Embed Size (px)
Citation preview

ImageImage--Guided and Adaptive Guided and Adaptive RadiotherapyRadiotherapyRadiotherapy Radiotherapy
PMH 50PMH 50thth ConferenceConference
A.A. FylesFylesyyDept. of Radiation OncologyDept. of Radiation OncologyPrincess Margaret HospitalPrincess Margaret Hospital

IMRT forIMRT forCervix CancerCervix Cancer
Four-field
IMRT
M. Milosevic, PMH-RMP IGRT, 25/1/2008

Challenges in IMRT for Cervix CancerChallenges in IMRT for Cervix Cancergg
Target IdentificationMR CT• MR vs CT
• Nodal targets• Online image qualityOnline image quality
Organ motion• Influence of
– Bladder filling– Rectal filling g– Normal uterus position
WorkloadWorkload

PMH CTV DefinitionPMH CTV Definition
GTVCervix
Vagina
Uterus
Cervix
CTV
g
Parametria
• CTV = GTV (+0.7cm margin) + Cervix + parametria + lower 2cm uterus + upper 2cm vagina• Nodal CTV as per Taylor et alNodal CTV as per Taylor et al• Normal Organs at Risk
• rectum, bladder, sigmoid, bowel, bone etc.

Point of Interest Analysis in 16 PatientsPoint of Interest Analysis in 16 Patients Mean ValuesMean ValuesPoint of Interest Analysis in 16 Patients Point of Interest Analysis in 16 Patients –– Mean ValuesMean Values
14.0 mm 3.8 mm
6.2 mm
9.6 mm
1.7 mm1.4 mm
1.6 mm5.6 mm
INTERFRACTION INTRAFRACTION
+
Internal Uterine FundusInternal Uterine Fundus
Cervical OsCervical Osy +
z

Point of Interest Analysis in 16 Patients Point of Interest Analysis in 16 Patients –– Mean ValuesMean Values
14.0 mm 3.8 mmUB = UB = Uncertainty Uncertainty
B dB d
CranioCranio--CaudalCaudal(mm)(mm)
AntAnt--PostPost(mm)(mm)
6.2 mm
9.6 mm
1.7 mm1.4 mm
1.6 mm5.6 mm
Bounds Bounds (confidence (confidence
limits)limits)
(mm)(mm) (mm)(mm)
INTERFRACTION INTRAFRACTIONTotalTotal IntraIntra TotalTotal IntraIntra
Fundus UBFundus UB 36.936.9 9.69.6 16.416.4 4.34.3
+
Internal Uterine FundusInternal Uterine Fundus
Cervical OsCervical Os
Fundus UBFundus UB 36.936.9 9.69.6 16.416.4 4.34.3
Os UBOs UB 14.814.8 3.63.6 24.824.8 4.04.0y +
z

Adapting to ChangeAdapting to Change
•• Tumors are heterogeneousTumors are heterogeneous•• Position changesPosition changes
+
–– InterInter--fraction, Intrafraction, Intra--fractionfraction
•• Size and shape changesSize and shape changes•• Biology changesBiology changes
+ +

