Embed Size (px)
Citation preview
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
1st Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patients
1st Form Diagnosis of the disease
CENTER Name __________________________________________________
Address __________________________________________________
Country __________________________________________________
Phone number __________________________________________________
Fax number __________________________________________________
Referant doctor __________________________________________________
Email __________________________________________________ Comments
IDENTIFICATION ID Patient Surname (Family name)
Name (First name) |__|__|
|__| Date of birth mm/yyyy |__|__| / |__|__|__|__|
Sex 1 Male 2 Female
Country _________________________ Comments
1st Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
DEMOGRAPHIC DATA AT DIAGNOSIS
Marital status
1 Married 2 Never been married 3 Divorced 4 Widowed
Highest graduation basic
1 Secondary school 2 Intermediate school 3 High graduation school, A level 4 University
Employment status
1 Unemployed 2 Full time employed 3 Part time employed 4 Not applicable
Weight kg |__|__|__|
Height cm |__|__|__| 0 No 1 Yes 1 < 20 2 > 20
Currently smoker (if yes, specify number of daily cigarettes smoked and for how long) Number of years |__|__|
0 No 1 Yes Number of years |__|__|
Past smoker (if yes, specify number of years and date of stop smoking) Date of stop smoking
(dd mm yyyy) |__|__| |__|__| |__|__|__|__|
0 No 1 Yes 2 Not applicable Name (use trade name if possible) _________________________
Dose _________________________
Oral contraception (if yes, then, please specify name, dose and for how long)
Number of years |__|__| 0 No 1 Yes Pregnancy at diagnosis If yes then please specify number of weeks |__|__|
Comments

1st Form, Page 3 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
DISEASE CHARACTERISTICS AT DIAGNOSIS
Date of diagnostic dd mm yyyy |__|__| |__|__| |__|__|__|__|
WHO Performance
0 0 – Fully active 1 1 – Restricted in physically strenuous activity but ambulatory
and able to carry out work of a light or sedentary nature 2 2 – Ambulatory and capable of all selfcare but unable to carry
out work activities 3 3 – Capable of only limited selfcare, confined to bed or chair
