Embed Size (px)
Citation preview

EDUCATION EXHIBIT 927
Imaging-guidedInjection Techniqueswith Fluoroscopy andCT for Spinal PainManagement1
Richard Silbergleit, MD2 ● Bharat A. Mehta, MD ● William P.Sanders, MD ● Sanjay J. Talati, MD3
Local spinal pain and radiculopathy are common conditions that de-bilitate millions of Americans annually. Most cases are successfullytreated conservatively with rest or physical therapy. Chiropractic ma-nipulation or, in some cases, surgery may also be performed. Percuta-neous injection has been used for spinal pain management for manyyears, but many of these procedures have historically been performedwithout imaging guidance. Recently, however, newer minimally inva-sive, imaging-guided percutaneous techniques have been added to thelist of available treatment options for spinal pain. Imaging-guided tech-niques with fluoroscopy or computed tomography increase the preci-sion of these procedures and help confirm needle placement. Cervical,thoracic, lumbosacral, and sacroiliac pain can be evaluated and treatedsafely and effectively with injections of local anesthetics or long-actingsteroids into facet joints, sacroiliac joints, selective nerve roots, spon-dylolytic areas, and the epidural space. Because imaging-guided tech-niques appear to provide better results and reduce complication rates,they are becoming more popular despite controversy regarding theireffectiveness. Controversy will continue to surround these imaging-guided techniques until large, double-blinded studies become avail-able. In the meantime, there is an increased demand for these proce-dures from referring physicians, and it is important to be able to safelyperform them with a minimum of patient discomfort.
Index terms: Computed tomography (CT), guidance, 30.1211 ● Fluoroscopy, 30.11, 30.12989, 30.92 ● Nerves, roots, 30.11, 30.1211 ● Nerves, spi-nal, 30.11, 30.1211 ● Spine ● Spine, anatomy, 30.92 ● Spine, CT, 30.1211 ● Spine, facet joints, 30.11, 30.1211, 30.92
RadioGraphics 2001; 21:927–942
1From the Department of Radiology, Henry Ford Hospital, Detroit, Mich (R.S., B.A.M., S.J.T.), and the Department of Diagnostic Radiology, Wil-liam Beaumont Hospital, 3601 W Thirteen Mile Rd, Royal Oak, MI 48073-6769 (W.P.S.). From the 1999 RSNA scientific assembly. ReceivedNovember 3, 2000; revision requested December 8 and received December 28; accepted December 29. Address correspondence to R.S.([email protected]).
2Current address: Department of Diagnostic Radiology, William Beaumont Hospital, Royal Oak, Mich.
3Current address: Department of Radiology, Covenant Health Care, Saginaw, Mich.
See the commentary by Zinreich and Murphy following this article.
©RSNA, 2001

IntroductionLocal spinal pain and radiculopathy are very com-mon conditions that debilitate more than half thepopulation of the United States at some time intheir lives. The prevalence of these conditions is atleast 5% annually (1,2). Most cases are successfullytreated conservatively with rest or physical therapy.Chiropractic manipulation is also very commonalthough not frequently recommended to patientsby their allopathic physicians. Surgery is reservedfor a small percentage of cases. Because imagingabnormalities do not correlate with symptoms inmost cases (3–5), many patients do not receive aspecific diagnosis and have continued pain.
Percutaneous injection techniques have beenused to treat back pain for many years—and havebeen controversial. Many of these procedureshave historically been performed without imagingguidance. Imaging-guided techniques with fluo-roscopy or computed tomography (CT) increasethe precision of these procedures and help con-firm needle placement. Because imaging-guidedtechniques should lead to better results and re-duced complication rates, they are now becomingmore popular. These improvements are probablydue in part also to better patient selection by ex-perienced spine physicians.
Cervical, thoracic, lumbosacral, and sacroiliacpain can be evaluated and treated with interven-tional procedures including injections of localanesthetics or long-acting steroids into facetjoints, sacroiliac joints, selective nerve roots,spondylolytic areas, and the epidural space.
In this article, we discuss and illustrate tech-niques for CT- and fluoroscopy-guided percuta-
neous injections used at our institution for spinalpain management. These include techniques forfacet joint injection, selective nerve root injection,epidural injection, sacroiliac joint injection, andinjection for spondylolysis.
TechniqueAll of the procedures discussed in this article areroutinely performed on an outpatient basis. Thepatient is questioned regarding previous steroiduse (oral, cutaneous, or injected) to avoid causingiatrogenic Cushing syndrome. We usually wait2–3 months before administering repeat injec-tions. This is particularly important when multi-level injections (eg, bilateral L3-4, L4-5, andL5-S1 facet joint injections) are performed. Rela-tive contraindications include hemorrhagic dia-thesis, local skin infection, and pilonidal cyst aswell as progressive neurologic disorder, whichmay be masked by the procedure.
