Embed Size (px)
Citation preview


( ) ) - فاكس: ) ٠١المركز الرئيسي: عمارة القصيبي - طريق الملك عبد العزيز - ھاتف: ٤۷۷١۳۷٤ ٠١ ٤۷۹۳٠٠٠
١٥٤ س ت - غ.ت: ١٠١٠٠٠۷۹٠١
( ) - الــدمــام - ھاتف: ( ٠۳ جــــدة - ھاتف: ( ۸٤۷٥٢۹۹ ٠٢ ٦۷٢٠۸۸۸
١١٤١١ص.ب الرياض - المملكة العربية السعودية ٢١٥
www.aralgosaibico.com
سـلسـلة امـداد حلقـاتهـا مـرنـة٦٥نخـدم المجـال الصحـي ألكثـر من عـامــاً

i
MJHS Editorial Board
EDITOR-IN-CHIEF
PROF. MOHAMMED AL-RUKBAN Vice Rector, Majmaah University and Dean, College of Medicine, Majmaah Uni-versity
EDITORIAL BOARD
PROF. ABDULRAHMAN M. AL MAZROU, FRCPC
Professor. of Pediatrics, KSU
Consultant, Pediatrics Infectious Diseases
Chief Supervisor & Dean AlRajhi colleges, Qassim, KSA
PROF. FAROOQ KHAN Professor of Medicine, State University of New York. Director Research and Publication Stony Brook, New York PROF. OMAR HASAN K KASULE, Sr MB ChB (MUK), MPH (Havard), DrPH (Havard), Faculty of Medicine at King Fahd Medical City, Riyadh Saudi Arabia. Professor of Epidemiology and Islamic Medicine Institute of Medicine, University of Brunei & Visiting Professor of Epidemiology, University Malaya
PROF. MOHAMMAD FAHEEM Head, Department of Physiology, Hamdard Institute of Medical Sciences & Research, Jamia Hamdard, New Delhi, India.
DR. IBRAHIM AL-HOQAIL Associate Professor Dermatology, College of Medicine, King Saud University
MAJMAAH JOURNAL OF HEALTH SCIENCES A JOURNAL PUBLISHED BY MAJMAAH UNIVERSITY
CONTENTS
Preface Prof. Mohammed Othman Al-Rukban, Editor in Chief Erratum Original Articles
A Comparison between Siwak and Tooth Brush use on Oral Hygiene in Sudanese Adults. Wafaa Abdelraouf Hussein Khalil, Mohammed Yousif Sukkar , Bakri Gobara Gismalla
Reliability of INFANIB among normal and high risk term neonates: A cross sectional study. Wong MY, Sai Lakshmi Ganesan, UV Shenoy, Jaya Shanker Tedla, VS Binu Knowledge and Attitudes of the Public, Primary Health Care Physicians and other Health Professionals, and Policy Makers towards Religious Medical Practices. Abdulla Bin Mohamed AlBedah, Asim Abdelmoneim Hussein, Ahmed Tawfik ElOlemy, Mohamed Khalil, Ibrahim AlSubai
Evaluation of Hepatitis B Core Antibody (Total) in the presence of ID-NAT. Ranjay Kumar Choudhary , Moattar Raza Rizvi
Reference Range For Copper In Adult Population of Lahore- Pakistan. Warda Hussain, Asim Mumtaz, Sana Khan, Tauqeer Butt Complementary and Alternative Medicine Use among Health Workers in Mid-Delta, Egypt. Ahmed Tawfik Mohammed ElOlemy, Nashwa Moham-med Radwan Ibrahim, Walid Mostafa AbdElHameed Dawood , Ihab AbdElHameed Mohammed Abo Ali , Latifa Mahmoud Fouda How many subjects should be studied: Sample Size Determina-tion through Hypothesis testing and Confidence interval. Waqas Sami, Mohammed Othman Al-Rukban, Mohammed Almansour, Tayyaba Waqas, Kamran Afzal, Rehan Asad
ISSN: 1658-645X Ref No.: 1434/5421
i iii iv 1 7 14 22 29 35 43

ii
MAJMAAH JOURNAL OF HEALTH SCIENCES A JOURNAL PUBLISHED BY MAJMAAH UNIVERSITY
CONTENTS
Case Report
Ultrasound and Phonophoresis effect on eczema lesions in a 37 year old male patient: A single case study. Jaya Shanker Tedla, Irshad Ahmad Unusual Presentation of Behcet Disease (NEURO-BEHCET) Abdulrahman Abdulwahab Alduraywish
MJHS Editorial Guidelines
Upcoming Conferences
DR. ABDULLAH ALI AL-GHASHAM Dean, College of Medicine, Qaseem Uni-versity, KSA
DR. SAMUEL LEE, Professor of Medicine, University of Calgary, Canada Head, Division of Gastroenterology, Foothills Hospital Gastrointestinal Research Group
EDITORIAL ASSISTANTS
DR. KHALID TOHAMI MD. Assistant Professor, Community Medicine, College of Medicine, Majmaah University
DR. MOHAMMED AL-MANSOUR MRCGP (INT), ABFM, SBFM. Assistant Professor, Family Medicine College of Medicine, Majmaah University
DR. FUZAIL AHMAD PHD PT, Lecturer, Department of Physical Therapy & Rehabilitation, College of Applied Medical Sciences, Majmaah University
DR. MOATTAR RAZA RIZVI PHD PHYSIOLOGY, Assistant Professor, Department of Medical Lab Technology, College of Applied Medical Sciences, Majmaah University.
MR. WAQAS SAMI MSC BIOSTATISTICS, Lecturer, Department of Public Health & Community Medicine, College of Medicine, Majmaah University
ISSN: 1658-645X Ref No.: 1434/5421
49 53 58 62

PREFACE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
iii
PREFACE
The first issue of the Majmaah Journal of Health Sciences was a great success in every respect.Not only was the quality of the scientific articles high, so was the enthusiasm and willingness withwhich our researchers and clinician alike have submitted their contributions. The editorial quality andthe design of our own journal are also in line with what may be expected of a scientific journal.
Majmaah Journal of Health Sciences has passed an important first test. The editorial team hassucceeded in making a high quality journal with its own image, with readable content and with aninterested and involved group of authors and readers. The challenge is now to continue and proceedon this chosen path. One issue does not make a journal yet. It is up to us to deliver content andcommitment over the coming years, which can result in a new, valuable tradition supporting thescientific development in health sciences.
This second issue of the Majmaah Journal of Health Sciences is the result of the dedicatedcontributions of many persons. We thank our editors for sharing their invaluable editorial experiencewith us. They have played outstanding role in taking on responsibilities to assist in the developmentand running of this journal. The editorial board has done a tremendous job; I thoroughly enjoyed theprofessionalism and enthusiasm of our editorial team.
The peer-reviewing processes developed for the journal engages leading scientists and clinicians inthe field of health sciences, and, working together with a robust editorial structure, they ensures thehighest quality and most original studies are published. The journal recognizes the support of itsreviewers, which is of the vital importance to its success.
We gratefully acknowledge the continuing guidance of Majmaah University’s Rector Dr. Khalid binSaad Al-Meqrin, Vice Rector, Dr. Mohammad Abdullah Al-Shaya and Dean Scientific Research Dr.Mohammad bin Nasser Al-Suwaid for their leadership and support, which has been instrumental inthe formation and running of this journal.
The journal would not be here before you without the continuous efforts of the editorial assistants Dr.Mohammed Al-Mansour, Dr. Khaled Al-Tohami, Dr. Moattar Raza Rizvi, Dr. Fuzail Ahmad and Mr.Waqas Sami, who kept us all; authors, reviewers and editors, on track and consequently made theJournal’s timely publication possible.
But most of all I would like to thank all authors who submitted their paper to the journal. I hope theyenjoyed the experience of getting their paper criticized and often improved by the reviewers’ andeditors’ comments.
I am grateful to all of those involved in the production and publication of this and future issues, andhope the demands of our readers and scientific community are met. May the Majmaah Journal ofHealth Sciences continue to be a success.
Prof. Mohammad Othman Al RukbanEditor in ChiefMajmaah Journal of Health SciencesVice Rector, Academic Affairs &Dean, College of Medicine,Majmaah University

ERRATUM MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
iv
ERRATUM
Erratum to CDP-CHOLINE NEUROPROTECTION AND VASCULAR REMODELLINGVIA IRS-1 MECHANISMS IN VASCULAR DEMENTIA- GROWING NEURONS ATOPMICROELECTRONIC CHIPS AS A NEW MODEL FOR NEURODEGENERATION
1*Raid Al -Baradie, 2Stephen Lynch, 3J Borresen, 4Jerzy Krupinski, 5Mark Slevin
MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 1
Received: 20 December, 2012; Accepted: 15 February, 2013
Copyrights© 2013 by Majmaah University. All right reserved.Reproduction without permission is prohibited. No part of this publication may be reproduced or transmitted in any form orby any means, electronic or mechanical, including photocopy, recording or any information and retrieval system withoutpermission in writing from the publisher. All article published, including editorial, letter and book review, represent theopinion of the authors and do not reflect the official policy of the publisher or the institution with which the author isaffiliated, unless it is clearly specified.
This erratum is inscribed with reference to the published paper “Raid Al -Baradie, Stephen Lynch, JBorresen, Jerzy Krupinski, Mark Slevin CDP-CHOLINE NEUROPROTECTION ANDVASCULAR REMODELLING VIA IRS-1 MECHANISMS IN VASCULAR DEMENTIA-GROWING NEURONS ATOP MICROELECTRONIC CHIPS AS A NEW MODEL FORNEURODEGENERATION. MJHS 2013; 1:11-16.
” The affiliation of the corresponding author Dr. Raid Al-Baradie should be written as “1AssistantProfessor, Pathology, College of Applied Medical Sciences, Majmaah University, Al-Majmaah, Saudi Arabia”and not “1Assistant Professor, Family Medicine, College of Medicine, Majmaah University, Al-Majmaah, Saudi Arabia.”
In addition, the caption for figure 1 should be read as “Figure 1 Possible signaling pathways throughmCRP linked to neuronal degradation and Alzheimer's disease/vascular dementia.” And not Figure 1shows the operation of a binary half-adder based on Fitzhugh-Nagumo oscillators (which aresimplified versions of the Hodgkin-Huxley models).
This has been corrected in the PDF versions of the manuscript and made available onlinehttp://mu.edu.sa/en/departments/majmaah-journal-health-sciences/current-issue-0

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Role of Siwak & Tooth Brush, Wafaa A Khalil et al. 1
ROLE OF SIWAK IN THE MAINTENANCE OF ORALHOMEOSTASIS AND DENTAL HYGIENE COMPARED WITH
TOOTH BRUSH*Wafaa A Khalil1, Mohammed. Y. Sukkar2, Bakri G Gismalla3
ABSTRACT
While previous research on Siwak has mostly focused on its microbiological effects, thisresearch is aiming to evaluate its role on the maintenance of oral homeostasis and dentalhygiene, an important factor for preventing caries and periodontal diseases. Two groups ofsubjects were studied: regular Miswak (n=60) and tooth paste brush users (n=59). Miswakused was from the “Arak” tree of Sudan, species of Salvadora Persica. Oral hygiene wasassessed by measurement of plaque index (PI), gingival index (GI) and decayed, missing andfilled (DMF) indices. The (PI) was significantly higher in Miswak users, but no differencewas noted in the DMF and GI values. A positive correlation was found between DMF valuesand age among Miswak users, as well as between gingival and plaque index on both studygroups. These findings suggest that use of Miswak offers a good option for maintaining oralhomeostasis and hence in preventing periodontal disease and cares formation.
KEY WORDS: Siwak; Miswak use; oral homeostasis; dental hygiene; dental plaque;periodontal disease.
ف على طرق لمكافحة لویحات األسنان الجرثومیھ یمكن استخدامھا یومیاً وبأمان. یُلحظُ اھتمام متزاید للتعر: المستخلصلقد تمت دراسات سابقة للجوانب األحیائیة المجھریة إلستخدام شجرة األراك (السواك)، بینما دراستنا الحالیة ھدفت إلى
لي في مكافحة التسوس وأمراض اللثة تقیم دور السواك فى المحافظة على مستوى التوازن واألستواء الصحي للفم وبالتاالسنیة. تضمنت الدراسة مجموعتین الجرثومیھواألسنان، وذلك من خالل أثره الكمیائي والمیكانیكي على اللویحات
وعددھم تسع وخمسون ، ومستخدمي معجون وفرشة األسنان بإنتظاموعددھم ستونرئیسیتن: مستخدمي السواك بانتظامبیرسكا والتي تكثر ا.أعواد السوك المستخدمھ كانت من شجرة األراك من فصیلة سلفادوروعتینبالغا متطوعا من المجم
كان . زراعتھا بالسودان. تم تقیم صحة الفم بقیاس مؤشر اللوحة السنیة ومؤشر اللثة ومؤشر تلف وفقدان وحشو األسنانیكن ھنالك فروق ذات داللة احصائیة في مؤشري حات السنیة أعلى بداللة احصائیة في مستخدمي السواك. لمیمؤشر اللو
اللثة وتلف وفقدان وحشو األسنان. كان ھنالك ارتباط أیجابي بین مؤشرتلف وفقدان وحشو األسنان والعمر في مستخدمي ھذه السواك. كما كان ھناك ارتباط ایجابي ذو داللة احصائیة بین مؤشر اللثة ومؤشر اللویحة السنیة في محموعتي الدراسة.
وبالتالى في منع تكون اللویحات السنیة واالسنانالنتائج تسنتج أن السواك قدیكون بدیالً جیداً في الحفاظ على صحة الفم التسوس.
Received: 26 March, 2013; Accepted: 13 June, 2013
*Correspondence: [email protected] Professor, Basic Sciences Department, Faculty of Dentistry, Khartoum University.2Professor,Physiology Department , Faculty of Medicine, Khartoum University.3Associated Professor, Periodontal Department, Faculty of Dentistry, Khartoum University.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Role of Siwak & Tooth Brush, Wafaa A Khalil et al. 2
INTRODUCTION
Oral hygieneis one of the most importantfactors for maintenance of oral homeostasisand health.1 The pathogenic natureof thedental plaque biofilm can be diminished bymaintaining normaloral flora via oralhygiene procedures such as toothbrushing,flossing and rinsing with anantimicrobial mouthrinse,whichcancompletely prevent caries and periodontaldiseases.2-4 Fluoride found in most toothpastes and mouth rinses, is known for itsanti caries properties which is attributed tothe formation of fluroapatite, calciumfluoride, leading to increase of enamelresistance to demineralization.5 Moreover,it reduces pH fall during frequent ingestionof carbohydrates.
The name miswak,an Arabic word meaningtooth cleaning stick, is known in English asthe "natural toothbrush",6-8 the mostcommon species is the medicinal plantSalvadora persica,, also known as Arak inEast Africa through to the ArabianPeninsula and the Asian subcontinent6,9 forcenturies and its fibrous branches have beenpromoted by theWorld HealthOrganization, for oral hygiene use.
When properly used, miswak had beenreported to be as effective as toothbrushing.10-12 Besidethe mechanical effectsof its fibers, if Left in mouth, stimulatesalivation and release of beneficialchemicals13; thus, there may be a bettercleansing effect. The roots of S. persica,contains a number of identifiedantimicrobial and other prophylacticcomponents including fluoride, alkaloids,sulphur compounds glucosinolates, andvolatile oils such as benzyl isothiocyanate.As to other researchers, Salvadora persica ,contains, in large amounts silica, sulphur,vitamin C, and small amounts of tannins,saponins, flavonoids and sterols. It alsocontains,trimethyline, salvadorine,chlorides, fluoride.14-18 The tannins and
resins have an astringent effect on themucus membrane and form a layer ofenamel, thus giving protection againstcaries.19
Baghdady and Gose in 1979 conducted astudy comparing caries prevalence amongIraqi and Sudanese schoolchildren using theWHO DMFT (diseases, missing, filledteeth) index. Their results reported thatSudanese children showed lower cariesprevalence due to use of miswak and theirdiet.20
Daroutet al (2000) also reported that theperiodontal status of miswak users in aSudanese population was better than that oftooth brush users, suggesting that theefficiency of miswak use for oral hygiene iscomparable or even better than toothbrush.21
A 2003 scientific study comparing the useof miswak with ordinary tooth brushesconcluded that the results clearly were infavor of the users, who had been using theMiswak, provided they had been givenproper instruction in how to brush using it[11]. The aim of this study is to comparemiswak use with conventional tooth pasteand brush use on dental health.
SUBJECTS AND METHODS
A volunteer non-probability Samplingtechnique was used to recruit studyparticipants. Volunteers were interviewedand verbal consent was taken. Oral hygienehabits were assessed using a structuredquestionnaire. The study was conducted ontwo categories of subjects: regular Miswakusers, regular tooth paste and brush users.One hundred and nineteen volunteerstudents and employees in the Faculty ofMedicine U of K, and from Masjid Bilal inJabra, Khartoum participated in the study.Age of the participants range was 18-65years.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Role of Siwak & Tooth Brush, Wafaa A Khalil et al. 3
Periodontal status was assessed clinicallyusing gingival and dental plaque indices(GI, PI) and decayed, missing and filled(DMF). The miswak used by theparticipants, from the “Arak” tree of Sudan,species of Salvadora Persica.Inclusioncriteria included regular miswak and brushusers, good general health, absence ofchronic illnesses such as diabetes andhypertension, no past or present history ofsmoking or snuff use (Tomback languages).Also excluded from our study, those whohad used antiseptic mouth wash or receivedantibiotics for at least one month beforeclinical assessment.
Periodontal status: Assessed on sixsextants/subject according to Loe andSilness22 for GI, PI and WHO23 for DMF.
Gingival index system as follows:
Appearance Bleeding Inflammation Points
Normal Nobleeding
None 0
Slight changein color andmild edemawith slightchange intexture
Nobleeding
Mild 1
Redness,hypertrophy,edema ,glazing
Bleedingon
probing/pressure
Moderate 2
Markedredness,hypertrophy,edema,ulceration
Spontaneous
bleeding
Sever 3
Gingival index mean calculation
The index for each volunteer is obtained bysumming the indices for all six teeth anddividing by six.
Plaque index calculation: The index of thesubject was obtained by summing theindices for all six teeth and dividing by six.
Plaque index system as follows:
Scores Criteria0 No plaque
1
A film of plaque adhering to the freegingival margin and adjacent area of thetooth. The plaque may be seen in situonly after application of disclosingsolution or by using the probe on toothsurface
2
Moderate accumulation of soft depositwithin the gingival pocket, or the toothand gingival margin which can be seenby the naked eye
3Abundance of soft matter on the toothand gingival margin.
Disclosing agent: used was in the form oftablets colored (red-cote dentdisclosingtabs. butler Code No 130065-0),examination was performed after chewingone tablet where supra gingival plaquecould be seen as a violet or purple spots.
Sites of examination: The teeth examinedin GI and PI represented six sites and 4surfaces on each tooth: 1)buccal,2)lingual, 3)mesial, 4)distal
DMF index: DMF index has beenrecommended by WHO, as a parameter toassess the dental health situation in varioussocieties.
DMF index calculation: The DMF indexmean was calculated simply as the totalnumber of decayed teeth (D), Missed (M)and Filled (F) teeth divided by the numberof cases investigated. Great variationsbetween societies, has been noted.
Statistical analysis: The data has beenorganized and analyzed using the statisticalprogram SPSS (Statistical Packages forSocial Sciences):The T-test for equality ofmeans; Regressions and curve estimationswere used to show relationships betweendifferent parameters; Descriptive statistics,include cross- tabulations; simple charts.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Role of Siwak & Tooth Brush, Wafaa A Khalil et al. 4
RESULTS
Below intermediate education, Miswakusers were 28.3% compared to 6.8% ofbrush users.Table.1
Education
level
Miswak BrushFr
eque
ncy
Perc
enta
ge
Freq
uenc
y
Perc
enta
ge
Illiterate 2 3.3 0 0
Elementary
school/ khalwa
15 25.0 4 6.8
Intermediate
school
9 15.0 6 10.2
Secondary
school
20 33.3 17 28.8
High education 14 23.3 27 45.8
Periodontal status concerning GI and DMF,were the same in both study groups(p=0.345, 0.390); higher PI index wasfound in Miswak users (p=0.034)[Table.2.].
Table.2. Comparison of the oral hygieneindices between study groups
Oralhygienemeasures
Miswak Brush
N Mean±SD
N Mean±SD
p-value
DMF 55
4.24± 4.13 52
5.00± 4.19 0.345
PI 60
1.62± 0.64 55
1.36± 0.62 0.034
GI 60
1.32±0.50 55
1.40±0.53 0.390
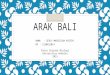
Also in Miswak users only DMF was foundto be related positively to age(p=0.009)[Fig.1], while no correlation
between age and DMF in brush users(p=0.127), nor between other indices andage in both study groups.
Fig.1.Relationship of the DMF index to agein Miswak users
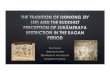
Strong positive correlation was foundbetween Gingival index (GI) and Plaqueindex (PI) in both study groups(p=0.000)[Fig.2]. No relationship had beendetected in both study groups between oralhygiene indices and years of toothbrush orMiswak use, nor with duration andfrequency of use.
Brush (r=0.305, p-value=0.000), Miswak(r=0.243,p-value=0.000)
Fig.2. Relationship between the PI and theGI index in both study groups

