Embed Size (px)
Citation preview
Imani K. Thornton, M.D.
St. Joseph Mercy OaklandAnesthesiology/Surgical Critical Care
Assistant Clinical ProfessorWayne State University
� NO DISCLOSURES
� “We need to give more fluid because the UOP is low….”
� “We need to give more fluid because the patient had a bowel prep…….”
� “We need to give more fluid because the patient is requiring phenylephrine…….”
� “We need to give more fluid because the patient has an epidural……..”
� “These patients are at increased risk of “pre-renal” kidney injury……….”
� Reasons for giving fluid¡ Urine output¡ Urine color¡ Urine concentration¡ Surgery type¡ Bowel prep (up to 4L)¡ ??Insensible losses¡ NPO ‘losses¡ 3:1 replacement of EBL¡ Tachycardia¡ Hypotension¡ “Maintenance” fluid hourly¡ 4:2:1 rule¡ Non-vigilance (leaving IV fluids open and running entire case)¡ Predicted response to induction
A LOT OF
FLUID
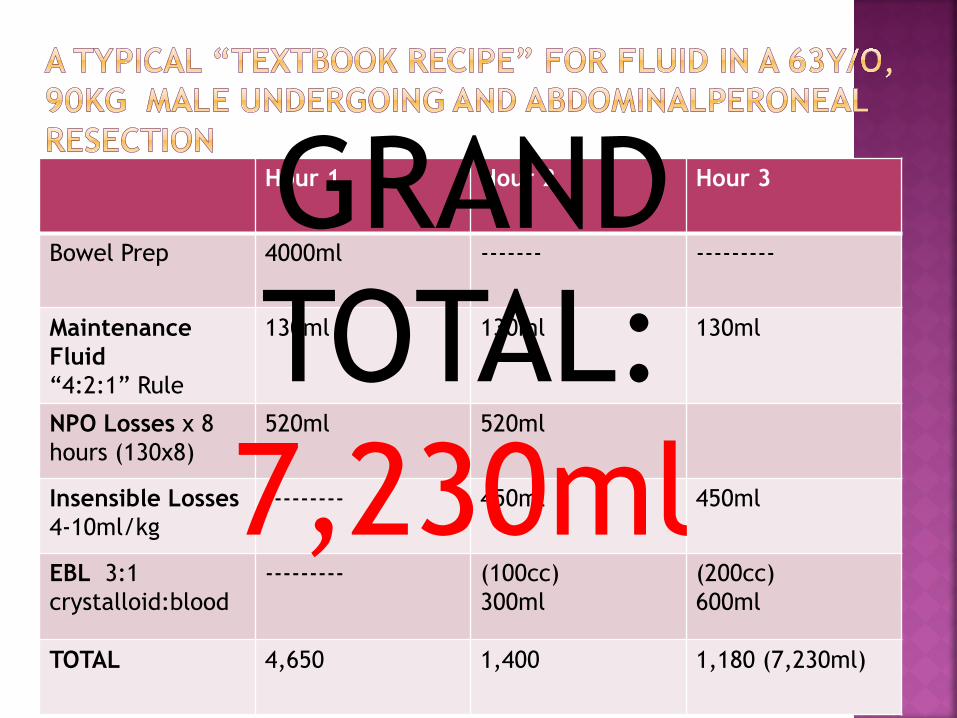
Hour 1 Hour 2 Hour 3
Bowel Prep 4000ml ------- ---------
MaintenanceFluid“4:2:1” Rule
130ml 130ml 130ml
NPO Losses x 8 hours (130x8)
520ml 520ml
Insensible Losses4-10ml/kg
--------- 450ml 450ml
EBL 3:1 crystalloid:blood
--------- (100cc)300ml
(200cc)600ml
TOTAL 4,650 1,400 1,180 (7,230ml)
GRAND TOTAL: 7,230ml

http://www.jnaccjournal.org/articles/2017/4/1/images/JNeuroanaesthesiolCritCare_2017_4_1_17_197439_f1.jpg
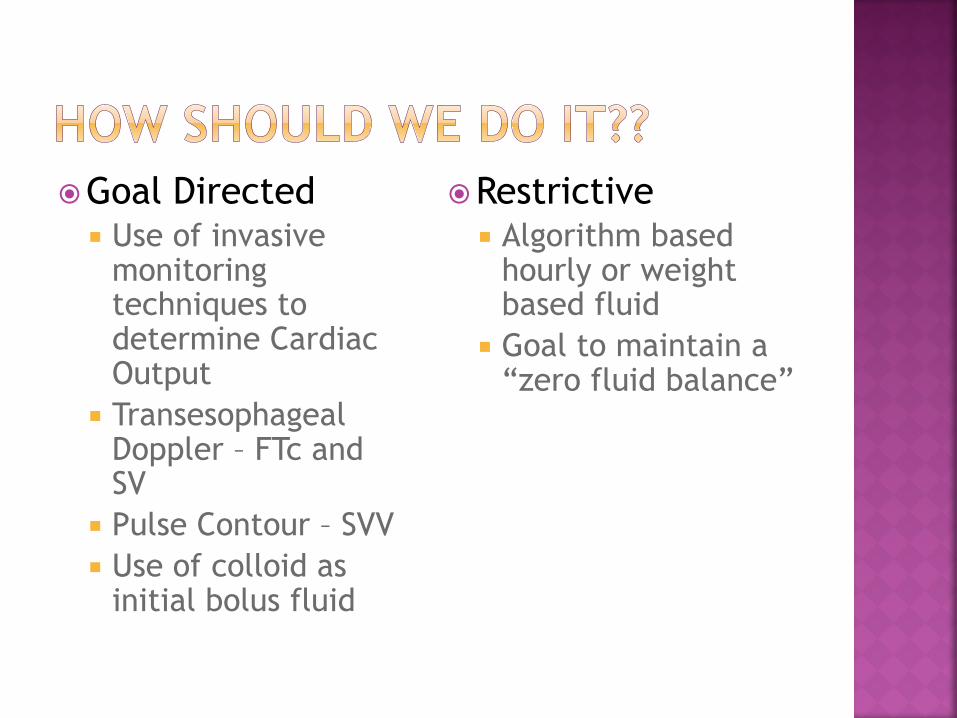
�Goal Directed¡ Use of invasive
monitoring techniques to determine Cardiac Output
¡ Transesophageal Doppler – FTc and SV
¡ Pulse Contour – SVV¡ Use of colloid as
initial bolus fluid
�Restrictive¡ Algorithm based
hourly or weight based fluid
¡ Goal to maintain a “zero fluid balance”
� GDFT¡ Individualized care¡ May help avoid
