patients with other types of dermatitis, the patch test was positive. He con-cluded that the atabrine patch test showed 3 % false positive reactions in pa-tients with normal skin and 8.3 % in patients with dermatitis not caused byatabrine. Peterkin and Hair (8a) stated that skin tests to atabrine (patch,scratch and intracutaneous) were negative in their series of patients.
CASE REPORTS
Cases 1 and 3 in our first paper (1) have developed acute exacerbations since the time ofpublication. Case 1, F. C., whose dermatitis began in July 1943, developed weeping, crusted

STUDIES ON POST-ATABEINE DERMATITIS 287
lesions on the abdomen in May 1951. It was during this acute flare that a 72 hour ntabrincpatch test was negative. In July, a widespread pruritic vesicular and weeping dermntitisappeared. Skin culture revealed stnphylococcus aureus, slightly sensitive to chloromycetinand streptomycin and resistant to other antibiotics. Chioromycetin by mouth caused onlytemporary improvement, and the patient was hospitalized in September 1951, at whichtime generalized elevated crythematous vesicular weeping excoriated plaques were de-scribed. Cortisone therapy caused prompt and dramatic improvement. Laboratory studies
Fiu. 4. T. 0. Eight years and one month after onset. Weeping and purulent lichenoiddermatitis in poplitcal fossa.
were within normal limits.* Following discharge from the hospital, cortisone was continuedfor two months, in a dosage of 75 to 150 milligrams per day. During this period, multiplegrouped weeping papulovesicles appeared in the lichenoid areas. While the patient wasreceiving cortisone, 87.5 milligrams per day, administration of a triple sulfonamide prepa-ration, 3 grams per day (prescribed because of the nummular character of the eruption)resulted within 24 hours in massive red edema of the face and mottled crythema on thechest. Sulfonamide was stopped after 48 hours; cortisone dosage was increased to 150 milli-
* We are grateful to Dr. Philip M. Gottlieb, who cared for the patient in the hospital,for permission to report his findings.

288 THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
grams per day, and the reaction disappeared within a week. In April, 1952, within hoursafter subcutaneous injection of procaine for a biopsy, erythema and edema of the face andneck again developed, and subsided within several days. Monocaine had been used previ-ously for dental extractions without reaction. In November, 1952, after ingestion of only10 grams of potassium paraaminobenzoic acid, an acnte eczematous reaction, of ten daysduration, sharply demarcated at the collar line, appeared on the face. In July, 1953, tenyears after the onset, the dermatitis is quite well controlled by local applications of hydro-cortisone ointment, but flares when treatment is discontinued. (Patient under treatmentby Dr. Walter Shelley).
Sweating studies in the heat cabinet, performed by Dr. Shelley, revealed completeanhidrosis below the mid chest, with compensatory hyperhidrosis of the face, neckand shoulders. Symptoms of heat intolerance (quickened heart rate, flushing of face andand neck, fatigue and anxiety) were elicited on mild elevation of environmental tempera-
Fin. 5. T. 0. Eight years and one month after onset. Lichenoid, scaling, weeping andcrusted plaques.
turc. Inunction of lanolin did not promote the appearance of sweat on the skin, as it doesin anhidrosis due to keratinous plugging of the distal portion of the sweat duct. In order todetermine whether or not the sweat glands in the anhidrotic areas were functional (21),biopsies were taken from an anhidrotic plaque on the back before and immediately aftera 45 minute period in the heating cabinet. The specimens were stained for glycogen with theMcManus stain. Glycogcn was present in normal abundance in the acinar tissue of the sweatglands in the specimen taken prior to ssvcating, but was almost completely absent in thepost-sweating sections. Hcmatoxylin and eosin stained sections showed no well-definedsweat ducts. On the basis of these studies, Dr. Shelley concluded that normally functioningcccrinc sweat coils were present, but that the sweat was excreted into the corium since ithad no means of egress to the surface. The anhidrosis is irreversible, since it is caused bydestruction of the sweat ducts.