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Role of Siwak & Tooth Brush, Wafaa A Khalil et al. 5
DISCUSSION AND CONCLUSION
Illiterate and elementary school educationrepresented (28.3%) of miswak userscompared to only (6.8%) among brushusers, indicating more frequent use ofSiwak compared to brush use among loweducational, and probably also low socio-economic groups in the community. Thestrong relationship between DMF and agein miswak users can only be explained byother studies that showed that DMF indexis directly correlated with the health &economic, cultural, social state of thesociety and therefore it can be used forcomparative studies.24
A direct significant relationship between PIand GI was found in both study groups,demonstrate the well, known relationshipbetween dental plaque and periodontaldisease.25
The three known periodontal variablesassessed (DMF, PI, GI), showed nosignificant differences between studygroups except for the plaque index (PI)where higher index was found in regularmiswak users compared to the brush users;a finding which could suggest improper useof miswak,11 as this is contrary to otherstudies that found that miswak efficacy wascomparable to that of the conventionaltooth brush.26 Gazi had demonstrated thatthere were no significant differences inplaque scores measurements betweenhabitual miswak and toothbrush and thatplaque scores could be significantly lowerfollowing the use of miswak whencompared with the conventional toothbrush, if used without tooth paste.12 Eidalso reported that the majority of miswakusers apply miswak to both aspects of theirteeth and that there was no significantdifference in plaque scores and attachmentloss noted between miswak and tooth brushusers.27 Higher (PI) in miswak userswithout significant difference in the (GI)and (DMF), despite the positive
relationship between PI and GI may suggestthe interplay of some other factors in Siwaksuch as abrasives, antiseptics, astringent,detergents, enzyme inhibitors and fluoride,that may suggest miswak as to be ofcomparable efficacy to that of theconventional tooth brush.
REFERENCES
1. Thomas and Nakaishi. Managing thecomplexity of a dynamic biofilm. J AmDent Assoc. 2006; 137: 10-15.
2. Mathiesen, A. T, Øgaard B, and Rølla G.Oral hygiene as a variable in dental cariesexperience in 14-year-olds exposed tofluoride. Caries Res. 1996; 30:29-33
3. Preeti Gupta, Gaurav Gupta. Tooth brushand tooth brushing. Indian journal of dentalscience 2009; 1: 5-8
4. Stecksen-Blicks C, GustafssonL. Impact oforal hygiene and use of fluorides on cariesincrement in children during oneyear.Community Dent. Oral Epidemiol1986; 14:185-189.
5. Bradshaw DJ, McKee AS, and Marsh PD.Prevention of population shifts in oralmicrobial communities in vitro by lowfluoride concentrations. J. Dent. Res.1990;69:436-441.
6. Elvin-Lewis M. Plants used for teethcleaning throughout the world. AmericanJournal of Preventive Medicine 1980; 6:61-70.
7. Hattab FN. Meswak: the natural toothbrush.J Clin Dent 1997; 8: 125-9.
8. Al Sadhan RH, Almas K. Miswak (chewingstick): A cultural and scientific heritage.Saudi Dent 1999; 1: 80-7.
9. Almas K, Al-Lafi TR. The natural toothbrush.World Health Forum 1995; 16: 206-10.
10. Darout IA, Albandar JM,SkaugN.Periodontal status of adultSudanese habitual users of miswak chewingsticks or toothbrushes.ActaOdontolScand2000; 58: 25-30.
11. AI-Otaibi M, Al-Harthy M, SِderB,Gustafsson A, Angmar-Mهnsson B.Comparative effect of chewing sticks andtoothbrushing on plaque removal andgingival health. Oral Health Prev Dent2003; 1:301-307.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Role of Siwak & Tooth Brush, Wafaa A Khalil et al. 6
12. Gazi M, Saini T, Ashri N, Lambourne A.Miswak chewing stick versus conventionaltoothbrush as an oral hygiene aid. ClinPrevDent 1990; 12: 19-23
13. Hardie J, Ahmed K. The miswak as an aidin oral hygiene. J Phillip Dent Assoc. 1995;47: 33-38.
14. MS, Ajmal M. Significance of chewinggums (Miswak) in oral hygiene from apharmacological view-point. J Pak MedAssoc. 1981; 31:89-95.
15. Khalessi AM, Pack AR, Thomson WM,Tomkins GR. An in vitro study of theplaque control efficacy of Persica: Acommercially available herbal mouthwashcontaining extracts of Salvadora Persica.Int. Dent. J. 2004; 54: 279-83.
16. Almas K, Al-Zeid Z. The immediateantimicrobial effect of a toothbrush andMiswak on cariogenic bacteria: A clinicalstudy. J.Contemp. Dent. Pract.2004; 5: 105-114.
17. Al-Lafi T, Ababneh H. The effect of theextract of the Miswak (Chewing stick) usedin Jordan and the Middle East on oralbacteria. Int dent J. 1995; 45: 218-222.
18. Ezmlrly ST, Cheng JC, Wilson SR. SaudiArabian medicinal plants: SalvadorapersicaPlanta Med 1979; 35: 191-192.
19. Almas K, Al-Lafi TR. The natural toothbrush.World Health Forum 1995; 16: 206-10.
20. Baghdady VS, Gose LJ. Comparison of theseverity of caries attack in permanent first
molars in Iraqi and Sudaneseschoolchildren.Community Dental OralEpidemiology 1979; 7:346-8.
21. Darout IA, Albandar JM, Skaug N.Periodontal status of adult Sudanesehabitual users of miswak chewing sticks ortoothbrushes. Acta Odontol Scand 2000;58: 25-30.
22. Loe H. The Gingival Index, the PlaqueIndex, and the Retention Index. JPeriodontol 1967; 38: 610-616.
23. World Health Organization. Oral healthsurveys. Basic methods. Geneva. WHO1987.
24. Barmess, DE. Features of oral health careacross cultures, International Dental Journal1976; 26: 353-68.
25. SCHROEDER MDS, RIBEIRO GLU,RIBEIRO BV. Evaluation of periodontalindex of gingival and plaque with dentalcrowding in development of gingivits inchildren and adolescents. de odontologic2004; 1: 17-21.
26. Sote EO.The relative effectiveness ofchewing sticks and toothbrush on plaqueremoval. Afr Dent J 1987;1:48-53.
27. Eid MA, Selim HA, Al-Shammery AR.Relationship between chewing sticks(Miswak) and periodontal health Part 1.Review of literature and profile of thesubjects. Quintessence International 1990;21: 913-917.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 7
RELIABILITY OF INFANIB AMONG NORMAL AND HIGH RISKTERM NEONATES: A CROSS SECTIONAL STUDY
MY Wong1, Sai L Ganesan2, UV Shenoy3, *Jaya S Tedla4, VS Binu5
ABSTRACTBackground: Infant Neurological International Battery (INFANIB) is one of the commonneurological assessment used for the infants. The reliability in the newborns is moreessential to prove because INFANIB is used to predict the infant motor capabilities at laterstages. Objective: Objective of the study is to establish intra-rater and inter-rater reliabilityof Infant Neurological International Battery between normal and high risk term neonates.Methods: In this cross sectional study a convenience sample of term neonates was included.Demographic data were completed from medical records. Rater one administered INFANIBon all the neonates and the assessments were being videotaped. The videos were anonymizedand were viewed by two independent raters so they were blinded from knowing the groupsfrom which each neonate belonged to. Rater three viewed 50 videos randomly for assessmentof intra-rater agreement after one month. All the raters were blinded from scores of oneanother as well to avoid bias during assessment. For intra- as well as inter-rater reliability,two-way mixed, absolute agreement and single measure ICC was calculated. Results: 112neonates (normal=56; high risk=56) with mean (SD) gestational age of 39.1 (1.1) and 38.9(1.1) weeks respectively on mean post natal day of 4 were assessed. For intra-rateragreement the ICC was 0.42 (0.05-0.7) for normal neonates and 0.33 (0-0.63) for high riskneonates. For inter-rater agreement the ICC was 0.1 (0-0.26) for normal neonates and 0.28(0.05-0.5) for high risk neonates. Conclusions: The intra-rater and inter-rater reliability ofINFANIB proved to be poor between the normal and high risk term neonates. Formaltraining should be given to any profession or health workers who are planning to useINFANIB as a screening tool for early neurodevelopmental delay among neonates toimprove the inter-rater agreement.
KEY WORDS: Neonatology, Neurodevelopment, Reliability, INFANIB, Screening.
الجھازلتقییمشیوعاالنظماكثرمنواحدةھي) INFANIB(الرضعلألطفالالدولیةالعصبیةالبطاریة:ملخصیتمألنھالوالدةحدیثياألطفالعليشفالكفيالوسیلةھذهموثوقیةاثباتاالھمیةمنو, الرضعلألطفالالعصبيموثوقیةتحدیدھوالدراسةھذهمنالھدف: الھدف. الحقةمراحلفيللرضعالحركیةبالمقدراتللتنبؤالنظامھذااستخدام
ھي:البحثمنھج. عاليخطورةمعدلذوواخرینطبیعیینوالدةحدیثيیقیمونالذینالمقیمینمختلفبینالتقییمنظاممنالدیموغرافیةالبیاناتاخذتوقد. النموكامليالوالدةحدیثياالطفالمنمناسبةعینةعلياشتملتمقطعیةدراسة
روجعت. بالفیدیووالتقییمالكشفعملیةتصویرجريواالولالمقیمبواسطةاالطفالكلتقییمتمثمالطبیةالسجالتعشوائیافیدیو٥٠عرضتمالتقییممنشھربعد. االطفالیتبعفئةأليةمعرفدوناخرینمقیمیینقبلمنالفیدیوھات
لتفادياالخرنتائجمعرفةدوندورهاديمقیمكل. والثانياالولالمقیمبینالنتائجفيالتوافقلمعرفةثالثمقیمعليTwo-way mixed, absolute(االرتباطمعاملباستخدامالتحلیلتمالمقیمیینبینالموثوقیةلحساب. االنحیاز
agreement and single measure ICC .(
Received: 21 March, 2013; Accepted: 2 June, 2013
*Correspondence: [email protected] of Paediatrics, Kasturba Medical College, Mangalore, India; 2Ex-Professor, Department ofPhysiotherapy, Kasturba Medical College, Mangalore, India; 3Professor, Department of Paediatrics, KasturbaMedical College, Mangalore, India; 4Assistant Professor, Program of Physical Therapy, Department of MedicalRehabilitation Sciences, College of Applied Medical Sciences, King Khalid University, Abha, Kingdom of SaudiArabia; 5Senior Grade Lecturer, Department of Statistics, Manipal University, Manipal, India.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 8
في(التقییمكانوقد) عالیةخطورةمعدلذو٥٦وطبیعي٥٦( والدةحدیثطفل١١٢لعددالتقییمتم:النتائج٣٨،٩وطبیعیینلل١،١معیاريانحرافمعأسبوع٣٩،١الحمليالعمرمتوسط. للوالدةالرابعالیومفي) المتوسط
٠،٤٢كانتوالثانياالولالمقیمیینبیناالرتباطمعامل. العالیةالخطورةلذوي١،١معیاريانحرافمعأسبوعبیناالرتباطمعامل. العالیةالمخاطرذوالوالدةلحدیثي) ٠،٦٣-٠(٠،٣٣والطبیعیةالوالدةلحدیثي) ٠،٧حتي٠،٠٥(
ذوالوالدةلحدیثي) ٠،٥-٠٫٠٥(٠،٢٨والطبیعیةالوالدةلحدیثي) ٠،٢٦- ٠(٠،١كانتواالخرینالثالثالمقیمبینالمختلفینالمقیمیینبواسطةالتقییمنظامتطبیقفيالموثوقیةضعفالدراسةاثبتت: االستنتاجات. العالیةالمخاطر
الذینالصحيالمجالفيللعاملینميالرسالتدریبیستوجبمما, العالیةالمخاطروذويالطبیعیینالوالدةحدیثي.الوالدةحدیثيبینمبكروقتفيالعصبيالنموتأخرلتشخیصأوليفحصكأداةلألطفالالدولیةالبطاریةیستخدمون
INTRODUCTION
Neonatal period is a crucial period indetecting neurological illness.1 Variousstudies have shown the value of earlyidentification of developmental delayamong children.2,3 Following which timelyintervention can be given, these includephysical therapy, speech and languagetherapy, occupational therapy and sensoryintegration. Evidence showed that earlytreatment of developmental delay leads tobetter outcomes for children and reducesthe costs of providing health care,educational support and treatment services.Hence, there is an increasing emphasis onthe use of appropriate developmentalscreening for children and early detectionof neurodevelomental delay. The idealscreening method should be a standardizedand validated tool with establishedpsychometric properties, easy to performand interpret, cost effective, and have agood sensitivity and specificity.2
Infant Neurological International Battery(INFANIB) was designed to assess themotor development of infants whosecorrected gestational age ranged from 0 to18 months though INFANIB wasconstructed based on a study consisted ofinfants from age three to 22 months in198.4,5 In view of motor development that ismost rapid in infancy,6 INFANIB is ascreening tool used for early detection ofgross motor developmental delay.7INFANIB has 20 items which were selectedfrom four methods of neurological
examination: 1) the Milani-Comparetti andGidoni method, 2) the French “angles”method, 3) the primitive reflexes method,and 4) the Paine and Oppe method8.
INFANIB is an instrument to assess theneurological integrity of infants and used infollow-up programs. The assessment ispractical because it can be completed by theclinicians within several minutes.4,8 In viewof tone abnormalities detected in earlyinfancy may resolve at the end of the firstyear of life,9,10 the standard scoring sheet ofINFANIB, which allows clinicians andphysical therapists to evaluate the infant’stone and posture in a quantified manner11
give a more accurate diagnosis when thechild is being followed-up in the future.
INFANIB was constructed based onpracticality and psychometric principles,but reliability is the major concern in viewof the variation in the force that theexaminer applies to the limbs of the infantand variation in the measurement of angle.Occasionally, clinicians and physicaltherapists have different rating for the sameinfant in view of different interpretations ofthe results when similar methods ofexamination have been used. This is due tothe fact that clinicians examined the infantsto make a diagnosis while physical therapistidentified minor impairments for therapy.4There is scarcity of literature available onthe inter- and intra-rater reliability of theINFANIB scale in the neonates.3,4,8 Sinceearly detection of high risk infant is crucial

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 9
for further follow up in the future, neonatalgroup was chosen as the subject of interest.
MATERIALS AND METHODS
This cross sectional study included a totalof 112 term neonates (56 Normal and 56High Risk) in the state 3 (eyes open, nogross movement) and 4 (eyes open, grossmovements, no crying) of Normal NeonatalBehavioral States of Prechtl andBeintema.12 This study was conducted inthe year 2010-2012 and the full termnewborns were selected by convenientsampling as and when they are available inthe hospital. Preterm neonates wereexcluded to eliminate errors from hypotoniaof prematurity.11 Term neonates withsystemic illness and congenitalmusculoskeletal disorder were not eligible.In addition, term neonates under maternalmedication in whom alertness was affectedwere excluded.13 High risk term neonateswere those neonates with risk factorsassociated with neurodevelopmental delay.The risk factors included low birth weight,perinatal asphyxia, low Apgar score,neonatal hypoglycemia, neonatal seizures,type II pneumonia, and pregnancycomplications.3,12,14,15
Approval from Institutional EthicalCommittee and permission from theMedical Superintendent of the GovernmentHospital were obtained prior tocommencement of the study. Informedsigned consents were taken from theparents. The demographic data werecompleted using the medical records. TheINFANIB was administered on theneonates by Rater one, an Intern of MBBSwho was new to INFANIB and studied themethod of assessment by reading theINFANIB manual written by Patricia H.Ellison, M.D. and via severaldemonstrations by the experiencedphysiotherapist. During each assessment, avideo recording was taken simultaneously.
The videos were being anonymized to blindthe raters from the groups from which theneonates belonged. The videos were viewedby two other independent raters they arerater two and rater three for the purpose ofassessing inter rater reliability of the scale.
Rater two was a postgraduate from thePhysiotherapy Department who wasinexperienced in the use of INFANIB scaleand Rater three was an experiencedphysiotherapist in pediatrics and wasskilled in neurological evaluation of infantsusing INFANIB scale. Rater three hadevaluated the score twice for the purpose ofintra-rater reliability. All the raters wereblinded to the scoring of one another toavoid bias.
Instrument14 out of 20 items in the INFANIB scalewere applied to the neonates. Each itemwas scored as 1, 3 or 5 points. The cutoffpoints for neonatal category was as follows:abnormal ≤ 48, transient = 49-65, normal≥66.8,11
Statistical analysis: Statistical analyseswere performed using SPSS version 11.5.0.Gestational age of the neonates, postnatalday on which they assessed and birthweight was analyzed by using descriptivestatistics. Two-way mixed, absoluteagreement and single measure ICC werecalculated for intra-rater reliability as wellas inter-rater reliability.
RESULTS
A total of 112 term neonates consisting of56 normal (25 males and 31females)neonates and 56 high risk (31 males and 25females) neonates was assessed by threeraters in this study. Rater three employedINFANIB scale to all the neonates and 50videos were randomly selected (23 normaland 27 high risk neonates) for reassessmentafter one month to assess intra-raterreliability.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 10
Perinatal characteristicsThe mean (SD) gestational ages of neonatesin normal and high risk group were 39.1(1.1) weeks and 38.9 (1.1) weeksrespectively. The median and quartiles fora post natal day on which they were beingevaluated were 4 (2 to 5) days and 4 (2.3 to7) days respectively. The mean (SD) birthweight of normal neonates was 2.9 (0.3)kilograms and for high risk group was 2.7(0.6) kilograms. Risk factors included inthis study were prenatal history of two ormore abortion, pre-eclampsia, maternalillness, gestational diabetes mellitus,oligo/polyhydramnios, natal history ofmeconium stained amniotic fluid,prolonged rupture of membranes,prolonged labor, cephalopelvicdisproportion and post natal history ofresuscitation, low Apgar scores (<3 at 1minute),12 low birth weight (birth weight<2500g),7 neonatal sepsis and pathologicalneonatal hyperbilirubinemia.
Reliability Group ICC 95% CIIntra-rater(Rater three)
Normal(n=23)
0.42 0.05-0.7
High risk(n=27)
0.33 0-0.63
Inter-rater(Rater one-Rater two -Rater three)
Normal(n=56)
0.1 0-0.26
High risk(n=56)
0.28 0.05-0.5
Reliability of INFANIBIntra-rater agreement the ICC was 0.42(0.05-0.7) for normal neonates and 0.33 (0-0.63) for high risk neonates. Inter-rateragreement the ICC was 0.1 (0-0.26) fornormal neonates and 0.28 (0.05-0.5) forhigh risk neonates. The intraclasscorrelation coefficient for the intra-rateragreement of the Rater 3 and inter-rateragreement are shown in Table-1.
DISCUSSION
During the construction of INFANIB,Ellison et al had done three hundred andsixty-five assessments among infants
between 3 and 22 months old. The studyconcluded that the internal consistency ofthis scale was 0.91 for all subjects. Forinfants aged less than 7 months, the internalconsistency of INFANIB scale was 0.88and for infants aged 8 months or more itwas 0.93.8
According to Soleimani et al, the reliabilitystudy between the pediatrician andoccupational therapists was conductedamong 6150 infants aged from 4 to 18months. The intraclass correlationcoefficient was 0.90.7
In the current study, the intra- and inter-rater reliability of INFANIB was pooramong the raters in both groups ofneonates. The raters in this study havedifferent level of experience in the use ofINFANIB. The purpose of this study was tofind out if there was good inter-rateragreement among different professionalsand health workers so that it could be usedmore widely. Hence, a pilot study forinterpretation of the finding for each item inINFANIB was not done for Rater one byskilled professionals in order to find outwhether it could be used widely by thehealth workers in the peripheral area as ascreening tool without formal trainingbeforehand.
Only term neonates in the state 3 and 4 ofNormal Neonatal Behavioural States ofPrechtl and Beintema12 were included inthis study due to the fact that the tone ofneonates changes according to the neonatalstate which would misguide the raters toevaluate hypertonia if they were in statefive and hypotonia if they were in state oneand two. Furthermore, term neonatesusually sleep 50 minutes out of each hourof the day12 and this prevented each rater toassess the neonates individually. Hence theuse of video capture was chosen. Intra- andinter-rater disagreement between the raterswas not due to the variation of tone in theneonates since they rated the individual

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 11
neonate from the same video. In addition,use of video capture for the study wasdecided from the ethical point of view sincerepeated handling by different raters wouldcarry the risk of infection to the susceptibleneonates and there was a need for neonatesbeing by their mothers’ side for warmth andbreastfeeding. Therefore, the poor intra-and inter-rater agreement was purelyaffected by the interpretation of findings bythe raters.
The lack of pictorial representation in item“hands closed/open” in the INFANIBscoring sheet made it difficult for theinexperienced professional in making thedecision of the findings. Most of theneonates had their hands partially closedand the only options available were“Closed” and “Sometimes closed”. Theexperienced professional agreed on“Sometimes closed” (score 3) while thenew user of INFANIB interpreted it as“Closed” (score 5).
Interpretation of items in the French anglemethod11 such as scarf sign, heel to ear,popliteal angle, leg abduction anddorsiflexion of foot was very subjective.The raters analyzed their observationaccording to their imaginary protractors.Although it may not be feasible, the use oflarge protractor or goniometer in theclinical setting may improve the intra- andinter-rater reliability since it is moreobjective.16 The evaluation of the aboveitems also required the examiner to feel theresistance during the movement which wascrucial in judging the range of angles.However, it was not possible for each of theraters to assess each neonate in view ofethical issue and the risk of infection to theneonates.
In items “tonic labyrinthine-supine andprone”11, there was a need to observe theshoulders, trunk and legs simultaneouslywhich would have been difficult for the lessexperienced raters. They could have missed
the findings which led to poor inter-rateragreement.
For the item “weight bearing”, the new usercould not detect the difference between “Noweight bearing”11 (score 5) and “Poorweight bearing, breaks at knees”11 (score3). This was because the neonates couldhardly stand for a few seconds beforebending their knees in the latter. It wasthose few seconds which differentiatedwhether the neonates would be scored as“3” or “5”.
Manual review of data for individual itemsof all the raters revealed maximumagreement in item “pull to sitting”11 andgood agreement in items “sittingposition”11 and “asymmetric tonic neckreflex”(ATNR). This could be due to theclear pictorial representation of findings initems “pull to sitting” and “sitting position”in the INFANIB scoring sheet thatsimplified the interpretation of findingsamong the raters. Meanwhile, item“ATNR” was a primitive reflex with clearcut findings which could be easilyidentified by the raters. It could only be“persistent”, “transitional” or “absence” ofposturing.
In the item “lifts head”11, there wereseveral neonates who did not raise theirheads but there were no results for “no headlifting” in the scoring sheet. In this study,we synchronize it as “3 scores” for thisfinding.
The poor inter-rater reliability found in thisstudy could also be explained by the factthat INFANIB was designed for theprofessionals including the pediatriciansand physical therapists. On top of that, lackof formal training beforehand made the lessexperienced raters unable to interpret thefindings confidently. Even though therecent study on the Chinese version ofINFANIB have excellent reliability for 3, 7and 10 months old infants but reliability in

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 12
neonates is still needs to be exploredfurther.17
The use of video limited the raters fromjudging the force exerted by the neonates initem “foot grasp” as well as items of“French angles method”. This contributedto the poor intra-rater reliability in theinterpretation of findings by theexperienced rater. Due to convenientsampling, results may not be generalizedand the present study was limited in thenumber of neonates aged more than 7 days.There were only 7 and 9 neonates in normaland high risk groups respectively who wereaged from 8 to 21 days post natally. Futurestudies should fill in the gap of day 8 to 28in neonatal groups. In addition, the inter-rater reliability between the experiencedraters can also be carried out in the future.
In conclusion, the intra- and inter-raterreliability are poor among the normal andhigh risk term neonates. However,INFANIB is potentially suitable and easytool to screen for early neurodevelopmentaldelay among the term neonates because itcan be completed in 5 to 10 minutes.Therefore, formal training should beorganized for any professions or healthworkers who are planning to utilizeINFANIB in their working set up toimprove the inter-rater agreement.
ACKNOWLEDGEMENTAll the authors thank Miss Anupama Bajaj,postgraduate in physiotherapy for herparticipation in video rating. We aregrateful to Dr Shetty Subhodh, Dr SarfarazNawas, nursing faculty in the GovernmentHospital and colleagues in theirparticipation during the data collection. Wealso thank Dr. B. Unnikrishnan and Mr.Shashidhar Kotian for their cooperation andguidance.
REFERENCES
1. Rennie JM. Roberton’s Textbook ofNeonatology. 4th Ed. Edinburgh(UK):
Elsevier Churchill Livingstone; 2005. p.1093-105.
2. Poon JK, Rosa ACL, Pai GS.Developmental Delay: TimelyIdentification and Assessment. Indian Paed2010;47:415-22.
3. Soleimani F, Vameghi RV, Hemmati S,Roghani RS. Perinatal and Neonatal RiskFactors for Neurodevelopmental Outcomein Infants in Karaj. Arch Iran MED2009;12 (2): 135-9.
4. Ellison PH. The INFANIB, A ReliableMethod for the Neuromotor Assessment ofInfants . Therapy Skill Builder, Tucson,AZ, USA. 1994
5. Wilhelm IJ. Physical therapy assessment inearly infancy. Churchill Livingstone, NewYork, USA. 1993: 46-8.
6. Lissauer T, Clayden G. IllustratedTextbook of Paediatrics. 3rd Ed. Edinburgh(UK): Mosby Elsevier; 2007. p. 23-38.
7. Soleimani F, Dadkhah A. Validity andreliability of Infant NeurologicalInternational Battery for detection of grossmotor developmental delay in Iran. ChildCare Health Dev 2007;33:262-5.
8. Ellison PW, Horn JL, Browning CA.Construction of an Infant NeurologicalInternational Battery (INFANIB) for theassessment of neurological integrity ininfancy. Phys Therapy 1985;65:1326-31.
9. Amiel-Tison C, Grenier A. Neurologicalassessment during the first year of life.Oxford University Press, New York, USA.1986.
10. Chaudhari S, Bhalerao M, Chitale A, et al.Transient tone abnormalities in “high risk”infants and cognitive outcome at five years.Indian Pediatr 2010;47:931-5.
11. Ellison PW. Scoring Sheet for the InfantNeurological International Battery(INFANIB). Phys Ther 1986;66:548-50.
12. McIntosh N, Helms PJ, Smyth RL, LoganS. Forfar & Arneil’s Textbook ofPediatrics. 7th Ed. Edinburgh: ChurchillLivingstone Elsevier; 2008. p. 297-301.
13. Van Baar AL, Fleury P, Soepatmi S, et al.Neonatal behavior after drug dependentpregnancy. Arch Dis Child 1989;64:235-40.
14. Reddihough DS and Collins KJ. Theepidemiology and causes of cerebral palsy.Aust J Physiother 2003;49:7-12.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reliability of INFANIB, MY Wong et al. 13
15. Elenjickal MG, Thomas K, Sushamabai S,Ahamed SKZ. Development of high-risknewborns-A follow-up study from birth toone year. Indian Pediatr. 2009;46:342-5.
16. Chaudhari S, Deo B. Neurodevelopmentalassessment in the first year with emphasison evolution of tone. Indian Pediatr2006;43:527-34.
17. Liao W, Wen EY, Li C, Chang Q, Lv KLand Yang W etal. Predictingneurodevelopmental outcomes for at-riskinfants: reliability and predictive validityusing a Chinese version of the INFANIB at3, 7 and 10 months. BMC Pediatr. 2012;12:72. doi: 10.1186/1471-2431-12-7.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 14
KNOWLEDGE AND ATTITUDES OF THE PUBLIC, PRIMARYHEALTH CARE PHYSICIANS AND OTHER HEALTH
PROFESSIONALS, AND POLICY MAKERS TOWARDSRELIGIOUS MEDICAL PRACTICES
Abdulla M AlBedah1, *Asim A Hussein2, Ahmed T ElOlemy3, Mohamed Khalil4,Ibrahim AlSubai5
ABSTRACTBackground: Religious care and support are vital for a holistic patient care. Thephenomenon has widely spread in Muslim countries and in the west as well. WHO isshowing marked concern and in our Arabic and Islamic region there is a growing concerntowards traditional Arabic and Islamic medicine. Objectives: 1. To explore knowledge andattitudes of the public, primary health care physicians and other health professionals, andpolicy makers towards religious and spiritual medical practices; 2. To describe the religiousand spiritual Islamic medical practices content of Arabic speaking Satellite TV channels.Subjects and Methods: The National Center for Complementary and Alternative Medicinein Saudi Arabia has conducted four cross-sectional surveys within the last four years from2009 to 2012, plus a media analysis survey on religious and spiritual medicine on Arabicspeaking Satellite TV channels. Studies targeted policy makers of Ministry of Health (112participated), health professionals (306 participated), primary health care physicians (113participated), and the public (518 participated). Also, topics and programs of religioushealing practices on the Arabic Satellite TV channels. Data were collected through pre-designed questionnaires some self-administered and some filled through direct interviews. Inthe media study a comprehensive survey was performed for two weeks covering all Arabicspeaking Satellite TV channels. Findings were statically presented and analyzed using SPSSstatistical package for windows. Results: Religious healing utilization reported high ratesreaching 70% in some studies, especially among females, older ages and low educationalgroups, and in particular for chronic and malignant diseases. Media survey on Arab TVchannels revealed religious programs and topics to be the most prominent and morefrequently repeated compared to other practices of complementary and alternative medicine.Conclusion: There is a health professional and community interest on religious therapies.There is a highlighted need for provision of authenticated information about CAM andreligious healing practices to the public and to health professional, provision of educationaland training programs for doctors and health care providers, for regulating those practicesagainst quackery and sorcery.
الدول الغربیة وتعتبر الممارسات الدینیة من أھم ممارسات الطب البدیل والتكمیلي انتشاراً في الدول اإلسالمیة خلفیة:ا بالطب الشعبي والطب البدیل والتكمیلي بما فیھعلى حدً سواء. ً ا واضح ا منطقتنا وقد بدأت منظمة الصحة العالمیة اھتمامً
. معرفة واتجاه ١: اھداف البحثالعربیة واإلسالمیة حیث یتوجھ االھتمام والطلب على الممارسات الدینیة والروحیة. في الممارسات الدینیة أفراد المجتمع وأطباء الرعایة الصحیة األولیة والعاملین بالقطاع الصحي ومتخذي القرار تجاه
Received: 19 March, 2013; Accepted: 9 June, 2013
*Correspondence: [email protected] Director. National Center for Complementary & Alternative Medicine, Kingdom of Saudi Arabia;2Associate Professor & Consultant Community Medicine, National Center for Complementary & AlternativeMedicine, Kingdom of Saudi Arabia; 3Professor of Public Health and Community Medicine, Faculty ofMedicine, Tanta University, Egypt, & Consultant, National Center for Complementary & Alternative Medicine,Kingdom of Saudi Arabia; 4Consultant Community Medicine. National Center for Complementary & AlternativeMedicine, Kingdom of Saudi Arabia; 5Assistant Professor & Consultant Community Medicine National Centerfor Complementary & Alternative Medicine, Kingdom of Saudi Arabia