unnecessary fluid therapy and fluid overload
¡ Requires add’lequipment
¡ $$$¡ Difficult to implement
wide-spread¡ Many interferences
with fluid responsivenes intraop
� RESTRICTIVE¡ $ - Cheaper¡ Easier¡ Not individualized¡ No visual data to
adjust¡ Tissue hypoperfusion
a risk if excessive¡ Fluid responsiveness
NOT evaluated real-time
� GDFT¡ Transesophageal doppler guided shown to reduce
LOS and postoperative complications in several RCTs¹
¡ Pulse Contour guided shown to decrease morbidity and accelerate recovery²
¡ Benefits more apparent in high risk patients3
¡ American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative(POQI) recommend the use of GDFT when available
(1) Gan TJ, et al. Goal-directed intraoperative fluid administration reduces length of stay after major surgery.
Anesthesiology 2002; 97: 820-6: Conway,et al. 2002, Noblet et al. 2006, Wakeling et al. 32005
(2) Benes J et al. The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Crit Care 2014: Benes J et al 2010, Pearse R et al. 2005: Feldheiser et al 2012
(3)Pearse et al. JAMA 2014: Hamilton et al. Anesth Analg 2011
� RESTRICTIVE¡ No difference in length of stay or incident
complications vs. GDFT1
¡ Shown to decrease morbidity vs. liberal approach in many studies2
¡ Fluid excess proven to increase surgical morbidity in multiple randomized trials3
(1)Phan et al. 2014; Brandstrup et al. 2012; Srinvase et al 2013(2)Wind et al. 2006; Kehlet et al. 2008,Lassen et all 2009; Rahbari et al
2009;Holte et al 2007
(3)Brandstrup et al 2003; Nisanevich et al 2005; Lobo et al 2002; Abraham-Nordling et al 2012
CRYSTALLOID COLLOID
� Normal Saline??� Balanced isotonic
solutions (LR, Plasmalyte)??
