Embed Size (px)
Citation preview

Neuroimag Clin N
Imaging of the hypopharynx and cervical esophagus
Ilona M. Schmalfuss, MD
Division of Neuroradiology, Department of Radiology, University of Florida College of Medicine, 1600 Southwest Archer Road,
Post Office Box 100374, Gainesville, FL 32610-0374, USA
Cross-sectional CT is a well-established method
used to evaluate the hypopharynx and the cervical
esophagus. Most institutions prefer CT: it is widely
available and better tolerated by patients because it
requires less imaging time [1]. In the hypopharyngeal
and cervical esophagus region, as many as 16% of
MR imaging studies have been reported to be
nondiagnostic secondary to claustrophobia or motion
artifacts [2]. MR imaging is particularly prone to be
inadequate in patients with recurrent tumor or
following radiation therapy [3]; however, MR imag-
ing is superior in evaluating the esophageal verge and
cervical esophagus because of better soft tissue
delineation and less obscuration of this area by
beam-hardening artifacts caused by the shoulders
(as seen on CT). Until recently, MR imaging’s
multiplanar capabilities have been a major advantage
[1]. The introduction of the multislice helical CT
scanner now almost outweighs this advantage.
Imaging protocol
Considerable differences in MR imaging proto-
cols exist based on personal preferences and ven-
dor-related variations in hardware and software.
Nevertheless, the following parameters should be
followed to obtain high-resolution images of the
1052-5149/04/$ – see front matter D 2004 Elsevier Inc. All rights
doi:10.1016/j.nic.2004.07.003
This article was originally published in Magnetic
Resonance Imaging Clinics of North America 10:3, 2002.
E-mail address: [email protected]
hypopharynx and cervical esophagus and to max-
imize the image quality:
1. Use of dedicated neck coil
2. Perform noncontrasted and contrasted T1-
weighted images and fast-spin-echo T2-
weighted images in axial plane parallel to
the true vocal cords extending from the naso-
pharynx to the thoracic inlet
3. Acquire all sets as contiguous 3-mm images
4. Use field-of-view less than or equal to 16 cm
5. Use image matrix of at least 256 � 256
Other sequences may be used to better evaluate
certain structures, such as the intramural fat planes
(see subsection on cross-sectional anatomy).
Normal anatomy
Descriptive anatomy
The hypopharynx extends from the level of the
hyoid bone to the esophageal verge and the cervical
esophagus from the hypopharynx to the thoracic
inlet. There is no anatomic barrier between the
two structures.
The hypopharynx is subdivided arbitrarily into
three regions: pyriform sinus (one on each side),
postcricoid area, and posterior hypopharyngeal wall.
The pyriform sinus arises at the level of the
aryepiglottic fold and extends inferiorly as an
inverted pyramid to the inferior margin of the cricoid
cartilage. The pyramid tip is called the pyriform sinus
apex. The pyriform sinus is formed by the anterior,
Am 14 (2004) 647 – 662
reserved.

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662648
medial, and lateral walls. Laterally, the superior
aspect of the pyriform sinus is bordered by the
thyrohyoid membrane containing the superior la-
ryngeal neurovascular bundle—a possible pathway
of tumor spread from the pharynx. The sensory axons
of the superior laryngeal nerve connect with the
Arnold nerve within the jugular foramen and are
responsible for the referred otalgia seen with tumors
of the pyriform sinus. The postcricoid area forms the
anterior wall of the hypopharynx. It extends from
the posterior surface of the arytenoid cartilage to the
esophageal verge. Anteriorly, it opens directly into
the larynx. The posterior hypopharyngeal wall
represents the posterior boundary of the hypophar-
ynx. It extends from the level of the top of the
aryepiglottic fold to the esophageal verge and has free
communication to the oropharynx and the esophagus.
It is separated from the vertebral and paravertebral
structures by the retropharyngeal space, which allows
the pharynx to move freely during swallowing.
The wall of the hypopharynx is composed of four
layers: a mucosal lining of stratified squamous
epithelium over loose stroma, a fibrous layer formed
by the pharyngeal aponeurosis, the muscular layer,
and the fascial layer derived from the buccopha-
ryngeal fascia. The loose stroma can be identified on
cross-sectional images as a thin fat plane (see
following subsection). Anteriorly, the muscular layer
consists of the posterior cricoarytenoid muscles and
posteriorly of the middle or inferior constrictor
muscles. The inferior constrictor muscle melts into
the cricopharyngeus muscle inferiorly, which forms
the upper esophageal sphincter at the esophageal
verge. The cervical esophagus abuts the posterior
trachea with a small amount of fatty tissue between
the two. It is lined by non-keratinizing squamous
epithelium over loose areolar tissue surrounded by a
muscular layer of inner circular and outer longitudi-
nal fibers. The muscular layer is covered by a fascial
sheath, which is continuous with the buccopharyn-
geal fascia. The tracheoesophageal (TE) groove abuts
the cervical esophagus on each side and contains the
recurrent laryngeal nerves and the TE groove lymph
nodes. Occasionally, the parathyroid and/or the
thyroid gland extend into the TE groove.
Cross-sectional anatomy
On cross-sectional images, all three components
of the hypopharynx contribute to the structures seen
posterior to the cricoid cartilage (postcricoid portion
of the hypopharynx): the postcricoid area anteriorly
located immediately posterior to the cricoid cartilage,
inferior aspect of the pyriform sinus laterally includ-
ing the pyriform sinus apex, and the posterior
hypopharyngeal wall posteriorly. Since the hypophar-
ynx collapses during MR imaging, the mucosa of the
postcricoid area and posterior hypopharyngeal wall
are in direct contact and are seen as one structure.
Because of their complex anatomy, the postcricoid
portion of the hypopharynx and the esophageal verge
are usually the most challenging images to evaluate.
The knowledge of normative data is essential in
detecting abnormalities [4].
The anteroposterior (AP) dimensions of the
postcricoid portion of the hypopharynx are relatively
constant from the upper to lower margin of the
cricoid cartilage, and an AP diameter of more than
10 mm should be considered abnormal [4]. The
postcricoid area is usually slightly thinner than the
posterior pharyngeal wall (average, 2.5 and 3.5 mm,
respectively) [4]. The transverse dimension of the
postcricoid portion of the hypopharynx tapers from
the upper to the lower margin of the cricoid cartilage.
Observation of lack of normal tapering, particularly
in combination with some other morphologic fea-
tures, such as obscuration of intramural or surround-
ing fat planes, is probably a better indicator of an
underlying abnormality than an overall change in size
[4]. The esophageal diameter varies with the amount
of intraluminal air and is not as useful for evaluation
as the thickness of the esophageal wall itself. An
esophageal wall thickness of less than 5 mm should
be considered normal [4]. The esophageal wall
should also be homogeneously isointense to the sur-
rounding musculature on T2-weighted images
(Fig. 1), demonstrating no signs of enhancement on
the contrasted T1-weighted images [4,5].
The surrounding fat planes lateral to the postcri-
coid portion of the hypopharynx and cervical
esophagus are most consistently seen with the left
side being visualized in most patients followed by the
right lateral fat plane (66% of patients; see Fig. 1) [4].
The posterior fat plane is less frequently seen, with
the best visibility around the esophageal verge (53%
of patients) and in contrast to adjacent levels (20%
of patients) [4]. No differences in visibility of the
surrounding fat planes can be detected with the
various sequences [4]. The fat planes of the TE
groove accommodate the TE groove lymph nodes.
Homogenous-appearing TE groove lymph nodes of
less than 1 cm should be considered normal by
imaging criteria [4,6].
The common wall of the trachea and the esopha-
gus is clearly seen (66% of patients) at the esophageal
verge, with a gradual decrease in frequency more
distally. The contrasted T1-weighted images are
superior to the other sequences in delineation of