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 15
القنوات القضائیة العربیة حیال الطب البدیل والتكمیلي وما تتضمنھ من برامج وموضوعات . توجھات٢المملكة السعودیة. : أجرى المركز الوطني للطب البدیل والتكمیلي على مدى منھجیة وطرق البحثخاصة بالممارسات الدینیة والروحیة.
–٢٠٠٩ھجریة / ١٤٣٣-١٤٣٠أربع سنوات عدد من الدراسات منھا أربعة دراسات مسحیة مقطعیة خالل الفترة م، إضافة إلى دراسحة مسحیة على مستوي القنوات الفضائیة العربیة لدراسة ظاھرة انتشار ممارسات الطب ٢٠١٢
ا والممارسات الدینیة على وجھ الخصوص، والعوامل المرتبطة بھا. شارك في الدراسات من أفراد البدیل والتكمیلي عمومً) ومتخذي القرار ٣٠٦) ومن العاملین بالقطاع الصحي (١١١٣الرعایة الصحیة األولیة () ومن أطباء٥١٨المجتمع (
)، وكذلك برامج وموضوعات الطب البدیل والتكمیلى في القنوات الفضائیة العربیة. تم ١١٢بالمملكة العربیة السعودیة (تمادھا عالمیاً لمثل ھذا النوع من جمع البیانات عن طریق استمارات استبیان مختبرة ومعدة مسبقًا ومنظمة تم اع
الممارسات الدینیة وعلى رأسھا الرقیة الشرعیة والذكر الدراسات، احتوت على المعرفة واتجاه ورؤیة المشاركین حول زمزم. تم استعراض النتائج وتحلیلھا احصائیا باستخدام برنامج ماء والمقروء علیھالماءوالصالة والدعاء واستخدام
بلغت نسبة استخدام المعالجات الدینیة والروحیة معدالت عالیة وصلت ألكثر من النتائج: .SPSSحصائي التحلیل اإلفي بعض الدراسات. أظھرت الدراسات أن معدل االستخدام كان أكثر بین اإلناث والفئات من عینات المستطلعین%٧٠
أظھر مسح القنوات األورام السرطانیة.المزمنة ومراض السنیة األعلى والفئات ذات المستویات التعلیمیة األقل وخاصة لألا في ھذه القنوات. ً الخالصة العربیة أن البرامج والموضوعات المتعلقة باالستشفاء الدیني كانت األبرز واألكثر تكرار
اأوصت الدراسات بالحاجة إلى المزید من المعرفة الموثقة والتوصیة: للحاجة لعقد للجمھور وللعاملین الصحیین، وأیضً، كما أوصت لمثل ھذه الممارساتالتي تقدم لألطباء ولكافة مقدمي الرعایة الصحیة لیة یالتأھالتعریفیة وت التدریبیة رادوال
ھا.بما یضمن بُعدھا عن ممارسات الدجل والشعوذة والتي قد تصاحبھذه المعالجات وتنظیمدعمبأھمیة
INTRODUCTION
Religious and spiritual care is a vital part ofholistic patient care. Awareness of commonpatient beliefs will facilitate discussionsabout religion and spirituality. Suchconversations are inherently good for thepatient, deepen the caring staff-patient-family relationship, and enhanceunderstanding of how beliefs influence caredecisions. This is especially clear in an areasuch as the Middle East, where religiousbeliefs are strong and widespread.1
According to the Islamic faith, sufferingplays an important role in life. For theMuslim, sickness and suffering are a part oflife, spiritual test from the AlmightyCreator. Emotional and physical sufferingcaused by illness is regarded as a test offaith in God, Allah, expunging the sins ofthe Muslim.2 Despite the fact that religionis important for a majority of our patients,yet that need is not supported by themedical team most of the time. As physicalhealth wanes, religion and spiritual healthmay increasingly play a central role indetermining patient well-being.3
It's to be assumed that this unmet need bymodern medicine practitioners is one of theimportant factors why more patients nowseek alternative healing options.
The National Center for Complementaryand Alternative Medicine is a newlyestablished official reference center forcomplementary and alternative medicine inthe Kingdom of Saudi Arabia. From theperiod from 2009 to 2012, the center hasconducted four cross-sectional surveys,plus a media analysis survey on Arabicspeaking Satellite TV channels on religioushealing practices. Those studies targetedpolicy makers of Ministry of Health, healthprofessionals, primary health carephysicians, and the public. A briefing ofthose study surveys are presented in thispaper, though they were targeting CAM ingeneral, our focus would be towardspractices related to religious and spiritualhealings.
The National Center for Complementaryand Alternative Medicines Studies onReligious Healing: A Brief Description:

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 16
1. Perception of Health Professionals andPolicy Makers about Complementaryand Alternative Medicine in SaudiArabia: September through December2009.
Aim: To determine perception and attitudestowards CAM among health professionals
and policy makers.
Subjects and Method: Healthprofessionals and policy makers working inthe Ministry of Health and National Guard,deans, vice deans and heads departments infaculties of health and medicine, pharmacy,dentistry, were all targeted. 700 self-administered questionnaires weredistributed manually, mailed or posted viaexpress mail services. 112 were returnedwith response rate of 16%. Data wasanalyzed using SPSS Statistical Packageversion 16.
Results: Most common traditional practicesreported were honey and bee products88.6%, Roquia (spiritual healing) 87.6%,medical herbs 81.4%, Hijama 63.7%, bodymassage 60.1%, and nutritionalsupplements 57.5%. These practices werepositively perceived by most in view ofsafety and effectiveness [Table 1].Quackery was the most feared threat by82.3%. Reasons reported for use includedsocial and inherited habits (85.9%), poorresponse to conventional treatment (83.1%)and poor physician patient communication(79.6%), and religious beliefs (78.7%)
2. Knowledge and Attitude of HealthProfessionals in Riyadh Region, SaudiArabia, towards Complementary andAlternative Medicine.
Aim: To identify knowledge and attitude ofhealth professionals in Riyadh regiontowards CAM.Subjects and Methods: Through a cross-sectional survey and multistage randomsample selection, a total number of 306
health professionals (physicians, other non-physician specialists, technicians) workingin 19 hospitals in Riyadh city andsurrounding governorates participated. Datacollected through a self-administeredquestionnaire.Results: 88.9% had some knowledge aboutreligious healing/CAM. Source ofinformation was mass media (60.1%),followed by family, relatives and friends(29.08%), and educational institutions(14.71%). Most common practicespositively perceived by participants were:prayer (spiritual healing) 90.5%, honey andbee products 85%, medical herbs 76.9%,Hijama 70.6%, medical massage 61.8%,nutrition and nutritional supplements61.4%, cauterization 55.9%, acupuncture55%, and camel milk and urine 52.5% [Fig.1].
3. Public Knowledge, Attitude andPractice about Complementary andAlternative Medicine in Riyadh Region,Saudi Arabia:
Aim: To identify knowledge, attitude andpractice of people in Riyadh region, aboutCAM.Subjects and Methods: A total number of518 individuals from the public in Riyadhcity and surrounding governorates weresurveyed and selected by a multistagerandom sample technique and a cross-sectional study design. Data were collectedthrough direct face-to-face interviews usingpre-designed questionnaires.Results: Saudis represented 70% of thesample and 30% non-Saudi nationalities.Religious therapies represented the mostused practices: medical herbs (58.89%),prayer (54%), honey and bee products(54%), hijama (35.71%), cauterization ormedical massage therapy (22%) [Fig. 2].Main users were: females, housewives,illiterate or just read and write individuals,and those aged 60 years and more. Massmedia e.g. (T.V., newspapers and radio)and family, relatives and friends

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 17
represented the main sources of knowledge(46.5% and 46.3%) respectively.
4. Knowledge and Attitude of PrimaryHealth Care (PHC) Physicians towardsComplementary and AlternativeMedicine in Riyadh Region, SaudiArabia
Aim: To assess PHC physicians'knowledge, attitude and believes regardingCAM and to identify factors that mightinfluence them.Subjects and methods: All physiciansworking in primary health care centers inRiyadh region affiliated by MOH andMinistry of Defence were studied through across-sectional survey. A total number of1113 physicians responded and answeredthe self-administration questionnaire; fortyfour physicians were excluded from thestudy due to incomplete answering of thequestionnaire. Data were collected througha self-administrative pretestedquestionnaire modified after adaptationfrom Dietlind L.4Results: Physicians were significantlyusing CAM and religious therapies forthemselves or their families (51.7%), withfemale physicians more than males(56.58% versus 49.53%). Of a long list ofCAM practices provided in thequestionnaire, physicians were significantlymore familiar and somewhat comfortablewith religious therapies than other non-religious ones: Roquia on top (51.8%)followed by honey and bee products(48.9%), dietary supplements (47.1%),medical herbs (40.8%), cupping (39.5%),and cauterization (32.7%) [Table 4]. Themajority of studied physicians (85.1%)agreed on the need for acquisition of goodknowledge about religious and othercommonly used CAM therapies in theregion. 67.4% of studied physiciansbelieved that patient's religious beliefs andpractices were important for healing, and61% of them believed that physicians'
religious beliefs and practices wereimportant for healing patients by 61%.
5. A Survey on CAM Programs at ArabSatellite TV Channels and Topics 18th to28th Oct 2010.
Aim: To identify CAM specialized,religious and other TV channels, CAMprograms and topics, and to clarify natureof those programs.Study Methods: All Arab TV channelsspecialized in or have programs aboutCAM been included namely: Arab Sat, NileSat, Hot Bird. All religious TV channelswhich present CAM programs weresurveyed. All programs about Propheticmedicine, Roqia, bee products and beehoney, medical herbs, Arabic medicine,Chinese medicine, were surveyed.Qualified media bachelor and masterholders personnel were trained for themission of observing Arab Satellite and TVchannels all round 24 hours day and night.Content analysis study design was adoptedfor analyzing CAM programs and topics.Survey started on the 10th of Dual Qaida1431 H (18th to 28th Oct 2010), andcontinued for two weeks. Twoquestionnaires were developed: TVchannels survey questionnaire, and CAMprograms analysis questionnaire. Datawere analyzed by SPSS version 18,descriptive statistical methods; Chi-squaretest and P-value 5% were employed.Results: 119 channels presented in one wayor another CAM topics. 1151 CAMprograms/topics repeatedly appeared withinthe two weeks study. Herbal medicineprograms were on top (23%), followed byProphetic medicine and religious Roqia(18.5%), then aromatherapy (15%), thendietary therapy (11.5%), then Bee honeyprograms (10.3%) and bee products(10.3%), and then rest of CAM practices.11 CAM topics were presented, somefrequently, some occasionally.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 18
Table (1): Religious therapies top the list of CAM practices used in Saudi Arabia from HealthProfessional and Policy Makers Perspective in Saudi Arabia
Common CAM practices Usually(>50%)
Sometimes(10-50%)
Total use Rarely(<10%)
Never(0%)
Totalnon-use Z p
1. Honey and bee products 45.2 43.4 88.6 4.4 7 11.4 8.03 0.000*
2. Roqia (spiritual healing) 71.7 15.9 87.6 2.7 9.7 12.4 7.84 0.000*
3. Medical herbs 29.2 52.2 81.4 9.7 8.9 18.6 6.52 0.000*
4. Hijama 17.7 46 63.7 27.4 8.9 36.3 2.74 0.003*
5. Body massage 21.2 38.9 60.1 28.3 11.6 39.9 1.98 0.02
6. Nutritional supplements 23 34.5 57.5 30.1 12.4 42.5 1.42 0.07
7. Aromatherapy 11.5 28.3 39.8 39.8 20.4 60.2 1.23 0.11
* Significant at level of 0.05
Figure (1) Religious practices are the most likely used CAM practices as to Healthprofessionals in Riyadh Region
Figure (2): Attitudes of the Public in Riyadh Region towards CAM: Religious practicesmostly used.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 19
Herbal medicine appeared most (31.37%),then Prophetic medicine & Roqia (18.43%),then dietary therapies (15.69%), thenaromatherapy (14.51%), then bee honeyand bee products (12.6%), while theremaining six only appeared so limited.
Table (4) Distribution of studied populationand familiarity with religious healingpractices
Religious healingpractices
Understand it and feelsomewhat comfortable about
counselling patients % among1113 studied physicians
Roquia (Spiritual
healing)
51.8%
Honey and bee
products
48.9%
Dietary
supplement
47.1%
Medical herbs 40.8%
Hijama-Cupping 39.5%
Cauterization 32.7%
DISCUSSION
As to WHO, an estimated 80% of thepopulation in the developing world relieson traditional systems of medicine, and 70-80% of the population in developedcountries have used some form ofalternative or complementary medicine.5Herbal treatments are the most commonlyutilized form of traditional medicine, andare lucrative in the internationalmarketplace yielding $5 billion US inrevenues in Western Europe, $14 billionUS in China and $160 million US inBrazil.5 Existing data, however, sparse asthey are, reveal that the frequency of use ofa spiritual healing or reliance on the prayersof others may exceed almost every otherCAM therapy.6 This finding has beenvalidated across racial and ethnic groups inthe U.S.7 The World Health Organizationdefines traditional medicine as “the sumtotal of knowledge, skills and practicesbased on the theories, beliefs andexperiences indigenous to different cultures
that are used to maintain health, as well asto prevent, diagnose, improve or treatphysical and mental illnesses”.5 Twoexamples are widely known traditionalsystems of medicine, namely TraditionalChinese Medicine (TCM) and Ayurvedicmedicine,8 however, ArabicIslamic/Prophetic traditional system ofmedicine is another vibrant and expansivesystem of healing traditions thriving andpervading modern life in the Arab andMuslim world,8 that need to be highlightedinternationally. In Saudi Arabia, CAMtherapies are attracting attention of all, thepublic, media, medical community andgovernmental agencies. A 2008 nationalsurvey on prevalence, costs, and patterns ofuse of alternative and complementarymedicine clearly demonstrated theextensive use of traditional Arabic andIslamic healing practices. Qur’anic healing,honey use and black seeds were the mostfrequent practices.9 Idioms used to connotesuch Islamic and Arab healing traditions,and which are sometimes usedinterchangeably, include Graeco-Arabic orUnani medicine, Islamic Medicine, andProphetic Medicine or Tibb Nabawi(medicine of the Prophet).8 Despite anextant, though finite, literature on thevarious practices of these healing traditions,no clear and concise model exists todistinguish and organize their multiple,intertwined elements.8 In the kingdom ofSaudi Arabia, the national center foralternative and complementary medicine isa newly established official reference foreverything concerning CAM practices.Though having a multitude of tasks,research studies and surveys to analysis thesituation in the kingdom are some of itsimportant tasks. Many surveys have beenconducted during this mean time todescribe people's traditional medicinepractices outside the official modernmedicine domain, their attitudes and theirknowledge. Results of surveys to daterevealed vividly an increased interest,knowledge and a positive attitude and