� NS Hyperchloremia
Kidney dysfunction, prolonged hospital stay and increased mortality* Increased risk of fluid overload
� HES� Albumin� Better blood volume
expanders� Less interstitial space
overload� May increase incidence
of AKI and impair hemostasis (HES)
� Most data in critical care literature (not perioperative)

Liberal or restrictive fluid administration in fast-track colonicsurgery: a randomized, double-blind study†
K. Holte1*, N. B. Foss2, J. Andersen1, L. Valentiner1, C. Lund2, P. Bie3 and H. Kehlet4
1Department of Surgical Gastroenterology and 2Department of Anaesthesiology, Hvidovre UniversityHospital, DK-2650 Hvidovre, Denmark. 3Department of Physiology and Pharmacology, University of
Southern Denmark, Denmark. 4Section for Surgical Pathophysiology, Rigshospitalet, Denmark
*Corresponding author. E-mail: [email protected]
Background. Evidence-based guidelines on optimal perioperative fluid management have notbeen established, and recent randomized trials in major abdominal surgery suggest that largeamounts of fluid may increase morbidity and hospital stay. However, no information is availableon detailed functional outcomes or with fast-track surgery. Therefore, we investigated theeffects of two regimens of intraoperative fluids with physiological recovery as the primaryoutcome measure after fast-track colonic surgery.
Methods. In a double-blind study, 32 ASA I–III patients undergoing elective colonic surgerywere randomized to ‘restrictive’ (Group 1) or ‘liberal’ (Group 2) perioperative fluid adminis-tration. Fluid algorithms were based on fixed rates of crystalloid infusions and a standardizedvolume of colloid. Pulmonary function (spirometry) was the primary outcome measure, withsecondary outcomes of exercise capacity (submaximal exercise test), orthostatic tolerance,cardiovascular hormonal responses, postoperative ileus (transit of radio-opaque markers),postoperative nocturnal hypoxaemia, and overall recovery within a well-defined multimodal,fast-track recovery programme. Hospital stay and complications were also noted.
Results. ‘Restrictive’ (median 1640 ml, range 935–2250 ml) compared with ‘liberal’ fluidadministration (median 5050 ml, range 3563–8050 ml) led to significant improvement in pul-monary function and postoperative hypoxaemia. In contrast, we found significantly reducedconcentrations of cardiovascularly active hormones (renin, aldosterone, and angiotensin II) inGroup 2. The number of patients with complications was not significantly different betweenthe groups (1 vs 6 patients, P¼0.08).
Conclusions. A ‘liberal’ fluid regimen led to a transient improvement in pulmonary functionand postoperative hypoxaemia but no other differences in all-over physiological recovery com-pared with a ‘restrictive’ fluid regimen after fast-track colonic surgery. Since morbidity tendedto be increased with the ‘restrictive’ fluid regimen, future studies should focus on the effect ofindividualized ‘goal-directed’ fluid administration strategies rather than fixed fluid amounts onpostoperative outcome.
Br J Anaesth 2007; 99: 500–8
Keywords: anaesthesia, general; complications, respiratory; fluids, i.v.; recovery, postoperative;surgery, gastrointestinal
Accepted for publication: May 17, 2007
Perioperative fluid management and its implications foroutcome in elective surgery are controversial and there isa large variability in fluid regimens in daily practice.1 – 4 Inlaparoscopic cholecystectomy (medium-size procedure),a recent randomized study found that intraoperative admin-istration of 40 ml kg21 (!3 litre) compared with 15 mlkg21 (!1 litre) Ringer’s lactate (RL) reduced the cardio-vascular hormonal responses [antidiuretic hormone
†Kathrine Holte participated in study design, data collection, dataanalysis and wrote the paper. Nicolai Foss participated in study design,data collection, data analysis and revised the paper. Jens Andersenparticipated in study design, data analysis and revised the paper. LotteValentiner participated in data collection and revised the paper. ClausLund participated in study design, data collection, data analysis andrevised the paper. Peter Bie participated in data collection, data analysisand revised the paper. Henrik Kehlet generated the idea for the study,participated in study design and data analysis, and revised the paper.
# The Board of Management and Trustees of the British Journal of Anaesthesia 2007. All rights reserved. For Permissions, please e-mail: [email protected]
British Journal of Anaesthesia 99 (4): 500–8 (2007)
doi:10.1093/bja/aem211 Advance Access publication August 6, 2007
Copyright 2014 American Medical Association. All rights reserved.