Fig. 1. Axial T2-weighted image (repetition time 6000 ms, echo time 91 ms) through the cervical esophagus demonstrates
homogeneous signal intensity of the esophageal wall. The hyperintense curvilinear structure within the center of the esopha-
gus represents the mucosa (.). The fat planes lateral to the cervical esophagus are well demarcated (arrows). The posterior
fat plane is not seen, a common finding at the level of the upper cervical esophagus. p, prevertebral musculature; T, trachea;
v, vertebral body.
Fig. 2. Axial noncontrasted T1- (repetition time [TR] 700 ms, echo time [TE] 15 ms) and gradient echo– (TR 733 ms, TE 18 ms,
flip angle 20�) weighted images through the upper cervical esophagus are shown in (A) and (B), respectively. The gradient
echo–weighted image (B) emphasizes the intact fat plane (arrows) within the common wall of the trachea and esophagus,
which is not as clearly seen on the T1-weighted image (A).
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 649

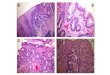
Fig. 3. Noncontrasted T1- (repetition time [TR] 650 ms, echo time [TE] 17 ms) and gradient echo– (TR 550 ms, TE 11 ms, flip
angle 30�) weighted images performed in axial plane at the same level through the hypopharynx demonstrate markedly decreased
visibility of the intramural fat planes (arrowheads) on the T1-weighted image (A) when compared with the gradient echo image
(B). Asymmetry of the intramural fat planes as visualized in (B) can be seen in approximately one third of patients. As in this
case, the left-sided intramural fat planes are typically more obvious. Notice the better delineation of the surrounding fat planes
(arrows) on the gradient echo image with a clear plane toward the prevertebral muscles. c, cricoid cartilage; p, prevertebral
muscles; t, thyroid cartilage; v, vertebral body.
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662650
the common wall of the trachea and the esophagus
(Fig. 2) [4].
The intramural fat planes in the postcricoid
portion of the hypopharynx are especially import
because obliteration of these fat planes might be the
only sign of infiltration by cancer. The visibility of
intramural fat planes decreases in frequency from the
upper to the lower cricoid cartilage (69–30%,
respectively) [4]. The intramural fat planes at the
mid- and lower cricoid levels are identified more
frequently on gradient- echo T2-weighted images
than on T1- or T2-weighted images (Fig. 3) [4]. In
addition, asymmetry of the intramural fat planes is
seen on MR imaging (30% of patients), and typically,
the left-sided fat planes are more obvious [4].
Pathology
Less than 5% of tumors of the hypopharynx and
cervical esophagus are of nonsquamous cell origin
[2]. These include benign tumors, such as lipomas,
retention cysts of minor salivary glands, leiomyomas,
papillomas, adenomas, or angiomatous tumors, and
nonsquamous cell malignancies, such as various
sarcomas, lymphoma, or malignant minor salivary
gland tumors [2,7,8]. Because these lesions are rare,
this article focuses on squamous cell carcinoma of the
hypopharynx and cervical esophagus alone. Pyriform
sinus cancer is the most common subtype of squa-
mous cell carcinoma of this region. Usually, the
definitive diagnosis of hypopharyngeal and esopha-
geal masses requires biopsy, and the radiologist must
recognize high-vascular masses to prevent extensive
bleeding when a biopsy is performed.
Hypopharyngeal and cervical esophageal cancer
are usually indolent and in advanced stage at pre-
sentation. Up to 75% of patients have nodal metas-
tasis and 20% to 40% patients have distant metastasis
at presentation [9]. Even patients with N0 neck have a
30% chance of having occult metastasis on elective
dissections [10].
The most often encountered symptoms are neck
masses secondary to metastatic lymph nodes, dys-
phagia, odynophagia, globus sensation, otalgia,
weight loss, voice changes (bhot potatoQ voice), andfood impaction. The main risk factors are smoking,
alcohol abuse, and previous radiation therapy. Post-
cricoid area tumors are also associated with Plum-
mer-Vinson syndrome, rarely seen in the United
States or continental Europe but commonly encoun-
tered in the United Kingdom [11]. In contrast to
most hypopharyngeal and cervical esophageal
cancers, tumors associated with Plummer-Vinson
syndrome typically occur in women and are hy-
pothesized to come from food stasis caused by
hypopharyngeal or esophageal webs, one of the
main findings besides iron deficiency anemia seen
with this syndrome.
Growth pattern
Overall, hypopharyngeal and cervical esophageal
cancers are predisposed to spread in sub-mucosal
fashion [12]. The submucosal spread is often unde-
tectable on clinical and/or endoscopic examination.