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 20
perception towards religious healingtherapies compared to other CAMtherapies, among studied subjects, whetherphysicians, health professionals, policymakers, or the public. Roquia (healingthrough reciting on patients specificQur'anic verses or Prophetic supplications),prayers, honey and bee products, medicalherbs, Hijama (cupping), nutritionalsupplements, were the most frequentlyused, understood and felt comfortable aboutof all CAM practices. They were as well ontop of CAM programs and topics in ArabSatellite TV Channels. Studies includedcommunity members, primary health carephysicians, health professionals and policymakers, and also what's happening in themedia. Conceptually, Islamic religious andArab traditional healing practices arelacking a scientific working definition aswell a conceptual model of representation.A few of such propositions and innovationshave now started to show on the scene.Azaizeh et al. recently proposed the termTraditional Arabic & Islamic Medicine,given it "TAIM".10 Conceptually, thoughneither a definition nor a conceptual modelwas proposed, this encompassing termrecognizes traditional Arabic and Islamicmedicine as one system to embrace theentirety of the historical roots and breadthof practices, and represents an innovativestep forward. Al-Rawi S & Fetters, gave apush forward to advance clinical andacademic applications of this healingtradition, proposing a working definition ofTAIM, and presenting a conceptualframework to delineate its scope.10 Theyhave weaved on the same patterns andtaxonomy of the already formalizedtheoretical frameworks of traditionalhealing systems, such as traditional Chinesemedicine (TCM) and Ayurveda, as well asComplementary and Alternative Medicine(CAM) in developed countries,11 whichincorporate manipulative and massagetechniques, herbal medicine, dietarypractices, meditation, and exercise.12 Auseful structure for characterizing TAIM
and organizing its elements was thenpresented. Al-Rawi & Fetters have definedTraditional Arabic and Islamic Medicine as"a system of healing practiced sinceantiquity in the Arab world within thecontext of religious influences of Islam andto be comprised of medicinal herbs (e.g.black seed), dietary practices (e.g. beeshoney, Zamzam water, observing a fast),mind-body practices (e.g. Islamic ritualprayer, Dhikr) spiritual healing (e.g.Quranic healing, recitations, devotions,supplications, Rugia) and applied therapy(e.g. cupping-hijama, hydrotherapy,massage), and whereby many of theseelements reflect an enduringinterconnectivity between Islamic medicaland prophetic influences as well as regionalhealing practices emerging from specificgeographical and cultural origins.9 From theresults of our study surveys, we canconclude that TAIM practices, if we canborrow that recent definition, are on top ofCAM practices that attracting the interest inthe Kingdom, and they are as well fittinginto that newly proposed conceptual modelof medicinal herbs, dietary practices, mind-body practices, spiritual healing, andapplied therapy.
The studies have generally came out withsome important recommendations tomention: need for further CAM's situationsurveys, strict regulation, blockadingsorcery and quackery, education andprovision of evidence-based information tothe public and professionals, andintegration of CAM in medical and healtheducation curricula and in the health caresystem.
REFERENCES
1. Puchalski C, Ferrell B, Virani R et al.Improving the quality of spiritual care as adimension of palliative care: the report ofthe consensus conference. Journal ofPalliative Medicine 2009; 12 (10): 885–904.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Knowledge & Attitudes towards Religious Medical Practices, Abdulla M AlBedah et al. 21
2. Hedayat K. When the spirit leaves:childhood death, grieving, and bereavementin Islam. Journal of Palliative Medicine2006; 9 (6): 1282-1291.
3. Balboni TA., Vanderwerker LC., BlockSD. et al., “Religiousness and spiritualsupport among .advanced cancer patientsand associations with end-of-life treatmentpreferences and quality of life. Journal ofClinical Oncology 2007; 25 (5): 555–560.
4. Dietlind L. Wahner-Roedler, Ann Vincent,Peter L. Elkin, Laura L. Loehrer, StephenS. Cha and Brent A. Bauer. Physicians'Attitudes towards Complementary andAlternative Medicine and Their Knowledgeof Specific Therapies: A Survey at anAcademic Medical Center. Evid BasedComplement Alternat Med. June2006;3(4):495-501.
5. WHO. Traditional Medicine. 2008, 2011,Retrieved March 13, 2010, fromhttp://www.who.int/mediacentre/factsheets/fs134/en/index.html
6. Cheung CK, Wyman JF, Halcon LL. Use ofcomplementary and alternative therapies incommunity-dwelling older adults. J AlternComplement Med 2007; 13: 99.
7. Graham RE, Ahn AC, Davis RB, O'ConnorBB, Eisenberg DM, Phillips RS. Use ofcomplementary and alternative medicaltherapies among racial and ethnic minorityadults: Results from the 2002 NationalHealth Interview Survey. J Natl Med Assoc2005; 97: 535–545.
8. Al-Rawi S & Fetters MD. TraditionalArabic & Islamic Medicine: A ConceptualModel for Clinicians and Researchers.Global Journal of Health Science 2012: 4(3): 164-69.
9. Al-Faris EA, Al-Rowais NA, Ashry GM,Al-Rukban MO, AlKurdi A, Al-Noor MA,Al-Harby S, and Sheikh A. Prevalence andpattern of alternative medicine use: theresults of a household survey. Ann SaudiMed 2008; 28,1(1): 4-10.
10. Azaizeh, H., Saad, B., Cooper, E., & Said,O. Traditional Arabic and IslamicMedicine, a Re-emerging Health Aid. EvidBased Complement Alternat Med 2010;7(4): 1-6.
11. NCCAM. What is Complementary andAlternative Medicine 2008. RetrievedFebruary 14, 2012, fromhttp://nccam.nih.gov/health/whatiscam
12. Nestler, G. Traditional Chinese medicine.Medical Clinics of North America 2002;86(1), 63-73.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 22
EVALUATION OF HEPATITIS B CORE ANTIBODY (TOTAL) INTHE PRESENCE OF ID-NAT*Ranjay K Choudhary1, Moattar R Rizvi2
ABSTRACTBackground & Aim: The testing for HBcAb is done by different blood centres to ensure theblood safety for transfusion. However, In India, HBcAb is not compulsory test as per Drugsand Cosmetics Act, 1940. Introduction of ID-NAT (Nucleic Acid Testing) for detection ofHBV DNA have proven to be of great success but on the contrary increase the cost of bloodtransfusion. Therefore, the present study was undertaken to find the possibility of obviatingthe need of screening of HBcAb with existing ID-NAT, so as to optimize the resourceutilization. Materials & Methods: Donor blood samples between October 2008 and April2010 covering 8221 samples were collected and tested simultaneously for Anti-HBc andHBsAg ELISA and ID-NAT tests. Results: Nearly 7% (581) were reactive for HBV marker.Further the samples reactive to serological markers HBsAg & HBcAb (Total), werecompared with ID-NAT. Of all the samples reactive for HBV, 7.6% was reactive by ID- NAT.About 2.07% of solitary HBcAb reactive samples were reactive by ID-NAT (Table 1).However, none of the non- reactive samples was reactive to ID-NAT. Conclusion: Still,HBcAb has a definitive role in ruling out the transmission of HBV among HBsAg non-reactive blood (2.07%; Table 1). On the contrary, not even one sample was NAT reactiveand not reactive by CLIA. Screening of blood by Anti- HBcAb didn’t enhance the bloodsafety. In addition, centers that have incorporated NAT testing may not derive any additionalbenefit as this cannot replace anti-HBc testing, especially in developing country like ours.KEY WORDS: Hepatitis core antibody, ID-NAT- Individual donor- Nucleic acid Test, HBsAg-Hepatitis B Surface Antigen, TTI- Transfusion Transmitted Infection
مراكزقبلمن(HBcAb)بنوعالكبدياللتھابفیروس النواةالمضادةاالجساماختباریتم:والھدفالخلفیة: خالصةواالدویةقانونحسبإجباریالیسالھندفي(HBcAb)اختبارفإنذلكومع. الدمنقلسالمةلضمانالمختلفةالدم
للكشف{ID-NAT (Nucleic Acid Testing)}النوويالحمضاراختبإدخالأثبت. ١٩٤٠للعامالتجمیلمستحضراتھذهأجریتلذلك. الدمنقلعملیةتكلفةمنیزیدولكنھكبیرنجاحبنوعالكبدالتھاب لفیروسالنوويالحمضعن
ID-NAT (Nucleic Acid}اختباربواسطة(HBcAb)لفحصالحاجةانتفاءاوتفاديإمكانیةالختبارالدراسةTesting)} ,٢٠٠٨أكتوبربینماالدمبلمتبرعینمن اعیناتالجمعتم: الدراسةمنھج. الموارداستخداملتحسینوذلك
فیروس لنواةالمضادةاالجسامأوال:لمعرفةواحدوقتفيواختبرتعینة٨٢٢١العیناتوبلغت٢٠١٠وأبریل( HbsAg ELISA )بنوعالكبديااللتھاب لفیروسالسطحيالمستضدثانیا:و(Anti-HBc)بنوعالكبدياللتھاباایجابیینكانوا) ٥٨١(٪٧حوالي: النتائج. {ID-NAT (Nucleic Acid Testing))}النوويالحمضاختبارثالثا:و
االجساموایضاالسطحيالمستضدلعالماتایجابیةالعیناتكانتذلكعلىوعالوة. بنوعالكبدفیروسلعالماتID-NAT (Nucleic(النوويالحمضاختبارمعجمیعامقارنتھمعند)( HBcAbو(HBsAg )المصلیةللنواةمضادةال
Acid Testing .(اختباربواسطةایجابیةنتیجةاعطي٪٧٫٦فقطالبائيالكبدالتھابلفیروساالیجابیةالعیناتكلمنكانتHBcAbلاالیجابیةالعیناتمن٪٢٫٠٧حواليو). ID-NAT (Nucleic Acid Testing(النوويالحمضایجابیةالنتیجةالسلبیةالعیناتمنأيتكنلمذلك،ومع). ID-NAT (Nucleic Acid Testing(اختباربواسطةایجابیة
ID-NAT(اختبارمع ,Nucleic Acid Testing (
Received: 12 March, 2013; Accepted: 17 June, 2013
*Correspondence: [email protected] Lecturer, College of Applied Medical Science, Department of Medical Laboratories, Majmaah University,Majmaah, Riyadh- KSA. 2Assistant Professor, College of Applied Medical Science, Department of MedicalLaboratories, Majmaah University, Majmaah, Riyadh- KSA.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 23
النتیجةالسلبيالدممنبنوعالكبدفیروسانتقالاستبعادفيحاسمدورلھHBcAb،اختباریزالال: االستنتاج.الحمضاختبارمنواحدةعینةحتىیكنلمذلك،منالعكسعلىو. HBsAg()(2.07٪(للفیروسالسطحيللمستضد
المضادةاالجسامطریقعنالدمفحص). CLIA(المناعيالتوھجفحصبواسطةكذلكتكنولمایجابیة) NAT( النوويأدرجتالتيالمراكزذلك،إلىوباإلضافة. الدمنقلسالمةیعززال) HBcAb( بنوعالفیروسيالكبديلاللتھاباةللنو
للنواةالمضادةاالجساماختبارمحلیحلأنیمكنالألنھإضافیةفائدةأيتستمدالقد) NAT( النوويالحمضاختبار.بلدنامثلالنامیةالبلدانفيوخاصة،)HBcAb( بنوعالفیروسيالكبديلاللتھاب
INTRODUCTION
Hepatitis B virus (HBV) infection is aserious global health problem which isaffecting two billion people worldwide, and350 million people suffer from chronicHBV infection. This is approximately 5% ofthe world population.1 There are over 4million new cases of acute clinical hepatitisyearly. About one million of those infecteddie annually from chronic hepatitis Binfection or one of its complications-cirrhosis and hepatocellular carcinoma.2Transmission of hepatitis through bloodtransfusion was first reported in 1943.3,4
In India, Hepatitis B virus (HBV) infectionvia blood transfusion is a serious healthproblem. After an incubation period that canrange between 50 to 180 days, this infectionhas an insidious onset. The viruses aredetectable in the blood for several monthsor even years and about 5-10% ofindividuals become chronic carriers.Chronic infection by HBV could lead to thedevelopment of cirrhosis and hepaticmalignancy.5 Screening for hepatitis Binfection by surface antigen (HBsAg)started in 1971.6 Usually testing for HBsAgis performed using EIA, radioimmunoassayor other immunological based assays. Thelatest, most sensitive HBsAg detectionmethod uses chemiluminescence and thismethod is widely used in Canada, Europe,and some parts of Asia.7 Method fordetection of HBsAg is not yet standardized.The only requirement now for HBsAgtesting is licensing or accreditation of thetest in this country became selection of thetest different in different countries.
In some tropical countries where blooddonor centres have limited resources, rapidand less expensive immuno filtration, latexbased, or immuno chromatographicmethods are used, without any confirmatorytesting techniques.8
The mandatory screening for HBsAg byELISA for over 20 years, still transfusion-associated HBV (TAHBV) continues to bea major problem in India, and more so inpatients receiving repeated bloodtransfusions.9 However, it has beenobserved that some HBsAg-negativeindividuals continue to replicate HBV.10,11
Hence, the non reactive result of HBsAg inthe blood can not reflect that the person iscompletely free from Hepatitis B Virus.Blood containing anti-HBc with or withoutdetectable presence of HBsAg might beinfectious. In 1992, antibody to the coreprotein of hepatitis B (anti HBc total) wasintroduced in the screening process as asurrogate marker for post-transfusion non Anon B hepatitis.12 With introducing of antiHBc (total) screening, a phenomenalreduction target has been achieved in thenumber of hepatitis B viral infectious unitsfrom entering the donor pool. Therefore,routine blood donor screening for anti-HBcwas implemented to reduce the risk of post-transfusion HBV infection.13 Screeningpractices of Transfusion TransmittedInfections (TTI) depends on pathogenicity,morbidity, mortality, endemicity ofpathogen. Ethics vs. financial viability haveled to varied practices across the globe.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 24
Hepatitis B core antibody screening iscontroversial in blood banks worldwide,because Hepatitis B core antigen is foundonly in liver cell and not in bloodcirculation, it is true that blood circulation isdetected mainly with anti HB core total(HBcAb IgM & IgG). Recently introducedID- NAT testing has reduced the windowperiod but does not completely eliminateHBV. Hepatitis B virus infection has aworldwide prevalence due to its infectivity,chronicity and ability to cause substantialmorbidity and mortality, in the form ofcirrhosis and Hepatocellular Carcinoma(HCC).14
However, current development of ID-NATtechnology can be proved more sensitivetesting for safe blood supply by HBVinfection, but it expensive. It can also be aneffective test to rule out occult hepatitis,HBsAg negative and anti-HBc positiveinfections with low levels of viraemia. Thecomplete elimination of traditional testingmethods in the near future is difficult.15,16,6
Screening of HBsAg and HBV DNA byNAT would appear preeminent in thecountries with a normal to high prevalenceof HBsAg. On the other hand, HBV DNAby NAT and anti-HBc testing may besuperior to HBV DNA by NAT and HBsAgtesting in countries with low prevalencerate. Pathogen inactivation will possiblyhave a role in increasing the chances of thesafety of blood products reducing the risk oftransfusion-transmitted HBV.17-19
In India, screening for HIV 1 & 2, HCV andHBsAg is mandatory by law. However, thescreening for Anti HBV core antibodiesIgM & IgG is employed by various bloodbanks to ensure the decrease of transmissionof HBV in case of HBsAg negative blood.
In Recent time, the use of nucleic acidtesting (NAT) of blood donors has beenadopted to detect the presence of occulthepatitis B virus in blood donors which is
considered a Potential risk for transfusion ofhepatitis B virus.9 Though the use of NATto prevent transfusion of hepatitis B virusmay offer a new opportunity to bloodscreening programmes, the feasibility ofimplementing it should be fully considered,since the requirements for infrastructure,financing, staffing levels, training andquality systems and the overall costs ofimplementation may far outweigh anypotential benefit in terms of increased bloodsafety. The present study was carried out tolook into the possibility of obviating theneed of screening HBV core if a facility ofNAT exists, so as to optimize the resourceutilization.
MATERIALS & METHODS
Donated blood was evaluated and collectedbetween October 2008 and April 2010covering 8221 samples. The hospital catersto patient population from different partsof country and world such as USA,Canada, Iraq, Nigeria, Oman, Kazakhstanetc. All samples were screened forserology and ID- NAT. Serologicalscreening was performed by random accessChemiluminescence Immuno Assay(CLIA) for TTI including HBsAg &HBcAb – Total (IgM & IgG), (Vitros ECI;OCD; JNJ from USA). Nucleic acidscreening (Supplementary test) Individualdonor ID-NAT was performed byTranscription Mediated Amplification(TMA) technology (Novartis Diagnosticfrom USA).
RESULTS
Of the 8221 blood donors, 581 (7%) werereactive for HBV marker. All the samplesscreened reactive by serological markers-HBsAg & HBcAb (Total), were comparedwith ID-NAT. Of all the samples reactivefor HBV, 7.6% is reactive by ID- NAT.About 2.07% of solitary HBcAb reactivesamples were positive by ID-NAT (Table 1& Figure 1). However, no non- reactive

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 25
sample was observed to be reactive by ID-NAT, over the study period.
DISCUSSION
In the present study, out of 8221, 581(7%)reactive samples for HBV marker,07(1.21%) samples were HBsAgreactive/anti HB core Total non reactive/ID-NAT non reactive, 17(2.93%) sampleswere HBsAg reactive/anti HB core Totalreactive - /ID-NAT non reactive, 13(5.34%)samples were found to be HBsAgreactive/anti-HB core total reactive/ID-NATreactive, 513(88.3%) samples were found tobe HBsAg non reactive/anti-HB core totalreactive/ID-NAT non reactive, 12(2.07%)samples were HBsAg non reactive/anti-HBcore total reactive/ID-NAT reactive, 0(0%)samples were found to be HBsAg nonreactive/anti-HB core total non reactive/ID-NAT reactive, and only 1(0.2%) sampleswere found to be HBsAg reactive/anti-HBcore total non reactive/ID-NAT reactive.The result shows that there was no samplewhich was neither ID-NAT reactive norreactive by CLIA.
Table 1 Distribution of HBV markers among allsamplesHBsAg HBcAb NAT Total Percentage
(%)
R NR NR 7 1.21
R R NR 17 2.93
R R R 31 5.34
NR R NR 513 88.3
NR R R 12 2.07
NR NR R 0 0
R NR R 1 0.2
NR NR NR 7640
The above mentioned fact suggests thatthough ID-NAT is not supporting toeliminate anti HB core but still is required
validity based upon time to time, becausemutation of the viral pathogen.
Safety of blood is a challenge in Indiabecause of the high prevalence of HBV,HCV and HIV, the relatively lowpercentage of volunteer donors and the lackof standardization of screening proceduresamong the multitude of blood collectioncentres.20 The potential of NAT yield inIndia is staggering when compared to othercountries that have already implemented thetechnology. The study showed that only0.2% of the positive samples were HBsAgreactive/ ant-HB core non reactive/ ID-NATreactive and none of the sample (0%) werefound to be HBsAg non reactive/ anti-HBcore non reactive/ ID-NAT reactive. Thesefindings clearly indicate that NAT is capitalextensive in the present scenario. Costeffectiveness of introducing universal anti-HBc screening and discarding large numberof blood units versus considering ID NATneeds to be assessed.
Another Indian study on large section ofblood donors demonstrated 4.2 per centanti-HBc only positivity.9 Hence, we haveobserved 6.24% (513 out of 8221)prevalence of anti-HBc positivity, whichcorroborates with our finding. The otherstudy supports the presence of occult HBVinfections in blood donors positive forantibodies against hepatitis B core antigenand emphasizes on the need for establishingsensitive screening modalities for bloodtransfusion.32 In our study, we also find thatthe presence of occult HBV infections inblood donor’s positive hepatitis B coreantibody and focuses on the need forestablishing sensitive screening modalitiesfor blood transfusion.
It is commonly followed that the diagnosisof infection by HBV is based on thepresence of the HBsAg in thebloodstream.21 However, screening of bloodbank donors for HBsAg does not totallyminimize the chances of the risk of HBV

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 26
infection through blood transfusion,22 sincethe absence of HBV marker in the serumdoes not exclude the presence of HBVDNA.23,24 It is in this context it can be saythat, donors with occult HBV infection,who lacked detectable HBsAg but whoseexposure to HBV infection was indicated bya positive anti-HBc and HBV DNA, may bea potential source of HBV infection.
In India, anti-HBc screening is notmandatory. However, higher prevalence ofonly anti-HBc (58.8%) cases with 22.8%HBV DNA reactivity from Kolkata.25
Similarly, other studies also substantiatewith Pakistani and Egyptian studiesshowing 17.2 and 21.47 per cent anti-HBcprevalence in HBsAg-negative, HBV DNA-negative blood donors.26,27 In India wherethe anti-HBc reactivity ranges from 4.2% to18.3 % in healthy donors.9,28 In this studyalso found that between the above findings.
Most studies on occult hepatitis B infectionhave reported higher rates of HBV- DNAdetection in liver or peripheral mononuclearcells compared with serum or plasma.22
The result of study on only serum or plasmasample showed that only 0.2% of thepositive samples were HBsAg reactive/ HB
core non reactive/ ID-NAT reactive andnone of the sample (0%) were found to beHBsAg non reactive/ HB core non reactive/ID-NAT reactive, these finding alsoindicate the HBV-DNA detection is verylow. Bre´chot et al.(2001) Reported thatoccult HBV infection exists and that mostcases are related to very low levels of HBVrather than to HBV mutants that do notexpress or produce abnormal surface
proteins and consequently are undetected bystandard method.29 Because HBV-DNAdetection is the gold standard method todiagnosis of occult HBV infection, the typeof assay used and its sensitivity must bespecified. The sensitivity of PCR assays forHBV DNA in studies on occult HBVinfection varies from 101 to 103copies/mL.30 However, most of the PCRassays including commercially availableassays are not standardized.31
Our earlier study shows out of 2740samples (n= 186) 6.7% sample reactive byHBV marker. There was no sample whichwas non reactive by serological markers butobserved to be ID-NAT reactive. This studyshows that about 6% of HB core antibodywere reactive and the other related studyshows the percentage of anti HB core

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 27
reactivity is 4.2% to 18.3 % in healthydonors in our country.9,28,31 Our study alsoshows no non- reactive sample wasobserved to be reactive by ID-NAT, duringthe study period. Further the study finds thatthe presence of various races in NCRincreases the chances of genetic diversity ormutation of genes and this tendency makesdifficult for ID-NAT. Hence, it is suggestedthat the reliability of NAT should beverified and assessed timely.
CONCLUSION
Anti-HB core is the most common cause ofblood discarding by TTI screening. Still,HBcAb should be carried out to rule outtransmission of HBV among HBsAg non-reactive blood (2.07%: Table 1). Oncontrary, no sample was observed, whichwas NAT reactive and is not reactive byCLIA. Screening of blood by Anti- HBcAbdoes enhance the blood safety. In addition,NAT facility can enhance the blood safetybut cannot replace Anti HB core Screening.
The facility for HBV core screening is sameas that of HBsAg, HIV & HCV, whereas,NAT is capital extensive requiringdedicated space and staff. Practical benefitsrandom access CLIA such as minimal useof rapid methods, high sensitivity,documentation and reproducibility shouldbe taken in to consideration for formulatingpolicies of TTI screening. Therefore, thescreening for core antibody seems to be abetter strategy than NAT in case of resourcelimitation. The policy should be based onavailable resources, potential humaneconomic value in the target population,technical competence and presence of viralstrains that can be detected by the NAT.
ACKNOWLEDGEMENT
Our sincere thanks to Prof. (Dr.) Nasser Al-Jarallah, Dean College of Applied MedicalSciences, Majmaah University, al Majmaah,Riyadh-KSA. Mr. Kunwar Singh,Laboratory Technician, Faculty of applied
Science, Manav Rachna InternationalUniversity. Mr. Prashant Srivastava teamleader Transfusion Medicine, Artemis healthInstitute, Gurgaon.
REFERENCES
1. Zarski JP, Ganem D, and Wright TL (2002)Hepatitis B virus. In Clinical Virology, edsD. D. Richman, R. J. Whitley and F. G.Hayden, pp. 623–57. Washington DC, ASMPress.
2. Previsani N, Lavanchy D and Siegl, G.(2004) Hepatitis A. In Viral Hepatitis:Molecular Biology, Diagnosis,Epidemiology and Control (Perspectives inMedical Virology, volume 10), ed. I. K.Mushahwar, pp. 1–98. Amsterdam, Elsevier.
3. Beeson PB. Jaundice occurring one to fourmonths after transfusion of blood or plasma:report of seven cases. JAMA 1943; 121:1332–4.
4. Morgan HW and Williamson DA. Jaundicefollowing administration of human bloodproducts. BMJ 1943; 1: 750–3.
5. Narayan S. Microbes and blood transfusion.Indian Journal of Medical Microbiology2001; 19 (3): 119-126.
6. Stramer SL. Pooled HBV DNA testing bynucleic acid amplification: implementationor not. Transfusion 2005; 45: 1242–6.
7. Biswas R, Tabor E, Hsia CC, Wright DJ,Laycock ME, Fiebig EW et al. Comparativesensitivity of HBV nucleic acid tests andHBsAg assays for detection of acute HBVinfections. Transfusion 2003; 43: 788–98.
8. World Health Organization. Hepatitis Bsurface antigen assays: operationalcharacteristics (May), Geneva, World HealthOrganization 2001.
9. Chaudhuri V, Nanu A, Panda SK, Chand P.Evaluation of serologic screening of blooddonors in India reveals a lack ofcorrelation between anti-HBc titer and PCR-amplified HBV DNA.Transfusion 2003; 43:1442-1448.
10. Nanu A, Sharma SP, Chatterjee K, Jyoti P.Markers for transfusion-transmissibleinfections in north Indian voluntary andreplacement blood donors: prevalence andtrends 1989-1996. Vox Sang 1997; 73: 70-73.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Evaluation of HbcAb in the presence of ID-NAT, Choudhary RK. 28
11. Yotsuyanagi H, Yasuda K, Moriya K,Shintani Y, Fujie H, Tsutsumi T et al.Frequent presence of HBV in the sera ofHBsAg- negative, anti-HBc- positive blooddonors. Transfusion 2001; 41: 1093-1099.
12. Infectious Disease Testing for BloodTransfusions. NIH Consens Statement 1995Jan 9-11;13(1):1-29.
13. Kleinman SH, Kuhns MC, Todd DS, GlynnSA, McNamara A, DiMarco A, et al.Frequency of HBV DNA detection in USblood donors testing positive for thepresence of anti- HBc: implications fortransfusion transmission and donorscreening. Transfusion 2003; 43: 696- 704.
14. Beasley RP. Hepatitis B virus. The majoretiology of hepatocellular carcinoma.Cancer 1988; 61: 1942–56.
15. Busch MP. Should HBV DNA NAT replaceHBsAg and/or anti-HBc screening of blooddonors? Transfus Clin Biol 2004; 11: 26–32.
16. Kleinman SH, Strong DM, Tegtmeier GG,Hepatitis B virus (HBV) DNA screening ofblood donations in mini-pools with theCOBASAmpliScreen HBV test. Transfusion2005; 45: 1247–57.
17. Klein HG. Pathogen inactivationtechnology: cleansing the blood supply. JIntern Med 2005; 257: 224–37.
18. Lin L, Cook DN, Wiesehahn GP, Alfonso R,Behrman B, Cimino GD et al.Photochemical inactivation of virus andbacteria in platelet concentrates by use of anovel psoralen and long- wavelengthultraviolet light. Transfusion 1997; 37: 423–35.
19. Snyder EL and Dodd RY. (2001) Reducingthe risk of blood transfusion. Hematology(Am Soc Hematol Educ Program), 433–42.
20. Kapoor D, Saxena R, Sood B, Sarin SK.Blood Transfusion practices in India:Results of a national survey. Indian JGastroenteral 2000; 19: 64-7.
21. Badur S, Akgun A. Diagnosis of hepatitis Binfections and monitoring of treatment. JClin Virol 2001; 121: 229-37.
22. Conjeevaram HS, Lok AS. Occult hepatitisB virus infection: a hidden menace?Hepatology 2001; 34:204-6.
23. Comanor L, Holland P. Hepatitis B virusblood screening: unfinished agendas. VoxSang 2006; 91: 1-12.
24. Dreier J, Kroger M, Diekmann J, Gotting C,Kleesiek K. Low-level viraemia of hepatitisB virus in an anti-HBc- and anti-HBs-positive blood donor. Transfus Med 2004;14 : 97-103.
25. Banerjee A, Chandra PK, Datta S, BiswasA, Bhattacharya P, Chakraborty S, et al.Frequency and significance of hepatitis Bvirus surface gene variant circulatingamong ‘antiHBc only’ individuals in EasternIndia. J Clin Virol 2007; 40 :312-7.
26. Bhatti FA, Ullah Z, Salamat N, Ayub M,Ghani E. Anti- hepatitis B core antigentesting, viral markers, and occult hepatitis Bvirus infection in Pakistani blood donors:implications for transfusion practice.Transfusion 2007; 47 : 74-9.
27. Zekri AR, Awlia AA, El Mahalawi H,Ismail EF, Mabrouk GM. Evaluation ofblood units with isolated anti HBc for thepresence of DNA. Dis Markers 2002; 18:107-10.
28. Bhattacharya P, Chandra PK, Datta S,Banerjee A, Chakraborty S, Rajendran K, etal. Significant increase in HBV, HCV, HIVand syphilis infections among blood donorsin West Bengal, Eastern India 2004-2005:exploratory screening reveals highfrequency of occult HBV infection. World JGastroenterol 2007; 13 : 3730-3.
29. Bre´chot C, Thiers V, Kremsdorf D, NalpasB, Pol S, Paterlini-Brechot P. Persistenthepatitis B virus: clinically significant orpurely occult? Hepatology 2001;34:194-203.
30. Pawlotsky JM, Bastie A, Hezode C, LonjonI, Darthuy F, Remire J, Dhumeauz D.Routine detection and quantification ofhepatitis B virus DNA in clinicallaboratories: performance of threecommercial assays.J Virol Methods2000;85:11-21.
31. Choudhary RK, Singh J, Singh H. Role ofanti-HBcore antibody screening byChemiluminescence in facility with ID-NATtesting; MR international journal ofEngineering & Technology 2010; 2(2): 42-45
32. Asim M, Ali R, Khan LA, Husain SA,Singla R, Kar P. Significance of anti-HBcscreening of blood donors & its associationwith occult hepatitis B virus infection:Implications for blood transfusion; Indian JMed Res 2010: 312-317.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reference Range for Copper in Adult Population, Warda Hussain et al. 29
REFERENCE RANGE FOR COPPER IN ADULT POPULATION(20-29 YEARS) OF LAHORE - PAKISTANWarda Hussain2, *Asim Mumtaz1, Sana Khan2, Tauqeer Butt1
ABSTRACT
Copper, an essential trace element for health, plays various biological roles in human body.Serum copper reference values are important for assessing copper associated abnormalitiesand the prevalence of copper deficiency. The aim of this study was to determine referencerange of copper in adult population of Lahore. Serum copper concentration was measuredby flame atomic absorption spectrometry in 450 healthy adults aged 20 to 29 years, whichwere randomly selected. After application of exclusion criteria reference values weredetermined in apparently healthy subjects according to guidelines of InternationalFederation of Clinical Chemistry. Reference value for serum copper concentration rangedbetween 4.72µmol/L to 31.48µmol/L (mean 17.62 µmol/L ±6.67). The mean serum copperlevel for males was 18.57µmol/L ± 6.61. The value for male subjects ranged between4.72µmol/L to 31.7µmol/L. The mean serum copper level in females being 16.52µmol/L ±6.67. Similarly the values for females range between 4.72 µmol/L to 30.48µmol/L. Inconclusion this study presents reference values for serum copper concentration in adultpopulation of Lahore. The results here shows that there is significant difference in serumlevel of copper among different countries. This difference may be due to racial and geneticdifference, dietary habits and socioeconomic and analytical variables. KEY WORDS: copper,reference value, atomic absorption spectrometry, population
المرجعیةالقیم. االنسانجسمفيمختلفةبیولوجیةأدوارویلعبالصحةفياالساسیةالعناصرمنالنحاس:ملخصنقصانتشارمعدلولتحدیدمصلالفيللنحاسطبیعیةالغیرالمستویاتلتحدیدضروریةالدممصلفيالنحاسلمستويتركیزقیاستم. الھورمدینةسكانمنللبالغینالنحاسلقیممرجعيمدىتحدیدھوالدراسةھذهمنالھدف. النحاساختیارھمتموالذین( عاما٢٩إلى٢٠بینأعمارھمتتراوحالذیناألصحاءالبالغینمن٤٥٠لعددالدمفيالنحاسلموجھاتوفقااالصحاءفيالمرجعیةالقیمتحدیدتماالستبعادمعاییرتطبیقبعد. الطیفيالتحلیلجھازبواسطة) عشوائیالتر/مولمیكرو٤،٧٢( بینتراوحتالدممصلفيالنحاسلتركیزالمرجعیةالقیمة. السریریةللكیمیاءالدولياالتحاد
المصلفيالنحاسمستوىمتوسطكان). ٦،٦٧± لتر/ مولمیكرو١٧،٦٢المتوسط()لتر/ مولمیكرو٣١،٤٨الي٣١،٧اليلتر/ مولمیكرو٤،٧٢(بینللذكورالقیمةتراوحتحیث), ٦٫٦١± لتر/ مولمیكرو١٨،٥٧(للذكورالقیمفإنوبالمثل،. ٦٫٦٧± لتر/ مولمیكرو١٦،٥٢لإلناثالمصلفيالنحاسمستوىمتوسطو). لتر/ مولمیكرو
الدراسةھذهتالخالصة: قدم). لتر/ مولمیكرو٣٠٫٤٨اليلتر/ مولمیكرو٤٫٧٢( بینتراوحتاإلناثمجموعةلفيكبیرفرقھناكأنأظھرتھناالنتائج. الھورمدینةسكانمنللبالغینالدممصلفيالنحاسلتركیزالمرجعیةالقیم
لالختالفأو, الجینیةأوالعرقیةاالختالفاتإلىراجعایكونقدلفرقاھذا, البلدانمختلفبینبالمصلالنحاسمستوى.التحلیلیةأوواالقتصادیةاالجتماعیةللمتغیراتأوالغذائیةالعاداتفي
Received: 5 April, 2013; Accepted: 6 June, 2013
*Correspondence: [email protected] Medical & Dental College, Lahore Pakistan2University of Health Sciences, Lahore Pakistan