Effect of a Perioperative, Cardiac Output–GuidedHemodynamic Therapy Algorithm on OutcomesFollowing Major Gastrointestinal SurgeryA Randomized Clinical Trial and Systematic ReviewRupert M. Pearse, MD; David A. Harrison, PhD; Neil MacDonald, FRCA; Michael A. Gillies, FRCA; Mark Blunt, FRCA; Gareth Ackland, PhD; Michael P. W. Grocott, MD;Aoife Ahern, BSc; Kathryn Griggs, MSc; Rachael Scott, PhD; Charles Hinds, FRCA; Kathryn Rowan, PhD; for the OPTIMISE Study Group
IMPORTANCE Small trials suggest that postoperative outcomes may be improved by the useof cardiac output monitoring to guide administration of intravenous fluid and inotropic drugsas part of a hemodynamic therapy algorithm.
OBJECTIVE To evaluate the clinical effectiveness of a perioperative, cardiac output–guidedhemodynamic therapy algorithm.
DESIGN, SETTING, AND PARTICIPANTS OPTIMISE was a pragmatic, multicenter, randomized,observer-blinded trial of 734 high-risk patients aged 50 years or older undergoing majorgastrointestinal surgery at 17 acute care hospitals in the United Kingdom. An updatedsystematic review and meta-analysis were also conducted including randomized trialspublished from 1966 to February 2014.
INTERVENTIONS Patients were randomly assigned to a cardiac output–guided hemodynamictherapy algorithm for intravenous fluid and inotrope (dopexamine) infusion during and 6hours following surgery (n=368) or to usual care (n=366).
MAIN OUTCOMES AND MEASURES The primary outcome was a composite of predefined30-day moderate or major complications and mortality. Secondary outcomes were morbidityon day 7; infection, critical care–free days, and all-cause mortality at 30 days; all-causemortality at 180 days; and length of hospital stay.
RESULTS Baseline patient characteristics, clinical care, and volumes of intravenous fluid weresimilar between groups. Care was nonadherent to the allocated treatment for less than 10% ofpatients in each group. The primary outcome occurred in 36.6% of intervention and 43.4% ofusual care participants (relative risk [RR], 0.84 [95% CI, 0.71-1.01]; absolute risk reduction, 6.8%[95% CI, −0.3% to 13.9%]; P = .07). There was no significant difference between groups for anysecondary outcomes. Five intervention patients (1.4%) experienced cardiovascular seriousadverse events within 24 hours compared with none in the usual care group. Findings of themeta-analysis of 38 trials, including data from this study, suggest that the intervention isassociated with fewer complications (intervention, 488/1548 [31.5%] vs control, 614/1476[41.6%]; RR, 0.77 [95% CI, 0.71-0.83]) and a nonsignificant reduction in hospital, 28-day, or30-day mortality (intervention, 159/3215 deaths [4.9%] vs control, 206/3160 deaths [6.5%]; RR,0.82 [95% CI, 0.67-1.01]) and mortality at longest follow-up (intervention, 267/3215 deaths[8.3%] vs control, 327/3160 deaths [10.3%]; RR, 0.86 [95% CI, 0.74-1.00]).
CONCLUSIONS AND RELEVANCE In a randomized trial of high-risk patients undergoing majorgastrointestinal surgery, use of a cardiac output–guided hemodynamic therapy algorithmcompared with usual care did not reduce a composite outcome of complications and 30-daymortality. However, inclusion of these data in an updated meta-analysis indicates that theintervention was associated with a reduction in complication rates.
TRIAL REGISTRATION isrctn.org Identifier: ISRCTN04386758
JAMA. 2014;311(21):2181-2190. doi:10.1001/jama.2014.5305Published online May 19, 2014.
Editorial page 2177
Author Audio Interview atjama.com
Supplemental content atjama.com
Author Affiliations: Queen MaryUniversity of London, London,England (Pearse, MacDonald, Ahern,Hinds); Intensive Care National Auditand Research Centre, London,England (Harrison, Griggs, Scott,Rowan); Critical Care Unit, Universityof Edinburgh, Edinburgh, Scotland(Gillies); Critical Care Unit, QueenElizabeth Hospital, King’s Lynn,England (Blunt); University CollegeLondon, London, England (Ackland);Integrative Physiology and CriticalIllness Group, University ofSouthampton, Southampton,England (Grocott).
Group Information: The members ofthe OPTIMISE Study Group are listedat the end of this article.
Corresponding Author: Rupert M.Pearse, MD, Adult Critical Care Unit,Royal London Hospital, London, E11BB, England ([email protected]).
Section Editor: Derek C. Angus, MD,MPH, Associate Editor, JAMA([email protected]).