more than 50 % of waking hours 4 4 – Completely disabled, cannot carry on any selfcare 5 5 – Dead
Disease related symptom 0 No 1 Yes 0 No 1 Yes
Extramedullary manifestations (apart from liver and spleen) If yes, please specify _________________________
cm below costal margin palpated |__|__|
Spleen size Longest diameter in ultrasound, cm |__|__|
cm below medium clavicular line |__|__|
Liver size Longest diameter in ultrasound, cm |__|__|
Sokal score (Before any treatment)
1 Low 2 Intermediate 3 High
Hasford score (Before any treatment)
1 Low 2 Intermediate 3 High
Comments

1st Form, Page 4 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
HEMATOLOGY AT DIAGNOSIS
PERIPHERAL BLOOD AT DIAGNOSIS
Peripheral blood analysis 0 No 1 Yes
If no, please specify the reason _________________________
If yes, please specify below: Date of peripheral blood analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Hemoglobin g/dl |__|__| , |__|
Hematocrit % |__|__| , |__|
Erythrocyte 1012/l |__| , |__|__|
Reticulocyte % |__|__| , |__|
Platelets 109/l |__|__|__|__|
Leukocyte 109/l |__|__|__| , |__|
Neutrophils % |__|__|
Eosinophils % |__|__|
Basophils % |__|__|
Monocytes % |__|__|
Lymphocytes % |__|__|
Myelaemia % |__|__|
Myeloblasts % |__|__|
Promyelocytes % |__|__|
Myelocytes % |__|__|
Metamyelocytes % |__|__|
Blasts % |__|__|
Erythroblasts % |__|__|
Others _________________________ Comments
1st Form, Page 5 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
BONE MARROW AT DIAGNOSIS
Bone marrow analysis 0 No 1 Yes 2 Not applicable
If not applicable or not done, please specify the reason ______________________
If yes, please specify below:
Date of bone marrow analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Cellularity 1 Low 2 Normal 3 High
Megakaryocyte 1 Low 2 Normal 3 High
Blasts % |__|__|
Myeloblasts % |__|__|
Promyelocytes % |__|__|
Myelocytes % |__|__|
Metamyelocytes % |__|__|
Neutrophils % |__|__|
Eosinophils % |__|__|
Basophils % |__|__|
Monocytes % |__|__|
Lymphocytes % |__|__|
Erythroblasts % |__|__|
Plasmocyts % |__|__| Comments
1st Form, Page 6 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
OSTEOMEDULLARY BIOPSY AT DIAGNOSIS
Osteomedullary biopsy 0 No 1 Yes
If yes, please specify