The procedure as well as possible benefits andcomplications are explained to the patient, andinformed consent is obtained. Because it is oftendifficult to determine the origin of spinal pain, thepatient is advised that the procedure may not beeffective. Possible complications that are dis-cussed include Cushing syndrome, infection,hemorrhage, pneumothorax, anaphylactic (idio-syncratic) reaction to iodinated contrast materialor anesthetic, and nerve damage.
Baseline vital signs are obtained. Physiologicmonitoring (pulse oximetry and intermittent auto-matic blood pressure and pulse rate monitoring) is
Figure 1. (a) Drawing of a lumbar segment (axial view) shows the medial branch of thedorsal ramus of the spinal nerve root innervating a facet joint. (b) Drawing of the midlumbarspine (lateral view) shows branches from one nerve root innervating both the level of the exit-ing root and the next lower level.
928 July-August 2001 RG f Volume 21 ● Number 4

used if conscious sedation is administered to thepatient. Physiologic monitoring is not necessary inotherwise healthy patients if sedation is not used(6). Intravenous sedation is required in less than20% of patients and consists of low doses of opioidsor anxiolytic drugs. Midazolam hydrogen chloride(initial dose, 1 mg) is used for sedation and anxioly-sis. In healthy adults, additional doses of 1 mg aregiven as needed up to a total of 4 mg with an inter-val of at least 2 minutes between doses. In patientsover 60 years of age and in chronically ill or debili-tated patients, additional doses are reduced to 0.5mg up to a total of 3 mg. Morphine sulfate (initialdose in healthy adults, 1–2 mg) is used for pain re-lief. Additional doses of 1–2 mg are given as neededup to a total of 10 mg with an interval of at least 2minutes between doses. Resuscitation equipmentshould be readily available.
Sterile procedure is followed. For cutaneousand tract local anesthesia, we use 1% lidocaine.We use triamcinolone acetonide suspension (Ke-nalog 10 or 40 [Apothecon, Princeton, NJ ]) as along-acting steroid and bupivacaine hydrochlo-ride (Sensorcaine 0.25% [Astra USA, Westbor-ough, Mass ]) as a long-acting local anesthetic.After the procedure, the patient is observed in therecovery room or short stay unit for 1–2 hoursdepending on his or her condition.
Most of these procedures can be performedwith either CT guidance or fluoroscopic guid-ance. The imaging technique used is largely amatter of personal preference. Different steroidsand anesthetics may also be used.
Facet Joint InjectionFacet joint pain is attributed to segmental instabil-ity, inflammatory synovitis, or degenerative arthritis(1,7,8). Cavanaugh et al (9) conducted a study us-ing New Zealand white rabbits and demonstratedthat the facet joints are heavily innervated, that sen-sitization and excitation of nerves occurs in the facetjoints when the joint is inflamed or exposed to cer-tain chemicals that are released during injury andinflammation, and that injection of hydrocortisoneand lidocaine results in a marked reduction in thisnerve activity. The signs of facet joint syndrome arelocal paraspinal tenderness; pain on hyperextension,rotation, and lateral bending; absence of neurologicdeficit; absence of root tension sign; and hip, but-tock, or back pain with straight leg raising (8).Symptoms include hip and buttock pain, crampingleg pain involving the thigh but not radiating belowthe knee, low back stiffness, and absence of pares-thesias (8). The back stiffness is typically mostmarked in the morning.