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 651
Otherwise, the various subtypes of the hypopharyng-
eal malignancies have a different spread pattern.
Postcricoid area tumors tend to invade the
posterior aspect of the larynx, causing vocal cord
paralysis and hoarseness. The cricoarytenoid joint
itself is rarely involved. In addition, these tumors
have a high tendency to involve the pyriform sinuses
Fig. 4. Axial noncontrasted (A, C) and contrasted T1- (B, D) weig
72-year-old patient with squamous cell carcinoma of the posterior
gus. (A, B) The noncontrasted T1-weighted image at the level of
(AP) diameter of the postcricoid region (between arrows) measuri
tumor is otherwise difficult to delineate but is clearly seen on the co
(C, D) The noncontrasted (C) and contrasted (D) T1-weighted imag
the cervical diameter in AP and lateral dimensions with 22 mm an
wall of the esophagus cannot be clearly identified as separate struc
fat plane within the common wall of the trachea and esophagus is n
tumor (arrows). E, esophagus; t, trachea.
(100%), trachea (71%), and/or esophagus (71%) [13].
Tracheal or esophageal invasion is missed by endo-
scopic evaluation in approximately 50% of these
patients [13].
Posterior hypopharyngeal wall cancers tend to
spread in a craniocaudal direction and can extend into
the nasopharynx and/or esophagus (Fig. 4) [14]. The
hted images (repetition time 800 ms, echo time 12 ms) of a
pharyngeal wall extending into the upper cervical esopha-
the hypopharynx (A) demonstrates abnormal anteroposterior
ng 13 mm. The normal AP dimension is up to 10 mm. The
ntrasted T1-weighted image at the same level (arrows in B).
es through the upper esophagus show marked enlargement of
d 26 mm, respectively. The muscosal layer and the muscular
tures as expected on contrasted T1-weighted image (D). The
ot seen on either image, consistent with gross invasion by the

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662652
craniocaudal extension of these tumors may occur in
superficial fashion only and remain undetectable on
cross-sectional examination. Rarely, these tumors
cause infiltration of the prevertebral fascia or
musculature at presentation. Even when there is
effacement of the prevertebral fat planes on cross-
sectional imaging, including MR imaging, the diag-
nosis of prevertebral fascia or muscle invasion cannot
be made. Surgical exploration is necessary for
Fig. 5. Axial T2-weighted images (repetition time 6000 ms, echo tim
cancer on the left side. Large nodal metastasis (N) is seen in the
(open arrow). (A) There are signs of invasion of the inferior constr
side seen as thinning of the muscle thickness when compared wi
focal area of disruption of the inferior constrictor muscle (arrows)
the neck at this level. (B) The tumor (T ) is extending between
(arrows) to grossly invade the true vocal cord on the left side in sub
suspected clinically because of the more medial position of the le
internal jugular vein.
definitive diagnosis because of the high false-positive
rate on imaging.
The growth pattern of pyriform sinus cancers
depends on their origin and extent. Tumors arising
from or involving the lateral wall tend to invade
the posterior aspect of the thyroid cartilage and ex-
tend into the soft tissues of the lateral compartment
of the neck (Fig. 5A). Direct infiltration of the
intrinsic laryngeal muscles is rarely seen, in con-
e 99 ms) of a 73-year-old patient with a large pyriform sinus
left neck with significant compression of the jugular vein
ictor muscle (small arrowheads) by the tumor (T) on the left
th the right side (large arrowheads). In addition, there is a
consistent with early invasion of the lateral compartment of
the thyroid cartilage and the cricoarytenoid joint anteriorly
mucosal fashion. The submucosal extension of the tumor was
ft true vocal cord when compared with the right. i, normal

Table 1
Spread pattern of pyriform sinus carcinomas
Lateral wall tumor (%) Medial wall tumor (%)
Tumor involving lateral
and medial wall (%)
Thyroid cartilage 83.3 12.5 60
Cricoid cartilage 0 12.5 20
Arytenoid cartilage 0 12.5 10
Cricoarytenoid joint 0 18.8 5
Paraglottic space 66.7 50 70
Pre-epiglottic space 0 50 35
Tumor outside of thyroid ala 66.7 0 50
Contralateral tumor extension 0 87.5 40
Submucosal spread >8 mm 16.7 56.3 25
Perineural invasiona 0 43.8 55
Thyroid gland 33.3 0 25
a Was always associated with involvement of the laryngeal muscles and never seen as an isolated finding.
Data from Zbaren P, Egger C. Growth pattern of piriform sinus carcinomas. Laryngoscope 1997;107:511–8.
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 653
trast to tumors arising from or involving the medial
wall of the pyriform sinus. The latter show early
laryngeal infiltration with cord fixation (60%;
Fig. 5B) [2,11,14]. Table 1 shows characteristics
in spread pattern of pyriform sinus cancers and
their frequency.
Cervical esophageal tumors tend to involve ana-
tomically adjacent structures, such as the trachea,
Fig. 6. Axial noncontrasted T1-weighted image (repetition time
squamous cell carcinoma of the cervical esophagus (E) illustrates co
fat plane on the left side (arrows). The left lateral fat plane is the
indicate gross extension of the tumor through the esophageal seros
(open arrows).
recurrent laryngeal nerve, and adjacent vasculature
(Fig. 6). In addition, they tend to spread in a sub-
mucosal fashion to the hypopharynx (Fig. 7).
The craniocaudal extension of the hypopharyngeal
tumor into the cervical esophagus and vice versa is
crucial for the extent of surgical resection (limited
versus extensive resection; see later discussion).
Because this type of tumor can spread in a superficial
850 ms, echo time 15 ms) of a 56-year-old patient with
mplete obliteration of the anterior portion of the surrounding
most consistently seen surrounding fat plane. These findings
a. Notice the normal appearance of the right lateral fat plane