Date dd mm yyyy |__|__| |__|__| |__|__|__|__|
Fibrosis 0 No 1 Yes
Adipocytes 1 Normal 2 Decreased
Granulopoesis 1 Increased 2 Normal
Erythropoesis 1 Increased 2 Normal 3 Decreased
Megakaryocyte 1 Increased 2 Normal 3 Decreased
Result ______________________________________________________ Comments
1st Form, Page 7 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
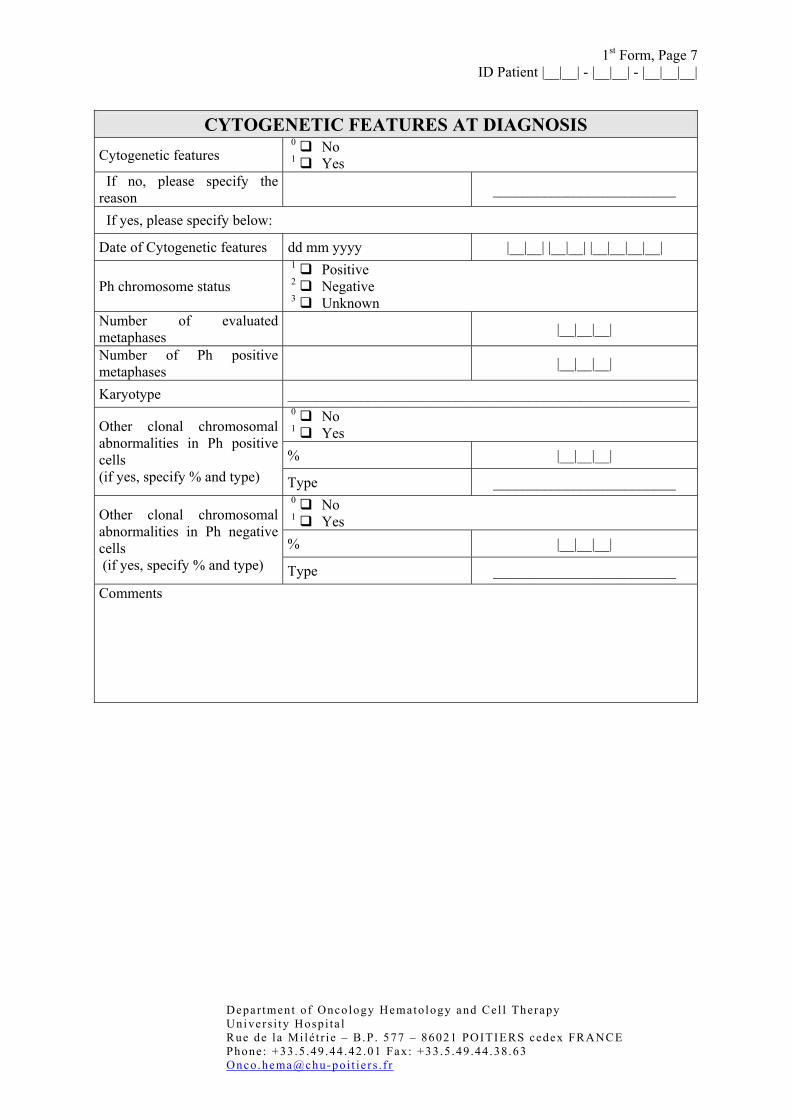
CYTOGENETIC FEATURES AT DIAGNOSIS
Cytogenetic features 0 No 1 Yes
If no, please specify the reason _________________________
If yes, please specify below:
Date of Cytogenetic features dd mm yyyy |__|__| |__|__| |__|__|__|__|
Ph chromosome status 1 Positive 2 Negative 3 Unknown
Number of evaluated metaphases |__|__|__|
Number of Ph positive metaphases |__|__|__|
Karyotype _______________________________________________________ 0 No 1 Yes % |__|__|__|
Other clonal chromosomal abnormalities in Ph positive cells (if yes, specify % and type) Type _________________________
0 No 1 Yes % |__|__|__|
Other clonal chromosomal abnormalities in Ph negative cells (if yes, specify % and type) Type _________________________ Comments

1st Form, Page 8 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
F.I.S.H AT DIAGNOSIS
FISH analysis 0 No 1 Yes
If no,
Technique failure 0 No 1 Yes
If yes
Date of F.I.S.H dd mm yyyy |__|__| |__|__| |__|__|__|__|
Number of evaluated nuclei |__|__|__| Number of BCR/ABL + nuclei |__|__|__|
Number of BCR/ABL + mitosis |__|__|__|
Deletion of genetic material on chromosome 9q+ (FISH)
0 No 1 Yes
Result ______________________________________________________ Comments

1st Form, Page 9 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
MOLECULAR BIOLOGY AT DIAGNOSIS
Molecular biology analysis 0 No 1 Yes
If no, please specify the reason
_________________________
If yes, please specify below:
Date of analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Source of material 1 Peripheral blood 2 Bone marrow
Volume ml |__|__|__|
BCR-ABL transcript 1 Positive 2 Negative 3 Unknown
Ratio BCR-ABL/ABL % |__|__|__| , |__|__|__|
Other control gene Please specify _________________________
Ratio BCR-ABL/other gene % |__|__|__| , |__|__|__|
Nested PCR 1 Positive 2 Negative 3 Not done