According to a study by Schwarzer et al (10), thedegree of degenerative change identified on CTscans is a poor indicator of the presence or degree
of facet joint syndrome. However, Lewinnek andWarfield (11) found radiographic evidence of facetjoint disease to correlate with the initial success offacet joint injections. Helbig and Casey (12) de-scribed four clinical criteria that led to a high long-term success rate, including back pain associatedwith groin or thigh pain, well-localized paraspinaltenderness, reproduction of pain with extension-rotation toward the symptomatic side, and signifi-cant facet joint arthrosis seen at radiography. Large-volume injections may cause joint rupture and ex-travasation into the epidural space, which mayaccount for part of their therapeutic effect (13).There is disagreement as to whether intraarticularinjection is preferable to periarticular injection(14,15). The true success of facet joint injections isuncertain despite numerous studies because ofquestions regarding patient selection, uncertainty asto whether the injections were intraarticular or peri-articular, and use of different medications. Facetjoint injection may be considered either diagnosticor therapeutic (1,16). CT guidance (7,16) or fluo-roscopic guidance (8,10,11,13,14) may be used forfacet joint injections. Levels for injection are se-lected on the basis of local pain or tenderness andimaging evidence of disease. It is often difficult tolocalize the pain to one level, so that generally twoand occasionally three levels are injected. If the painis bilateral, injections are performed bilaterally.There are reports of long-term (3–6 months) suc-cess and failure (14–17). Denervation of the facetjoint may also be performed with CT guidance orfluoroscopic guidance. This procedure has beenperformed with 95% ethanol or with radio-fre-quency techniques (7,18). Gangi et al (7) denervatefacet joints using CT guidance with 95% ethanol.Twenty-two–gauge spinal needles are advancedinto the internal superior borders of the transverseprocesses above and below the target facet joint.One mL of nonionic contrast material is injected topredict ethanol diffusion, and 1.5 mL of 95% etha-nol is injected at each level. Van Kleef et al (18) de-nervated facet joints using C-arm fluoroscopic guid-ance and 60-second 80° C treatment with a radio-frequency generator. Bogduk and Long (19)studied the anatomy of facet joint innervation andfound that the most commonly used techniquesusually result in injury to the medial branch of thedorsal ramus rather than to the small nerves of thefacet joints. A facet joint is supplied by the nerveexiting at the level of the facet joint as well as at thenext higher level (Fig 1). Denervating a facet jointrequires that two rhizotomies be performed. Forexample, denervation of the right L3-4 facet jointrequires rhizotomy of right L2 and L3.
RG f Volume 21 ● Number 4 Silbergleit et al 929

Fluoroscopic GuidanceWe routinely use fluoroscopic guidance for theinjection of cervical facet joints. The patient isplaced in the supine oblique position at an ap-proximately 45° angle with the side to be injectedfacing up. The head is turned away from the sideto be injected. The frontal tube is angled to openthe facet joint, and a 22-gauge needle is advancedinto the joint (Fig 2a). The patient is then placedflat, and true lateral and anteroposterior views areobtained to confirm the needle position (Fig 2b).A posterior approach is usually used to avoid thevertebral arteries. If the shoulders are large, ananterior approach may be required. A 25-gaugeneedle is usually used for this approach. Fortherapeutic injection, 0.5 mL of triamcinoloneacetonide suspension (Kenalog 40) and 1–2 mLof 0.25% bupivacaine hydrochloride are used.For diagnostic purposes, only the latter is in-jected. If more than four joints are being injected,the dose of triamcinolone acetonide is reduced tokeep the total dose below 80 mg.
We prefer CT guidance for the injection oflumbar facet joints and use a technique that isdescribed in the next section; however, fluoro-scopic guidance may also be used. The patient is
Figure 2. (a) Frontal oblique radiograph obtained with fluoroscopic guidance (standard posterior ap-proach) demonstrates angulation of the tube to open the facet joints for cervical facet injection. (b) Lat-eral radiograph obtained with fluoroscopic guidance helps confirm the needle position.
Figure 3. (a) Frontal oblique radiograph obtained with fluoro-scopic guidance for optimal visualization of the facet joints demon-strates a needle in the L3-4 joint. (b) Drawing of the L3-4 level(oblique view) shows the needle at an exaggerated angle.
930 July-August 2001 RG f Volume 21 ● Number 4

placed in the prone oblique position with the sideto be injected facing up slightly. The patient isthen rotated until the facet joint is best visualized(Fig 3). A 22-gauge needle is advanced verticallyinto the joint, and its position is confirmed withtrue lateral and anteroposterior views. Our thera-peutic and diagnostic injections are identical tothose used for cervical facet joints. Gangi et al (7)use 3.75 mg (1.5 mL) of cortivazol mixed with1.5 mL of 0.25% bupivicaine hydrochloride forevery two facet joints. Sarazin et al (20) have de-scribed a fluoroscopically guided technique forinjecting the inferior articular recess of the facetjoint that does not require profiling the joint.
CT GuidanceCT guidance is our preferred technique for lum-bar facet joint injection. The patient is placed inthe prone position, and several images are ob-
tained at the level of interest to determine entrysite and angle of approach. The entry site ismarked on the skin, and a 22-gauge needle is ad-vanced into the joint (Fig 4). A coaxial systemmay be used to approach a horizontally orientedjoint. Injections are identical to those performedwith fluoroscopic guidance. We also prefer CTguidance for thoracic facet joint injections. In thethoracic region, the horizontal orientation of thefacet joints and overlying ribs usually limits ac-cess. Access may be limited in other areas bybridging spurs. In such cases, periarticular injec-tion is performed (Fig 5). The steroid and anes-thetic doses are the same as for other facet jointinjections. Cervical facet joint injections may alsobe performed with CT guidance (Fig 6).