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reference Range for Copper in Adult Population, Warda Hussain et al. 30
INTRODUCTION
The availability of accurate trace elementreference values in human is an importantindicator to the health status of the generalpopulation and the occupational groupswhich are exposed to trace elements.1 Thekey role of the laboratory scientist is to helpthe clinician in interpreting observedvalues, by providing relevant referencevalues in a convenient and practical form.2In Pakistan, reference values used inlaboratories have been established in thewestern population. But these can bequestioned due to differences in geneticload, lifestyle, and diet.3
Copper, an essential trace element isinvolved in multiple biological processes.4The importance of this trace element inhealth and disease cannot be ignored. Toassess the relation of this trace element withdifferent diseases, it is important to have abaseline status of this trace element in thebody in the healthy sample of population.So this requires establishment of accuratereliable reference values that can be used inclinical decision.5
The recommended daily requirement ofcopper in our body is 2.5 - 3 mg/day. About30% of ingested copper is absorbed in theintestine, bound to albumin and transportedto the liver, where it is stored. The majorcirculating form ceruloplasmin issynthesized in the liver.
Copper is an integral component of at least16 essential metalloproteinase, includingcytochrome oxidase, monoamine oxidase,lysyl oxidase, tyrosinase and ceruloplasmin.It participates in prostaglandin synthesis, inthe formation of connective tissues, in thefunction of Central nervous system and inhematopoiesis. It is required for red andwhite cell maturation, cholesterol andglucose metabolism and myocardialcontractility. The stability of vein'smembrane depends on the adequate amount
of copper in the tissues. Copper is involvedin the transport of iron and vitamin A.6 Itsdeficiency contributes to the development& progression of certain diseases.
The objective of this study was to establishreference range for copper in adultpopulation with 20 to 29 years of ageresiding in Lahore.
DESIGN AND METHODS
This was a descriptive cross sectional studywhich was conducted on apparently healthyindividual of age range 20 to 29 years fromnine different zones of Lahore. A total of450 healthy individuals comprising of 216males & 234 females were randomlyselected using a multistage samplingmethod. Five union councils were selectedrandomly from each zone. From eachselected union council ten healthy subjectswho were assessed clinically were selectedfor the study. So a total of 450 sampleswere collected from randomly selected 45union councils. The exclusion andinclusion criteria were based on the IFCCguidelines for the establishment ofreference values. The study was approvedby Ethical Committee. Written consent wastaken from all the subjects.
At the time of sampling based on pastmedical history and physical examinationonly those individuals were included whodid not prove any signs and symptoms ofdisease.
The samples were collected under asepticconditions. 7 ml of blood was collected in 2serum separator vacutainer tubes (SST, BDvacutainer) one for the determination oftrace elements and other 3.5 ml blood wascollected in SST for determination ofalbumin, glucose & ALT without venousstasis and without frothing. The sample wastransported to University of HealthSciences, Lahore in an ice box containingice bags.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reference Range for Copper in Adult Population, Warda Hussain et al. 31
Serum was separated by centrifugation at3000 g for 05-10 minutes. Serum separatedwas then carefully shifted into 1ml nitricacid treated aliquot (for trace elementsdetermination) & the other separated serumwas collected in a separate aliquot for ALT,albumin and sugar levels. Hemolyzed andsamples having high levels of glucose,albumin or ALT were excluded from thisstudy.
Only nitric acid washed plastic lab warewas used for sample and standardpreparation for trace elements. Urineexamination for protein & sugar was alsoperformed. Trace element Copper wasperformed on Hitachi Z-2000 SeriesAtomic Absorption Spectrophotometer.
Serum copper was measured by flameatomic absorption spectrometry (Hitachi Z-2000) following a one in five dilution withdistilled water. The results were multipliedby dilution factor 5.
Statistical analysis: Data was analysedusing SPSS version 20. Serum Copperlevels were expressed as Mean ± SD.
RESULTS
A total of 450 healthy subjects wereincluded in which 216 were males and 234were females. Only those subjects wereincluded who fulfilled the inclusion criteria.Their health status was assessed afterdetailed history & physical examination.Blood sugar random, ALT, Albumin, urinefor proteins & sugar were performed. Theresults of these tests were also in the normalrange. The blood samples of these healthy450 subjects were then selected for theestimation of serum copper which wasestimated on atomic absorptionspectrometer.
The mean age range of these healthysubjects was 25 years. The mean for serumcopper was found to be 17.62±6.67 µmol/L.Here the value of serum copper ranged
between 4.72 to 31.48µmol/L. The meanserum copper level for males was18.57±6.61 µmol/L with a range of 4.72 to31.7µmol/L. The mean serum copper levelin females being 16.52±6.67 µmol/L. Herethe values for females ranged between 4.72to 30.48 µmol/L. Minimum & maximumlevels of Copper in µmol/L along with95th confidence interval, also the 2.5thpercentile & 97.5th percentile are shown intable 1.
Table 1: Minimum & Maximum levels ofCOPPER in µmol/L with 95th confidenceinterval (CI), also the 2.5th percentile &97.5th percentile
Copp
er
Min
µmol
/L
Max
µmol
/L
95th
CI
2.5th
Perc
entil
e
97.5
th
Perc
entil
e
Male 3.14 33.05 17.31 -19.83 4.72 31.7
Female 3.14 41.40 15.58–17.78 4.72 30.48
Overall 3.14 42.49 16.84–18.41 4.72 31.48
DISCUSSION
Reference interval refers to the intervalbetween reference limits that includesusually 95% of the reference values.7 It isalso defined as a range comprising between2.5th & 97.5th percentile of the datadistribution from a given referencepopulation.8 Establishing a normal range oftrace elements in the sera of healthyindividuals in any geographical area is very

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reference Range for Copper in Adult Population, Warda Hussain et al. 32
important for interpretation of trace elementresults and for further studies in thatparticular region.9
Copper, an essential trace element isrequired in body for performing majorfunctions. Copper is an importantcomponent of ceruloplasmin and variousenzymes including ferroxidase II, lysyloxidase, Zn-Cu superoxide dismutase,tyrosinase.9
The range for copper varies from 4.72 to31.48µmol/l with a mean of 17.62µmol/L.These results were in close proximity withanother study carried out in Pakistan in2004 in Islamabad / Rawalpindi area wheremean copper concentration was found to be18.1µmol/L with a range of 9.4 to 30.06µmol/L.10 This slight difference in the meanvalue of copper might be attributed to thedifference in the age range of thepopulation included in that study. Anotherfactor contributing to this difference may bethe integrated diet mainly consisting ofwheat & wheat products.10
A study conducted by Manser and Khan11
in Karachi on normal population found thatthe mean concentration of copper was14.71µmol/L which was lower as comparedto this study. The main contributing factorfor this difference could be the excessiveuse of the automobiles & pesticidesresulting in environmental pollution.
Another factor contributing to the increasein the concentration of copper is thedistribution of water for domestic uses,particularly in the system where an acidicpH exists.12 In this regard, WHO conducteda study in Pakistan on quality of drinkingwater and found that the concentration ofthe copper in the drinking water varieswidely which is constantly adding copperelement to the drinking water. Along withthe manufacturing of the commercialappliances like wires & pipes, copper wasalso used as the copper sulphate
pentahydrate for the control of algae inwater pipes.
The other factors include the inhalation ofcopper fumes produced mainly duringwelding & plumbing increases copperconcentration in blood. Copper could alsobe present in drinking water pipes as itremains in pipes during water supply. Thedeficiency of iron, zinc, vitamin B andvitamin C also raises copper concentrationin human.13
Copper is being constantly added in soilform of pesticides, fertilizers, industry &sewage sludge. Similarly melting, grinding& cutting of copper may produce fumes &dusts & exposure & inhalation of thesefumes may be the contributors of raisedcopper levels in our body.14
A study conducted in Iran in 2011 showedthat the mean value of serum copper in ageranging from 20 to 29 years was14.2µmol/L. The mean age range being 25years is comparable to population in Lahorewhere mean copper concentration was17.62µmol/L. This was mainly attributed tothe lifestyle & habits of the people living inIran.15 Urbanization & educationalattainments might be the factorscontributing to the changes in serum copperlevels.
The reference range used by the traceelement & Environment ToxicologyLaboratory at the University of Alberta hada mean of 19µmol/L for copper which isclose to the mean (17.62µmol/L) of ourpopulation under study. The authormentioned that the range for a trace elementanalysis is only suggestive of the usualexposure of this element encountered indaily life.16
Similar study conducted in Kuwaitdetermined serum level of copper in normalpopulation. Here mean copperconcentration was found to be 23µmol/L.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reference Range for Copper in Adult Population, Warda Hussain et al. 33
This large difference in mean concentrationof copper is mainly attributed toDesalination plants which are used inArabian Gulf. These plants were the mainsource of increased copper levels in theenvironment. On the other hand industries& oil pollution were constantly addingcopper to the environment.17
The concentration of copper in our studywas comparable to the reported values fromSpain and China where mean copperconcentration was 17.27µmol/L and17.11µmol/L respectively.18 Similarly meanconcentration of copper reported from Italywas 19.15µmol/L which was alsocomparable with the mean concentration ofour study.19
The mean copper level (17.62µmol/L) ofour study was found to be greater than thatreported in studies from Bangladesh &Japan that had a mean concentration of15.38 µmol/L & 12.56µmol/Lrespectively.20,21
Our study did not show a significantdifference in mean concentration of copperwhen compared with mean concentration ofcopper quoted in reference books (p = 0.9).
The mean serum copper concentration ofour study compared with various countriesis shown in following figure.
CONCLUSION
This study provides data for theestablishment of reference range for copperin healthy population of Lahore. Here themean concentration of copper is17.62±6.6µmol/L. The results showed thatthere is significant difference in serum levelof copper among different countries. Diet,physical environment and socioeconomicconditions all affect the physiology of apopulation. These values can be useful forinterpretation and clinical management ofcopper disorders. As there are noestablished reference ranges for trace
elements in Pakistan, these findings canform the basis and reference for any futurestudies on trace elements in Pakistan.
LIMITATION OF THE STUDY
The study was carried out on only specificage group due to financial constraint facedduring the study.
REFERENCES
1. Goldbeck-Wood S, Dorozynski A, Lie LG,Kučera J, Benckob V, Sabbionic E, Van derVenne MT. Review of trace elements inblood, serum and urine for the Czech andSlovak populations and critical evaluationof their possible use as reference values.Science of the total environment. 1995;166(1): 211-34.
2. Ashavaid TF, Todur SP, Dherail AJ.Establishment of reference intervals inIndian population. Indian J Clin Biochem.2005; 20(2): 110–18
3. Mansoor R, Saadat A, Khan FA, Sattar A,Iqbal A. Reference values for serumcalcium. Pak J Pathol 2004;15(2):49-53.
4. Lux O, Naidoo D. The assessment ofbiological variation components of copper,zinc, and selenium. The Journal ofNutritional Biochemistry. 1995; 6(1): 43-7.
5. Rahil-Khazen R, Bolann JB, Ulvik JR.Trace elements reference values in serumdetermined by inductively coupled plasmaatomic emission spectrometry. Clin ChemLab Med. 2000;38(8):765-72
6. Marjani A, Mojerloo M, Mansorian AR,Golalipour MJ. Serum Zinc and Copperlevel before and after haemodialysis.Iranian Red Crescent Medical Journal.2005; 8(1);71-75
7. How to define and determine referenceintervals in the clinical laboratory:approved guidelines, NCCLS documentC28-A2. 2001; 20(13)http://www.nccls.org/
8. Trujillano J, Muiño JM, March J, SorribasA. A more flexible parametric estimation ofunivariate reference intervals: A newmethod based on the GS-distribution. ClinChim Acta. 2007;379(1-2):71-80
9. Al-Sayer H, Al-Bader A, Khoursheed M,Asfar S, Hussain T, Behbehani AI, Mathew

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Reference Range for Copper in Adult Population, Warda Hussain et al. 34
A, Dashti H. Serum values of copper, zincand selenium in adults resident in Kuwait.Med Principles Pract. 2000; 9:139–146
10. Rahman S, Khalid N, Ahmad S, Ullah N,Iqbal ZM. Essential trace metals in humanwhole blood in relation to environment.Pakistan J. Med. Res. 2004; 43(2):46-51
11. Manser WW, Khan MA. Trace elementsstudies on Karachi population, part 1:Normal ranges for blood copper, zinc andmagnesium for adults. J Pak Med Assoc1989; 39(2):43-9
12. National standards for drinking waterquality. Pakistan Environmental ProtectionAgency (Pak EPA). Ministry ofEnvironment, Government of Pakistan,Islamabad. 2008. Pak, E.http://scholar.google.com.pk/scholar?q=National+Standards+for+Drinking+Water+Quality+in+pakistan&btnG=&hl=en&as_sdt=0%2C5&as_ylo=2008&as_yhi=2008
13. Ali SFA, Imtiaz N, Mehdi SU, Asif M.Determination of Copper Concentration inHuman Blood Serum by Using FlameAtomic Absorption Spectroscopy (FAAS).Paper presented at: InternationalConference on Chemical Engineering andPharmaceutical Sciences (ICCEPS'2012)April 13-15, 2012 Pattaya
14. Khan MA, Ahmad I, Inayat ur Rahman.Effect of environmental pollution on heavymetals content of Withania somnifera.Journal of the Chinese Chemical Society.2007;54:339-343
15. Parizadeh RMS, Kazemi-Bajestani RMS,Moghaddam SA, Mobarhan GM, EsmaeiliH, Majidi RM, Emadzadeh A, Safarian M,Nezhad AM, Khodaei HG, Hosseini JS,Parizadeh JMS, Oladi RM, Ferns G. Serumzinc and copper concentrations andsocioeconomic status in a large Persiancohort. Asian Biomedicine. 2011; 5 (3):329-35
16. Guidotti TL, McNamara J, Moses MS. Theinterpretation of trace element analysis inbody fluids. Indian J Med Res. 2008 Oct;128(4):524-32 .
17. Lattemann S, Höpner T. Environmentalimpact and impact assessment of seawaterdesalination. Desalination. 2008; 220(1-3):1–15
18. Shang S, Hong W. Flame atomicabsorption spectrometry using amicrovolume injection technique for thedetermination of Cu, Zn, Ca, Mg and Fe inwhole blood from healthy infant andmother ears. Fresenius' Journal ofAnalytical Chemistry. 1997; 357(7): 997-99
19. Minoia C, Sabbioni E, Apostoli P, Pietra R,Pozzoli L, Gallorini M, Nicolaou G,Alessio L, Capodaglio E. Trace elementsreference values in tissues from inhabitantsof the European community I. A study of46 elements in urine, blood and serum ofItalian subjects. Sci Total Environ.1990;95: 89-105
20. Khan AH, Khaliquzzaman M, Zaman MB,Husain M, Abdullah M, Akhter S. Traceelement composition of blood in adultpopulation in Bangladesh. Journal ofRadioanalytical Chemistry. 1980;57(1):157-167
21. Satoh Y, Yazawa A. Contents of heavymetals in the blood of inhabitants inYokohama city in Japan. Yokohama E.,Ken Nenpo. 1978;17: 63-66.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 35
COMPLEMENTARY AND ALTERNATIVE MEDICINE USEAMONG HEALTH WORKERS IN MID-DELTA, EGYPT
*Ahmed T. ElOlemy1, Nashwa M. Radwan2, Walid Dawood3, Ihab Ali3, Latifa M. Fouda3
ABSTRACTBackground: Alternative and complementary medicine (CAM) attracted national attentionfrom the media, governmental agencies, and the public. The Study aimed at assessing pattern ofCAM use among health workers in mid-Delta, Egypt. Design and Methods: A cross-sectionaldescriptive survey with multi-stage random sample technique was used. A total sample size of873 health workers (technicians, allied health personnel, pharmacists and physicians) waschosen randomly from two university hospitals and four general hospitals in mid-Delta. Theyfulfilled self-administered questionnaire regarding their socio-demographic data, knowledge onCAM and their sources, causes of CAM use, diseases for which CAM used and commonly usedCAM practices in the area. Results: females constituted 77.32% of the sample, 47.42% aged 20- 25 years, 54.64% have less than 5 years of work, 46.39% have bachelor's degree and 50.52%have diploma. Three fourths of health workers have knowledge about CAM, 4.12% usually useCAM and 38.14% sometimes use it. Media was the source of CAM knowledge for 54.79%,followed by relatives and friends for 31.51%. One fourth of participants talk on CAM with theirpatients and 28.87% advice patients to use CAM. Minimal side effects (43.29%) and religiousbelieves (21.64%) are the main causes of using CAM. Patients use CAM for backache, jointpain, abdominal colic and flatulence (18.45%, 14.56%, and 12.62%) respectively. Propheticmedicine, Honey and bee products, herbal products, food supplements and Hijama were thecommonly used CAM practices in the area (73.2%, 65.98%, 47.42%, 45.26% and 38.14%respectively). Conclusion: There is an increasing interest in CAM knowledge among healthworkers. Media, relatives and friends are the main sources of information. Religious practicesas Prophetic medicine, honey and bee products, herbs and hijama are the most prevalent CAMpractices in the area. There is reluctance in talking with their patients on CAM or referringpatients to CAM practitioners. KEY WORDS: Alternative, Complementary, Medicine, Healthworkers, knowledge, causes, mid-Delta, Egypt.
. والجمھورالحكومیةوالوكاالتاإلعالموسائلخاللمنبھالوطنياالھتمام) CAM(والتكمیليالبدیلالطبجذب: خصملمنھج. بمصرالدلتاوسطفيالصحةمجالفيالعاملینبینوالتكمیليالبدیلالطباستخدامنمطتقییمإلىالدراسةھذهھدفتالعاملینمن٨٧٣العینةحجمبلغ. المراحلةمتعددعشوائیةعینةوباختیار, عيالمقطالوصفيالمسحاستخدامتم: البحث
الجامعیةالمستشفیاتمناثنینمنعشوائيبشكلاختیارھمتم) واألطباءوالصیادلة،،الصحةوموظفيفنیین(الصحیینالطبعنوالمعرفةوالدیمغرافیة،الجتماعیةاالبیاناتیحوياستبیاناستخدم. بمصرالدلتاوسطفيعامةمستشفیاتوأربعةیشیعالتيوالتكمیليالبدیلالطبوممارساتیعالجھاالتيواألمراضاستخدامھ،أسبابومصادرھا،والتكمیليالبدیل
اعأربثالثة. عاما٢٥- ٢٠بیناعمارھم) ٪٤٧،٤٢. (العینةمن) ٪٧٧،٣٢(اإلناثشكلت: النتائج. المنطقةفياستخدامھاوالتكمیليالبدیلالطبیستخدمونماعادة) %٤،١٢(،والتكمیليالبدیلالطبحولمعرفةلدیھمالصحةمجالفيالعاملین
،)٪٥٤٫٧٩(لوالتكمیليالبدیلبالطبالمعرفةمصدراالعالموسائلكانت. األحیانبعضفيیستخدمونھ) ٪٣٨،١٤(وعنمرضاھممعتحدثواانلھمسبقبالدراسةالمشاركینربع). ٪٣١٫٥١(لواألصدقاءاألقارببواسطةالمعرفةتلیھا
من) ٪٤٣٫٢٩(اتفق. والتكمیليالبدیلالطبباستخداممرضاھمعلياشاروا) ٪٢٨٫٨٧( ،والتكمیليالبدیلالطبمن) ٪١٨٫٤٥(یستخدم. نیةدیلمعتقدات) ٪٢١٫٦٤(والجانبیةآثارهلقلةوالتكمیليالبدیلالطباستخدامعليالمشاركینكان. البطنوانتفاخللمغص) ٪١٢٫٦٢( والمفاصل،آلالم) ٪١٤٫٥٦(والظھر،آلالموالتكمیليالبدیلالطبالمرضى
Received: 30 March, 2013; Accepted: 10 June, 2013
*Correspondence: [email protected]. of Public Health and Community Medicine, Faculty of Medicine, Tanta University, Egypt, and Consultant inNCCAM, Saudi Arabia. 2Prof. of Public Health and Community Medicine, Faculty of Medicine, Tanta University,Egypt.3Assistant. Prof. of Public Health and Community Medicine, Faculty of Medicine, Tanta University, Egypt

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 36
البدیلالطبممارساتمنوالحجامةالغذائیةوالمكمالتاألعشابومنتجاتالنحل،ومنتجاتوالعسلالنبويالطبعلى٪٣٨٫١٤و٪٤٥٫٢٦،٪٤٧٫٤٢،٪٦٥٫٩٨،٪٧٣٫٢(التالیةبالنسبالمنطقةفيعادةخدمتستالتيوالتكمیلي
وسائل. الصحةمجالفيالعاملینبینوالتكمیليالبدیلالطببخصوصالمعرفةفيمتزایداھتمامھناك: الخالصة). التواليالنحلومنتجاتوالعسلالنبوي،والطبالدینیةاتالممارس. للمعلوماتالرئیسیةالمصادرھيواألصدقاءواألقارباإلعالم
البدیلالطبعنالمرضيمعالحدیثفيترددھناك. المنطقةفيانتشارااألكثرالممارساتھيوالحجامةواألعشاب.والتكمیليالبدیلالطبممارسینإلىالمرضىإحالةأووالتكمیلي
INTRODUCTION
Complementary and Alternative Medicine(CAM) is defined as a group of diversemedical and health care systems, practices,and products that are not generallyconsidered to be part of conventionalmedicine.1 National surveys performedworldwide suggest that CAM is popularthroughout the industrialized world.2Population who use CAM therapies duringthe last 12 months has been estimated to be10% in Denmark (1987),3 33% in Finland(1992),4 49% in Australia (1993),5 and 15%in Canada (1995).6 A considerable useexists in many developing countries(Colombia, 40%; Chile, 71%; up to 80% inAfrican countries).7,8 Exact estimates ofexpenditure on CAM have been difficult todetermine though there is little doubt that itis enormous. In 2002, it was estimated thatthe amount spent on CAM in the USA wasUS $2.7 billion, US$ 2.4 billion in Canada,and US$ 2.3 billion in the UnitedKingdom.9
CAM services are usually used alongsideand in addition to conventional medicine.Thus, a vast informal and silent health caresector exists in almost all countries. Nocomprehensive picture of this sector existsas yet in any country.10 Data oneffectiveness of various CAM treatmentsbeing used alone and in combination areinadequate. CAM is used by the people inmanagement of chronic conditions that arecostly to society, such as chronic pain andarthritis, and more life-threatening diseases,such as heart diseases and cancer.11
The exact reasons for the popularity ofCAM are complex; they change with timeand place; they may vary from therapy totherapy. They are different from oneindividual to another.12 On the contrary,many health professionals refuse to takeCAM seriously as it lacks, to their opinion,the scientific evidence.13 Lack of scientificevidence may be related to the financial,methodological and ethical obstacles inresearching CAM.13
Health workers may be source ofknowledge about CAM as they are turnedto frequently by some of their patients forseeking advice. This may explain the hugevariation in the prevalence rate.14 Somestudies demonstrated a wide variation in theknowledge and practice of physicians.However, there was a tendency towardsincreasing use and more positive attitudetowards CAM. Many factors areinterplaying, most importantly the type oftraining in medical education, as well as thecommunity itself.15-17 In a Canadian andUnited States data base search, physicians'attitude towards CAM was more negativecompared to other health care professionalssuch as nurses, public health professionals,dietitians, social workers, medical/nursingschool faculty, and pharmacists.18
Tibbu Nabawi or prophetic medicine isbroadly accepted and practiced by mostphysicians and the public in Saudi Arabiaand most Arab and Islamic countries.National Center for CAM in Saudi Arabia2010,19 Al-Faris et al.,20 and Hassan et al.,21