Level BCR-ABL transcript _________________________ 1 b2a2 2 b3a2 3 b2a3 4 b3a3 5 e1a2 6 b2a2 and b3a2 7 e6a2 8 e19a2 9 Others
Transcript
If others, please specify _________________________
HLA status
1 A 2 B 3 C 4 DR 5 DQ
Comments
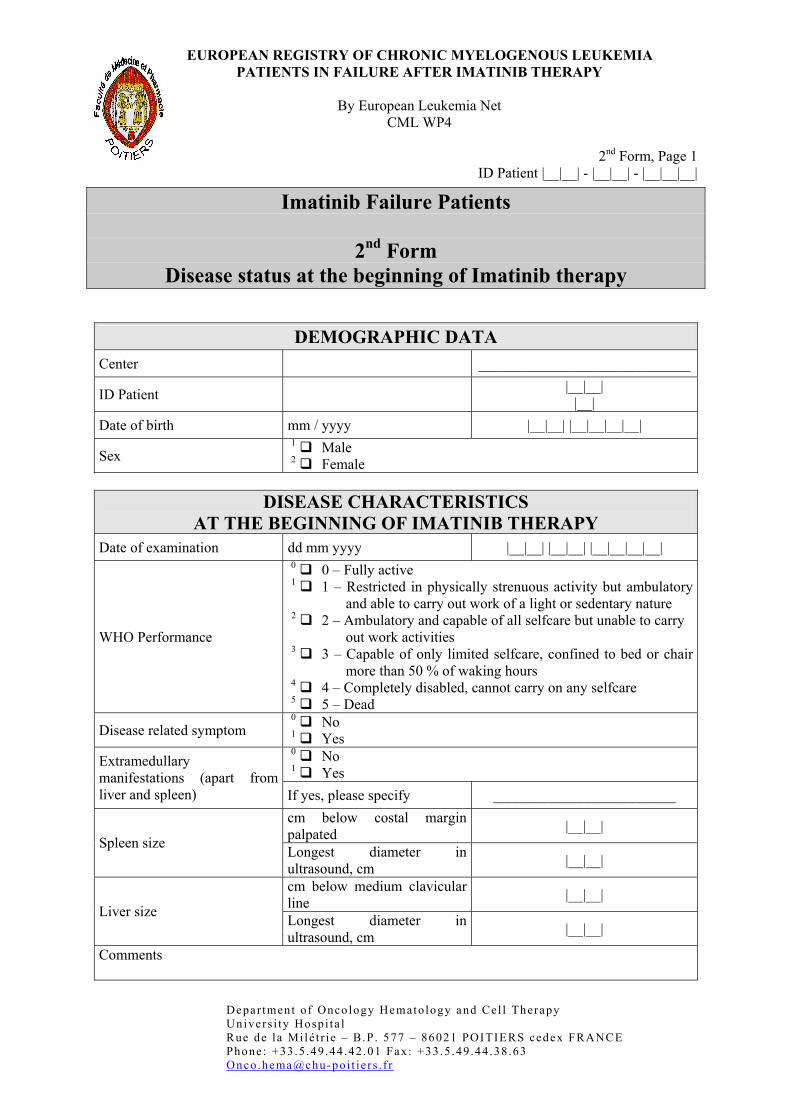
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
2nd Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patients
2nd Form Disease status at the beginning of Imatinib therapy
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
DISEASE CHARACTERISTICS
AT THE BEGINNING OF IMATINIB THERAPY Date of examination dd mm yyyy |__|__| |__|__| |__|__|__|__|
WHO Performance
0 0 – Fully active 1 1 – Restricted in physically strenuous activity but ambulatory
and able to carry out work of a light or sedentary nature 2 2 – Ambulatory and capable of all selfcare but unable to carry
out work activities 3 3 – Capable of only limited selfcare, confined to bed or chair
more than 50 % of waking hours 4 4 – Completely disabled, cannot carry on any selfcare 5 5 – Dead
Disease related symptom 0 No 1 Yes 0 No 1 Yes
Extramedullary manifestations (apart from liver and spleen) If yes, please specify _________________________
cm below costal margin palpated |__|__|
Spleen size Longest diameter in ultrasound, cm |__|__|
cm below medium clavicular line |__|__|
Liver size Longest diameter in ultrasound, cm |__|__|
Comments
2nd Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
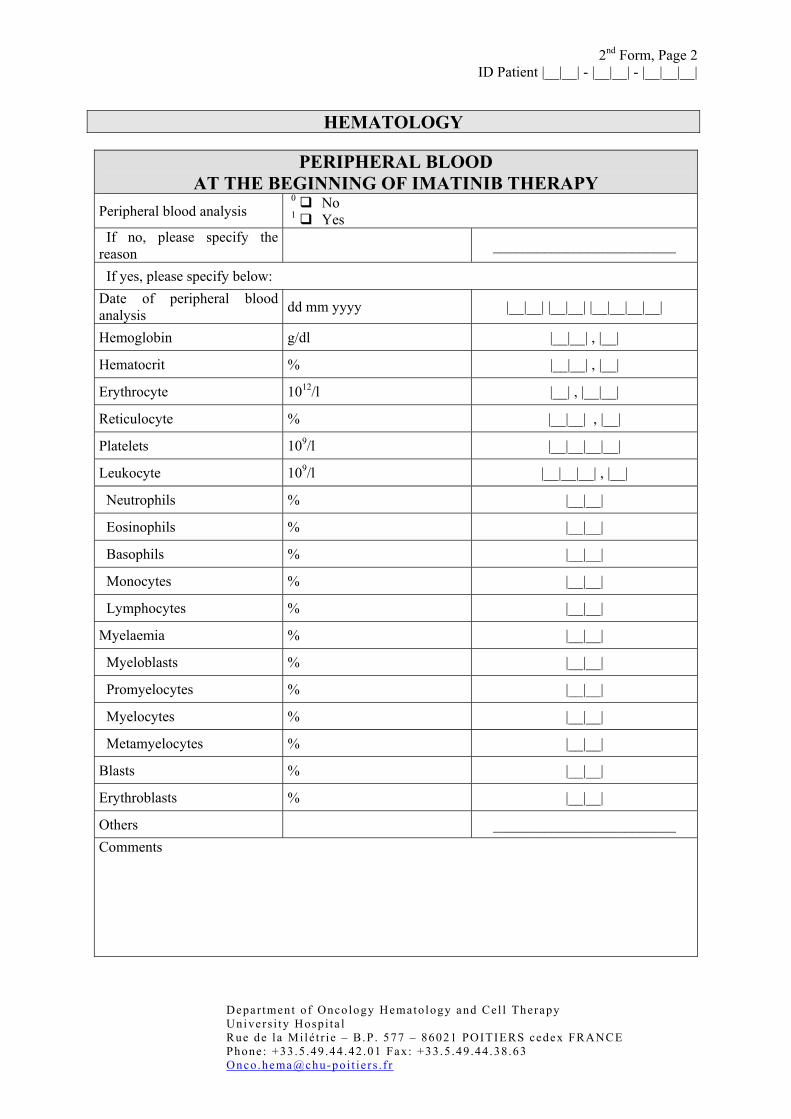
HEMATOLOGY
PERIPHERAL BLOOD
AT THE BEGINNING OF IMATINIB THERAPY Peripheral blood analysis 0 No
1 Yes If no, please specify the reason _________________________
If yes, please specify below: Date of peripheral blood analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Hemoglobin g/dl |__|__| , |__|
Hematocrit % |__|__| , |__|
Erythrocyte 1012/l |__| , |__|__|
Reticulocyte % |__|__| , |__|
Platelets 109/l |__|__|__|__|
Leukocyte 109/l |__|__|__| , |__|
Neutrophils % |__|__|
Eosinophils % |__|__|
Basophils % |__|__|
Monocytes % |__|__|
Lymphocytes % |__|__|
Myelaemia % |__|__|
Myeloblasts % |__|__|
Promyelocytes % |__|__|
Myelocytes % |__|__|
Metamyelocytes % |__|__|
Blasts % |__|__|
Erythroblasts % |__|__|
Others _________________________ Comments
2nd Form, Page 3 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
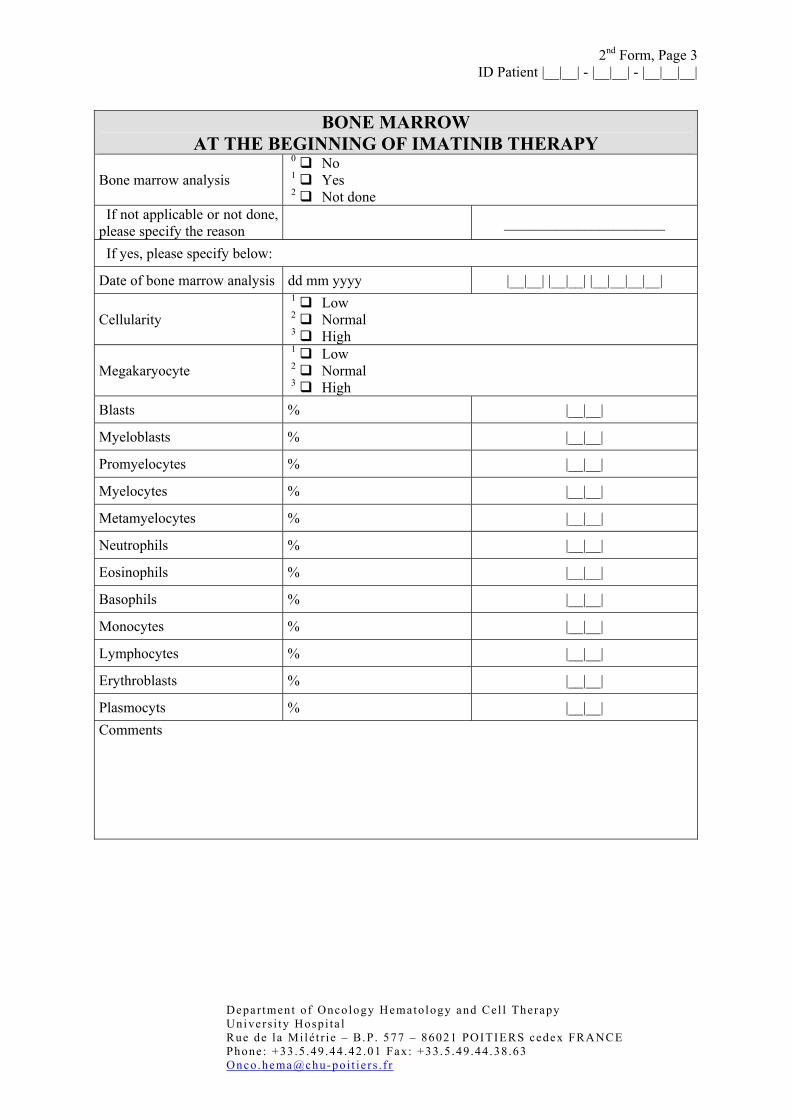