Figures 4–6. (4) CT scans demonstrate a bilateral L4-5 facet joint injection with the vertical approach (a)and an L5-S1 facet joint injection with the angled approach (b). (5) CT scan shows a T6-7 facet jointinjection. (6) CT scan shows a C5-6 facet joint injection.
RG f Volume 21 ● Number 4 Silbergleit et al 931

Selective Nerve Root InjectionNerve root injection is indicated in patients withradicular symptoms in the cervical, thoracic, lum-bar, or sacral region; acute diskogenic symptomswithout nerve paralysis that is resistant to conven-tional medical therapy; and post-diskectomy syn-drome (1). Inflammation of the nerve root is pre-sumed to be the cause of the pain. In a study byZennaro et al (21), selective nerve root injectionprovided pain relief in 70% of all patients and in95% of patients with foraminal stenosis secondaryto degenerative stenosis rather than disk herniation.These authors used CT guidance and injected 0.8mL of 1% lidocaine with 75 mg of hydrocortisone.Selective nerve root injections often result in a de-gree of epidural injection, which may play a role inpain relief. Typically, injection is performed at asingle level that correlates with the radiculopathy.
Fluoroscopic GuidanceCervical nerve root injections may be performed withCT guidance or fluoroscopic guidance. For a fluo-roscopically guided selective cervical nerve root in-jection, the patient is placed in the supine obliqueposition with the side to be injected facing up. Thehead is turned slightly to the opposite side. Obliquity isadjusted until the foramina are well seen (Fig 7a). A22-gauge spinal needle is advanced toward the fora-men. The patient is placed flat, and anteroposteriorand lateral views are obtained to confirm the needleposition (Fig 7b). The needle should not projectmedial to the medial margin of the pedicle on thefrontal view. The patient often reports reproductionof symptomatic pain along the nerve distribution asthe needle nears the appropriate location. For C1and C2 nerve root injections, the patient is placed inthe prone position and the needle is advanced underfrontal and lateral fluoroscopic guidance (Fig 8).The stylet is then removed, and absence of cerebro-
Figure 7. (a) Lat-eral oblique radio-graph obtained withfluoroscopic guid-ance with the pa-tient’s head turned tothe left demonstratesa cervical nerve rootinjection with theneedle projectinginto the C6-C7 neu-ral foramen. (b) On afrontal radiographobtained with fluoro-scopic guidance, theneedle tip has beenadvanced to thepedicle.
Figure 8. Frontal(a) and lateral(b) radiographs ob-tained with fluoro-scopic guidancedemonstrate a C2nerve root injection.
932 July-August 2001 RG f Volume 21 ● Number 4

spinal fluid flow is verified with aspiration. Two mLof Kenalog 10 and 2 mL of Sensorcaine 0.25% areinjected. If the dura mater is perforated, the proce-dure is terminated and subsequently rescheduled.
Similarly, for fluoroscopically guided selectivethoracic nerve root injections, the patient isplaced in the prone position and the needle isadvanced under frontal and lateral fluoroscopicguidance (Fig 9). Care is taken to keep the needleposterior and medial to avoid the pleural space.Although we have used this technique in manypatients without causing a pneumothorax, this isa serious concern, and CT guidance may be safer,particularly in thin patients. Injections are thesame as for cervical nerve roots.
For a fluoroscopically guided selective lumbarnerve root injection, the patient is placed in theprone oblique position with the side to be injectedfacing up. A 22-gauge needle is advanced under thepedicle with the patient in this position (Fig 10a).The patient is then placed flat, and needle positionis confirmed with frontal and lateral views (Fig10b). L5 nerve root injections require marked angu-lation of the needle to avoid the iliac crest (Fig 11).Injections are the same as for cervical nerve roots.Selective sacral nerve root injections may be per-formed with a dorsal approach using the same tech-nique used for a sacral foraminal epidural injection.
Figure 9. Frontal (a) and lateral (b) radiographs obtained with fluoroscopic guidancedemonstrate a T10 nerve root injection. Arrow in b indicates the needle tip.
Figures 10, 11. (10a) Prone oblique radiograph obtained with fluoroscopic guidance demonstrates a needle tipunder the pedicle of L1. (10b) Lateral radiograph obtained with fluoroscopic guidance helps confirm needle place-ment in the L1 neural foramen. (11) Prone oblique radiograph obtained with fluoroscopic guidance demonstrates theangled approach to the L5 foramen.