8 GyPre-Tx
Tumour Shrinkage & Deformation
20 Gy 28 Gy
• Influence of:
– Tumour factors• Biology
– Hypoxia
T t t f t
38 Gy 48 Gy
– Treatment factors• Chemo-radiation
Adaptive ImageAdaptive Image--Guided RTGuided RTAdaptive ImageAdaptive Image--Guided RTGuided RT
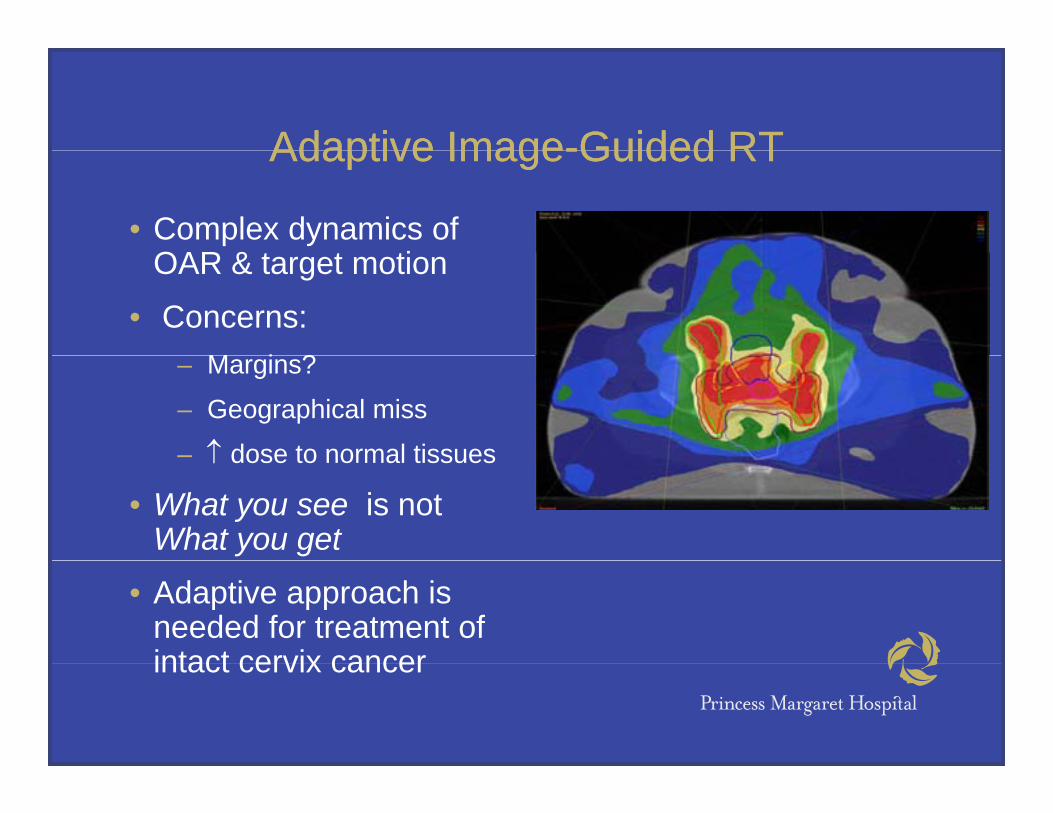
• Complex dynamics of OAR & t t tiOAR & target motion
• Concerns:M i ?– Margins?
– Geographical miss
– ↑ dose to normal tissues↑ dose to normal tissues
• What you see is not What you get
• Adaptive approach is needed for treatment of intact cervix cancerintact cervix cancer

IMRT Lymph Node PlanIMRT Lymph Node PlanIMRT Lymph Node PlanIMRT Lymph Node Plan
Role for image-guidedguided nodal targeting using gUSPIO MR

Lymph Node MarginsLymph Node Margins
2 cm radial expansionaround iliac vessels
Shih, 2005Shih, 2005 Taylor, 2005Taylor, 2005

LN Movement During RTLN Movement During RT
Coverage of Unified nCTV7
105
100
105
age
Day 1 CTV
Summed CTV
95
enta
ge C
over
a85
90Perc
e85
0 4 8 12 16 20
2-mm Expansions of nCTV7Chan and DinniwellChan and Dinniwell
4 mm PTV expansion encompasses 4 mm PTV expansion encompasses >90% of LN movement>90% of LN movement
M. Milosevic, PMH-RMP IGRT, 25/1/2008

Delivered vs. Planned Dose Delivered vs. Planned Dose Image at T=0 Image at T=1
Mesh-BasedBiomechanical Model
•• MotionMotion•• MotionMotion•• DeformationDeformation•• Dose accumulation Dose accumulation •• Adaptive reAdaptive re--planningplanning
MORFEUSMORFEUSMORFEUSMORFEUS Slide c/o Kristy BrockSlide c/o Kristy Brock
pp p gp g