BONE MARROW
AT THE BEGINNING OF IMATINIB THERAPY
Bone marrow analysis 0 No 1 Yes 2 Not done
If not applicable or not done, please specify the reason ______________________
If yes, please specify below:
Date of bone marrow analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Cellularity 1 Low 2 Normal 3 High
Megakaryocyte 1 Low 2 Normal 3 High
Blasts % |__|__|
Myeloblasts % |__|__|
Promyelocytes % |__|__|
Myelocytes % |__|__|
Metamyelocytes % |__|__|
Neutrophils % |__|__|
Eosinophils % |__|__|
Basophils % |__|__|
Monocytes % |__|__|
Lymphocytes % |__|__|
Erythroblasts % |__|__|
Plasmocyts % |__|__| Comments
2nd Form, Page 4 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
OSTEOMEDULLARY BIOPSY
AT THE BEGINNING OF IMATINIB THERAPY Osteomedullary biopsy 0 No
1 Yes If yes, please specify
Date dd mm yyyy |__|__| |__|__| |__|__|__|__|
Fibrosis 0 No 1 Yes
Adipocytes 1 Normal 2 Decreased
Granulopoesis 1 Increased 2 Normal
Erythropoesis 1 Increased 2 Normal 3 Decreased
Megakaryocyte 1 Increased 2 Normal 3 Decreased
Result ______________________________________________________ Comments
2nd Form, Page 5 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
CYTOGENETIC FEATURES
AT THE BEGINNING OF IMATINIB THERAPY Cytogenetic features 0 No
1 Yes If no, please specify the reason _________________________
If yes, please specify below:
Date of Cytogenetic features dd mm yyyy |__|__| |__|__| |__|__|__|__|
Ph chromosome status 1 Positive 2 Negative 3 Unknown
Number of evaluated metaphases |__|__|__|
Number of Ph positive metaphases |__|__|__|
Karyotype _______________________________________________________ 0 No 1 Yes % |__|__|__|
Other clonal chromosomal abnormalities in Ph positive cells (if yes, specify % and type) Type _________________________
0 No 1 Yes % |__|__|__|
Other clonal chromosomal abnormalities in Ph negative cells (if yes, specify % and type) Type _________________________ Comments
2nd Form, Page 6 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
F.I.S.H
AT THE BEGINNING OF IMATINIB THERAPY FISH analysis 0 No
1 Yes If no
Technique failure 0 No 1 Yes
If yes
Date of F.I.S.H dd mm yyyy |__|__| |__|__| |__|__|__|__|
Number of evaluated nucleus |__|__|__| Number of BCR/ABL + nucleus |__|__|__|