RG f Volume 21 ● Number 4 Silbergleit et al 933

CT GuidanceFor selective lumbar and thoracic nerve root in-jections, the area of interest is scanned with thepatient in the prone position. For selective cervi-cal nerve root injections, the procedure can beperformed with the patient in the supine, prone,or lateral decubitus position. The skin entry siteand the angle of approach are determined, anda 22-gauge needle is advanced adjacent to theexiting nerve root. Patients usually report repro-
duction of pain along the distribution of thenerve. Cervical (Figs 12, 13), thoracic (Fig 14),lumbar (Figs 15, 16), and sacral (Fig 17) nerveroots may be injected under CT guidance.
Epidural InjectionPatient selection for epidural injections is poorlydescribed in the literature. We have used epiduralinjections for treatment of local pain or radiculop-athy in the settings of documented disk hernia-tion, central or foraminal stenosis, and absentimaging findings. The technique is usually used if
Figures 12–17. (12) CT scan (posterior angled approach) obtained with the patient in the prone position demon-strates needles positioned at both exiting C2 nerve roots. (13) On a CT scan (anterior angled approach), a needle isseen posterior to the carotid and vertebral (cursor) arteries for a C7 nerve root injection. (14) CT scan obtained withthe patient in the prone position shows a T12 nerve root injection. (15) CT scan obtained with the patient in theprone position shows an L4 nerve root injection. (16) CT scan obtained with the patient in the prone position showsan L5 nerve root injection. (17) CT scan (posterior sacral foramen approach) shows an S1 nerve root injection.
934 July-August 2001 RG f Volume 21 ● Number 4

rest has failed to relieve the symptoms or if thepatient is considered a surgical candidate butdoes not desire to undergo surgery. The tech-nique is infrequently used in acute situations.
Various combinations of saline solution, localanesthetics, and steroids have been injected (22–25). Theories for explaining the method of reliefinclude lysis of adhesions, change in relationshipbetween the disk and the nerve root, anestheticbreaking the pain cycle, and reduction of inflam-mation and swelling (23,24). Epidural injectionhas been performed mostly by anesthesiologists.White (22), using both sacral hiatus and lumbarinterlaminar approaches, documented that evenin experienced hands, the needle was not in theepidural space 25% of the time when the proce-dure was performed without imaging guidance.The needle may be inadvertently placed intra-durally or intravascularly or may not even be inthe canal. Fluoroscopic guidance is recom-mended for all epidural injections. Injection ofnonionic contrast material to confirm the needleposition is also recommended.
The choice of steroid is controversial. Methyl-prednisolone acetate (Pharmacia & Upjohn,Kalamazoo, Mich) was used extensively prior to theearly 1980s (23,26,27). This steroid mixture con-tains polyethylene glycol, which is neurotoxic. Themost common complications associated with meth-ylprednisolone acetate injection include asepticmeningitis and arachnoiditis (26). These complica-tions are probably related to intrathecal injection;however, there may also be toxicity from epiduralinjection. In a comprehensive literature review,Abram and O’Connor (27) concluded that epiduralinjection of steroid preparations containing polyeth-ylene glycol is safe. Because of the slight risk of in-trathecal injection, even with fluoroscopic guidance,we do not inject methylprednisolone for spinal pro-cedures. El-Khoury and Renfrew (1) inject 3 mL(18 mg) of betamethasone (Celestone Soluspan;Schering, Kenilworth, NJ) followed by 5–10 mL ofsterile saline solution or diluted 0.25% bupivacainehydrochloride via the sacral hiatus. Bush and Hillier(24) inject 80 mg of triamcinolone acetonide with0.5% procaine hydrochloride in saline solution viathe sacral hiatus. Gangi et al (7) use 3.75 mg of cor-tivazol with or without 2 mL of 0.5% lidocaine.
We use fluoroscopic guidance for epidural in-jections. Gangi et al (7) describe CT guidance forlumbar epidural injections. Dorsal interlaminar,
sacral hiatus, and foraminal approaches may beused for lumbosacral epidural injection. Epidu-rography with nonionic myelography-approvediodinated contrast material (iopamidol [Isovue200; Bristol-Myers Squibb, Wallingford, Conn])is performed to document epidural position andevaluate the distribution pattern. If the area ofclinical concern is not opacified, the needle posi-tion is changed. The plica medianis is a midlinedural reflection that may be complete or incom-plete. If complete, it may confine the contrast ma-terial and steroid to one side. If the patient hasbilateral symptoms, one-half of the dose is in-jected followed by repositioning of the needle toopacify the contralateral epidural space and injec-tion of the other half of the dose. If the pain isunilateral, we attempt to inject all the medicationon the ipsilateral side in the presence of a com-plete plica medianis.