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 37
recorded that more than 70% of the publichad used practices related to propheticmedicine in their lifetime. The Study aimedat assessing pattern of CAM use amonghealth workers in mid-Delta, Egypt.
DESIGN AND METHODS
Study design: A cross-sectional descriptivesurvey.
Study settings: General and universityhospitals in the four governorates of Mid-Delta region (Gharbia, Kafr El-Sheikh,Dakahlia and Menofyia governorates).
Study population: Health workers(technicians, allied health personnel,pharmacists and physicians) working inmid-Delta region.
Study sample: Multistage sampletechnique was used. First phase oneGeneral hospital was chosen randomlyfrom all general hospitals in eachgovernorate, in addition to two universityhospitals Chosen randomly from the threeuniversity hospitals in mid-Delta region.The second phase a stratified randomsample was taken from Tanta Universityhospitals and Zifta general hospital inGharbia governorate, Kafr El-Sheikhgeneral hospital in Kafr El-Sheikhgovernorate, Met-Ghamr general hospital inDakahlia governorate and Menofyiauniversity hospitals and Berket El-Sabegeneral hospital in Menofyia governorate.Health workers in different hospitals wereclassified into different strata; techniciansincluding nurses, allied health personnelincluding psychologists, dietitians, socialworkers and physiotherapists, pharmacistsand physicians. The third phase asystematic random sample was taken fromeach stratum. One hundred fifty healthworkers were chosen from each hospital.The total sample size was 873 participantswho completed the study.
Methods of data collection: Aninternational self-administeredquestionnaire approved by the NationalCenter for CAM in United States was usedfor data collection.11 Questionnaires weredistributed and collected within 10 minutesat the same session. The questionnaireincluded: 1. socio-demographic data e.g.age, sex, residence, highest qualification,occupation and years of experience. 2.Knowledge about CAM and its sources. 3.Causes of using CAM. 4. Common diseasesfor which CAM used. 5. Commonest CAMmodalities used in the area. Data werecollected from July 2011 to December2011.
Statistical analysis: Data were collected,presented in tables, and statisticallyanalysed using SPSS statistical packageversion 18. Data were presented using
Table (1): Socio-demographiccharacteristics of studied population
Characteristics Number(873)
Percent
Age:20- 414 47.4125- 252 28.8730- 81 9.2835- 63 7.2240+ 63 7.22
Sex:Males 198 22.68Females 675 77.32
Years of work:-5 477 54.645- 207 23.7110- 63 7.2215- 72 8.2420+ 54 6.19
Education:Bachelor 405 46.39Diploma 441 50.52Master 27 3.09
Occupation:Physicians 54 6.19Pharmacists 72 8.25Allied healthpersonnel
270 30.92
Techniciansincluding nurses
477 54.64
Work siteMinistry ofHealth
576 65.98
Universityhospitals
297 34.02

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 38
frequencies, percentages and 95%confidence interval. CAM practices wereclassified according to use into commonlyused (>80%), usually used (60-80%),neutral (40-<60%), sometimes used (20-<40%) and rarely used (<20%).
Medical ethics: Approval of the study wastaken from administrators of Ministry ofHealth (MOH) in Mid-Delta governorates(Gharbia, Menofyia, Kafr El-Sheikh andDakahlia). Also, approval from managersof Tanta and Menofyia university hospitalswas taken. A verbal approval was takenfrom each participant to share in the study.Confidentiality was ensured.
RESULTS
Table (1) showed socio-demographic dataof study participants. Most of participants(47.42%) aged 20 to less than 25 years and28.87% aged 25 to less than 30 years.Males represented 22.68% while femalesconstituted 77.32%. About fifty fivepercent have less than 5 years of work,23.71% have less than 10 years of work and6.19% have 20 years or more of work.More than four hundred participants(46.39%) have bachelor degree, 50.52%have diploma and 3.09% have Masterdegree. Technicians including nursesconstituted 54.64% and 30.93% alliedhealth personnel. 65.98% of participants areworking in hospitals related to MOH.
Health workers have knowledge aboutCAM represented 75.26%. Only 4.12% ofparticipants usually use CAM and 38.14%sometimes use it. Different media was thesource of CAM knowledge for 360 ofknowledgeable participants (54.79%),relatives and friends were the source ofknowledge for 31.51%, health educationalorganizations 6.85% and books, lectures,workshops and internet only 6.85%. Only24.74% of participants talk on CAM withtheir patients and 28.87% advice patients to
use CAM. Minimal side effects of CAM isthe main cause of using it (43.29%)followed by religious beliefs (21.64%),effectiveness of CAM (17.13%), low cost(14.43%) and failure of conventionalmedicine (11.72%). Easy accessibility,acceptability and more confidence in CAMwere the cause for only 1.8% of participants(Table 2).
Table (2): Knowledge and causes of use ofCAM among studied population
Know
ledg
ean
d Ca
uses
of C
AM u
se
Num
ber
Perc
ent
Conf
iden
cein
terv
al
Knowledge about CAM (n=873)Participants haveknowledge
657 75.26 72.40-78.12
Participants have no orsome knowledge
216 24.74 21.88-27.60
Sources of knowledge (n=657)Media 360 54.79 50.98-58.60Relatives and friends 207 31.51 27.96-35.06Health educationalorganization
45 6.85 4.92-8.78
books, lectures,workshops and internet
45 6.85 4.92-8.78
Use of CAM for themselves or their familyParticipants usually useCAM
36 4.12 2.80-5.44
Participants sometimesuse CAM
333 38.14 34.92-41.36
Participants never useCAM
504 57.73 54.45-61.01
Talking on CAM withpatients
216 24.74 21.88-27.60
Advice patients to useCAM
252 28.87 25.86-31.88
Causes of CAM use*Minimal side effects 432 43.29 40.22-46.36Religious beliefs 216 21.64 19.09-24.19Effectiveness of CAM 171 17.13 14.79-19.47Low cost 144 14.43 12.25-16.61Failure of conventionalmedicine
117 11.72 9.72-13.72
Others# 18 1.80 0.97-2.63#Others include; easy accessible, acceptable andmore confidence.*Each participant may check more than one answer.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 39
The most common diseases for whichpatients use CAM were; backache, jointpain, abdominal colic and flatulence, kneepain, influenza and common cold, anxiety,migraine, hypertension, depression,diabetes mellitus, obstetric andgynaecological disorders (18.45%, 14.56%,12.62%, 10.36%, 8.09%, 7.12%, 6.8%,5.18%, 4.53%, 3.88% and 3.56%respectively). While the least diseases forwhich CAM used were renal failure, eyeinfection, asthma and cancer andmalignancy (1.62%, 1.29%, 1.29% and0.65% respectively) (Table 3).
The most commonly used CAM practicesby health workers were spiritual healing asprayer and roquia (73.2%), honey and beeproducts (65.98%), herbal products(47.42%), food supplements (45.36%),hijama (38.14%), acupuncture and massagetherapy (about 19%). Among CAMpractices rarely used; reflexology, energymedicine, magnetic therapy, ozone therapy,
aromatherapy, camel milk and urine andcauterization (Table 4).
DISCUSSION
Definition of CAM was explained to allparticipants in the current study beforefulfilling questionnaires to avoid confusionand misconception about CAM meanings.The sample technique was planned onscientific basis to be representative ofpopulation with low cost. The response ratewas 97.0% and this was high comparedwith the previous studies. However, therewere some limitations in the present study.It represented mid-Delta region only andhence results cannot be generalized to allEgyptian regions due to different cultures,habits and believes in different areas ofEgypt. At the same time, Lack of similarlocal studies on CAM makes it difficult toensure about the credibility of results.
Religious affiliations and prevailing localculture may be reflected in prevailing CAMpractices. Our studied health workersreported a high use of spiritual healing asprayer and roquia, honey and bee products,herbal products, food supplements andhijama, which are both highlighted healthpractices in the Holy Qura’n and HonoredSunnah. Studies from Saudi Arabia andGulf countries have, however, shown asimilar or slightly different situation.General Practitioners (GPs) in Doha, Qatarwere more familiar with diet therapy andfood supplements, acupuncture, andmassage,22 whereas in the United ArabEmirates (UAE) preference of healthprofessionals was given to herbal products,acupuncture, and homeopathy.21 On theother hand, Western countries show adistinctly different portrait of CAM use andknowledge of health workers: 86% hadknowledge of hypnosis, 79% ofacupuncture, 59% of homeopathy, 47% ofosteopathy, and only 19% of herbalmedicines.16
Table (3): Diseases for which CAM used
Diseases forwhich CAMused*
Number Percent Confidenceinterval
Backache 513 18.45 17.01-19.89
Joint pain 405 14.56 13.25-15.87
Abdominalcolic andflatulence
351 12.62 11.39-13.85
Knee pain 288 10.36 9.23-11.49Influenza &common cold
225 8.09 7.08-9.10
Anxiety 198 7.12 6.16-8.08Migraine 189 6.8 5.86-7.74Hypertension 144 5.18 4.36-6.00Depression 126 4.53 3.76-5.30Diabetesmellitus
108 3.88 3.16-4.60
Obstetric &gynecologicaldisorders
99 3.56 2.87-4.25
Renal failure 45 1.62 1.15-2.09Eye infection 36 1.29 0.87-1.71Asthma 36 1.29 0.87-1.71Cancer andmalignancy
18 0.65 0.35-0.95
*Each participant may check more than oneanswer.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 40
In the current study, 24.74% reported poorknowledge about CAM compared with39% of the general practitioners in Doha,Qatar.22 In a study among fellows of theMichigan chapter of the AmericanAcademy of Paediatrics, majority ofpaediatricians believed a small percentageof their patients were seeking alternatives toconventional medicine, half would considerreferring patients for CAM.23
Our study findings of 57.73% of healthworkers never utilized CAM is very similarto the reported CAM utilizationworldwide.24,25 The present study showedthat 28.87% of health workers advisepatients to use CAM and 24.74% ofphysicians talk with their patients on CAM.Some recent surveys reported a similarpattern.26,27 Our low rates may be attributedto the absence of specific CAM centers inEgypt like The NCCAM in USA and KSAand the lack of knowledge and training ofphysicians in CAM. Recognition orlegitimization of certain CAM practicesmay encourage physicians to advise andrefer patients to CAM practitioners.28 Only24.74% of physicians in the present studyinitiated a discussion of the potential harmand benefits of CAM therapies with their
patients, which is in agreement withpublished data.29,30
Among causes of CAM use in the presentstudy was agreement of health workersabout safety (43.29%) and effectiveness(17.13%). Primary health care physicians inSaudi Arabia reported agreement rates of23.36% and 28.93% for safety and efficacyof CAM therapies, respectively, which issimilarly to the majority of Dutch GPs whodid not believe in the effectiveness of manyalternative therapies, particularly herbalmedicines and nutritionalsupplementation.31 The physicians’agreement about safety and effectivenessvaries from one country to anotherdepending on culture, knowledge, andlegitimacy in a country. Unavailability ofreliable information, data, and evidence areall important factors for the widespreadlack of belief and confidence in CAMwithin the medical profession.16
Different media, relatives, and friends asmain sources of CAM knowledge for healthworkers in our study are considereddevastating. Of health professionals in thepresent study, only 6.85% take theirknowledge from educational academies
Table (4): Most important CAM modalities used by health workers
CAM modalities Commonlyused
Usuallyused
Neutral Sometimes used Rarely used
No. % No. % No. % No. % No. %Spiritual healing asprayer and roquia
639 73.2 72 8.24 108 12.37 18 2.06 36 4.12
Honey and beeproducts
576 65.98 189 21.65 63 7.22 9 1.03 36 4.12
Herbal products 414 47.42 171 19.59 162 18.56 63 7.22 63 7.22Food supplements 396 45.36 171 19.59 81 9.28 90 10.31 135 15.40Hijama 333 38.14 153 17.53 99 11.34 153 14.43 162 18.56Acupuncture 171 19.59 162 18.56 144 16.49 162 18.56 243 27.89Massage therapy 162 18.56 135 15.46 171 19.59 162 18.56 243 27.89Cauterization 117 13.4 135 15.46 162 18.56 171 19.59 828 32.99Camel urine and milk 90 10.31 36 4.12 72 8.25 54 6.19 621 71.13Aromatherapy 45 5.15 81 9.28 144 16.49 144 16.49 459 52.54Ozone therapy 36 4.12 63 7.22 117 13.4 180 20.62 477 54.64Magnetic therapy 36 4.12 63 7.22 72 8.5 171 19.59 631 60.82Energy therapy 27 3.09 45 6.19 72 8.25 153 17.53 567 64.95Reflexology 27 3.09 18 2.06 45 5.15 162 18.56 621 71.13

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 41
compared with 29.08% of healthprofessionals in Saudi Arabia. This mayindicate lack of medical curricula in CAM.In addition, 6.85% of participants take theirknowledge from books, lectures, workshopsand internet. This was unexpected wheremany licensed electronic databases (e.g.Natural Medicine ComprehensiveDatabase, http://www.naturaldatabase.com)have been available several years ago.Therefore, educational campaigns shouldbe initiated through lectures, seminar seriesand other activities demonstrating andhighlighting the tools associated with thosedatabases. The surge of informationavailable to the public in the media and theinternet is reflected on patients’ need forguidance and direction. Physicians may bea source of such knowledge as they areturned to frequently by some of theirpatients for seeking advice.14
CONCLUSION ANDRECOMMENDATIONS
There is an increasing interest in CAMknowledge among health workers. Most ofthem depend on the media, relatives andfriends as their main sources ofinformation. Most of physicians arereluctant in talking with their patients onCAM or referring patients to CAMpractitioners. Safety, religious beliefs,effectiveness, low cost and chronic pain areimportant determinant factors for seekingalternative care. Religious practices as asprayer and roquia, honey and bee products,herbs and hijama are the most prevalentCAM practices in the area. Provision oftuition, educational courses, continuingmedical education and postgraduateeducational opportunities on CAMmodalities are essential. Evidenced sourcesof CAM information must be available andeasily accessible for health workers.
REFERENCES
1. National Institute of Health: What iscomplementary and alternative medicine
(CAM)? NCCAM. January 201 Availableat nccam.nih.gov/health/whatiscam .
2. Goldbeck-Wood S, Dorozynski A, Lie LG,Zinn C, Josefson D, Ingram M.Complementary medicine is boomingworldwide. BMJ. 1996; 313:131-133.
3. Rasmussen NK, Morgall JM. The use ofalternative treatments in the Danish adultpopulation. Complementary Med Res.1990; 4:16-22.
4. Vaskilampi T, Merilainen P, Sinkkonen S,et al. The use of alternative treatments inthe Finnish adult population. In: LewithGT, Aldridge D, eds. Clinical ResearchMethodology for ComplementaryTherapies. London, England: Hodder andStoughton 1993; 204-229.
5. MacLennan AH, Wilson DH, Taylor AW.Prevalence and cost of alternative medicinein Australia. Lancet. 1996; 347:569-573.
6. Millar WJ. Use of alternative health carepractitioners by Canadians. Can J PublicHealth. 1997; 88:154-158.
7. Bannerman RH. Traditional Medicine andHealth Care Coverage. Geneva,Switzerland: World Health Organization;1993.
8. WHO Traditional Medicine Strategy 2002–2005. May 2002. Available at:http://www.who.int/medicines/organization/trm/orgtrmmain.shtml
9. MacLennan AH, Wilson DH, Taylor AW.The escalating cost and prevalence ofalternative medicines. Prev Med 2002;35:166-73.
10. Bodeker G. Planning for cost-effectivetraditional health services. In: TraditionalMedicine. Better Science, Policy andServices for Health Development.Proceedings of a WHO InternationalSymposium, Awaji Island, Japan 11–13September 2000. Kobe, Japan: WHO KobeCentre; 2001:31–70.
11. Wootton JC, Sparber A. Surveys ofcomplementary and alternative medicine,part IV: use of alternative andcomplementary therapies forrheumatological and other diseases. JAltern Complement Med. 2001; 7:715–721.
12. Ernest E. The role of complementary andalternative medicine. BMJ 2000; 321:1133-1135.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
CAM use among health workers in mid-Delta, Egypt, Ahmed T ElOlemy et al. 42
13. Ernest E. Obstacles to research incomplementary and alternative medicine.MJA 2003; 179(6):279-280.
14. Frenkel MA, Borkan JM. An approach forintegrating complementary-AlternativeMedicine into primary care. J Fam Pract2003; 20(3):324-332.
15. Huang N, Chou Y-J, Chen L-S, Lee C-H,Wang P-J and Tsay J-H. Utilization ofWestern Medicine and Traditional ChineseMedicine Services by Physicians and TheirRelatives: The Role of TrainingBackground. Evid Based ComplementAltern Med 2009; 6(3): eCAM AdvanceAccess 10.1093/ecam/nep094
16. Fujiwara K, Imanishi J, Watanabe S, OzasaK, Sakurada K. Changes in Attitudes ofJapanese Doctors toward Complementaryand Alternative Medicine: Comparison ofSurveys in 1999 and 2005 in Tokoyo. EvidBased Complement Altern Med 2009; May21:e1-e7.
17. Münstedt K, Harren H, von Georgi R,Hackethal A, Med Wieku Rozwoj.Complementary and Alternative Medicine:Comparison of Current Knowledge,Attitudes and Interest among GermanMedical Students and Doctors. Evid BasedComplement Altern Med 2008; Dec 20:e1-e7.
18. Sewitch MI, Cepoiu M, Rigillo N andSproule D. A Literature Review of HealthCare Professional Attitudes TowardComplementary and Alternative MedicineStudies. Complementary Health PracticeReview. 2008; 13(3):139-154
19. El-Olemy A, AlBedah MN. PublicKnowledge, attitude and practice ofcomplementary and alternative medicine inRiyadh region, Saudi Arabia. Oman Med J2012; 27(1):20-26.
20. Al-Faris EA, Al-Rowais N, Mohamed AG,Al-Rukban MO, Al-Kurdi A, Al-Noor MA,et al. Prevalence and pattern of alternativemedicine use: The results of a householdsurvey. Ann Saudi Med 2008;1:4-10.
21. Hassan MY, Das M and Bahjat S.Alternative medicine and the medicalprofession: views of medical students andgeneral practitioners. EasternMediterranean Health Journal. 2000;6(1):25-33.
22. Al Shaar AM, Ismail MFS, Yousufi AA,Salama RE: Knowledge, attitudes andpractice of general practitioners towardscomplementary and alternative medicine inDoha, Qatar. East Mediterr Health J2010;16:522–527.
23. Sikand A, Laken M. Pediatricians'Experience With and Attitudes towardComplementary/Alternative Medicine.Arch Pediatr Adolesc Med. 1998;152:1059-1064.
24. Ismail A, Chan SC: Knowledge andpractice of complementary medicineamongst public primary care clinic doctorsin Kinta district, Perak. Med J Malaysia2004;59:4–10.
25. Rooney B, Fiocco Guy, Hughes P, HalterS: Provider attitudes and use of alternativemedicine in a Midwestern medical practicein 2001. WMJ 2001; 100:27–31.
26. Wahner-Roedler DL, Vincent A, Elkin PL,Loe¬hrer LL, Cha SS, Bauer BA:Physicians’ attitudes towardscomplementary and alternative medicineand their knowledge of specific therapies: asurvey at an academic medical center. EvidBased Complement Alternat Med June2006;3:495–501.
27. Kurtz ME, Nolan RB, Rittiger WJ: Primarycare physicians’ attitudes and practicesregarding com¬plementary and alternativemedicine. JAOA 2003; 103:597–602.
28. Berman BM, Singh BB, Hartnoll SM,Singh BK, Rielly D: Primary carephysicians and complementary-alternativemedicine: training, attitudes, and practicepatterns. J Am Board Fam Pract 1998;11:272–228.
29. Busse JW, Heaton G, Wu Ping, Wilson KR,Mills EJ: Disclosure of natural product useto primary care physicians: a cross-sectional survey of naturopathic clinicattendees. Mayo Clin Proc 2005;80: 616–623.
30. 24 Corbin Winslow L, Shapro H:Physicians want education aboutcomplementary and alternative medicine toenhance communication with their patients.Arch Intern Med 2002;162:1176–1181.
31. Leach MJ: Public, nurse and medicalpractitioner attitude and practice of naturalmedicine. Complement Ther NurMidwifery 2004;10:13–21.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
How Many Subjects Should Be Studied, Waqas Sami, et al. 43
HOW MANY SUBJECTS SHOULD BE STUDIED:SAMPLE SIZE DETERMINATION THROUGH HYPOTHESIS
TESTING AND CONFIDENCE INTERVAL*Waqas Sami1, Mohammed O. Al-Rukban2, Mohammed Almansour3, Tayyaba Waqas4,
Kamran Afzal5, Rehan Asad6
ABSTRACT
One of frequently asked question by health researchers is how many individuals will I needto study. Sample size determination is one of the central canons of health research. A studyis always better when planned scientifically and determining the sample size for a study is aprime component as it will help to determine optimum number of subjects so that statisticallysignificant results can be detected. If the sample size is larger than what is needed, the studywill become cumbersome and ethically exorbitant. On the converse, using too few subjects’will eventually result in wasted time, effort and money etc. Literature is full of examples inwhich sample size is incorrectly determined for health studies thus resulting in biasconclusions. To ensure the reliability of the results, the significance level and power of studymust be fixed before the sample size determination. Sample size determination is veryimportant and always a difficult process to handle. It requires the collaboration of aspecialist who has good scientific knowledge in the art and practice of medical statistics.There are numerous situations in which sample size is determined that varies from study tostudy. This article will focus on the sample size determination for hypothesis testing andconfidence interval situations commonly used in health studies.KEY WORDS: Hypothesis testing, confidence interval, significance level, power of study,effect size, sample size
:ملخصالعیینةحجمفإنولذلك".الدراسة؟بھذهللقیامنحتاجمشاركاكم"ھوالصحیینالباحثینمنالمتكررةاألسئلةأھممنواحداإلحصائیةنتائجھافيمصداقیةوأكثرأفضلالدراسةماتكونفدائما,رصینعلميببحثللقیاماألساسیةالركائزمنیعتبر
العینةحجمكانلدراساتبنماذجملیئةالعلمیةوالمصادراألدبیاتإن. علميأساسعلىالعینةحجمإختیاربنيإذاالسھلباألمرولیسمھمالمناسبالعینةحجمإختیارفإنولذلك,الدراسةجدوىعدمفيسبباانقصأوزیادةالغیرمناسب
.الحیوياإلحصاءفيوالمختصالدراسةتحتھتنطويالذيالفنفيالخبیربینتعاونیحتاجفھوفيالثقةفاصلوضعدوتحدیالبحثفرضیةإلختبارالعینةحجملتحدیدالمناسبةالطریقةعلىالتعرف:الدراسةھدف
.الصحیةاألبحاث
Received: 2 April, 2013; Accepted: 12 June, 2013
*Correspondence: [email protected] of Biostatistics, Department of Public Health & Community Medicine, College of Medicine,Majmaah University, Saudi Arabia, 2Professor of Family Medicine, King Saud University, Saudi Arabia.3Assistant Professor of Family Medicine, College of Medicine, Majmaah University, Saudi Arabia.4Biostatistician, Punjab Institute of Cardiology Lahore, 5Lecturer of Physiology, Department of BasicMedical Sciences, College of Medicine, Majmaah University, Saudi Arabia. 6Assistant Professor ofAnatomy, Department of Basic Medical Sciences College of Medicine, Majmaah University, Saudi Arabia