Number of BCR/ABL + mitosis |__|__|__|
Deletion of genetic material on chromosome 9q+ (FISH)
0 No 1 Yes
Result ______________________________________________________ Comments
2nd Form, Page 7 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
MOLECULAR BIOLOGY
AT THE BEGINNING OF IMATINIB THERAPY Molecular biology analysis 0 No
1 Yes If no, please specify the reason
_________________________
If yes, please specify below:
Date of analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Source of material 1 Peripheral blood 2 Bone marrow
Volume ml |__|__|__|
BCR-ABL transcript 1 Positive 2 Negative 3 Unknown
Ratio BCR-ABL/ABL % |__|__|__| , |__|__|__|
Other control gene Please specify _________________________
Ratio BCR-ABL/other gene % |__|__|__| , |__|__|__|
Nested PCR 1 Positive 2 Negative 3 Not done
Level BCR-ABL transcript _________________________ 1 b2a2 2 b3a2 3 b2a3 4 b3a3 5 e1a2 6 b2a2 and b3a2 7 e6a2 8 e19a2 9 Others
Transcript
If others, please specify _________________________
HLA status
1 A 2 B 3 C 4 DR 5 DQ
Comments
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
3rd Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
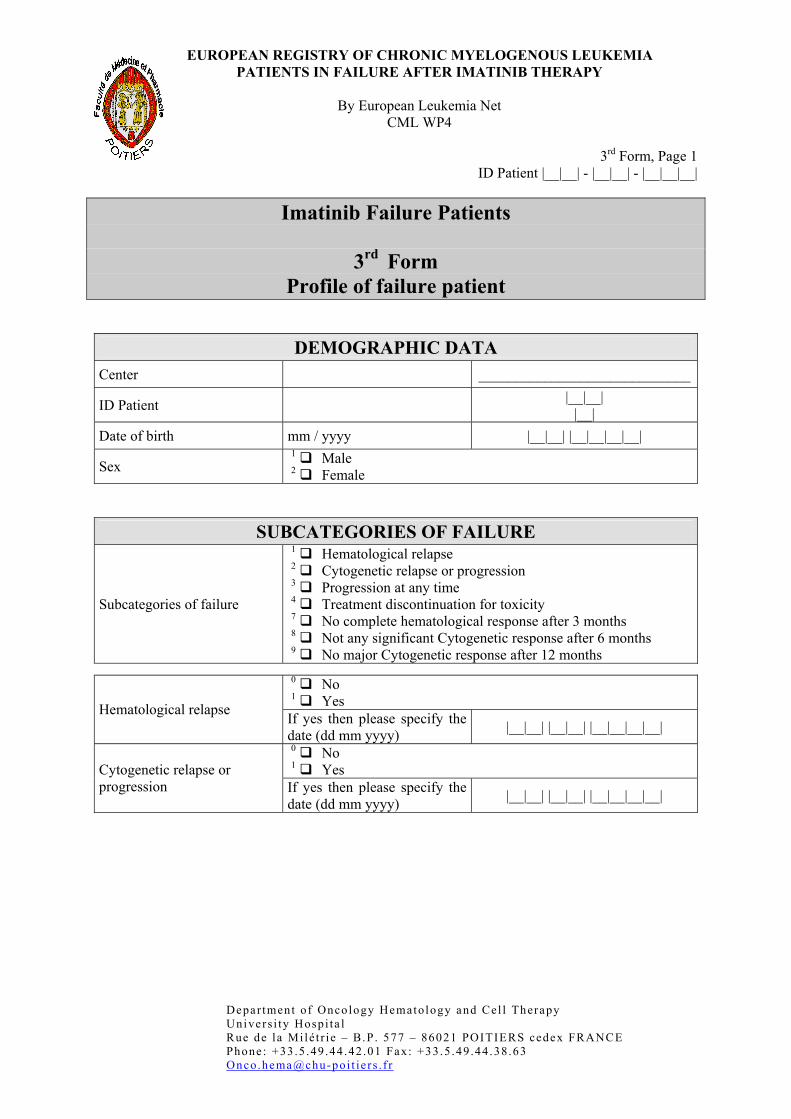
Imatinib Failure Patients
3rd Form Profile of failure patient
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
SUBCATEGORIES OF FAILURE
Subcategories of failure
1 Hematological relapse 2 Cytogenetic relapse or progression 3 Progression at any time 4 Treatment discontinuation for toxicity 7 No complete hematological response after 3 months 8 Not any significant Cytogenetic response after 6 months 9 No major Cytogenetic response after 12 months
0 No 1 Yes Hematological relapse If yes then please specify the date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
0 No 1 Yes Cytogenetic relapse or
progression If yes then please specify the date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
3rd Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
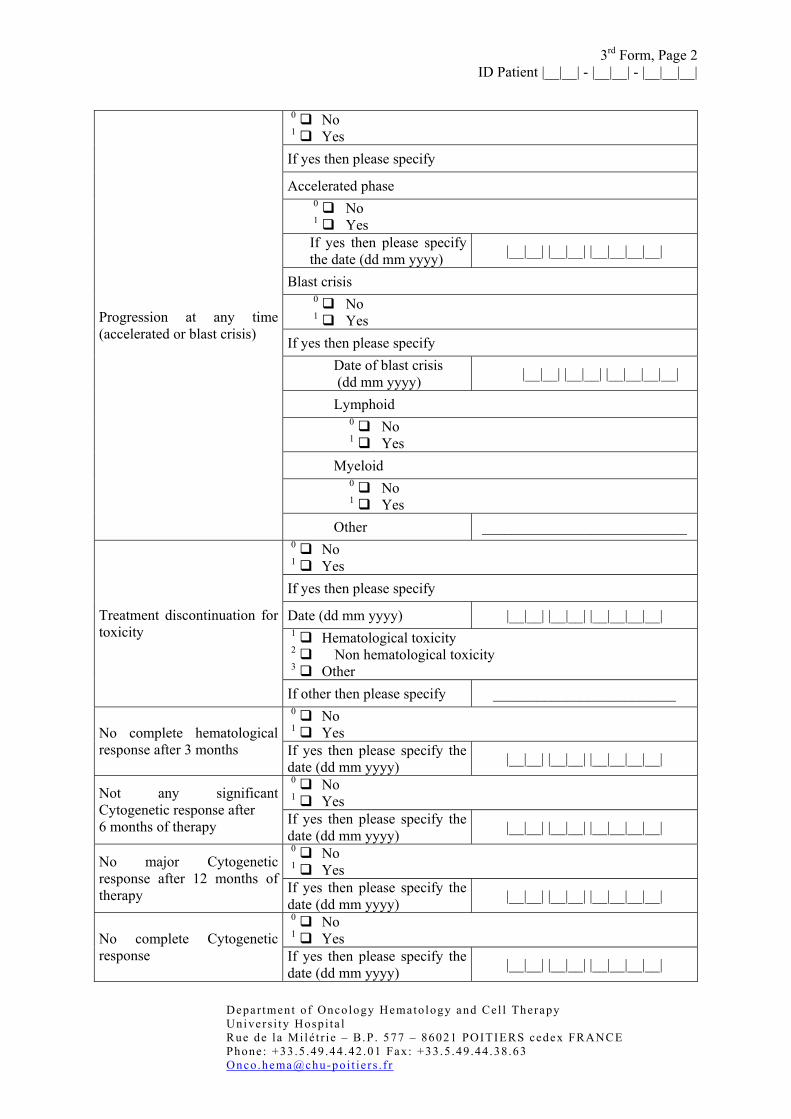
0 No 1 Yes If yes then please specify
Accelerated phase 0 No 1 Yes If yes then please specify the date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
Blast crisis 0 No 1 Yes
If yes then please specify Date of blast crisis (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