For a dorsal interlaminar approach, the patientis placed in the prone position. A 22-gauge spinalneedle is advanced to the posterior margin of thespinal canal. Positioning in the epidural space isdetected with a loss-of-resistance technique.Gentle intermittent pressure is applied on a sy-ringe while advancing the needle. A sudden lossof resistance occurs on entering the epiduralspace. Standard plastic syringes are usually notadequate; instead, glass syringes or special low-resistance plastic syringes (Pulsator Loss of Resis-tance Syringe; Sims Portex, Keene, NH) may beused. Absence of cerebrospinal fluid flow is veri-fied with aspiration. Epidurography is performedwith 2–3 mL of nonionic myelography-approvediodinated contrast material.
The sacral hiatus approach described by El-Khoury et al (25) is the one most frequently usedat our institution. The patient is placed in theprone position. The sacral cornua (ie, the borderof the sacral hiatus) and median sacral crest arepalpated and localized fluoroscopically. Gauzepads are placed between the buttocks to preventpovidone-iodine (Betadine; Purdue Frederick,Norwalk, Conn) from irritating the perineum andgenitals. A 5-inch-long, 22-gauge spinal needle isadvanced via the sacral hiatus into the sacral canaluntil its tip reaches the S3 level (Fig 18). Keepingthe needle below the S2-3 disk space minimizes
RG f Volume 21 ● Number 4 Silbergleit et al 935

Figures 18, 19. (18) Frontal (a) and lateral (b) radiographs obtained with fluoroscopic guidance show a needle in-serted into the sacral canal via the sacral hiatus. (19) Frontal epidurogram shows an epidural injection via the sacral hiatus.
Figures 20, 21. (20) Frontal epidurogram demonstrates an epidural in-jection with the S1 foraminal approach. This approach is also used for se-lective sacral nerve root injections. (21a) Frontal radiograph obtained withfluoroscopic guidance (dorsal interlaminar approach) shows a needle in theposterior epidural space at C7-T1. (21b) Subsequent frontal radiographobtained with fluoroscopic guidance demonstrates contrast material dis-persion. (21c) Drawing shows the needle directed medially over the T1lamina.
936 July-August 2001 RG f Volume 21 ● Number 4

the risk of dural puncture. It is helpful to keep theneedle as horizontal as possible. The needle isusually advanced primarily under lateral fluoro-scopic guidance with intermittent frontal guid-ance. On a frontal projection, the needle shouldlie between the pedicles of the sacral segments.The stylet is removed, and absence of cerebrospi-nal fluid flow is confirmed with aspiration. Epidu-rography is performed with injection of 3 mL ofnonionic myelography-approved iodinated con-trast material (Fig 19). The lumbosacral epiduralspace is usually opacified to the L4 level and oc-casionally higher.
The needle bevel is directed to the symptom-atic side, and 5–7 mL of Kenalog 10 is injected.We do not usually inject local anesthetic into theepidural space because of the possibility of pos-tural hypotension, particularly in older patients.Many authors use local anesthetic in lower tho-racic and lumbosacral epidural injections (1,6,7).If the dura mater is accidentally punctured, we donot perform the injection, and the procedure isrescheduled.
For a lumbar foraminal approach, the patient isplaced in the prone position and a 22-gauge needleis advanced under the pedicle of the appropriatesegment, similar to the approach used for lumbarnerve root injection (Figs 10, 11). Sacral foraminalinjection is performed with a direct dorsal approach,a technique that can also be used for selective sacralnerve root injection (Fig 20).
For a cervical epidural injection, a dorsal inter-laminar (Fig 21) or transforaminal (Fig 22) ap-
proach can be used. The patient is placed in theprone position for the dorsal interlaminar approach.This procedure is performed only at the C7-T1 diskspace, where the dorsal epidural space is larger (1–2mm thick) than at the higher cervical levels (6). A22- or 25-gauge Whitacre needle with a blunt tipand side hole is advanced through an 18-gaugeneedle using a paramedian approach. The needle isdirected to the top of the T1 lamina in the midline.The needle contacts the bone and is then slowlyadvanced into the epidural space with the loss-of-resistance technique. Test injections of contrast ma-terial may also be performed while advancing theneedle. An epidurogram is obtained to documentneedle position and evaluate the extent of opacifica-tion. We inject 5–6 mL of Kenalog 10. Local anes-thetic is not used in upper thoracic or cervical epi-dural injections because of the risk of spinal anes-thesia and respiratory suppression. A similarapproach may be used for thoracic epidural injec-tions (6). In the transforaminal approach, a 25-gauge spinal needle is advanced into the inferiorneural foramen with the patient in an oblique posi-tion to open the foramen. The needle is positionedin the anterolateral epidural space with the loss-of-resistance technique. This approach carries the riskof nerve root or vertebral artery injury. It is usedprimarily when the dorsal interlaminar approach doesnot result in opacification of the area of interest.