CT_0
BASELINE WEEK 1 WEEK 2 WEEK 3 WEEK 4 WEEK 5
MRI_0
ContoursContours
MRI_1
ContoursContours ContoursContours
MRI_2
ContoursContours
MRI_3
ContoursContours
MRI_4
ContoursContours
MRI_5
Surface Surface MeshesMeshes
Surface Surface MeshesMeshes
Surface Surface MeshesMeshes
Surface Surface MeshesMeshes
Surface Surface MeshesMeshes
Surface Surface MeshesMeshes
Nominal Nominal PlanPlan
Dose Dose Accumulated Accumulated
PlPlMeshesMeshes MeshesMeshes MeshesMeshes MeshesMeshes MeshesMeshesMeshesMeshes PlansPlans
Acc DoseAcc Dose Acc DoseAcc Dose Acc DoseAcc Dose Acc DoseAcc Dose Acc DoseAcc Dose
Deformable Dose AccumulationDeformable Dose AccumulationDeformable Dose AccumulationDeformable Dose Accumulation Dose Dose Accumulated Accumulated
Acc Dosewk1
Acc Dosewk1
Acc Dosewk2
Acc Dosewk2
Acc Dosewk3
Acc Dosewk3
Acc Dosewk4
Acc Dosewk4
Acc DoseWk5
Acc DoseWk5
PlansPlans
Nominal Nominal PlanPlan
Adaptive Adaptive Adaptive Adaptive ReRe--plan plan

Initial IMRT strategyInitial IMRT strategy –– 10 pts10 ptsInitial IMRT strategy Initial IMRT strategy –– 10 pts10 pts
• LM (large margin) plan • SM (small margin) plan– 1-2 cm PTV margin– Expectation
• little OAR sparing
– 0.5 cm PTV margin– Expectation
• Some OAR sparinglittle OAR sparing• Target always covered
Some OAR sparing• Target missed

Initial IMRT strategyInitial IMRT strategy –– 10 pts10 ptsInitial IMRT strategy Initial IMRT strategy –– 10 pts10 pts
• Adaptive re-plan p p– Union CTV of 1st 3 image sets (iCTV)– Expectation
M OAR i• More OAR sparing• Target coverage better
• Results– LM plan covered most pts– SM plan seemed adequate for more pts than
expectedexpected– Re-plan did not spare as much OAR as hoped
• WHY?WHY?

WHY?WHY?WHY?WHY?
• Large CTV – tumour shrinkage did not influence treatment volume as much as expected
• Organ motion – iCTV – resulted in even larger CTVs than baselinethan baseline
• Estimates of 3D margins too generous based on previous POI data
• Influence of bladder / rectal filling– Heterogeneous despite bowel & bladder prep
Caused large displacements in CTV location in some pts– Caused large displacements in CTV location in some pts
• Influence of uterus position

22ndnd Adaptive strategyAdaptive strategy –– 25 pts25 pts22 Adaptive strategy Adaptive strategy –– 25 pts25 pts
• Use of ultra-small PTV margins (0.3cm)g ( )• Assume perfect set-up daily (CBCT)• Separate out pts into consistent & variableSeparate out pts into consistent & variable
bladders• Adaptive re-plan – after 2nd wk treatment, use p p ,
only imaging at that time point, no union CTV.