Lymphoid 0 No 1 Yes
Myeloid 0 No 1 Yes
Progression at any time (accelerated or blast crisis)
Other ____________________________ 0 No 1 Yes If yes then please specify
Date (dd mm yyyy) |__|__| |__|__| |__|__|__|__| 1 Hematological toxicity 2 Non hematological toxicity 3 Other
Treatment discontinuation for toxicity
If other then please specify _________________________ 0 No 1 Yes No complete hematological
response after 3 months If yes then please specify the date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
0 No 1 Yes Not any significant
Cytogenetic response after 6 months of therapy If yes then please specify the
date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
0 No 1 Yes No major Cytogenetic
response after 12 months of therapy If yes then please specify the
date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
0 No 1 Yes No complete Cytogenetic
response If yes then please specify the date (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
3rd Form, Page 3 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
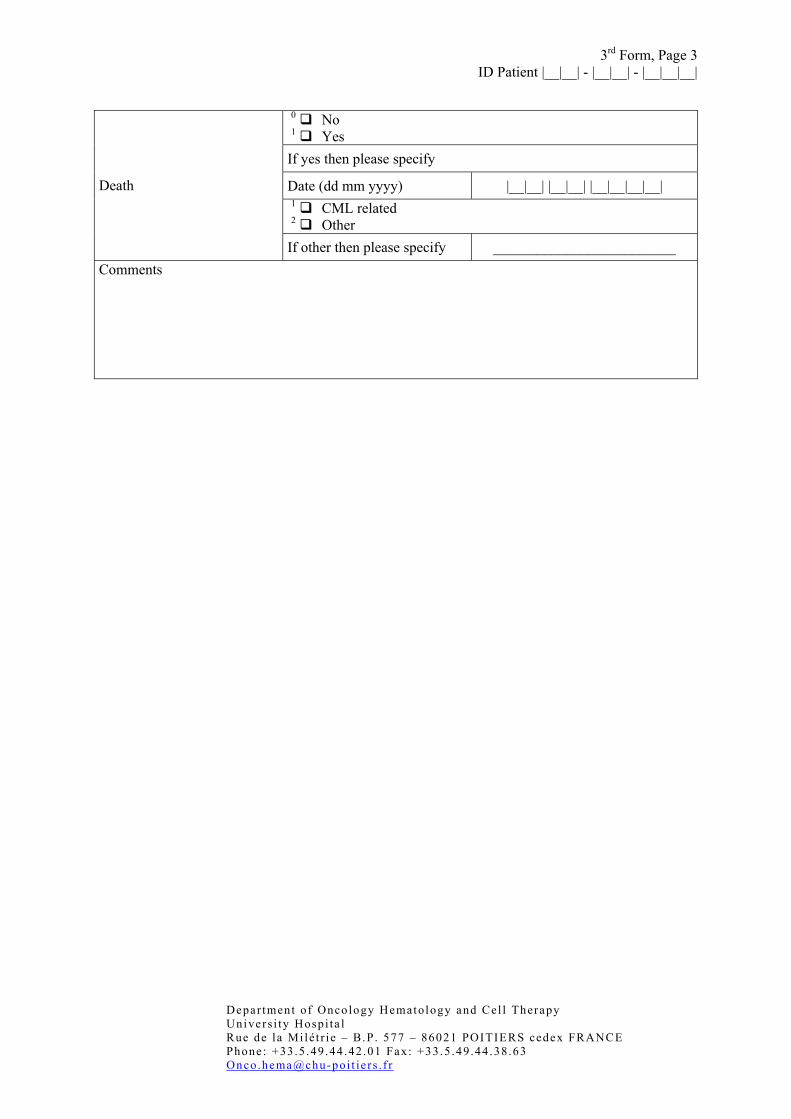
0 No 1 Yes If yes then please specify
Date (dd mm yyyy) |__|__| |__|__| |__|__|__|__| 1 CML related 2 Other
Death
If other then please specify _________________________ Comments
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
4th Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
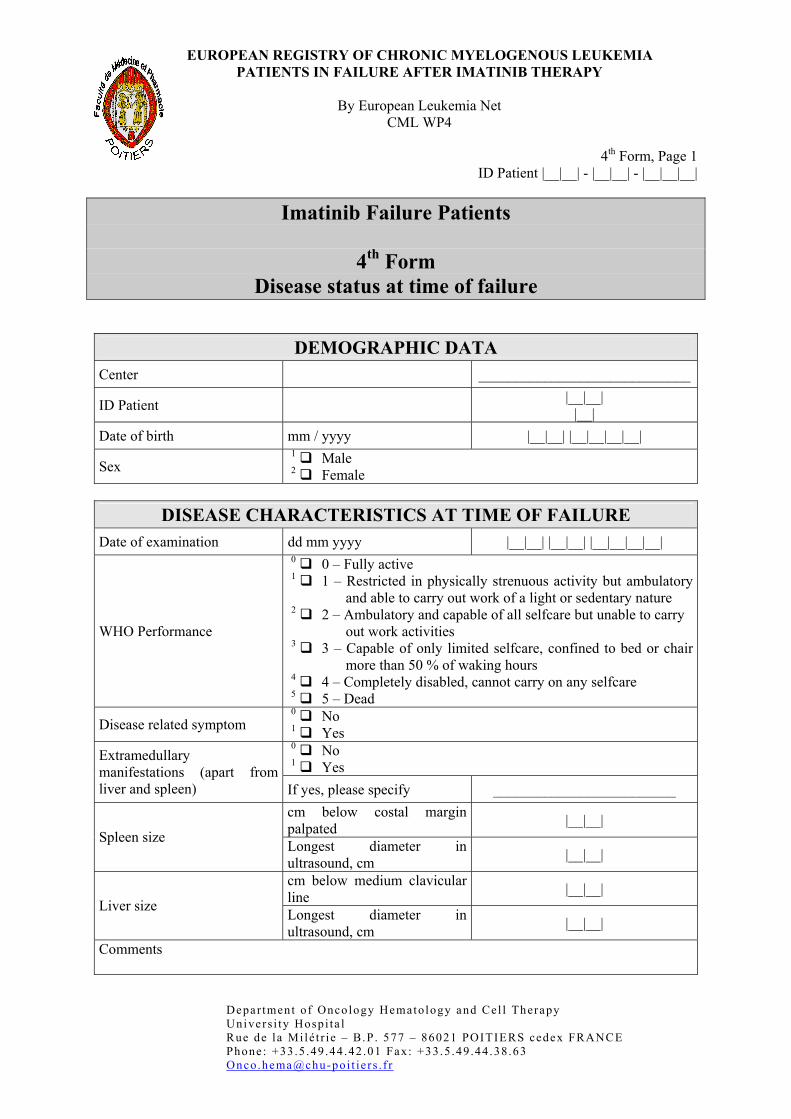
Imatinib Failure Patients
4th Form Disease status at time of failure
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
DISEASE CHARACTERISTICS AT TIME OF FAILURE
Date of examination dd mm yyyy |__|__| |__|__| |__|__|__|__|
WHO Performance
0 0 – Fully active 1 1 – Restricted in physically strenuous activity but ambulatory
and able to carry out work of a light or sedentary nature 2 2 – Ambulatory and capable of all selfcare but unable to carry
out work activities 3 3 – Capable of only limited selfcare, confined to bed or chair
more than 50 % of waking hours 4 4 – Completely disabled, cannot carry on any selfcare 5 5 – Dead
Disease related symptom 0 No 1 Yes 0 No 1 Yes
Extramedullary manifestations (apart from liver and spleen) If yes, please specify _________________________
cm below costal margin palpated |__|__|
Spleen size Longest diameter in ultrasound, cm |__|__|
