Embed Size (px)
Citation preview

GI IMAGE
Image Findings in Celiac Artery Stenosis Due to MedianArcuate Ligament CompressionA Crucial Diagnosis When Planning for Pancreaticoduodenectomy
Keli M. Turner & Kunmi Majekodunmi &Alif Manejwala & David Neschis & Zina Novak &
Cherif Boutros
Received: 25 September 2013 /Accepted: 17 December 2013 /Published online: 9 January 2014# 2014 The Society for Surgery of the Alimentary Tract
Abstract Celiac axis stenosis caused by extrinsic compression by the median arcuate ligament (MAL) is present in up to 5 % ofpatients undergoing pancreaticoduodenectomy. Failure to identify and manage MAL compression can lead to potentiallydevastating postoperative consequences that include frank liver necrosis and death. We report an incidental discovery of celiacaxis stenosis by MAL in a patient prepared for pancreaticoduodenectomy. Image findings and operative management arediscussed.
Keyword Celiac stenosis . Pancreaticoduodenectomy .
Median arcuate ligament
Case Report
A 57-year-old otherwise healthy male was referred to thesurgical oncology department with a several week history ofpainless jaundice. The patient had an endoscopic retrogradecholangiopancreatography (ERCP) that demonstrated a distalcommon bile duct stricture for which a pancreatic stent wasplaced for biliary drainage. Brush cytology showed atypicalcells. An MRI was obtained that revealed a pancreatic headmass suspicious for malignancy as well as compression of theceliac axis. Additional work-up revealed no evidence of met-astatic disease and a computed tomographic angiogram (CTangiogram) showed a 90 % stenosis of the celiac artery for adistance of 1.5 cm with a markedly enlarged gastroduodenalartery (GDA) of 5.6 cm in length along with dilatedpancreaticoduodenal arcades (Figs. 1 and 2). These imaging
findings were highly suspicious for celiac axis compressiondue to external compression by the median arcuate ligament(MAL). A pancreaticoduodenectomy with MAL release orpossible celiac axis bypass was planned.
The patient subsequently underwent a pancreatic-oduodenectomy. Upon assessment of the celiac axis, the MALwas found to be thick and fibrotic, and it was divided usingMayo scissors. The released celiac trunk was found to behypotrophic and failed to fully expand despite full release ofthe external compression. Clamping trial of the GDA with abulldog resulted in an immediate and significant drop of theblood flow thru the proper hepatic artery on Doppler examina-tion. The appearance of the celiac artery along with the poorhepatic arterial flow during GDA clamping necessitated anaortohepatic bypass to ensure adequate hepatic arterial perfusionwhichwas performedwith a 6mmPTFE graft. The anastomosiswas conducted with partial clamping of the suprarenal aorta anda Satinsky clamp to the proper hepatic artery just distal to theGDA using 5-0 prolene stitches. The remainder of thepancreaticoduodenectomy was completed uneventfully. Postop-eratively, the patient’s transaminases remained normal, and hisbilirubin decreased markedly from preoperative values. Thepatient recovered well from the surgery with no liver-relatedcomplications. The resected specimen revealed a 2.5 cm mod-erately differentiated invasive pancreatic adenocarcinoma withneural invasion, and eight out of 16 positive lymph nodes andnegative resection margins were pathologically staged as aT2N1 lesion. The patient received adjuvant chemotherapy, butultimately succumbed from systemic metastasis after 9 months.