25pts25pts98% of the PTV to be covered by the 95% isodose for all plans98% of the PTV to be covered by the 95% isodose for all plans
Plan evaluation criteria:Plan evaluation criteria:98% of GTV received 5000cGy; 98% HRCTV received ≥ 4900cGy98% of GTV received 5000cGy; 98% HRCTV received ≥ 4900cGy
Dose Accumulation with InterDose Accumulation with Inter--Fraction Motion AppliedFraction Motion Applied
Consistent BladdersConsistent Bladders
Dose Accumulation with InterDose Accumulation with Inter Fraction Motion AppliedFraction Motion Applied
Variable BladdersVariable Bladders
Nom SMNom SM Acc SMAcc SM Acc AMAcc AM
GTV GTV (D98)(D98) 50365036 50145014 50315031
HRCTV HRCTV (D98)(D98) 49234923 48584858 49094909
Nom SMNom SM Acc SMAcc SM Acc AMAcc AM
GTV GTV (D98)(D98) 50245024 49874987 50085008
HRCTV HRCTV (D98)(D98) 49114911 47834783 47804780HRCTV HRCTV (D98)(D98) 49234923 48584858 49094909
Rectum Rectum (V45)(V45)
5454 5151 4141
Sigmoid Sigmoid 5959 6161 3939
HRCTV HRCTV (D98)(D98) 49114911 47834783 47804780
Rectum Rectum (V45)(V45) 5252 5050 4141
Sigmoid Sigmoid (V45)(V45) 6161 6767 5151Sigmoid Sigmoid
(V45)(V45)5959 6161 3939
Bladder Bladder (Mean)(Mean)
40024002 41034103 39633963
Bladder Bladder (Mean)(Mean)
40654065 39603960 39303930
P < 0.05P < 0.05 compared to Nominal SM plan

Conclusions of MR StudyConclusions of MR Study• Tumour & organ dynamics within the
pelvis is complex
• Inter-fraction motion is a major issue in cervix cancer, supporting IGRT
S ll i t f ti d LN• Small inter-fraction and LN motion/deformation
• Tumour regression during treatment g gsuggests adaptive IGRT
• Conventional plan ≠ Delivered dose
• Daily image-guidance and adequate bladder prep is essential
• Adaptive strategy may be successful forAdaptive strategy may be successful for some patients

Cervical Stump CarcinomaCervical Stump CarcinomaCervical Stump CarcinomaCervical Stump Carcinoma
• 45 year old woman, y ,previous sub-total hysterectomy for ffibroids
• MR– 6 cm. tumor
replacing cervix, small pelvic nodesp
– sigmoid looped over over tumor

IMRT Boost TreatmentIMRT Boost TreatmentIMRT Boost TreatmentIMRT Boost Treatment
• 5-10% of patients - • Boost to 70 - 75 Gy unsuitable for brachytherapy
• Gross nodal disease may be treated to 65-70 Gy
• Cervical stump
• Sidewall or nodal disease that receives less than 60
• Other means of radiation boost
St d d EBRTthat receives less than 60 Gy (EBRT and IC)
• PMH IMRT dose of 25.2
– Standard EBRT
• Limited by normal tissue tolerance
Gy in 14 fractionstissue tolerance (dose of 60-65 Gy)

IMRT BoostIMRT Boost -- IssuesIssuesIMRT Boost IMRT Boost -- IssuesIssues
• Boost Volume• Cervix alone – simulating IUA brachytherapy• Cervix and pelvic sidewall(s)
• Organ movement.I l di bl dd d t l ti• Including bladder and rectal preparation
• Set-up reproducibilityI bili ti• Immobilization

IMRT Boost Spares Normal OrgansIMRT Boost Spares Normal OrgansBladder/Rectum
Femoral heads

ParaPara--aortic Radiationaortic RadiationParaPara--aortic Radiationaortic Radiation
• Positive pelvicPositive pelvic nodes and/or small PAN or recurrence
• Concurrent cisplatin
• Risk of toxicity GI, hematologic

ParaPara--aortic Radiation with Simultaneous aortic Radiation with Simultaneous Integrated BoostIntegrated BoostIntegrated BoostIntegrated Boost
Dose-Volume HistogramKidneys/Small BowelHistogramBowel