Figure 22. (a) Supine oblique radiograph obtained with fluoroscopic guidance (transforaminal approach) demon-strates an open foramen. (b) Lateral radiograph obtained with fluoroscopic guidance demonstrates opacification ofthe anterior epidural space. (c) Frontal radiograph obtained with fluoroscopic guidance shows the needle tip just me-dial to the pedicle.
RG f Volume 21 ● Number 4 Silbergleit et al 937
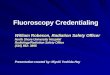
Sacroiliac Joint InjectionThe indications for sacroiliac joint injection areacute or chronic sacroiliac joint pain that is notadequately controlled with nonsteroidal anti-in-flammatory agents. The procedure is frequentlyperformed in patients with seronegative inflam-matory sacroiliitis. Maugars et al (28) inject 1.5mL of cortivazol, the equivalent of 62.5 mg ofprednisone, without local anesthetic.
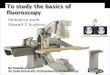
Fluoroscopy or CT may be used for guidance.With fluoroscopic guidance, the patient is placedin the prone oblique position with the side to beinjected facing down to create a vertical pathwayto the inferior synovial joint (Fig 23). The patientis then turned to the prone position, and 22-gauge spinal needle placement is confirmed withlateral fluoroscopy. Five mL of Kenalog 10 and1–2 mL of Sensorcaine 0.25% are injected. WithCT guidance, the middle third of the joint is usu-ally most accessible and is accessed with a dorsalangulated approach (Fig 24).
Injection for SpondylolysisInjection for spondylolysis is used for otherwiseunexplained local pain at the affected level. Weperform injections directly into the spondylolyticarea. El-Khoury and Renfew (1) have demon-strated that injection of adjacent facet jointsopacifies the affected area and can be used fortherapeutic injections.
CT guidance is used because pars defects areeasily identified at CT. The procedure is similarto a CT-guided facet joint injection (Fig 25). A
22-gauge spinal needle is used, and 0.5 mL ofKenalog 40 and 1 mL of Sensorcaine 0.25% areinjected on each side.
ConclusionsOur preference for a given technique is largelydue to our training and experience and does notnecessarily mean that we consider the alternativesto be inferior or more dangerous. Further experi-ence with fluoroscopically guided CT may show itto be superior to fluoroscopy for many of the pro-cedures for which we now routinely use the lattermodality.
We recommend using the smallest needle thatcan be effectively directed to the target site (usu-ally 22-gauge or smaller). For cervical proce-dures, a 25-gauge needle is preferred if a sharp tipis used. Occasionally, a 20-gauge needle will beused in the lumbar region in a very large patientin whom it is difficult to maneuver the needle.Contrast material should be injected to confirmneedle placement for epidural injections unlessthe patient has a history of contrast material sen-sitivity. Contrast material injection is also usefulfor this purpose in the other procedures, althoughit is not as critical. We usually do not inject con-trast material for the other procedures unless weare unsure of the needle position. Studies similarto that of White (22) on needle placement forepidural injections may be useful in evaluatingwhether contrast material should be routinelyinjected for these procedures. We have safely usedKenalog as our choice of steroid and Sensorcaineas a local anesthetic. Celestone Soluspan appearsto be a good alternative steroid.
Controversy will continue to surround theseimaging-guided techniques until large, double-blinded studies become available. The contradic-
Figure 23. Oblique radiograph obtained withfluoroscopic guidance shows two needles in thesacroiliac joint. We now routinely use only oneneedle at the level of the lower needle.
Figure 24. CT scan shows a needle positioned in thesacroiliac joint.
938 July-August 2001 RG f Volume 21 ● Number 4

tory results of the existing small studies are likelycaused by differing patient selection methods,questions about accurate needle placement, andvarying definitions of success. Despite the contro-versy, there is an increased demand for these pro-cedures from referring physicians, and it is impor-tant to be able to safely perform them with aminimum of patient discomfort.
References1. El-Khoury GY, Renfrew DL. Percutaneous pro-
cedures for the diagnosis and treatment of lowerback pain: diskography, facet joint injection, andepidural injection. AJR Am J Roentgenol 1991;157:685–691.