Research
Original Investigation | CARING FOR THE CRITICALLY ILL PATIENT
2181
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jamanetwork.com/pdfaccess.ashx?url=/data/journals/jama/930297/ on 04/23/2017
� Less fluid as part of an enhanced recovery program has been shown to decrease surgical morbidity
� Isotonic chloride poor solutions may be better than Normal saline and high volume colloids
� Colloid alone vs. low chloride crystalloids have not yet been evaluated in the perioperative setting
� Widespread implementation of Goal-Directed Fluid Therapy may not be necessary to achieve benefits of an enhanced recovery program
� What exactly does “restrictive” fluid management mean???¡ Lack of standardization in the research¡ Data pooling is challenging
� Who gains the most benefit from GDFT or is it even necessary at all????¡ May be difficult to do in centers with limited
resources� Is the increased expense and possible
complications of colloid worth the effort??¡ Most studies used at least some colloid in both
intervention and control groups

� Abraham-Nordling M, Hjern F et al. Randomized clinical trial of fluid restriction in colorectal surgery. Br J Surg 2012; 99: 186-191
� Benes J, Chytra I, et al. Intraoperative fluid optimization using stroke volume variation in high risk surgical patients: results of prospective randomized study. Crit Care 2010;14: R118
� Benes J, Giglio M, et al. The effects of goal directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Crit Care 2014; 18: 584
� Brandstrup B, Tonnesen H, et al. Danish Study Group on Perioperative Fluid Therapy. Effects of intravenous fluid restriction on postoperative complication: comparisons of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial. Ann Surg 2003 238: 641-648
� Brandstrup B, Svendson PE, et al. Which goal for fluid therapy during colorectal surgery is followed by the best outcome: near-maximal stroke volume or zero fluid balance? Br J Anaesth. 2012;109:191-9
� Conway DH, Mayall R et al. Randomised controlled trial investigating the influence of intravenous fluid titration using oesophageal Doppler monitoring during bowel surgery. Anaesthesia 2002; 57: 845-9
� Feldheiser A., Aziz O et al. Enhanced Recover After Surgery (ERAS) for gastrointestinal surgery, part 2: consensus statement for anaesthesiapractice. Acta Anaesthesiologica Scandinavica 60(2916) 239-334
� Feldheiser A, Conroy P et al. Anaesthesia Working Group of the Enhanced Recovery After Surgery. Development and feasibility study of an algorithm for intraoperative goaldirected haemodynamic management in anoncardiac surgery. J Int Med Res 2012; 40: 1227-41
� Gan TJ, Soppitt A, et al. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 2002; 97: 820-6
� Hamilton MA, Cecconi M, Rohdes A. A systematic review and meta-analysis on the use of preemptive hemodynamic intervention to improve postoperative outcomes in moderate and high-risk surgical patients. Anesth Analg 2011; 112: 1392-402
� Holte K, Foss NB et al. Liberal or restrictive fluid administration in fast track colonic surgery. A rendomized, double-blinded study. Br J Anaesth2997;99:500-508
� Hubner, M, Lovely JK et al. Intrathecal Analgesia and Restrictive Perioperative Fluid Management within Enhanced Recovery Pathway: Hemodynamic Implications. J Am Coll Surg 2013; Vol. 216, No. 6: 1124-34
� Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg 2008; 248: 189-98
� Lobo DN, Bostok KA et al. Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection: a randomisedcontrolled trial. Lancet 2002; 359: 1812-18
� Nisanevich V, Felsenstrin I et al Effect of intraoperative fluid management on outcome after intraabdomial surgery. Anesthesiology 2005: 103: 25-32
� Noblett SE, Snowden CP, et al. Randomized clinical trial assessing the effect of Doppler-optimized fluid management on outcome after elective colorectal resection. Br J Surg 2006; 93: 1069-76
� Pearse R, Dawson D et al. Early goal-directed therapy after major surgery reduces complications and duration of hospital stay A randomised, controlled trial. Crit Care 2005; 9: R687-93
� Pearse RM, Harrison DA et al. Effet of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: a randomized linical trial and systematic review. JAMA 2014; 311: 2181-90
� Wakeling HG, McFall MR et al. Introperative oesophageal Doppler guided fluid mamagement shortens postoperative hospital stay after major bowel surgery. Br J Anaesth 2005; 95: 634-42
� Wind J, Polle SW, et al. Systemic review of enhanced recovery programmes in colonic surgery. Br J Surg 2006; 93: 800