Fig. 7. Axial noncontrasted T1-weighted images (repetition time 800 ms, echo time 15 ms) through the upper esophagus (A) and
the hypopharynx (B) of a 69-year-old patient with entirely submucosally located squamous cell carcinoma of the esophagus. The
diagnosis was made by percutaneous biopsy under CT guidance. The anteroposterior (between arrows) and lateral diameters
(between arrowheads in A) of the esophagus are markedly increased with 30 and 33 mm, respectively. The tumor extended in
submucosal fashion into the postcricoid region on the right side reflected as mild posterior bulging of the right postcricoid region
(arrows in B) and lack of intramural fat planes on the right when compared with the left (arrowheads in B).
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662654
or submucosal pattern, a combination of clinical
examination and crosssectional study should be used
in the treatment planning process.
Nodal chain involvement
The three portions of the hypopharynx and
cervical esophagus have slightly different lymphatic
drainage pathways: the postcricoid area tumors tend
to metastasize to group III, IV, and VI lymph nodes
(paratracheal/TE groove); the pyriform sinus tumors
drain primarily into group II, III, and V lymph nodes;
and posterior hypopharyngeal wall cancers have the
tendency primarily to involve the retropharyngeal
lymph nodes and secondarily the internal jugular
chain lymph nodes. In contrast, the other types of
hypopharyngeal cancer involve the retropharyngeal
lymph nodes (15%), but only if the neck is also
positive [9]. The cervical esophageal cancer drains
into group VI and mediastinal lymph nodes. The
group VI lymph nodes are involved usually (71%) at
the time of diagnosis [15].

Table 2
Staging of primary tumors of the hypopharynx
Stage Characteristics
Primary tumor
Tis Carcinoma in situ
T1 Tumor limited to one subsite of hypopharynx and 2 cm or less in greatest dimension
T2 Tumor invades more than one subsite of hypopharynx or an adjacent site, or measures more
than 2 cm but not more than 4 cm in greatest dimension without fixation of hemilarynx
T3 Tumor more than 4 cm in greatest dimension or with fixation of the hemilarynx
T4 Tumor invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, esophagus, or central
compartment soft tissuesa
Central compartment soft tissues includes prelaryngeal strap muscles and subcutaneous fata
Regional lymph nodes
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node, of 3 cm or less in greatest dimension
N2
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm in
greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
a Adapted from American Joint Committee on Cancer. AJCC cancer staging handbook. 6th edition. Philadelphia: Lippincott,
Williams, & Wilkins; 2002.
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 655
Tumor, node, metastases classification
Classification of primary tumors of the hypophar-
ynx and cervical esophagus according to the Amer-
ican Joint Committee on Cancer [16] is listed in
Tables 2 and 3, respectively. The recommended
staging of cervical esophageal lesions is identical to
that of the intrathoracic esophagus.
able 3
taging of primary tumors of the cervical esophagus
tage Characteristics
rimary tumor
Tis Carcinoma in situ
T1 Tumor invades the lamina propria
or submucosa
T2 Tumor invades muscularis propria
T3 Tumor invades adventitia
T4 Tumor invades adjacent structures
egional lymph nodes
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Regional lymph node metastasis
dapted from American Joint Committee on Cancer. AJCC
ancer staging handbook. 6th edition. Philadelphia: Lippin-
ott, Williams, & Wilkins; 2002.
Secondary involvement by other tumors
Direct invasion of the hypopharynx and cervical
esophagus by surrounding tumors is uncommon but
may be seen with advanced head and neck tumors,
thyroid tumors, and bronchogenic carcinomas [17].
Focal areas of increased signal intensity on the
T2-weighted images suggest presence of invasion
[17] (Fig. 8). Focal enhancement following contrast
administration might also be a sign of infiltration;
however, it is not as specific as the T2 changes [17]
(see Fig. 8). Circumferential mass at the level of the
cervical esophagus is the most sensitive and specific
sign of invasion (accuracy, 100%) [17]. An intact fat
plane, absence of wall thickening, and normal
T2 wall signal intensity indicate no invasion with a
very high degree of confidence (see Fig. 1) [17].
Impact of cross-sectional imaging
Multiple published studies document the impact
of cross-sectional imaging on staging of hypophar-
yngeal and/or esophageal cancer [1,2,13,14,18,19].
Most of these studies focus on CT, but the limited
data on MR imaging suggest that a similar or
T
S
S
P
R
A
c
c