T. 0., case 3 in our first paper (1), whose dermatitis began in April, 1944, developed asycosiform pustular process at the nape of the neck in June, 1950. In December, 1951, pop-litcal pustulation and crusting occurred. In January, 1952, a widespread papular pruriticdermatitis, marked edema of the face, cars, penis and scrotum, and weeping dermatitis onthe legs appeared. He was hospitalized for a month. Histologic examination showed only anon-specific chronic dermatitis, and other laboratory studies were normal except for a 5%

4 S
.$ The1
'-'ii
F
STUDIES ON POST-ATABEINE DEEMATITIS 289
eosinophilia. On bland local therapy and vitamin A by mouth there was rapid improvementand on discharge from the hospital, the patient showed only a diffuse dry keratotic folli-cular dermatitis.* However, within a month the process flared again, and in May examina-tion revealed multiple widespread lichenoid, scaly, pustular crusted and weeping plaques(Figs. 4, 5, and 6), and spotty depigmentation without atrophy. The alopecia of the scalpillustrated in our first paper (1) remained unchanged. A patch test with atabrine at this timewas positive. On hospitalization from May to July, 1952, and following another similarlichenoid and pustular flare, in September 1953, nine years and five months after the onset,the dermatitis again responded well to bland therapy.
Fm. 6. T. 0. Eight years and one month after onset. Close-up of sacral plaque in Fig-ure 5.
DISCUSSION
In this second study we have presented additional evidence of prolonged andeven permanent disability resulting from post-atabrine dermatitis.
Long term manifestations include, in descending order of severity:(1) Anhidrotic asthenia. F. C. is permanently crippled by his severe wide-
spread complete anhidrosis, which incapacitates him for any physical exertionin a warm environment.
* IDrs. Lawrence Katzenstein and Herbert Mescon cared for the patient in the hospital.

290 THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
(2) Chronic or recurrent lichenoid and eczematous dermatitis. F. C. and T. 0.,both of whom are suffering from severe and extensive dermatitis over nine yearsafter the onset, are the most seriously invalided patients with post atabrinedermatitis we have encountered. It appears probable that their dermatitis willpersist indefinitely, in spite of treatment.
(3) Pruritus with no or minimal dermatitis.(4) Permanent alopecia. Of cosmetic importance only.(5) Skin atrophy. Of cosmetic importance only.We are unable to throw light on the relationship of epidermal sensitization
to atabrine (as demonstrated by a positive patch test), to persistence of derma-titis. Of the five patients suffering from post-atabrine dermatitis who werepatch tested with atabrine, two had positive reactions and three showed noreaction. The negative reactors were F. C., and patients 5 and 11 in Table 1.In all of these active dermatitis was present at the time of testing.
A number of investigators (22—25) have reported cross-sensitization to pro-caine, sulfonamide and para-aminobenzoic acid, the phenomenon demonstratedclinically in F. C. In addition Rogers (26) has seen cross-sensitization betweensulfonamide and procaine, and Baer (27) between sulfonamide and para-amino-benzoic acid. These chemicals contain a primary amino group in the para posi-tion, and this identity in chemical configuration is considered responsible forthe frequency of cross-sensitization, not only to the three substances to whichF. C. was found reactive, but also to paraphenylenediamine, azo dyes, benzo-cain, butesin and para-aminosalicylic acid. Baer (27) states that cross-sensitiza-tion may occur between chemicals with identical or closely related allergeniccomponents, so that the sensitized cells do not differentiate between them.Mayer (28) believes that the common property of the various substances in-volved in cross-sensitization is represented by the metabolic formation of oxida-tion or reduction products, probably compounds of quinone structure, and thatthese metabolites, rather than the original compounds, are the active antigens.With the exception of the warning by Livingood and Diuaide (2) that patientswith atabrine dermatitis frequently react to sulfonamides, we are not aware ofprevious reports of cross-sensitization to para-compounds in patients withatabrine dermatitis or post-atabrine dermatitis. Atabrine is also a para sub-stituted compound. It is suggested, therefore, that atabrine may also enter intocross-sensitization with the above mentioned chemicals, and that search forgroup sensitivity should be made in other patients with post-atabrine dermatitis.