2. Frymoyer JW. Back pain and sciatica. N EnglJ Med 1988; 318:291–300.
3. Haldeman S. Failure of pathology to predict backpain. Spine 1990; 15:718–724.
4. Wiesel SW, Tsourmas N, Feffer HL, Citrin CM,Patronas N. A study of computer assisted tomog-raphy. I. The incidence of positive CAT scans inan asymptomatic group of patients. Spine 1984;9:549–551.
5. Boden SD, Davis DO, Dina TS, et al. Abnormalmagnetic-resonance scans of the lumbar spine inasymptomatic subjects: a prospective investiga-tion. J Bone Joint Surg Am 1990; 72:403–408.
6. Johnson BA, Schellhas KP, Pollei SR. Epidurogra-phy and therapeutic epidural injections: technicalconsiderations and experience with 5334 cases.AJNR Am J Neuroradiol 1999; 20:697–705.
7. Gangi A, Dietemann JL, Mortazavi R, Pfleger D,Kauff C, Roy C. CT-guided interventional proce-dures for pain management in the lumbosacralspine. RadioGraphics 1998; 18:621–633.
8. Lippitt AB. The facet joint and its role in spinepain: management with facet joint injections.Spine 1984; 9:746–750.
9. Cavanaugh JM, Ozaktay AC, Yamashita HT,King AI. Lumbar facet pain: biomechanics, neuro-anatomy, and neurophysiology. J Biomechanics1996; 29:1117–1129.
10. Schwarzer AC, Wang S, O’Driscoll D, HarringtonT, Bogduk N, Laurent R. The ability of computedtomography to identify a painful zygapophysialjoint in patients with chronic low back pain. Spine1995; 20:907–912.
11. Lewinnek GE, Warfield CA. Facet joint degenera-tion as a cause of low back pain. Clin Orthop1986; 213:216–222.
12. Helbig T, Casey KL. The lumbar facet syndrome.Spine 1988; 13:61–64.
13. Moran R, O’Connell D, Walsh MG. The diagnos-tic value of facet joint injections. Spine 1988; 13:1407–1410.
14. Lynch MC, Taylor JF. Facet joint injection forlow back pain: a clinical study. J Bone Joint SurgBr 1986; 68:138–141.
15. Lilius G, Laasonen EM, Myllynen P, HaralainenA, Gronlund G. Lumbar facet joint syndrome: arandomised clinical trial. J Bone Joint Surg Br1989; 71:681–684.
16. Murtaugh FR. Computed tomography and fluo-roscopy guided anesthesia and steroid injection infacet syndrome. Spine 1988; 13:686–689.
17. Carette S, Marcoux S, Truchon R, et al. A con-trolled trial of corticosteroid injections into facetjoints for chronic low back pain. N Engl J Med1991; 325:1002–1007.
18. Van Kleef M, Barendse GA, Kressels A, et al.Randomized trial of radiofrequency lumbar facetdenervation for chronic low back pain. Spine1999; 24:1937–1942.
19. Bogduk N, Long DM. The anatomy of the so-called “articular nerves” and their relationship tofacet denervation in the treatment of low backpain. J Neurosurg 1979; 51:172–177.
20. Sarazin L, Chevrot A, Pessis E, et al. Lumbar facetjoint arthrography with the posterior approach.RadioGraphics 1999; 19:93–104.
21. Zennaro H, Dousset V, Viaud B, et al. Perigangli-onic foraminal steroid injections performed underCT control. AJNR Am J Neuroradiol 1998; 19:349–352.
22. White AH. Epidural injections for the diagnosis andtreatment of low back pain. Spine 1980; 5:67–86.
23. White AH. Injection techniques for the diagnosisand treatment of low back pain. Orthop ClinNorth Am 1983; 14:553–567.
24. Bush K, Hillier S. A controlled study of caudalepidural injections of triamcinolone plus procainefor the management of intractable sciatica. Spine1991; 16:572–575.
25. El-Khoury GY, Ehara S, Weinstein JN, Mont-gomery WJ, Kathol MH. Epidural steroid injec-tion: a procedure ideally performed with fluoro-scopic control. Radiology 1998; 168:554–557.
26. Nelson DA. Intraspinal therapy using methylpred-nisolone acetate: twenty-three years of clinicalcontroversy. Spine 1993; 18:278–286.
27. Abram SE, O’Connor TC. Complications associ-ated with epidural steroid injections. Reg Anesth1996; 21:149–162.
28. Maugars Y, Mathis C, Vilon P, Prost A. Cortico-steroid injection of the sacroiliac joint in patientswith seronegative spondylarthropathy. ArthritisRheum 1992; 35:564–568.
Figure 25. CT scan (posterior angled approach)demonstrates an injection for spondylolysis.
RG f Volume 21 ● Number 4 Silbergleit et al 939