K. M. Turner : C. Boutros (*)Division of General and Oncologic Surgery, Department of Surgery,University of Maryland School of Medicine, Baltimore, MD, USAe-mail: [email protected]
K. M. Turner :K. Majekodunmi :A. Manejwala :D. Neschis :Z. Novak :C. BoutrosTate Cancer Center, University of Maryland Baltimore WashingtonMedical Center, 301 Hospital Drive, Glen Burnie, MD 21061, USA
J Gastrointest Surg (2014) 18:638–640DOI 10.1007/s11605-013-2445-5

Discussion
Themedian arcuate ligament is a band of connective tissue thatruns transversely across the aorta and connects the diaphrag-matic crura. In the case of patients with MAL syndrome, theligament crosses in an abnormal position across the proximalportion of the celiac axis; this may lead to clinical symptomssuch as abdominal pain with eating and weight loss. However,in most cases, celiac artery stenosis by the MAL is a purelyradiographic finding without clinical significance.1
It is estimated that up to 5 % of patients undergoingpancreaticoduodenectomy have celiac axis stenosis caused byextrinsic compression from the MAL.2,3 In the cases of celiacaxis stenosis, antegrade blood flow is reduced thru the commonhepatic and gastroduodenal arteries. As a consequence, largecollaterals develop from the superior mesenteric artery (SMA)via the inferior pancreaticoduodenal and dorsal pancreatic arter-ies to provide retrograde flow thru the GDA to the liver. Duringpancreaticoduodenectomy, the GDA as well as thepancreaticoduodenal arcades from the SMA are transected; inpatients with celiac axis stenosis, this may cause ischemia orinfarction of the liver with death as an unintended consequence.4
Most cases of celiac axis stenosis secondary to compres-sion by the MAL are detected radiographically by CTduring the preoperative work-up in preparation forpancreaticoduodenectomy. Findings consistent with celiaccompression by the MAL include hypertrophy of the dia-phragmatic crura, a hooked appearance or kinking of theceliac artery, a prominent GDA, and the presence of prom-inent dorsal pancreatic and pancreaticoduodenal arteries.1,5
In patients in whom celiac axis compression by the MAL issuspected preoperatively, a CT angiography should be per-formed for better delineation of the vascular anatomy.Whereas a CT angiography is generally sufficient to detectfindings consistent with MAL compression, a standardangiography is the only study that can demonstrate retro-grade flow thru the GDA.2 In our institution, distinguishingbetween physiological intermittent compression versus a fixedstenosis can be assessed by duplex ultrasound. In the setting ofa physiologic compression, elevated velocities generally nor-malize during deep inspiration. In the setting of a high gradefixed lesion and enlarged collaterals, the hemodynamic sig-nificance of the lesion is of little doubt. However, if the lesionis fixed and the stenosis is moderate, angiography withintrarterial pressure measurements might be helpful indistinguishing hemodynamic significance (pressure gradientacross the celiac artery >10 mmHg). Intraoperatively, prior todivision, the GDA should be clamped with palpation orDoppler assessment of the hepatic artery to ensure that thereis adequate blood flow to the liver. If blood flow thru thehepatic artery is deemed inadequate, division of theMALmaybe performed; celiac artery revascularization via arterial re-construction is reserved for instances in which MAL divisiondoes not improve perfusion, which is most likely to occurwhen prominent collaterals are evident.3 There are a variety ofrevascularization options including anastomoses between themiddle colic artery and GDA and aorta and hepatic artery, asperformed in this case. Bypass grafting is commonly usedwith these techniques with autologous or synthetic grafts. Themost commonly used autologous conduit is the greater saphe-nous vein, although use of the radial artery as a conduit hasbeen described. Synthetic graft was chosen in this instancebecause of its established patency in high flow, low resistancevascular beds, and, in the author’s experience, is less likely tokink than autologous conduit. Endovascular managementwith balloon angioplasty and stenting of the celiac axis isincreasingly being advocated if MAL release proves unsuc-cessful in reestablishing adequate flow.6 Whereasendovascular treatment of celiac stenosis has been shown tohave excellent short term patency rates and decreased mor-bidity over bypass, long term patency rates are improved withopen revascularization techniques.7