Fig. 8. A 77-year-old man with large medullary thyroid cancer (T) on the right side. At the level of the lower hypopharynx, there
are signs of early infiltration of the inferior pharyngeal constrictor muscle on the left side (arrowheads, B). This is clearly
identified on the contrasted T1-(repetition time [TR] 600 ms, echo time [TE] 15 ms) and T2- (TR 5000 ms, TE 99 ms) weighted
images (B and C, respectively), but difficult to appreciate on the noncontrasted T1-weighted image (A). On the noncontrasted
T1-weighted image (A), the absence of the intramural fat planes on the left side when compared with the right (arrows) should
raise the suspicion for tumor invasion. (D) Axial T2-weighted image at the level of the upper cervical esophagus demonstrates
the significant impression of the esophagus from left lateral by the tumor and the gross invasion of the posterior esophageal wall
(arrows) and the left lateral tracheal wall (open arrows).
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662656
even higher percentage in upstaging of tumors is
expected with MR imaging alone [1,2]. Overall,
the clinical tumor stage was increased with cross-
sectional imaging in up to 90% of patients [1,13,14,
18,19]. In up to 67% of patients, the T stage
was changed based on soft tissue involvement
(�88% of patients) or bone/cartilage invasion
(�23% of patients) [13,14,18]. The N stage was
changed in up to 33% of patients [14,18]. According
to Wenig et al [1], the accuracy in tumor staging
improved in 40% of patients with MR imaging alone.
The tumor staging accuracy when compared with
pathologic findings has been reported to be 58% for
clinical examination, 80% for CT, and 85% for MR
imaging [2]. These facts clearly demonstrate the
essential role of cross-sectional imaging in staging
of hypopharyngeal and esophageal cancer. None of
the other cancers of the head and neck region

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 657
shows such a significant impact of cross-sectional
imaging on staging.
Radiologist’s role during pretreatment
As with other cancers of the head and neck region,
the radiologist must report the origin and full extent
of the primary tumor and the nodal status throughout
the neck. The specific issues pertinent to hypophar-
yngeal and esophageal cancer in the following
subsections should be emphasized.
Submucosal spread
Submucosal tumor spread remains undetectable
in a significant number of patients on clinical and
endoscopic examination [12]. The tumor often grows
over a significant distance in submucosal fashion,
precluding planned limited surgical intervention
(see later discussion) in a significant number of
patients. Occasionally, the entire tumor is submucosal
in location and cannot be assessed to endoscopic
biopsy. Under these circumstances, the radiologist
may offer percutaneous biopsy performed with cross-
sectional guidance.
Cartilage involvement
Most radiologists prefer CT for evaluating carti-
lage involvement. This is partially because of the
assumption that cartilage involvement (cartilage
sclerosis and cartilage erosion or lysis) is more easily
detected on CT studies than MR imaging. MR
imaging findings indicating cartilage invasion might
be more difficult to be interpreted by the inexper-
ienced radiologist.
The assessment of MR imaging should include
detection of altered signal intensity of the hyaline
cartilage and bone marrow within it [2]. The invaded
hyaline cartilage typically demonstrates increased T2
and decreased T1 signal intensity [2]. The involved
bone marrow demonstrates decreased attenuation on
T1-weighted images in relation to the uninvolved
fatty replaced bone marrow typically seen in older
patients [2]. Both involved hyaline cartilage and bone
marrow enhance markedly after contrast administra-
tion. With these imaging criteria, a very high
sensitivity (89% to 100%) for detection of cartilage
involvement can be found [1,2]. The problem,
however, is that similar changes can be caused by
reactive inflammation, edema, or fibrosis [2]; there-
fore, MR imaging has an overall specificity of
only 74% to 88%, and an even lower positive pre-
dictive value of 68% to 71% [1,3,20,21]. In addition,
the specificity depends on the cartilage type, as
also demonstrated for CT [2]. The thyroid cartilage
with its variable ossification has the lowest specificity
for cartilage involvement (56%) [2]. Therefore,
thyroid cartilage involvement by tumor should only
be made with caution when based on MR imaging
findings alone. The specificity for cartilage invasion
detection is the highest for arytenoid cartilage (95%)
and intermediate for cricoid cartilage (87%) [2].
Nevertheless, MRimaging is valuable as a good pre-
dictor of the absence of cartilage invasion with
negative predictive values of more than 92% [2,3,
20,21].
Why is it so important to detect involved cartilage
even though it does not play a role in tumor staging
itself? It is well known that nonremoval of an
involved cartilage carries a risk (50–60%) of leaving
tumor behind; therefore, this information is pertinent
for therapy planning, particularly if the patient is
suitable for limited laryngectomy.
Tumor volume
In recent years, emphasis has been placed on
stratifying patients in high- or low-risk groups re-
garding certain treatment modalities and their out-
come. The most important criteria have been volume
of the tumor and cartilage involvement (see previ-
ous discussion).
Pameijer et al [22] found two important prognos-
tic factors for T1 and T2 pyriform sinus cancers
treated with radiation therapy alone: tumor volume
and amount of disease at the pyriform sinus apex
[22]. Although this study was conducted based on CT
imaging findings, the same or similar results are
expected for MR imaging. The authors defined
pyriform sinus apex disease as bminimal apical
diseaseQ if the tumor was less than 10 mm in diameter
at the level of the base of the arytenoid cartilage and
upper 3 mm of the cricoid cartilage or as bbulkyapical diseaseQ if the diameter was greater than or
equal to 10 mm. Their results characterized three
different patient groups with the following criteria
and local control rates if treated with radiation
therapy alone:
Low-risk group: Patients with tumor volume
<6.5 mL and no or minimal apical disease
showed a local control rate of 94% [22].
Moderate-risk group: Patients with tumor volume
of <6.5 mL and bulky apical disease or tumor
volume �6.5 mL and no or minimal apical