PostPost--Operative Adjuvant Pelvic IMRTOperative Adjuvant Pelvic IMRT
• Recent RTOG Phase II trial of feasibilityy
• Toxicity decreased esp. GI
• Possible benefit if chemo-radiation
• Target motion issuesTarget motion issues minimized with ITV (simulation bladder
t d f ll)empty and full)• Cone-beam imaging
for bone matchingfor bone matching

MR ImageMR Image GuidedGuidedMR ImageMR Image--Guided Guided BrachytherapyBrachytherapy
for Cervix Cancerfor Cervix Cancerfor Cervix Cancer for Cervix Cancer
• Adapt to changing volumeAdapt to changing volumep g gp g g•• IRIR--CTVCTV::
Tumor at diagnosisTumor at diagnosis20 Gy20 Gyyy
•• HRHR--CTVCTV::Residual tumor at BTResidual tumor at BT40 Gy from BT40 Gy from BT40 Gy from BT40 Gy from BT
•• Reduced toxicityReduced toxicity•• Identification ofIdentification of
“non“non responders”responders”“non“non--responders”responders”
M. Milosevic, PMH-RMP IGRT, 25/1/2008

ImageImage--Guided BrachytherapyGuided BrachytherapyStd brachytherapy is not optimal for all patientsStd brachytherapy is not optimal for all patientsy py p py py p p
90
100
70
80
%)
40
50
60
Volu
me
(%
HR-CTV20 patients
10
20
30
V Standard plansMR-dosimetry
(Zwahlen)V100
0
10
0 20 40 60 80 100 120 140 160 180 200Dose (%)

ImageImage--Guided BrachytherapyGuided Brachytherapy
303030
gg y pyy py
20
25
me
(cm
3 )
20
25
me
(cm
3 )
20
25
me
(cm
3 ) HR-CTV20 patientsStandard plans
15
wal
l vol
um Rectum15
wal
l vol
um Rectum15
wal
l vol
um RectumMR-dosimetry(Zwahlen)
5
10
Rec
tal w
D2cm35
10
Rec
tal w
5
10
Rec
tal w
D2cm3
00 1000 2000 3000 4000 5000
D2cm0
0 1000 2000 3000 4000 50000
0 1000 2000 3000 4000 5000
D2cm
Dose (cGy)Dose (cGy)Dose (cGy)
M. Milosevic, PMH-RMP IGRT, 25/1/2008

Optimized IGOptimized IG--BrachytherapyBrachytherapyD2cm3
OAR Tumor size Conventional
(Gy) Optimized
(Gy) Change (%)
AllOptimizationOptimization
All tumors 25 ±8.7 22 ±6.6 -14%*
Small 26 ±3.2 19 ±5.7 -32%* Sigmoid
colon Large 25 ±7.4 24 ±6.7 -3%
20 cases20 casesHRHR--CTV CTV >>40 Gy40 GyIRIR CTVCTV >>20 G20 G Large 25 ±7.4 24 ±6.7 3%
All tumors 16 ±6.2 16 ±6.7 0
Small 16 ±7.8 14 ±7.6 -14%* Rectum
IRIR--CTV CTV >>20 Gy20 GyPoint A Point A <<40 Gy40 Gy
Large 17 ±4.5 19 ±4.5 +14%* All
tumors 31 ±9.2 30 ±9.8 -2%
Small 30 ±8.7 26 ±9.6 -12%* Bladder
Large 32 ±9.9 34 ±8.6 +6%
Daniel Zwahlen, 2007Daniel Zwahlen, 2007M. Milosevic, PMH-RMP IGRT, 25/1/2008

Optimized IGOptimized IG--BrachytherapyBrachytherapypp y pyy py
145 patients145 patientsLocal control
T1b/2a 15%T1b/2a 15%T2b/3a 59%T2b/3a 59%
Local control
CSS
T3b 26%T3b 26%>5 cm 54%>5 cm 54%
OS
LN 39%LN 39%RTRT++CTCT
Late ToxicityLate Toxicity
Gr. 3Gr. 3--4 GI 4%4 GI 4%Optimized BTOptimized BT
8080--85 Gy85 Gy
G 3G 3 G %G %GU 4%GU 4%
Vaginal 5%Vaginal 5%
Potter, 2007Potter, 2007M. Milosevic, PMH-RMP IGRT, 2008