The maximum incidence of atabrine dermatitis has been estimated at twoper thousand troops (4). It is probable that most patients who sustained atabrinedermatitis escaped without permanent disability, and that the number ofveterans seriously disabled as a result of post-atabrine dermatitis is small.
SUMMARY
1. Twenty-two veterans were observed who had had atabrine dermatitisduring World War II.
2. Eighteen of these were suffering from chronic or remittent eczematous or

STUDIES ON POST-ATABRINE DERMATITIS 291
liehenoid dermatitis of varying degrees of severity from three nnd a half to tenyears after the onset. Post-atabrine dermatitis is submitted as the name forthis entity.
3. In the great majority the dermatitis was \vorse during the summer.4. Thirteen patients had atrophic residua of the disease. Four presented per-
manent anhidrosis, eight permanent alopecia and ten cutaneous atrophy. Age,race, duration of atabrine ingestion and duration of observation could not becorrelated with presence or absence of atrophic residua.
5. Atabrine patch tests were positive in two of five patients with post-atabrinedermatitis.
6. Hands, feet and groin were the areas most frequently involved initially.Post-atabrine dermatitis also had a predilection for the hands, and the neck andlegs were next most frequently affected.
7. Incapacitating anhidrotic asthenia, due to permanent widespread completeanhidrosis, has been observed. The sweat glands were found to be functional,but because of destruction of the ducts, sweat could not reach the skin surface.
8. The reason for persistence of dermatitis years after contact with the allergenhas been discontinued is not known. It is suggested that escape of sweat intothe cutis as a result of permanent occlusion of the sweat ducts in the presenceof functioning sweat glands may be an etiologic factor.
9. Post-atabrine dermatitis, because of its banal appearance in some, anddespite the bizarre picture in others, is often misdiagnosed, even by experienceddermatologists.
10. One patient in this study presented cross-sensitivity to procaine, sul-fonamides and parn-aminobenzoic acid. As atabrine shares para substitutionwith these compounds it is suggested that this finding may not be merely coin-cidental.
CONCLUSION
Post atabrine dermatitis may cause serious and prolonged disability, as aresult of persistent or recurrent eczematous and lichenoid dermatitis, or, lessfrequently, as a result of anhidrotic asthenia.
REFERENCES
1. SCi-LAMBREG, I. L.: Studies on atabrine dermatitis. I. Long term observation of veteranswith permanent atrophic residua of the disease. J. Invest. Dermat., 17: 85, 1951.
la. ANDREw5, G. C.: Diseases of the Skin. W. B. Saunders Co., 2nd Edition, 1938, p. 141.lb. BECKER, S. W. AND OBERMAYER, M. E.: Modern Dermatology and Syphilology. J. B.
Lipincott and Co. 1st. Edition, 1940, p. 141.2. LTVINGOOD, C. S. AND DIRIJAIDE, F. R.: Evaluation of the untoward reactions attribut-
able to atabrine. J. A. M. A. 129: 1091, 1945.3. SCHMrTT, C. L., ALPINS, 0. AND CHAMBERS, C.: Clinical investigation of a new cutaneous
entity. Arch. Dermat. & Syph. §2: 226, 1945.4. STJLZBREGRR, MARTON B. AND BARR, H. L.: The 1945 Year Book of Dermatology and Sy-
philology, Addendum on Drug Eruptions Due to Atabrine (Quinacrine Hydrochloride)p. 30. The Year Book Publishers, Chicago, Ill.
5. BAZEMOHE, J. M., JOHNSON, H. H., SwANsoN, E. H. AND HAvMAN, J. M.: Relation of

292 THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
quinacrine hydrochloride to liehenoid dermatitis (atypical lichen planus). Arch.Dermat. & Syph. 54: 308, 1946.
6. WILsoN, D. J. : Eczematous and pigmentary lichenoid dermatitis. Atypical lichen planus;preliminary report. Arch. Dermat. & Syph. 54: 377, 1946.