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662658
disease demonstrated local control rates of
50% [22].
High-risk group: None of the patients survived
with tumor volume of �6.5 mL and bulky
apical disease [22].
Therefore, reporting of tumor volume and apical
disease should be done for all T1 and T2 stage
pyriform sinus cancers.
Detection of second primary tumors
The rate of second primary tumors in patients with
hypopharyngeal or cervical esophagus cancer is
higher than for the remainder of head and neck
cancers, with a reported frequency of up to 15% [9].
In 25% of patients, the second primary tumor (syn-
chronous lesion) is found at the time of the diagnosis
of the hypopharyngeal or esophageal cancer and in
75% of patients at other times (metachronous lesion)
[9]. Therefore, every cross-sectional study, including
posttreatment examinations, should be evaluated for
a second primary tumor.
Radiologist’s role during treatment
Currently, the radiologist does not play a signifi-
cant role during the treatment phase itself unless the
patient requires a percutaneous feeding tube place-
ment or complications occur, such as development of
fistula, vascular rupture requiring embolization, or
abscess formation. Advances in current therapy
options and development of new treatment regimes,
however, may require the radiologist to take an
active role in the therapy delivery, such as intra-
arterial administration of chemotherapy and intra-
arterial or percutaneous administration of gene
therapy agents.
The published results for intravenous administra-
tion of induction, neoadjuvant, or adjuvant chemo-
therapy have been rather disappointing because all of
these studies demonstrated no significant differences
in survival or local control [23–25]. The addition of
chemotherapy to other treatment options, however,
significantly reduced the incidence of distant meta-
stasis [23–25]. Cisplatin-based chemotherapy agents
showed the most effect upon head and neck cancers,
which might be due to higher sensitivity of esoph-
ageal cell lines to cisplatin as suggested by Kovacs
et al [26]. Potentially this might also apply to the cell
line of the hypopharyngeal region. Published results
of intra-arterial administration of a supradose of
cisplatin into the tumor supplying vessels combined
with concurrent radiation therapy (bRADPLAT pro-
tocolQ) suggest a significantly increased rate of local
control in advanced head and neck tumors (80%) and
an improved 5-year disease-specific and overall
survival rate (54% and 39%, respectively) [27].
Preliminary results of the RADPLAT protocol
applied to pyriform sinus cancers specifically showed
a complete local response rate of 92% and of 76% at
the nodal site and the 5-year disease-specific and
overall survival rates (of 50% and 23%, respectively)
[28]. These survival rates are similar or slightly
higher than reported by other treatment modalities;
however, the main advantage of this treatment regime
is the very high organ preservation rate (88%) with
adequate voice preservation (88%) and acceptable
swallowing abilities at 6-month and 12-month fol-
low-up (50% and 67%, respectively) [28]. Samant
et al [28] noted an altered pattern of failure with
shift from local recurrences to distant metastasis. No
data regarding other sites of the hypopharynx or
cervical esophagus are available.
Radiologist’s role during posttreatment
Currently, most tumors of the hypopharynx and
cervical esophagus present at advanced stage and,
therefore, only a relatively small percentage of
patients can undergo organ preservation therapy, such
as seen with the larynx, sparing surgical resection or
radiation therapy alone. Most patients undergo total
laryngectomy with resection of the entire larynx,
pyriform sinuses, surrounding strap muscles, and
various options for reconstruction of the pharynx (eg,
primary closure with hypopharyngeal mucosa and
inferior constrictor muscles, jejunal interposition, or
gastric pull-up) [29]. Often, these patients also
receive pre- or postsurgery radiation therapy, possibly
combined with chemotherapy. Despite the extensive
treatment protocols, the 5-year survival rates are
dismal (range, 20–34%), with local recurrence rates
of 32% to 46% at 2 years for advanced hypophar-
yngeal and cervical esophageal cancers [10,29,30].
The addition of pre-surgery radiation therapy also
has a high incidence of postsurgical complications
(47%) [30].
Postradiation therapy
Postradiotherapy changes sometimes are difficult
to be distinguished from recurrent tumor on clinical
examination. Therefore, the referring physicians rely
on imaging evaluation. Up to 40% of recurrent
tumors are detected with cross-sectional imaging