There are reports in the literature of GDA sparingpancreaticoduodenectomy as a means to reduce duodenal is-chemia in the case of pylorus preservation as well as to prevent
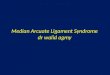
Fig. 1 CTangiogram (sagittal view) depicting the hooked appearance ofthe celiac artery (arrow) due to compression by the median arcuateligament (arrowhead). Also labeled are the aorta (A) and the superiormesenteric artery (SMA)
Fig. 2 CT angiogram 3D reconstruction (coronal view) demonstrating aprominent GDA (arrowhead) as well as a markedly distendedpancreaticoduodenal artery (arrow). Note the smaller size of the commonhepatic artery (CHA) and the size of the common bile duct stent (S) inrelation to the enlarged GDA
J Gastrointest Surg (2014) 18:638–640 639

fatal hemorrhage from the GDA stump. This technique hastheoretical advantages in cases of celiac axis stenosis in whichmaintaining blood flow thru the GDA is imperative for perfu-sion to the liver. However, the question of adequate lymphnode resection has not been resolved with this technique and,moreover, it may prove exceedingly difficult to preserve theGDA for larger tumors of the pancreatic head. In our case, weexpected that the main blood flow to the GDAwas retrogradethrough the pancreaticoduodenal arcade as per the significantstenosis of the celiac trunk. Because of the size of the tumor(2.5 cm) and the need for a full regional lymph node dissectionfor an oncologically sound operation, we chose to bypass theceliac axis to ensure adequate hepatic blood supply.8
Conclusion
Celiac artery stenosis is present in up to 5 % of patients under-going pancreaticoduodenectomy. Prior to any pancreatic sur-gery, preoperative assessment of the celiac artery and pancreaticarterial supply should be performed to evaluate for potentialceliac axis stenosis. Routine clamping of the GDA is imperativeto ensure that antegrade flow occurs by way of the celiac arteryand that hepatic arterial flow is not compromised. If celiaccompression by the MAL is present, it may be successfullymanaged by MAL release; however, in some instances, arterialbypass is necessary to maintain adequate hepatic arterial perfu-sion. Failure to identify celiac artery stenosis prior to surgery or
intraoperatively can lead to potentially devastating conse-quences that include frank liver necrosis and death.
References
1. Horton KM, Talamini MA, Fishman EK. Median arcuate ligamentsyndrome: evaluation with CT angiography. Radiographics 2005;25:1177-82.
2. Farma JM, Hoffman JP. Nonneoplastic celiac axis occlusion in patientsundergoing pancreaticoduodenectomy. Am J Surg 2007;193:341-4.
3. Sugae T, Fujii T, Kodera Y, Kanzaki A, Yamamura K, Yamada S,Sugimoto H, Nomoto S, Takeda S, Nakao A. Classification of theceliac axis stenosis owing to median arcuate ligament compression,based on severity of the stenosis with subsequent proposals for man-agement during pancreaticoduodenectomy. Surgery 2012;151:543-9
4. Gajoux S, Sauvanet A, Vuillerme MP, Cortes A, Dokmak S,Sibert A, Vilgrain V, Belghiti J. Ischemic complications afterpancreaticoduodenectomy. Ann Surg 2009;249:111-117.
5. Ilica AT, Kocaoglu M, Bilici A, Ors F, Bukte Y, Senol A, Ucoz T,Somuncu I. Median arcuate ligament syndrome: multidetector com-puted tomography findings. Comput Assist Tomogr 2007;31:728-31.
6. Duffy AJ, Panait L, Eisenberg D, Bell RL, Roberts KE, Sumpio B.Management of median arcuate ligament syndrome: a new paradigm.Ann Vasc Surg 2009;23:778-84.
7. AbuRahma AF, Campbell JE, Stone PA, Hass SM, Mousa AY,Srivastava M, Nanjundappa A, Dean LS, Keiffer T. Perioperativeand late clinical outcomes of percutaneous transluminal stentings ofthe celiac and superior mesenteric arteries over the past decades. J VascSurg 2013;57:1052-61.
8. Nagai H, Ohki J, Kondo Y, Yasuda T, Kasahara K, Kanazawa K.Pancreatoduodenectomy with preservation of the pylorus and gastro-duodenal artery. Ann Surg 1996:223:194-98.
640 J Gastrointest Surg (2014) 18:638–640