Optimized IGOptimized IG--BrachytherapyBrachytherapypp y pyy py
145 patients145 patientsLocal controlSmall tumors
T1b/2a 15%T1b/2a 15%T2b/3a 59%T2b/3a 59%
Local control
CSSLarge tumors
Small tumors
T3b 26%T3b 26%>5 cm 54%>5 cm 54%
OS
LN 39%LN 39%RTRT++CTCT
Late ToxicityLate Toxicity
Gr. 3Gr. 3--4 GI 4%4 GI 4%
Local Control
Optimized BTOptimized BT8080--85 Gy85 Gy
G 3G 3 G %G %GU 4%GU 4%
Vaginal 5%Vaginal 5%
Potter, 2007Potter, 2007M. Milosevic, PMH-RMP IGRT, 2008

What Next?What Next?What Next?What Next?
• Work by our group & th
• Contouring l t &others
– poor correlation between rectal & bladder volumes and cervix position
nomenclature & guidelines (e.g. GEC-ESTRO and Post-op RTOG)and cervix position
• Look at influence of uterus position on target
ti
RTOG)– International
collaboration – RTOG group in June 08motion
• Simple class solution / margin recipe unlikely
group in June 08• Any adaptive strategy
needs to be i di id li d
g ygiven complexity of target motion & deformation
individualised• At present IMRT not
ready for intact cervixy

What next?What next?What next?What next?
• Validate modeled findings with independent g pcohort of pts with more frequent imaging– 2-3 MR scans per wk– Initial bladder full & bladder empty MRIs– CBCT during treatment
E l f ibili f i CBCT• Explore feasibility of contouring on CBCT imagesUlti t l ti d ti• Ultimate goal – propose prospective adaptive IMRT strategy for cervix patients

Princess Margaret HospitalPrincess Margaret HospitalRadiation Oncology: Radiation Oncology: M. Milosevic, K. Lim, P. Chan, D. Zwahlen, R. Dinniwell, W. M. Milosevic, K. Lim, P. Chan, D. Zwahlen, R. Dinniwell, W.
Levin, L. ManchulLevin, L. ManchulMedical Physics: Medical Physics: YY--B Cho, K. Brock, J. Jezioranski, I. Yeung, T. Craig,B Cho, K. Brock, J. Jezioranski, I. Yeung, T. Craig,
A BeikiA Beiki Ardakani J Stewart J Moseley M Sharpe D JaffrayArdakani J Stewart J Moseley M Sharpe D JaffrayA. BeikiA. Beiki--Ardakani, J. Stewart, J. Moseley, M. Sharpe, D. JaffrayArdakani, J. Stewart, J. Moseley, M. Sharpe, D. JaffrayMedical Imaging: Medical Imaging: M. HaiderM. HaiderRadiotherapy: Radiotherapy: V. Kelly, J. PatersonV. Kelly, J. PatersonBiostatistics:Biostatistics: M Pintilie G LockwoodM Pintilie G LockwoodBiostatistics: Biostatistics: M. Pintilie, G. LockwoodM. Pintilie, G. Lockwood
RaySearch Laboratories ABRaySearch Laboratories ABA. Lundin, H. Rehbinder, J. LA. Lundin, H. Rehbinder, J. Lööff
Supported by:Supported by:National Cancer Institute of Canada through the Terry Fox RunNational Cancer Institute of Canada through the Terry Fox RunGiovanni and Concetta Guglietti Family TrustGiovanni and Concetta Guglietti Family Trust
M. Milosevic, PMH-RMP IGRT, 25/1/2008





