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 659
prior to visibility on clinical examination [30]. To
allow easier and faster detection of recurrent or
persistent tumor, a follow-up CT and/or MR imaging
study is recommended at 3 to 4 months following
completion of radiation therapy. Hermans et al [31]
characterized three groups of patients based on the
3-to 4-month follow-up CT scans of patients treated
for laryngeal or hypopharyngeal carcinoma:
1. None of the patients showed local failure if
complete resolution of the tumor and symmet-
ric-appearing soft tissue planes were seen on
the baseline CT examination at 3 to 4 months
following completion of radiation therapy. This
patient group requires continued clinical fol-
low-up and cross-sectional imaging only if
suspicion for recurrent tumor is raised on the
clinical examination [31].
2. Patients with tumor volume reduction of <50%
or a persistent mass of �1 cm in diameter
demonstrated a high likelihood of local failure,
with failure rates of 100% and 30%, respec-
tively. These patients should undergo immedi-
ate further investigation with biopsy for lesions
with less than 50% response in tumor volume.
In patients with a persistent mass of �1 cm in
diameter, follow-up imaging at 3 to 4 months,
fluorine-18 fluorodeoxyglucose (FDG) positron
emission tomography scan and/or biopsy are
appropriate alternatives [31,32].
3. If the baseline CT shows a residual mass of <1
cm in diameter or asymmetry, of the soft tissue
planes, cross-sectional follow-up at 3-to
4-month intervals for 2 years should be
performed if there is no clinical suspicion for
recurrent tumor [31]. Two consecutive stable
studies after the baseline study are consistent
with control at the primary site.
Although all results were conducted on CT
imaging alone, MR imaging studies are expected to
yield the same data [31].
In the same study, Hermans et al [31] also
evaluated cartilage alterations and likelihood of
recurrence. They found that a persistent mass �1 cm
in diameter in association with cartilage changes
should be considered as local failure. Minimal soft
tissue asymmetry and cartilage changes should be
closely monitored because these changes could be
caused by recurrent tumor or chondronecrosis [30].
It is uncertain if the results regarding cartilage
alteration can be transferred, and to what degree, to
MR imaging studies. Fluorine-18 FDG positron
emission tomography may also gain a dominant
role in posttreatment evaluation of patients with
hypopharyngeal and/or cervical esophageal cancer
treated with the newer, more aggressive type of
therapy options as more results are published in this
regard [33].
Postsurgery
Recurrent tumors typically occur at the margins of
the resection or within the deep tissues of the neck in
surgical patients. Therefore, it is pertinent that the
radiologist is familiar with the normal appearance of
the reconstructed pharynx and possible complica-
tions. The most commonly encountered complica-
tions are fistula formation (26%), wound infection
(22%), and stricture (9%) [10,34].
Currently, the methods of hypopharyngeal recon-
struction most often employ the jejunal free flap, with
microvascular anastomosis, or the gastric pull-up.
Pectoralis major myocutaneous and radial forearm
flaps may be used for subtotal hypopharyngeal
defects in which a posterior stripe of mucosa remains
intact. Their use is precluded if extension of the
tumor into the cervical esophagus is present. The use
of the radial forearm flap over jejunal interposition
has the advantage of improved swallowing function
[35]. The pectoralis flap is associated with higher
incidence of fistulas and strictures, which may be
because of difficulty in formation of the required
tubal shape secondary to lack of pliability. A free
jejunal graft with microvascular anatostomosis is the
reconstructive method of choice for lesions of the
hypopharynx that require total pharyngectomy for
reconstruction of extensive defects and for limited
invasion of the cervical esophagus. The jejunal graft
has a low incidence of strictures and fistula formation
and tolerates postoperative radiation therapy better
than any other method of reconstruction [36]. Occa-
sionally, dysphagia and stasis symptoms may be seen
because of a kink in the conduit if a too-long jejunal
interposition was chosen [36]. Gastric pull-up is the
reconstruction method of choice in patients with
cervical esophagus involvement of a longer segment.
It shows a low rate of fistula formation, but dumping
and reflux are frequent patient complaints.
On cross-sectional images, the appearance of the
mucosa is not very helpful in evaluating recurrent
tumor because single or multiple irregular-appearing
folds are typically seen in jejunal inter-position and
with gastric pull-up. The evaluation of cross-sectional
imaging studies should instead focus on regular
thickness and smooth external margins of the neo-
pharyngeal wall (Fig. 9) [2].

Fig. 9. Sagittal noncontrasted T1- (repetition time [TR] 700 ms, echo time [TE] 15 ms) weighted image of a 72-year-old man
demonstrates the craniocaudal extent of the squamous cell cancer of the posterior pharyngeal wall (arrows in A). (A, B) The
bulk of the tumor is superior to the cricoid cartilage (c), but it is extending into the postcricoid region. The axial noncontrasted
T1-weighted image (TR 500 ms, TE 15 ms) confirms the left-sided tumor (T) in the postcricoid region identified as absence
of the intramural fat plane on the left when compared with the right (arrowheads in B). This patient underwent total
laryngectomy and pharyngectomy with jejunal interposition. (C) Axial contrasted T1- (TR 500 ms, TE 17 ms) weighted
image through the neopharynx performed 2 years after the surgery shows a polypoid lesion (white arrows) along the right
lateral wall of the jejunal interposition. Because the external wall of the neopharynx (black arrows) is well defined, this
should be considered a mucosal fold rather than mistaken for recurrent tumor.
I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662660