7. AGRESS, C. M.: Atabrine as a cause of fatal exfoliative dermatitis and hepatitis, J. A.M. A., 131: 14, 1946.
8. BERESTON, E. S. AND SASLOW, M. S.: Complications of lichenoid dermatitis. Arch.Dermat. & Syph. 54: 325, 1946.
8a. PETEEKIN, G. A. AND HAIR, H. C.: Preliminary report of a dermatosis due possibly tomepacrine. A description of 26 cases seen in Italy. Brit. J. Dermat. & Syph. 58: 263,1946.
8b. BIGHAM, A.: Tropical lichenoid dermatitis. Brit. J. Dermat. & Syph. 58: 271, 1946.9. LIvINGOOD, C. S.: Dermatologic problems in the returning veteran. Pennsylvania
M. J. 50: 581, 1947.
10. NIsBET, T. W.: Dermatitis due to quinacrine hydrochloride (atabrine). J. A. M. A.134: 446, 1947.
11. SULZBERGER, MARION B.AND BALE, H. L. : The 1947 Year Book of Dermatology & Syphil-
ology. Editorial Comment, pa. 206, The Year Book Publishers, Chicago, Ill.12. MILLER, 0. B., HEREMANN, F. AND HUBIN, J.: The effects of mepacrine hydrochloride
(atabrine) upon the human skin. J. Invest. Dermat. 15: 445, 1950.13. HEEEMANN, F. AND MILLER, 0. B.: Pharmacologic and pathogenetic effects of mepacrine
chloride (atabrine) upon the human skin. 1. Clinical and experimental observations.Acta Dermato-Venereol. 32: 304, 1952.
14. HEEEMANN, F. AND MILLER, 0. B.: Pharmacologic and pathogenetic effects of mepacrinechloride (atabrine) upon the human skin. 2. Microscopic studies of vital staining effectin the skin. Ibid. 32: 317, 1952.
15. SEELLEY, W., HOEvATH, P. AND PILLSBURY, D. M.: Anidrosis, an etiologic interpreta-tion. Medicine 29: 195, 1950.
16. SULZBEEGEE, MARION B., HERRMAN, F. AND ZAK, F. G.: Studies of sweating. I. Prelim-inary report with particular emphasis on a sweat retention syndrome. J. Invest.Dermat. 9: 221, 1947.
17. SULzBERGEE, MARION B., HEEEMANN, F., KELLER, H. AND PISHA, B. V.: Studies ofsweating. III. Experimental factors influencing the function of the sweat ducts. J.Invest. Dermat., 14: 91, 1950
18. GOLDBERG, L. A.: An unusual lichenoid dermatosis, J. A. M. A. 130: 775, 1946.19. ScHMITT, C. L.: Present status of quinacrine (atabrine) dermatitis. Heport of six cases.
Arch. Dermat. & Syph. 59: 16, 1949.20. BLANK, H.: Personal Communication.
21. SHELLEY, W. B. AND MEscoN, H.: Histochemical demonstration of secretory activityin human eecrine sweat glands. J. Invest. Dermat. 18: 289, 1952.
22. SULZBEEGEE, MARION B., KANOF, A. AND BARE, H. L.: Sensitization by topical appli-cation of sulfonamides, J. Allergy, 182: 92, 1947.
23. BAEE, H. L. AND MELTzEE, L.: Sensitization to monoglyceryl para-aminobenzoate.Preliminary report. J. Invest. Dermat., 11: 5, 1948.
24. MELTzEE, L. AND BARE, H. L.: Sensitization to monoglyceryl para-aminobenzoate. Acase report. J. Invest. Dermat., 12: 31, 1949.
25. SIDI, E. AND DOBKEvITcE-MOEEILL, S.: The injection and ingestion test in cross sen-sitization to the para group. J. Invest. Dermat. 16: 299, 1951.
26. HOGEES, E. B.: Sensitization reaction to sulfanilamide, J. A. M. A. 111: 2290, 1938.27. BARE, H. L.: Examples of cross sensitization in allergic eczematous dermatitis. Arch.
Dorm. & Syph., 58: 276, 1948.28. MAYER, H. L.: Compounds of quinone structure as allergens and cancerogenic agents.
Experientia., 6: 241, 1950.