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
How Many Subjects Should Be Studied, Waqas Sami, et al. 44
INTRODUCTION
Progress in almost every field of sciencedepends upon the contributions made bysystematic research, thus research is oftenviewed as the cornerstone of scientificprogress.1 A scientific research is a onewhich is a carefully planned investigation,addressing all the important aspects; fromgeneration of research ideas till thepublication.2 The ever increasing demandfor research has created a need for anefficient method of determining the samplesize to be representative of a givenpopulation3. Sample size determination is aprocess of deciding before a study begins,how many subjects should be studied.Whatever type of research design is usedfor a study, the health researcher will facethe problem of sample size determination.4The sample size is now easily calculatedwith the help of computer statisticalprograms, but the principles underlying thecalculation and the limitations must beclearly understood by the investigators.5 Itis not necessarily true that the bigger thesample, the better the study. Beyond acertain point, an increase in sample size willnot improve the study in fact, it may do theopposite.6 Calculation of an appropriatesample size is usually dependent upon sixparameters; objectives of the study,variables of interest (qualitative orquantitative), desired significance level,desired power, effect size / clinicalimportant difference, measurementvariability and one tailed or two tailedtests.7 Although a biostatistician may do thenecessary exercise to determine the samplesize, he/she can only do it with guidancefrom the investigator on the level ofuncertainty that is considered acceptable.8In addition, the aforementioned sixparameters have to be taken intoconsideration while calculating the samplesize. Since the data are not available beforethe study begins, the investigators will haveto make some assumptions about the data,and provide these assumptions to the
biostatistician to be able to calculate thedesired sample size. The procedure forestimating sample size is not as precise asinvestigators may be led to think. One suchassumption is about the prevalence,incidence or frequency of the condition orevent. If the rate of the event is large,statistical power will be high with a smallernumber of cases. If the event is rare, alarger sample size will be needed. Someinformation may be available from previousstudies to guide the estimates. If not, it is upto the investigators to come up with atentative estimate which the biostatisticiancan use.9-11 The ability of a study todemonstrate an association or causalrelationship between two variables giventhat an association exists is known as powerof study, for example, 80% power in aclinical trial means that the study has an80% chance of ending up with a p value ofless than 5% in a statistical test.12 The effectsize in a study refers to the actual size of thedifferences observed between groups or thestrength of relationships between variables.The likelihood that a study will be able todetect an association between a predictorand an outcome variable depends on themagnitude of the association we decide tolook for. The choice of effect size isdifficult and arbitrary, but it must be setbeforehand and must make a meaningfuldifference.13,14 There are numeroussituations in which sample size isdetermined that varies from study to study.This article will focus on the sample sizedetermination for hypothesis testing andconfidence interval situations commonlyused in health studies.
Various effects while determining thesample size15:
The information below is a guideline abouthow sample size is affected by variationsthat incur due to change in differentparameters.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
How Many Subjects Should Be Studied, Waqas Sami, et al. 45
Values for power of study andsignificance level9:
Power of study and significance level’s arethe core components for determiningsample size. Earlier, it was cumbersome tocalculate the power of study andsignificance level due to complex formulasand tables respectively, but now due torecent advancements in the field, expertshave prepared tables of normal deviates forcorresponding exact values of power ofstudy and significance level.
Sample Size Determination throughHypothesis Testing approach:
One Group Proportion:One group proportion is use to compare ahypothesized value of population with thesample value, for example, Drug A isadministered to 100 patients to treat aparticular disease, after administration thehealth of 50 patients improved. Testwhether this drug is better than drug B,which is known to produce improvement in45% of patients.
Example for sample size determination:The five-year cure rate for a particularcancer is reported in the literature to be50%. An investigator wishes to test thehypothesis that this cure rate can be appliedin a certain local health district. What is therequired sample size if the investigator isinterested in detecting a true rate of 40%.The level of significance is set at 5% with90% power of study.
Formula for determination of sample sizefor one group proportion is4:
Where;P1 is the anticipated proportion = 40%Po is the Null Hypothesis value or actualproportion (test cure rate) = 50%p1– po is the difference between proportions= 0.10Z 1 – β is the desired power of study = 90%Z 1-α/2 is the desired level of significance =5%Alternate hypothesis is two sidedPutting the values in the formula therequired sample size is 259.
Two Groups Proportion:Compares responses in two groups but theresponses in both groups are independent,for example, two preparations of same drugin tablet form were tested for their efficacyin alleviating headache. Preparation A wasgiven to 25 patients of which 17 claimingits effectiveness, while drug B was given to20 patients of which 16 claiming itseffectiveness. Compare the effectiveness ofpreparation A and B.
Example for sample size determination:It is believed that the proportion of patientswho developed complications afterundergoing one type of surgery is 5% whilethe proportion of patients who developedcomplications after second type of surgeryis 15%. How large should be the samplesize in each of the two groups of patients ifthe investigator wishes to detect with apower of 90% at 5% level of significance.
Formula for determination of sample sizefor two group proportion is19:
Table 2: NormalDeviates α values
Table 1: NormalDeviates 1-β values
2
21112
21
221112/1
pp
ppppZppZn
221 pppWhere
2)(
2)1()1(
1
2/1111
o
oo
pp
ppZppZn

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
How Many Subjects Should Be Studied, Waqas Sami, et al. 46
Where;P1 and P2 are the anticipated proportions =5% & 15%p1– p2 is the difference between proportions= 10%Z 1 – β is the desired power of study = 90%(1.28)Z 1-α/2 is the desired level of significance =5% (1.96)P is the average of proportions = 0.10Alternate hypothesis is two sided
Putting the values in the formula therequired sample size is 93 patients in eachgroup.
Paired Groups Proportion:Two proportions are paired if they share acommon feature that affects the outcome.For example, when comparing twolaboratory methods (culture media) todetect bacteria in samples of blood, if bloodfrom the same sample is put into bothmethods, this is the "pairing". Pairs ofresults from multiple samples can then becompared as a pair of proportions:
Example for sample size determination:Two drugs A and B were used to treatpatients of depression and were comparedin-terms of possible side-effects, nausea.The drugs were given to patients on twodifferent occasions. It is believed thatincidence of nausea from drug A is 20%less than drug B. Calculate the number ofpatients required in each group assuming90% power of study and 5% level ofsignificance.
Formula for determination of sample sizefor paired group proportion is20:
Where;P1 and P2 are the anticipated proportions =20% & 50%
p1– p2 is the difference between proportions= 30%Z 1 – β is the desired power of study = 90%(1.28)Z 1-α/2 is the desired level of significance =5% (1.96)P is the average of proportions = 0.35Alternate hypothesis is one sided
Putting the values in the formula therequired sample size is 47 participants.
Correlation:Correlation is the degree to which two ormore quantities are linearly associated. Thisassociation may be positive or negative. Apositive correlation exists where the highvalues of one variable are associated withthe high values of the other variable(s). A'negative correlation' means association ofhigh values of one with the low values ofthe other(s). For example, age and bloodpressure are positively correlated, whereas,volume and pressure and negativelycorrelated.
Example for sample size determination:According to the literature, the correlationbetween salt intake and systolic bloodpressure is around 0.3. A study isconducted to test the correlation in apopulation, with the significance level of1% and power of 90%. How manyparticipants should be there in the study?
Formula for determination of sample sizefor correlation is10:
Where:Z 1 – β is the desired power of study = 90%(1.28)Z 1-α/2 is the desired level of significance =1% (2.81)r is the correlation coefficient = 0.30
3
11log
41
2
212/1
rr
ZZN
e
221
22/
)())(1(
ppZZpp
n

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
How Many Subjects Should Be Studied, Waqas Sami, et al. 47
Putting the values in the formula therequired sample size is 158 participants.
Sample Size Determination through(Confidence Interval):There is only one method of determiningsample size that allows the researcher topre-determine the accuracy of the sampleresults that is “The Confidence IntervalMethod of Determining the Sample Size”.This method allows the investigator to drawconclusions about the true value of theoutcome measure on the basis ofinformation in the sample.16,17 The samplesize is calculated in such a way that there isa 95% probability that it includes the truevalue. To calculate the sample size fromconfidence interval the followinginformation is necessary; AnticipatedPopulation Proportion which is usuallyreported in the form of prevalence,incidence or rate etc. Confidence Level, tellsyou an estimated range of values that islikely to include the population parameterbeing calculated. For example, howconfident are we that our confidenceinterval of 23 – 27 years of age contains themean age of our population? If this range ofages was calculated with a 95% confidencelevel, we could say that we are 95%confident that the mean age of ourpopulation is between 23 and 27 years [18-
19]. Absolute or Relative Precision which isa measure of consistency i.e. if a survey isrepeated several numbers of times the sameresult is yielded every time; it is usuallyreported in percentage.20
Example for sample size determination(one group):A local health department wishes toestimate the prevalence rate of tuberculosisinfection among children less than fiveyears of age in its locality. How manychildren should be included in the sampleso that the rate may be estimated to within 5percentage points of the true value with95% confidence if it is known that the truerate is unlikely to exceed 20%.
Formula for determination of sample sizefor one group is18:
Where:Anticipated population proportion = 20%Confidence Level = 95%Precision = 5%(15% - 25%)
Putting the values in the formula therequired sample size is 244 children.
Example for sample size determination(two groups):Suppose that in a pilot study of 50agricultural workers in an irrigation project.It was observed that 40% had activeschistosomiasis. A similar pilot study of 50agricultural workers outside the projectdemonstrated that 32% had activeschistosomiasis infection. If we would liketo carry out a larger study to estimate thetrue schistosomiasis risk difference towithin 5 percentage points of the true valueof the confidence interval, how manypeople must be studied in each of the twogroups.
Formula for determination of sample sizefor two groups is:
Where:Anticipated population proportion= 40% &32%Confidence Level = 95%Precision = 5%age points
Putting the values in the formula therequired sample size is 354 people in eachgroup.

ORIGINAL ARTICLE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
How Many Subjects Should Be Studied, Waqas Sami, et al. 48
Tips in calculation of sample size forConfidence Interval approach:For situations in which no anticipation ispossible a figure of 0.5 should be used. Ifthe anticipation is given in range the closestto 0.5 should be used. The sample sizerequired will be largest when P is equal to0.5 and in two groups calculation the largerproportion should be kept first.16
CONCLUSION
Sample size is best considered early in theplanning of a study. The accuracy of samplesize calculations depends on the accuracy ofthe estimates of the parameters used in thecalculations. Determining sample size isnecessary so that optimum numbers ofsubjects are available to achieve statisticallysignificant results. On the converse, If thesample size is larger than what is needed,the study will become cumbersome andethically exorbitant. For successfulresolution of sample size issue close andhonest collaboration of biostatisticians andsubject-matter experts is required.
REFERENCES
1. Waqas Sami, M. O. AlRukban, TayyabaWaqas, Rehan Asad, Kamran Afzal.Sample size determination in healthresearch. J Ayub Med Coll Abbottabad2012; 24:4.
2. Feinstein AR. Principles of medicalstatistics. Boca Raton 2003, Fla: CRC; 503.
3. Moher D, Dulberg CS, Wells GA.Statistical power, sample size, and theirreporting in randomized controlled trials.JAMA 1994; 272:122–124.
4. Naing, NN. Determination of sample size.Malaysian Journal of Medical Science2003; 10(2): 84-86.
5. Uitenbroek DG. Sample size: SISA—simple interactive statistical analysis.Available at:http://home.clara.net/sisa/samsize.htmlAccessed March 3, 2003.
6. Armitage P, Berry G, Matthews JNS. 2002,Statistical Methods in Medical Research,4th ed. Blackwell, Oxford.
7. Naing L, Winn T and Rusli BN. SampleSize Calculator for Prevalence Studies.2006. Available at:http://www.kck.usm.my/ppsg/stats_resources.htm
8. Bland M. An Introduction to MedicalStatistics, 2000, 3rd. ed. Oxford UniversityPress, Oxford.
9. Eng J. Sample size estimation: how manyindividuals should be studied? Radiology2003; 227: 309–13.
10. Gerstman BB. Basic Biostatistics: statisticsfor public health practice: 2008. Jones andBartlett Publishers, Sudbury,Massachusetts.
11. Van Belle G. Statistical Rules of Thumb.Wiley: 2002, New York, NY.
12. Moher D, Dulberg CS, Wells GA.Statistical Power, Sample Size, and TheirReporting in Randomized Controlled Trials.JAMA 1994; 272:122-124
13. Spiegelhalter DJ, Freedman LS, ParmarMKB. Bayesian approaches to randomizedtrials. In Bayesian Biostatistics. 1996, NewYork.
14. Fleiss JL. Statistical methods for rates andproportions. 2nd ed. New York, NY: Wiley,1981; 45.
15. Casagrande JT, Pike MC, Smith PG. Animproved approximate formula forcalculating sample sizes for comparing twobinomial distributions. Biometrics 1978;34:483–6.
16. Gardner, MJ., Altman D.G. Statistics withconfidence-confidence intervals andstatistical guidelines. British MedicalJournal 1986; 5:1-13.
17. Daniel WW. Biostatistics: A Foundation forAnalysis in the Health Sciences. 1999, 7thedition. New York: John Wiley & Sons.
18. Lwanga, SK., and Lemeshow, S. Samplesize determination in health studies: Apractical manual. 1991, World HealthOrganization, Geneva.
19. Chan YH. Randomized Control Trials: Themagic number. Singapore Med J 2003; vol44(4): 172 – 174.
20. Schulz KF, Grimes DA. Sample sizecalculations in randomized trials:mandatory and mystical. Lancet 2005; 365:1348–53.

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Ultrasound & Phonophoresis Effect on Eczema Lesions, Jaya S Tedla 49
ULTRASOUND AND PHONOPHORESIS EFFECT ON ECZEMALESIONS IN A 37-YEAR-OLD MALE PATIENT:
A SINGLE CASE STUDY*Jaya S Tedla1, Irshad Ahmad2
ABSTRACT
Eczema is a very common form of the dermatological condition with painful lesions andultrasound is most commonly used electrotherapy modality by physical therapist to providetissue healing. In this case study, we have treated two such lesions on the left ankle for a 37-year-old patient with ultrasound and phonophoresis. Ultrasound alone was provided tolateral lesion on the ankle. Phonophoresis was provided to the anterior lesion on the ankle.Outcome measures were pain, swelling, itching, redness, litchenification and quality of life.We have seen improvements in the clinical features of both lesions but the anterior lesionwhere we provided phonophoresis had shown more effect that plain ultrasound.
كأكثرالصوتیةفوقالموجاتوتستخدممؤلمةجروحعليتحتويالتيالجلدیةاالمراضمنجداشائعشكلھواألكزیما٣٧العمرمنیبلغمریض عالجنافقد،الحالةھذهفي. األنسجةلشفاءالطبیعيالعالجأخصائيقبلمنشیوعاالطرق
فوقوبالموجاتفقطالصوتیةفوقبالموجاتالمعالجةتمت, األیسرحلالكاعلىالجروحھذهمناثنینیعاني منو عاما( الطرفيللجرحفقطالصوتیةفوقالموجاتاستخدمت) . phonophoresis(ھایدروكورتیزونمرھممعالصوتیة. احلللكاالماميجرحللphonophoresisھایدروكورتیزونمرھممعالصوتیةفوقالموجاتوللكاحل) الوحشيالسریریةالعالماتعلىتحسنشھدنالقد. للنتائجكمقاییسالحیاةونوعیة, التلین, االحمرار, الحكاك, التورم, االلماستخدم
نتائجمنافضلنتائجأظھرتقدفphonophoresisالفیھااستخدمناوالتياألمامیةاالصابةولكنالجرحینلكالقطفالصوتیةفوقالموجاتاستخدام
INTRODUCTION
Eczema is a broad term used to designate avariety of skin conditions that cause anitchy, inflamed skin rash.1 It is a verycommon form of the dermatologicalcondition2 and extensively studies inliterature.3 Eczema is broadly classified intotwo types exogenous (contact) andendogenous (non - contact). The clinicalfeatures are varied for each sub-type ofeczema, but the features common to mostpatterns divided into three stages, i.e. acute,sub acute and chronic.4 In acute stage thereare erythema, epidermal swelling, orvesciculation, papules, blisters, oozing orcrusting.
In sub-acute stage along withabove featuresthere will be scaling. In chronic stages theskin is scaly, hypo or hyper pigmented andthickened. As the condition persists, theskin reaches to a dry leathery thickenedstage called litchenification, with increasedskin markings and painful fissuressecondary to scratching or rubbing.2,5
Ultrasound is commonly used as adiagnostic method, operative tool andtherapeutic intervention.6 Ultrasound is themost widely used therapeutic modality inphysical therapy departments throughoutthe world.7-12 The major effects ofultrasound are divided into thermal and
Received: 9 April, 2013; Accepted: 22 June, 2013*Correspondence: [email protected] Professor, Department of Medical Rehabilitation, College of Applied Medical Sciences, King KhalidUniversity, Abha, Kingdom of Saudi Arabia. 2Lecturer at Department of Medical Rehabilitation, College ofApplied Medical Sciences, King Khalid University, Abha, Kingdom of Saudi Arabia.

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Ultrasound & Phonophoresis Effect on Eczema Lesions, Jaya S Tedla 50
nonthermal effects. The thermal effects aredue to increased tissue temperature thisleads to increase in blood flow, increasedmetabolic activity, and analgesic effect onnervous system results in improvements inhealing and pain relief.13 The non-thermaleffects include cavitation andmicrostreaming that are useful for alteringthe cellular function and make it moreuseful for tissue healing.
CASE DESCRIPTION
Patient history
The subject chosen in this case study is amale 37-year-old Asian originated fromIndia, but currently residing in theKingdom of Saudi Arabia. He had chroniceczema with inflamed painful fissures at theankle region on the anterior and lateralaspect of the left ankle. The itching was sosevere in the night disturbing his sleep;unknowingly he used to scratch it in thenight leading to an inflamed fissure. Torelieve his symptoms he was prescribed atopical hydrocortisone cream, but it was notdecreasing his problems even after manyweeks of application. He consulted physicaltherapy department casually for hisproblem. Discussing his condition wedecided to provide him effective drugdelivery into the cutaneous system by usingan ultrasound technique calledPhonophoresis.
Examination
After obtaining the written consent form,treatment protocol was explained to him.Following this procedure, we started withthe clinical examination of symptoms onvisual analog scores. Each symptom visualanalog score was assessed on a 10cm linewithout any markings. The left-hand sidestarting point was denoted with ‘0’ whichindicates no symptom at all and right handsides ending point was denoted by number‘10’ which indicates maximum symptomswhich they cannot tolerate (Figure-1).
No symptom ‘0’_________ ‘10’ Maximumat all symptom
Figure -1 : Sample of visual analog scale
The subject was asked to tick any point ofthe line. After ticking, the length of the linefrom ‘0’ to the tick mark was measured byscale and distance was noted in centimeters.This kind of VAS was assessed for all thefollowing clinical features, i.e. pain,swelling, itching, redness, litchenificationand quality of life. The scores of all thesesymptoms related to eczema are provided intable-1.
Figure 2: Pre and post phonophoresis treatmentfor anterior eczema lesion
Table-1: VAS scores of clinical characteristics,pre and post intervention
Clinicalcharacteristics
Ultrasound forlateral lesion
Phonophoresisfor anteriorlesion
Pre Post Pre Post
Pain 7 0.5 6.2 0
Swelling 8.7 0.9 8 0
Itching 10 6.4 8.7 0.6
Redness 10 4.8 6.8 1
Litchenification 10 5.6 8.3 1
Quality of life 10 6 7.7 0.4

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Ultrasound & Phonophoresis Effect on Eczema Lesions, Jaya S Tedla 51
Figure 3: Pre and post ultrasound treatment forlateral eczema lesion
Treatment MethodWe choose Enraf-Nonius™ ultrasoundmission for both phonophoresis and plainultrasound treatment. For phonophoresisthe frequency of ultrasound was 1MHz,mode continuous, intensity 0.8 w/cm2 forthe anterior lesion on the ankle withhydrocortisone ointment prescribed by theclinician to him. We mixed the ultrasoundgel and cream thoroughly, and applied ontothe skin and set the apparatus withappropriate settings discussed above andapplied for five minutes on the first day andincreased one minute every day for fivedays in a week reached a duration of 10minutes. Treatment continued same 10minutes of duration for five days in the nextweek as well. The other lesion on the lateralaspect of the ankle was treated with plainultrasound of 1MHz frequency, pulsedmode 1:4, intensity 0.8 w/cm2 for the sameduration of the anterior lesion. Totalfrequency of treatment is 10 days in twoweeks. Post treatment we have seenimprovements in both of the lesions, butanterior lesion with phonophoresis hadshowed better results than plain ultrasoundalone. We present both the lesion pre andpost photographs and scores in figures-2, 3and table -1 respectively.
DISCUSSION
The major clinical problem with eczema areinflamed lesion with pain, swelling, itching,redness, scaling and disturbed life. As the
thermal effects of ultrasound increase thelocal blood flow [14]. The substanceswhich precipitate inflammation will bewashed off and all the signs ofinflammation that is swelling, pain, andredness will be decreased.
Therapeutic ultrasound alters the plateletmembrane permeability leading to releaseof serotonin and it also stimulates therelease of macrophages and neutrophils.15
Therapeutic ultrasound can alter thepermeability of various ions especiallycalcium,16,17 by increasing the intracellularcalcium there will be mast celldegranulation and which releases histaminein the surrounding tissues.18 These are theimportant steps in inflammatory phase oftissue healing by which there will beadequate readiness of the system for therepair process.
In the second phase of tissue repair, theultrasound is pro-proliferative bystimulating fibroblasts, myofibroblasts andendothelial cells.15 It maximizes theproliferative phase of tissue repair andenhances optimal scar formation.15 Theultrasound is even effective in scarremodelling during this phase of tissuerepair it acts on collagen in terms ofappropriate orientation and conversion oftype-3 collagen to type-1 by this there willbe increased tensile strength and scarmobility.15 By all these cellular changes,the ultrasound helps in all phases of tissuerepair this may be the reason for healing ofthe lesion and decreased symptoms.
Phonophoresis is defined as transferringchemical molecules in to skin by usingultrasound19. In our study, one of the lesionwas applied phonophoresis usinghydrocortisone topical cream. This lesionhas shown better effect than the plainultrasound. This can be due to additionalanti-inflammatory effect of the steroidalong with the usual effects of ultrasounds.In future, we recommend multi centric

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Ultrasound & Phonophoresis Effect on Eczema Lesions, Jaya S Tedla 52
randomized controlled trial with largesample to prove the effectiveness ofultrasound and phonophoresis on eczemarelated lesions.
CONCLUSION
Application of ultrasound on eczema isinnovative mode of physical therapyapplication in dermatological conditions. Inour case study we have seen improvementsin the eczema related clinical problems withplain ultrasound as well as withphonophoresis. But phonophoresis wasbetter than ultrasound in this patient. Infuture we require further research toultimately conclude these effects.
REFERENCES
1. Haggerty M. Atopic Dermatitis. In: TheGale Encyclopedia of Medicine edited byLonge JL. Volume – 1, 3rd Edition, Detroit,Gale. 2006:448-451.
2. Hunter JAA, Savin JA and Dahl MV.Eczema and Dermatitis in. ClinicalDermatology. London, Blackwell Science.1996:86-90.
3. Futamura M, Thomas KS, Grindlay DJC,Doney EJ, Torley D, Williams HC.Mapping Systematic Reviews on AtopicEczema-An Essential Resource forDermatology Professionals andResearchers. PLoS ONE 2013;8 (3):e58484. doi:10.1371/journal.pone.0058484.
4. Lawley LP, McCall CO and Lawley TJ.Eczema, Psoriasis, Cutaneous infections,Acne and other common skin disorders. In:Harrison’s principles of internal medicine.Edited by Longo DL et al. Volume - 1, 18thedition,. McGraw-Hill company U.S.A .2012.
5. Clark RAF and Hopkins TT. The othereczemas. In: Moschella and HurleyDermatology. Edited by Moschella et al.Volume – 1, 3rd edition, W.B saunderscompany, Pennsylvania U.S.A.1992.
6. Berna´-Serna JD, Sa´nchez-Garre J,Madrigal M, Zuazu I, Berna´-Mestre JD.Ultrasound therapy in rectus sheathhematoma. Phys Ther 2005;85:352–357.
7. Warden SJ, McMeeken JM. Ultrasoundusage and dosage in sports physiotherapy.Ultrasound Med Biol 2002;28:1075–1080.
8. Wong RA, Schumann B, Townsend R,Phelps CA. A survey of therapeuticultrasound use by physical therapists whoare orthopaedic certified specialists. PhysTher 2007;87:986–994.
9. Lindsay D, Dearness J, Richardson C, et al.A survey of electromodality usage inprivate physiotherapy practices. Aust JPhysiother 1990;36:249 –256.
10. Ter Haar G, Dyson M, Oakley S.Ultrasound in physiotherapy in the UnitedKingdom: results of a questionnaire.Physiotherapy Practice. 1988;4:69 –72.
11. Green J. Outpatient physiotherapy practicein osteoarthritis of the hip joint.Physiotherapy 1991;36:737–740.
12. Robinson AJ, Snyder-Mackler L. Clinicalapplication of electrotherapeutic modalities.Phys Ther 1988;68:1235–1238.
13. Baker KG, Robertson VJ, Duck FA. Areview of therapeutic ultrasound:biophysical effects. Phys Ther2001;81:1351-1358
14. John LD. Non thermal effects oftherapeutic ultrasound: the frequencyresonance hypothesis. J Athl Train 2002; 37(3):293-299.
15. Watson T, Young SR. TherapeuticUltrasound in; Electrotherapy evidencebased practice. Edited by Watson T. Twelthedition, Churchill Livingstone Elsevier,Philadelphia, USA 2008. pg 179-200.
16. Dinno MA, Dyson M, Young SR, MortimerAJ, Hart J, Crum LA. The significance ofmembrane changes in the safe and effectiveuse of therapeutic and diagnosticultrasound. Phys Med Biol1989;34(11):1543-52.
17. Mortimer AJ, Dyson M. The effect oftherapeutic ultrasound on calcium uptake infibroblasts. Ultrasound Med Biol1988;14:499-506
18. Fyfe MC, Chahl LA. Mast celldegranulation; A possible mechanism ofaction of therapeutic ultrasound. UltrasoundMed Biol 1982;8 (Suppl1):62.
19. Nancy N Byl. The Use of Ultrasound as anEnhancer for Transcutaneous DrugDelivery: Phonophoresis. Phys Ther 1995;75:539-553.