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662 661
References
[1] Wenig BL, Ziffra KL, Mafee MF, et al. MR imaging of
squamous cell carcinoma of the larynx and hypophar-
ynx. Otolaryngol Clin North Am 1995;28:609–19.
[2] Becker M. Larynx and hypopharynx. Radiol Clin
North Am 1998;36:891–920.
[3] Castelijns JA, Gerritsen GJ, Kaiser MC, et al. Invasion
of laryngeal cartilage by cancer: comparison of CT and
MR imaging. Radiology 1987;166:199–206.
[4] Schmalfuss IM, Mancuso AA, Tart R. Postcricoid
region and cervical esophagus:normal appearance at
CT and MRimaging. Radiology 2000;214:237–46.
[5] Quint L, Glazer G, Orringer M. Esophageal imaging
by MR CT: study of normal anatomy and neoplasms.
Radiology 1985;156:727–31.
[6] Glazer GM, Gross BH, Quint LE, et al. Normal
mediastinal lymph nodes: number and size according
to American Thoracic Society mapping. AJR Am J
Roentgenol 1985;144:261–5.
[7] Hovelmann B, Pau HW. Diagnostische schwierigkeiten
bei gutartigen hypopharynxgeschwulsten. Laryngo-
Rhino-Otol 1991;70:239–42.
[8] Jungehulsing M, Fischbach R, Pototschnig C, et al.
Rare benign tumors: laryngeal and hypopharyngeal
lipomata. Ann Otol Rhinol Laryngol 2000;109:301–5.
[9] Million RR. Pharyngeal walls, pyriform sinus, post-
cricoid pharynx. In: Million RR, editor. Management
of head and neck cancer. Philadelphia7 JB Lippincott,
1994. p. 502–32.
[10] Kraus DH, Zelefsky MJ, Brock HA, et al. Combined
surgery and radiation therapy for squamous cell
carcinoma of the hypopharynx. Otolaryngol Head
Neck Surg 1997;116:637–41.
[11] Zbaren P, Egger C. Growth pattern of piriform sinus
carcinomas. Laryngoscope 1997;107:511–8.
[12] Saleh E, Mancuso AA, Stringer S. Relative roles of
computed tomography and endoscopy for determining
the inferior extent of pyriform sinus carcinoma:
correlative histopathologic study. Head Neck 1993;
15:44–52.
[13] Aspestrand F, Kolbenstvendt A, Boysen M. Carcinoma
of the hypopharynx: CT staging. J Comput Assist
Tomogr 1990;14:72–6.
[14] Nowak B, Di Martino E, Janicke S, et al. Diagnostic
evaluation of malignant head and neck cancer by F-18-
FDG PET compared to CT/MRI. in GermanNuklear-
medizin 1999;38:312–8.
[15] Weber RS, Marvel J, Smith P, et al. Paratracheal lymph
node dissection for carcinoam of the larynx, hypo-
pharynx and cervical esophagus. Otolaryngol Head
Neck Surg 1993;108:11–7.
[16] American Joint Committee on Cancer. AJCC cancer
staging handbook. 6th edition. Philadelphia7 Lippin-
cott, Williams, & Wilkins; 2002.
[17] Roychowdhury S, Laevner LA, Yousem DM, et al.
MR imaging for predicting neoplastic invasion of the
cervical esophagus. AJNR Am J Neuroradiol 2000;
21:1681–7.
[18] Prehn RB, Pasic TR, Harari PM, et al. Influence of
computed tomography on pretherapeutic tumor staging
in head and neck cancer patients. Otolaryngol Head
Neck Surg 1998;119:628–33.
[19] Thabet HM, Sessions DG, Gado MH, et al. Compar-
ison of clinical evaluation and computed tomographic
diagnostic accuracy for tumors of the larynx and
hypopharynx. Laryngoscope 1996;106:589–94.
[20] Becker M, Zbaren P, Laeng H, et al. Neoplastic
invasion of the laryngeal cartilage: comparison of
MR imaging and CT with histopathologic correlation.
Radiology 1995;194:661–9.
[21] Zbaren P, Begger M, Laeng H. Pretherapeutic staging
of laryngeal cancer: clinical findings, computed
tomography and magnetic resonance imaging versus
histopahtology. Cancer 1996;77:1263–73.
[22] Pameijer FA, Mancuso AA, Mendenhall WM, et al.
Evaluation of pretreatment computed tomography as a
predictor of local control in T1/T2 pyriform sinus
carcinoma treated with definitive radiotherapy. Head
Neck 1998;20:159–68.
[23] Adjuvant chemotherapy for advanced head and neck
squamous carcinomas. Final report of the Head and
Neck Contracts Program. Cancer 1987;60:301–11.
[24] Laramore GE, Scott CB, Al-Sarraf M, et al. Adjuvant
chemotherapy for resectable squamous cell carcinomas
of the head and neck: report on intergroup study 0034.
Int J Radiat Oncol Biol Phys 1992;23:705–13.
[25] Paccagnella A, Orlando A, Marchiori C, et al. Phase III
trail of initial chemotherapy in stage III or IV head and
neck cancers: a study by the Gruppo di Studio Sui
Tumori Della Testa e Del Collo. J Natl Cancer Inst
1994;86:265–72.
[26] Kovacs AF, Cinatl Jr J. In vitro cytotoxic close-relation
of cisplatin and sodium thiosulphate in human tongue
and oesophageal squamous carcinoma cell lines.
J Craniomaxillofac Surg 2002;30:54–8.
[27] Robbins KT, Kumar P, Wong FS, et al. Targeted
chemoradiation for advanced head and neck cancer:
analysis of 213 patients. Head Neck 2000;22:687–93.
[28] Samant S, Kumar P, Wan J, et al. Concomitant
radiation therapy and targeted cisplatin chemotherapy
for the treatment of advanced pyriform sinus carci-
noma: disease control and preservation of organ
function. Head Neck 1999;21:595–601.
[29] Kraus DH, Pfister DG, Harrison LB, et al. Larynx
preservation with combined chemotherapy and radia-
tion therapy in advanced hypopharynx cancer. Otolar-
yngol Head Neck Surg 1994;148:31–7.
[30] Pawlik AB, Stockli SJ, Schmid S. Salvage surgery
in laryngeal and hypopharyngeal carcinoma. in
GermanSchweiz Med Wochenschr Suppl 2000;116:
27S–30S.
[31] Hermans R, Pameijer FA, Mancuso AA, et al. Laryn-
geal or hypopharyngeal squamous cell carcinoma:
can follow-up CT after definitive radiation therapy
be used to detect local failure earlier than clinical
examination alone? Radiology 2000;214:683–7.
[32] Mukherji SK, Mancuso AA, Kotzur IM, et al. Radio-

I.M. Schmalfuss / Neuroimag Clin N Am 14 (2004) 647–662662
logic appearance of the irradiated larynx. Part 2. Pri-
mary site response. Radiology 1994;193:149–54.
[33] Kitagawa Y, Nishizawa S, Sano K, et al. Prospective
comparison of 18-FDG PET with conventional imag-
ing modalities (MRI, CT, and 67 Ga scintigraphy) in
assessment of combined intraarterial chemotherapy
and radiotherapy for head and neck carcinoma. J Nucl
Med 2003;44:198–206.
[34] Wei WI, Lam KH, Choi S, et al. Late problems after
pharyngolaryngoesophagectomy and pharyngogastric
anastomosis for cancer of the larynx and hypopharynx.
Am J Surg 1984;148:509–13.
[35] Anthony JP, Singer MF, Mathes SJ, et al. Pharyngoe-
sophgeal reconstruction using the tube free radial
forearm flap. Clin Plast Surg 1994;21:137–47.
[36] Reece GP, Schusterman MA, Miller MJ, et al. Morbid-
ity and functional outcome of free jejunal transfer
reconstruction for circumferential defects of the phar-
ynx and cervical esophagus. Plast Reconstr Surg 1995;
96:1307–16.