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Case Report Neuro-Behcet, Abdulrahman A Alduraywish 53
UNUSUAL PRESENTATION OF BEHCET DISEASE(NEURO-BEHCET)
*Abdulrahman A Alduraywish1
ABSTRACT
Behcet disease is a common disease and usually present by oral, genital ulcers. Can beaffect multiple systems in the body. CNS can be affect but usually after present of orogenitalulcer. In our case report, the patient present with neurological manifestations beforeorogenital ulcers, and that is rare presentation (less than 3 percent).
Key words: Behcet disease, neurobehcet disease, Vasculitis
أنالممكنومنالتناسلیةواألعضاءبالفمبتقرحاتعادةویظھرمنتشرومعروفمرضھوبھجتمرض:ملخص.العصبيالجھازضمنھاومنالمریضجسممنكثیرةأجزاءعلىیؤثر. التناسلیةواألعضاءالفمفيالتقرحاتظھوربعدعادةتظھرالعصبيالجھازأعراضلكنشيوھذاالتناسلیةواألعضاءالفمفيالتقرحاتظھورقبلالعصبيالجھازأعراضمناشتكىالمریضالحالةھذهفي
)%٣مناقل. ( الحدوثنادر
INTRODUCTIONBehcet’s disease is a multisystem,recurrent, inflammatory disorder.2 It wasfirst described by H. Behcet (1924) as athree-symptom complex comprising uveitis,oral aphthae and genital ulcerations. Later,in 1930, the Greek physician Adamantiadesreported a patient with inflammatoryarthritis, oral and genital ulcers, phlebitis,and iritis.1
Behcet disease can affect central nervoussystem in less than one- fifth of patient.There is, a period of approximately five tosix years elapsed between the onset of theearliest non-neurologic symptoms ofBehçet’s disease and the appearance ofneurologic symptoms or findings.Nevertheless, neurologic findings may alsoappear concurrently (7.5 %) or precedenon-neurologic features (3 %). Twentypercent of those with neurologic findingswere asymptomatic.3,4
DIAGNOSIS
CNS manifestation according to site oflesion, they are commonly present (>50%)by pyramidal signs, hemiparesis andheadach. Some patient present by brainstemsign, fever, paraparesis, meningeal sign(aseptic meningitis), movement disorder,sensory disturbance (10-40 % of case). Lesscommon manifestations (5% of case) likeseizure, cerebellar syndrome, opticneuropathy, psychiatry disorders maypresent.6 It can also present with asepticmeningitis or encephalitis, and Vasculitis.And occurs more commonly in male thanfemale.5
Coarse of disease can be recurrent attacks,primary progression or secondaryprogression.3
Received: 20 April, 2013; Accepted: 25 June, 2013*Correspondence: [email protected], Al jouf university, Faculty of medicine, MBBS, internal medicine Jordanian board

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Case Report Neuro-Behcet, Abdulrahman A Alduraywish 54
Neuro-Imaging: MRI
The lesion type during an acute attack isusually located in the basal ganglion regionor in the brainstem, extending to thediencephalic structures, in about 30% of thecases the lesion are bilateral. In some casesa mass effect may be noted, and the centreof these lesions shows contrastenhancement. And can be small scatteredlesions located in the basal ganglion region,brainstem or the internal capsule. In chroniccases, atrophy of the brainstem andenlargement of the third ventricledisproportionate to the lateral ventricles orcortical sulci can occurs.3
CSF examination:
Can be completely normal and can showpleocytosis and/or elevated protein content.CSFs with a high cell count, had eitherneutrophilic predominance or bothneutrophils and lymphocytes, orlymphocytic predominance.3
Management:
Neuro-behcet consider as life threateningcondition so we should treat the patientwith intensive immunosuppressant. Thecombination of high dose of glucocorticoidand another immunosuppressive agent (likeAzathioprine, Infliximab, and cyclosporine)is required.7,8
Aseptic meningitis may occur intermittentlyin-patient with behcet disease. In absenceof other manifestation usually treated withhigh dose of glucocorticoid with greatresponse.
In case of recurrent aseptic meningitis mayneed to use long-term maintenance therapywith another immunosuppressive agent likeazathioprine.9
CASE REPORT
A 21-year-old male Saudi presented tohospital initially with 12 days history ofheadache and fever, followed by 3 dayshistory of left sided body weakness, doublevision and inability to open right eye.
Fig 1: T2 flair (right basal gangliahyperintense signal)
Fig 2: T2 flair (left midbrainhyperintense signal)
There was no history of oral or genitalulcer, red or painful eye and seeing halos.No skin rashes and swollen or painful jointjoints.
There was no past history or family historyof similar condition.

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Case Report Neuro-Behcet, Abdulrahman A Alduraywish 55
O/E: Temp: 37.80C, BP: 125/85 mmHg,RR: 19 cpm. Pulse: 90
Patient was confused and slightly slow inmentation. Had left 3rd and 4th cranialnerve palsies with left hemiparesis andbilateral hyper-reflexia. Also had milddysmetria and ataxia over the right side,though was mobile without support. Othersystems including skin and musculoskeletalsystems were unremarkable, had no oro-genital ulcers, no evidence oflymphadenopathy
X-Ray Chest; unremarkable
CT brain was unremarkable.
MRI showed multiple signal change low T1bright T2 and flair sequences at right basalganglia, right parietal lobe, left occipitallobe and midbrain (Figure 1 and 2).
CSF-Analysis; Lumber Puncture was doneopening pressure was normal, WBC 200cell/mm3, 85% lymphocyte, 15%polymorph, protein 1.06 gm/L, sugar 2.3mmol/L. Gram stain and AFB stains werenegative, culture revealed no growth. PCRand C/S for mycobacterium was notavailable at the local hospital so it was sendout to the central laboratory butunfortunately no result could be obtainedlatter on.
CBC and routine Chemistry wereunremarkable. ESR and C-reactive proteinwere normal and ANA was negative.
Possibilities of CNS Tuberculosis, AcuteDemylenating Encephalomyelitis (ADEM),Vasculitis (Behcet’s disease) andSarcoidosis were thought off and patientwas started on steroids (dexamethasone 4mg TID then decrease to 2 mg BID atdischarge for 1 month then start tapering),and Anti-Tubercular drug(ATT).
Follow up; Patient improved clinically overperiod 2 weeks, MRI was repeated after one
month, which showed regression in the sizeand number of lesions (Figure 3 and 4).
Fig 3: T2 flair (improve midbrain lesion)
Fig 4: T2 (right basal ganglia lesionimprove)
Unfortunately, patient was not compliant tomedication and after 10 months had arelapse of his condition. This time patientalso reported oral ulcers but no genitalulcer, no visual symptoms or skinmanifestations.
Patient was confused, dysartheric, had rightside complete and left partial ptosis, pupil3mm bilateral reactive to light. Fundusexamination was normal also had right 6thnerve palsy. Had left hemiparesis (4/5weakness). Sensations were normal, Gait

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Case Report Neuro-Behcet, Abdulrahman A Alduraywish 56
was ataxic. No evidence of uveitis orretinitis. Chest, CVS and abdominalexamination was unremarkable
INVESTIGATIONCBC, Chemistry was unremarkable. ESR:15mm 1st hour, ANA was Negative andcomplements C3 and C4 were normal.Serology for HSV 1 & II, Brucellosis,VDRL and HIV was negative. PPD test andskin Pethargy tests were normal.
X-Ray Chest; unremarkable
MRI Brain and cervical Spine:Multiple T1 hypointense, T2 and flairhyperintense lesion were seen involvingbrainstem, thalamus, Cerebellar peduncleand left occipital lobe and basal ganglia.Some of the lesions were partially enhancedwith GAD contrast. Cervical spine wasunremarkable (Figure 5 and 6).
Cerebrospinal fluid (CSF):Opening pressure was Normal. WBC 60cells/cmm, 40% were polymorphs and 56%lymphocyte. Proteins; was 1 gm/ L.
Gram & AFB stains and culture werenegative.HLA-B52, Mycobacterium cultureand PCR were sent to central lab and resultcame negative.
In Differential Diagnosis this timesuspicion of Neuro Behcet’s disease wasvery high so again started on high dose ofsteroids (methylprednisolone 1g for 5 daysfollowed by prednisolone 50 mg and steroidsparing drug Azathioprine 50 mg for 1week then increase to 100 mg daily.
Hospital Course and Follow up:Patient again showed clinical recovery inabout 2 weeks. He was discharged on oralprednisilone 50 mg daily then tapering dosewith calcium, vitamin D supplementationand Azathioprine 100 mg daily.
Fig 5: T2 flair ( midbrain hyperintenselesion)
Fig 6: T2 flair (basal ganglia hyperintenselesion)
DISCUSSION
Our patient had a diagnostic challenge at 1st
presentation, as he presented withbrainstem, basal ganglia deficit andalteration of sensorium, fever and headacheof subacute to chronic course. It wassuggestive of subacute multifocaldisseminated and diffuse involvement ofCNS with progressive course. Initiallydiagnosis of Encephalitis, including ADEM(Acute disseminating encephalomyelitis),were thought of. Suspicion of CNS-

CASE REPORT MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
Case Report Neuro-Behcet, Abdulrahman A Alduraywish 57
Tuberculosis could not be ruled out,because of the clinical subacutepresentation with headache, fever.Neuroimaging, CSF findings weresuggestive and PCR and culture forMycobacterium were not available at ourhospital. However patient was started onHigh dose IV methyl prednisolone for5days with anti-tubercular (ATT) and anti-viral coverage, followed by oral steroids(dexamethasone) tapering dose.
Possibility of Vasculitis includingneurobehcet’s disease was remote at thisstage, as there were no other symptoms andsigns suggestive or fulfilling diagnosticcriteria. Anyhow, our patient was luckyenough to be started on steroids withoutdelay, though for treatment of ADEM andas adjunct with ATT. He was saved fromdevastating consequences of NeuroBehcet’s disease and made a good clinicalrecovery.
The relapse of his condition due to noncompliance to medications, the history oforal ulcer and pattern of lesions on MRIraised our index of suspicion furthertowards Vasculitis particularly NeuroBehcet’s disease. Furthermore, the anti-tubercular workup and serology forconnective tissue disease and infectionswas negative.
CONCLUSION
Neuro-Behcet can be devastating if leftuntreated, so it is very important to havehigh index of suspicion and this rarepossibility should be considered in thedifferential diagnosis of such cases.
REFERENCES
1. Adamantiades B. A case of recurrenthypopyon iritis. Medical Society of Athens.1930;586-93. Akman-Demir G, SerdarogluP, Tasçi B. Clinical
2. O'Duffy JD. Behçet's disease. [Review].Curr Opin Rheumatol 1994; 6: 39–43.
3. Akman-Demir G, Serdaroglu P, Tasçi B.Clinical patterns of neurologicalinvolvement in Behçet's disease: evaluationof 200 patients. The Neuro-Behçet StudyGroup. Brain 1999; 122 ( Pt 11):2171.
4. Al-Araji A, Kidd DP. Neuro-Behçet'sdisease: epidemiology, clinicalcharacteristics, and management. LancetNeurol 2009; 8:192.
5. Atasoy HT, Tunc TO, Unal AE, et al.Peripheral nervous system involvement inpatients with Behçet disease. Neurologist2007; 13:225.
6. International Study Group for Behçet'sDisease. Criteria for diagnosis of Behçet'sdisease. International Study Group forBehçet's Disease. Lancet. 1990;335(8697):1078-80.
7. Hatemi G, Silman A, Bang D, et al.EULAR recommendations for themanagement of Behçet disease. AnnRheum Dis 2008; 67:1656.
8. Barnes CG. Treatment of Behcet'ssyndrome. Rheumatology (Oxford) 2006;45:245.
9. azici H, Pazarli H, Barnes CG, et al. Acontrolled trial of azathioprine in Behçet'ssyndrome. N Engl J Med 1990; 322:281.

EDITORIAL POLICIES MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
58
EDITORIAL POLICY
We welcome all contributions that enhanceor illuminate medical sciences. In additionto scientific articles, letters, news, andcomments are welcome if they serve thepurpose of transfer of original and valuableinformation to our readers.
To give an equal publishing chance tomanuscripts from different environments,we will normally publish no more than twopapers by the same author or co-authorwithin one calendar year. This rule alsoapplies to editors. Also, we recommendauthors not to separate fragments of astudy into individual reports, but rather topresent a full report on the topic.
EDITORIAL PROCEDURE
The Editor-in-Chief reads everymanuscript received and assigns it ageneral priority level: (a) manuscripts sentto reviewers immediately; (b) manuscriptsreturned to authors with suggestions forthe improvement of data presentation; and(c) rejected manuscripts. Editors-in-Chiefread the revised manuscript. If themanuscript is improved adequately, it issent to two reviewers for extramuralreview and to the Statistical Editor, if itcontains numerical data. This editorialprocedure reinforces our author helpfulpolicy because all manuscripts undergoeditorial scrutiny and advice.
AUTHORSHIP
According to the International Committeeon Medical Journal Ethics (ICMJE), anauthor is defined as one who has madesubstantial contributions to the conceptionand development of a manuscript.Majmaah Journal of Health Sciencesadheres to the ICMJE guidelines(http://www.icmje.org/#author), whichstate that “authorship credit should bebased on all of the following: 1)substantial contributions to conception and
design, acquisition of data, or analysis andinterpretation of data; 2) drafting thearticle or advising it critically forimportant intellectual content; and 3) finalapproval of the version to be published.All submissions are expected to complywith the above definition. Changes to theauthorship list after submission will resultin a query from the publisher requestingwritten explanation.
SUBMISSION
Majmaah Journal of Health Sciencesaccepts all manuscripts on the strictcondition that they have been submittedonly to us, and had not been published inany other journal, nor are they underconsideration for publication or in presselsewhere. The journal adheres to the Codeof Conduct and Best Practice Guidelinesset forth by the Committee on PublicationEthics (COPE).
PEER REVIEW
All manuscripts will be subjected toconfidential peer review by experts in thefield and, on the basis of reviewers’feedback; papers will be acceptedunconditionally, accepted subject torevision or rejected.
ETHICS AND CONSENT
Do not use patients' names, initials, orhospital numbers, especially in illustrativematerial. Identifying information shouldnot be published in written descriptions,photographs, and pedigrees unless theinformation is essential for scientificpurposes and the patient (or parent orguardian) gives written informed consentfor publication. Informed consent for thispurpose requires that the patient be shownthe manuscript to be published.

EDITORIAL POLICIES MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
59
COPYRIGHT AND PERMISSIONS
It is a condition of publication that authorsassign copyright or license the publicationrights in their articles, including abstracts,to Majmaah Journal of Health Sciences.This enables us to ensure full copyrightprotection and to disseminate the article,and the Journal, to the widest possiblereadership in print and electronic formatsas appropriate. Authors may, of course,use the article elsewhere after publicationwithout prior permission from MajmaahJournal of Health Sciences, provided thatacknowledgement is given to the Journalas the original source of publication, and itis notified so that our records show that itsuse is properly authorised.
Authors are required to sign an agreementfor the transfer of copyright to thepublisher. All accepted manuscripts,artwork, and photographs become theproperty of the publisher. A copyrightagreement form can be downloaded bycorresponding authors of acceptedmanuscripts with proofs. This should besigned and returned to Majmaah Journal ofHealth Sciences.
Authors are themselves responsible forobtaining permission to reproducecopyright material from other sources.
DECLARATION OF INTEREST
It is the policy of Majmaah Journal ofHealth Sciences, to adhere in principle tothe Conflict of Interest policyrecommended by the ICMJE. All authorsmust disclose any financial and personalrelationships with other people ororganizations that could inappropriatelyinfluence (bias) their work. It is the soleresponsibility of authors to disclose anyaffiliation with any organization with afinancial interest, direct or indirect, in thesubject matter or materials discussed in themanuscript that may affect the conduct or
reporting of the work submitted. Allsources of funding for research are to beexplicitly stated. If uncertain as to whatmight be considered a potential conflict ofinterest, authors should err on the side offull disclosure. If there are no declarations,authors should explicitly state that thereare none. This must be stated at the pointof submission. Manuscript submissioncannot be completed unless a declarationof interest statement (either stating thedisclosures or reporting that there arenone) is included.
This will be made available to reviewersand will appear in the published article. Ifany potential conflicts of interest are foundto have been withheld followingpublication, the journal will proceedaccording to COPE guidance. The intent ofthis policy is not to prevent authors withany particular relationships or interestfrom publishing their work, but rather toadopt transparency such that reviewers,editors, the publisher, and mostimportantly, readers can make objectivejudgements concerning the work product.
POLICY FOR SUBMISSIONS BYMEMBERS OF THE EDITORIAL
TEAM
As all editors and Editorial Boardmembers are active professionals andresearchers, it may happen that they wouldwant to submit their articles to theMajmaah Journal of Health Sciences. Thisrepresents a potential conflict of interest,especially in cases of submissions fromdecision-making editors. In reviewingsubmissions from its editors and EditorialBoard members, we follows the guidelinesfor good editorial practice set byinternational editorial organizations, suchas World Association of Medical Editors(WAME;http://www.wame.org/resources/publication-ethics-policies-for-medical-journals#conflicts) and Committee on

EDITORIAL POLICIES MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
60
Publication Ethics (COPE;http://publicationethics.org/case/editor-author-own-journal).
The review of such manuscripts will not behandled by the submitting editor(s); thereview process will be supervised anddecisions made by a senior editor who willact independently of other editors. In somecases, the review process will be handledby an outside independent expert tominimize possible bias in reviewingsubmissions from editors.
REVIEW PROCESS
1. Authorship statement. Upon the receiptof the submission, authors will receivethe Authorship Statement form, whichshould be filled in, signed and returnedto the Editor. In this way, the authorsconfirm the originality of the report andvalidity of authorship, and assertcompliance with the review process, i.e,that he or she shall not withdraw thepaper until it is published or rejected.We advise the authors to promptly sendback the filled out authorshipstatements, or otherwise the editorialprocessing of the manuscript may bedelayed.
2. Pre-review (if necessary). One to threeweeks after submission of themanuscript, the author may receiveEditor’s letter with a copy of themanuscript with suggestions for theimprovement of data presentation. Thisis the manuscript pre-review. Theauthor should closely follow theinstructions, revise the manuscript, andsubmit the revised version.
3. Peer review. The Majmaah Journal ofHealth Sciences promotes expertrefereeing by peers as a best availablemethod for the maintenance ofstandards of excellence in the scientificcommunity, and is committed to
promoting its peer review quality andfairness, as well as its speed andefficiency. Authors are welcome tosuggest up to three potential reviewersfor their manuscript (excluding co-authors or collaborators for the lastthree years), or to ask for the exclusionof reviewer(s) and the reasons for it.The reviewers are asked to treat themanuscript with confidentiality, andreveal any research conflict of interestwith the reviewed manuscript.Reviewers do not have to sign thereview forms with suggestions to theauthors, but may do so if they wish.Within two months of submission of themanuscript, the authors will receive thereviews. The comments and suggestionsmade by the reviewers should beaddressed and closely followed. In thisrespect, the Editor’s accompanyingletter will give clear general instructionsfor further work on the manuscript.
4. Author’s cover letter accompanying therevised version of the paper. Theauthors should state clearly andprecisely every step taken in accordancewith the reviewers’ requests. Thedescription should be listed on anumbered basis, in the order ofreviewers’ comments. Alteredparagraphs in the new version of themanuscript should be specified usingpage and paragraph numbers. Paragraphon top of a page is considered No. 1,even if it does not begin on that page.
ACCEPTANCE CRITERIA
The reviewers are asked to apply highestinternational standards in their assessmentof the submitted work. The key advice onconcrete criteria that they receive fromeditors is to look for the originality ofwork and its importance/relevance to thesubject as a whole. If the article does notfulfil these primary criteria, it should notbe accepted. The articles which receive

EDITORIAL POLICIES MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No. 2
61
one or more reviewers’ recommendationsfor “major review,” are sent, after revision,with the respective author’s cover letter, tothe same reviewer, who makes the finalrecommendation on acceptance orrejection. To ensure the transparency ofthe editorial process and responsibilities ofall authors, the formal letter of acceptanceis sent to all authors on the manuscript,and not just to the corresponding author. Inthe case of rejection, the authors have theright to appeal if they think that thereviewers did not understand or appreciatesome points in the manuscript. The editorsof the Majmaah Journal of Health Scienceswill then decide if there are grounds forreconsidering the manuscript.
Scientific integrity The Editorial Board isdevoted to the promotion of scientificintegrity as a vital component of theresearch process. The Research IntegrityEditor will deal with all issues related topossible scientific misconduct inmanuscripts submitted to or published inthe journal. Majmaah Journal of HealthSciences follows the ethics flowchartsdeveloped for dealing with cases ofpossible misconduct. The COPEflowcharts are available at:http://publicationethics.org/flowcharts.The following brief guidelines are aimedto increase awareness of our authors anddecrease misunderstandings about thepublication process in a scientific journal.Although rare events, duplicate publicationand scientific fraud (falsification andfabrication of data, and plagiarism) areimportant issues with serious impact onthe integrity of the scientific community.The Majmaah Journal of Health Scienceswill not consider papers that have alreadybeen published as an article or have beensubmitted or accepted for publicationelsewhere in print or in electronic media.This policy does not precludeconsideration of a paper that has beenrejected by another journal or of a
complete report that follows publication ofa preliminary report, such as an abstract orposter displayed at a professional meeting.Short abstracts (400 words) of preliminaryresearch findings presented at conferencesand included in conference proceedingsare not considered previous publications.Authors should indicate this on the firstpage of the manuscript and in the coverletter. Presentations longer than an abstractmay disqualify the paper. The authorshould alert the Editor if the work includessubjects on which a previous report hasbeen published.
Any such work should be referred to andreferenced in the new paper. If the Editorwas not aware of the violations and thearticle has already been published, a noticeof duplicate publication will be publishedwithout the authors’ explanation orapproval. This policy is based on theinternational copyright laws, ethicalconduct, and cost effective use ofresources). If the Editor discovers or ispresented evidence of such problems, hewill contact the appropriate official(s) atthe institution(s) from which themanuscript originated. It is then left to theinstitution(s) in question to pursue thematter appropriately. Depending on thecircumstances, publish errata, corrigenda,or retractions of manuscripts. In cases ofscientific disagreement about themethodology and/or contents of an articlepublished in the journal, which do notallege fraud, we encourages the concernedindividuals to either directly contact theauthors or write a letter to the Editor.

UPCOMING CONFERENCE MAJMAAH J. HEALTH SCIENCES, 2013 – Vol. 1, No.2
62
UPCOMING CONFERENCES
Sep 14, 2013- Sep 18, 2013
12th Asian Oceanian Congress on ChildNeurology
Venue: InterContinental RiyadhLocation: Riyadh, Saudi Arabia
Jan 21, 2014 - Jan 23, 20142014 International Conference onPhysical Science and Technology
(ICPST 2014)Venue: ARAMAS HOTEL MADINAH
Location: Medina, Saudi Arabia
Jan 22, 2014 - Jan 23, 20142014 The 4th International Conference
on Advanced Materials Research(ICAMR 2014)
Venue: ARAMAS HOTEL MADINAHLocation: Medina, Saudi Arabia
10th to 12th February 20141st International conference onClinical Teaching / Learning in
Nursing and Health SciencesVenue: Jeddah - Kingdom of Saudia Arabia ,
Western Region, Saudi Arabia
01-04 September 2013Emergency Medicine & HyperbaricMedicine Conference & Workshop
Venue: Le Meridien Hotel, Jeddah,Kingdom of Saudi Arabia
24 - 28 August 20132nd Pediatric Intensive Review Course
Venue: Prince Sultan Military Medical City,Riyadh, Kingdom of Saudi Arabia