cm below medium clavicular line |__|__|
Liver size Longest diameter in ultrasound, cm |__|__|
Comments
4th Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
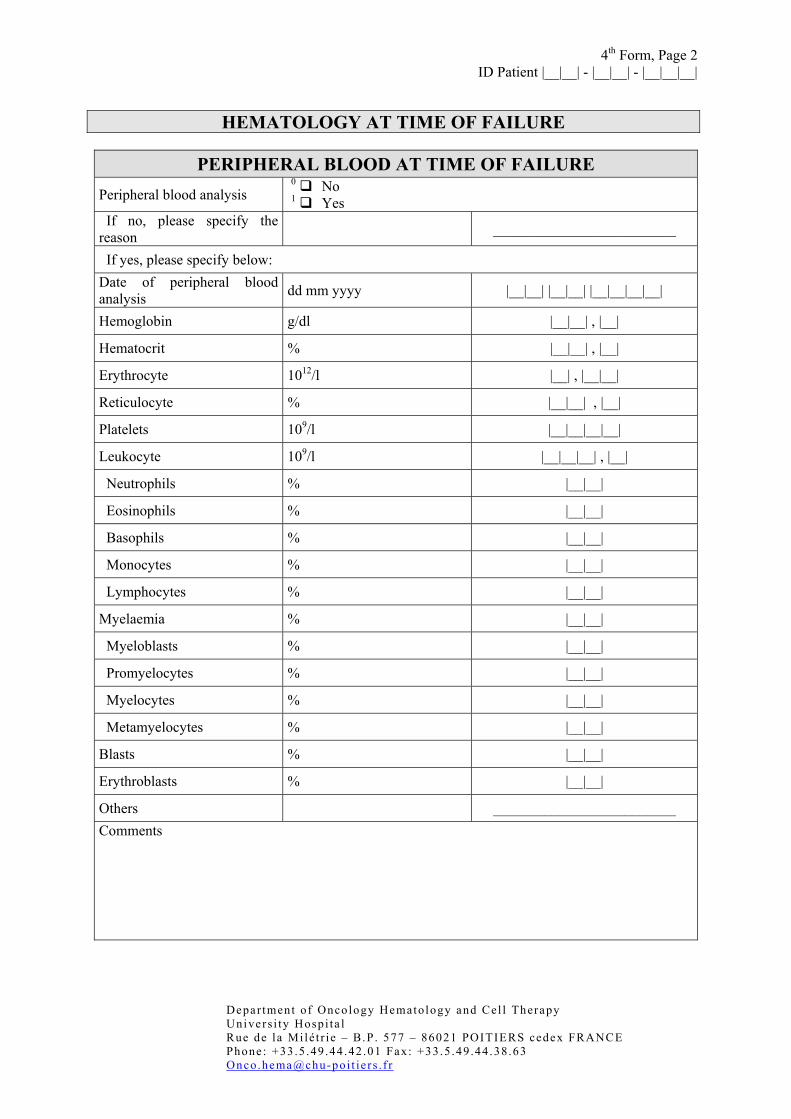
HEMATOLOGY AT TIME OF FAILURE
PERIPHERAL BLOOD AT TIME OF FAILURE
Peripheral blood analysis 0 No 1 Yes
If no, please specify the reason _________________________
If yes, please specify below: Date of peripheral blood analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Hemoglobin g/dl |__|__| , |__|
Hematocrit % |__|__| , |__|
Erythrocyte 1012/l |__| , |__|__|
Reticulocyte % |__|__| , |__|
Platelets 109/l |__|__|__|__|
Leukocyte 109/l |__|__|__| , |__|
Neutrophils % |__|__|
Eosinophils % |__|__|
Basophils % |__|__|
Monocytes % |__|__|
Lymphocytes % |__|__|
Myelaemia % |__|__|
Myeloblasts % |__|__|
Promyelocytes % |__|__|
Myelocytes % |__|__|
Metamyelocytes % |__|__|
Blasts % |__|__|
Erythroblasts % |__|__|
Others _________________________ Comments
4th Form, Page 3 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
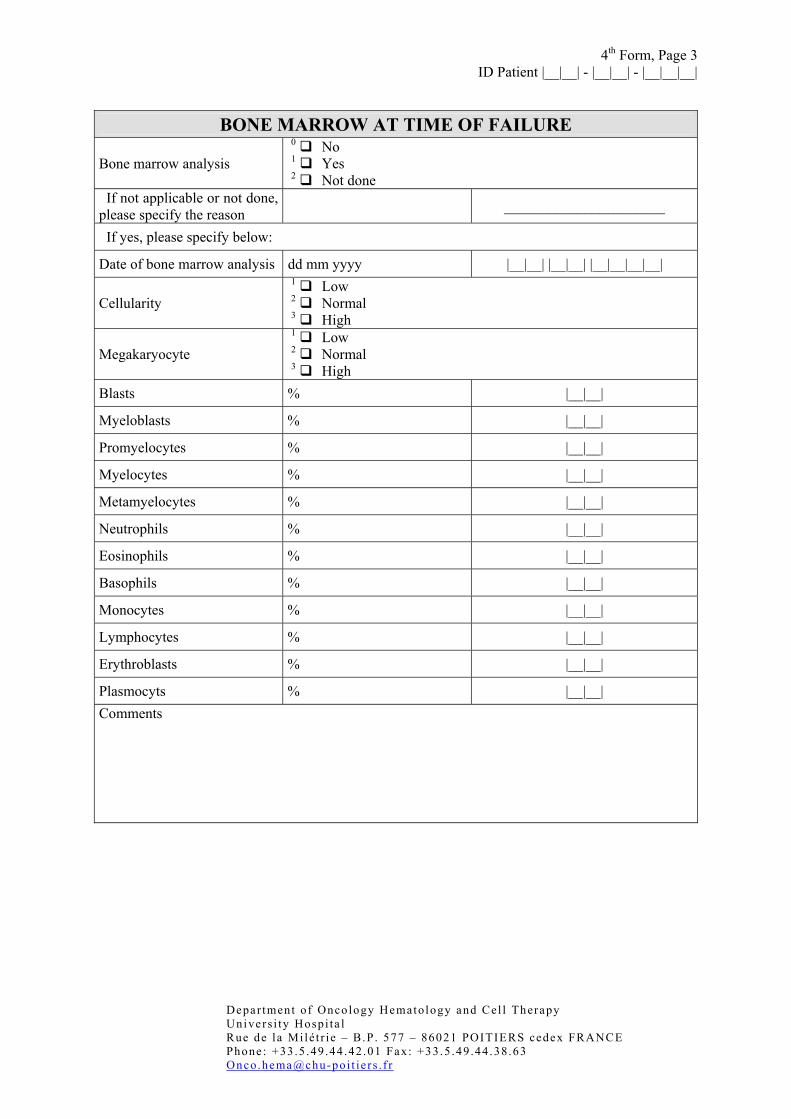
BONE MARROW AT TIME OF FAILURE
Bone marrow analysis 0 No 1 Yes 2 Not done
If not applicable or not done, please specify the reason ______________________
If yes, please specify below:
Date of bone marrow analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Cellularity 1 Low 2 Normal 3 High
Megakaryocyte 1 Low 2 Normal 3 High
Blasts % |__|__|
Myeloblasts % |__|__|
Promyelocytes % |__|__|
Myelocytes % |__|__|
Metamyelocytes % |__|__|
Neutrophils % |__|__|
Eosinophils % |__|__|
Basophils % |__|__|
Monocytes % |__|__|
Lymphocytes % |__|__|
Erythroblasts % |__|__|
Plasmocyts % |__|__| Comments
4th Form, Page 4 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
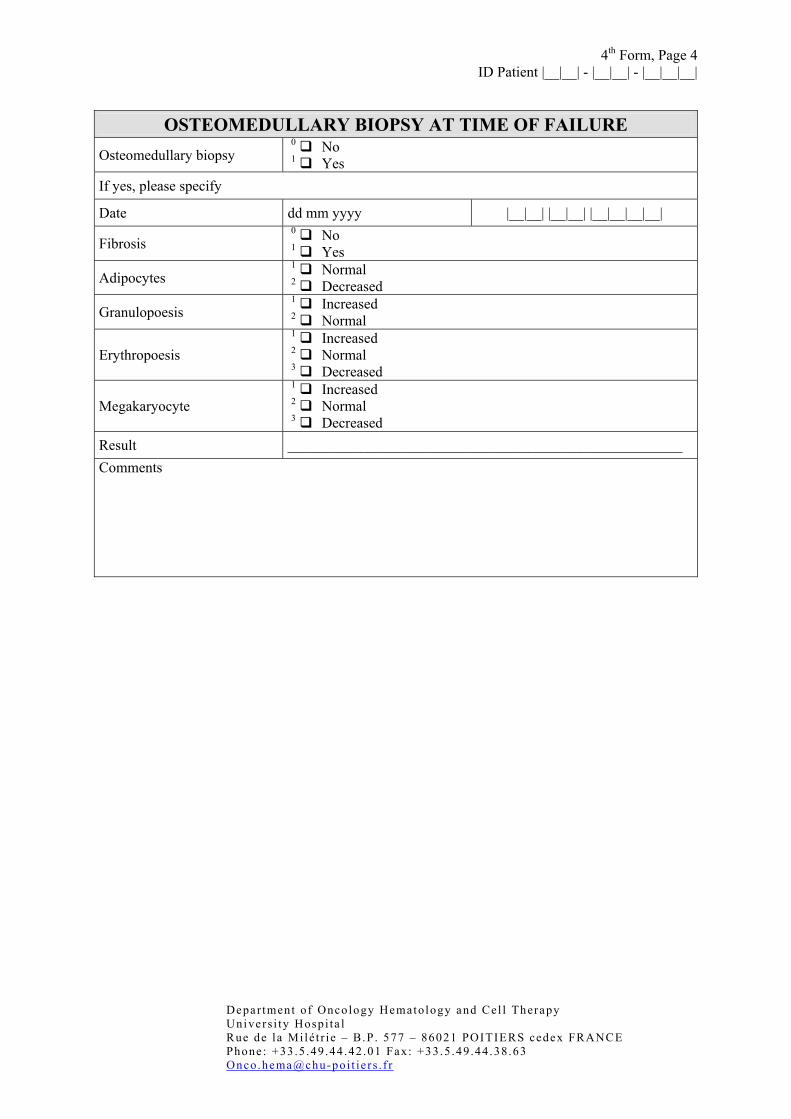
OSTEOMEDULLARY BIOPSY AT TIME OF FAILURE
Osteomedullary biopsy 0 No 1 Yes
If yes, please specify
Date dd mm yyyy |__|__| |__|__| |__|__|__|__|
Fibrosis 0 No 1 Yes
Adipocytes 1 Normal 2 Decreased
Granulopoesis 1 Increased 2 Normal
Erythropoesis 1 Increased 2 Normal 3 Decreased
Megakaryocyte 1 Increased 2 Normal 3 Decreased
Result ______________________________________________________ Comments
4th Form, Page 5 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
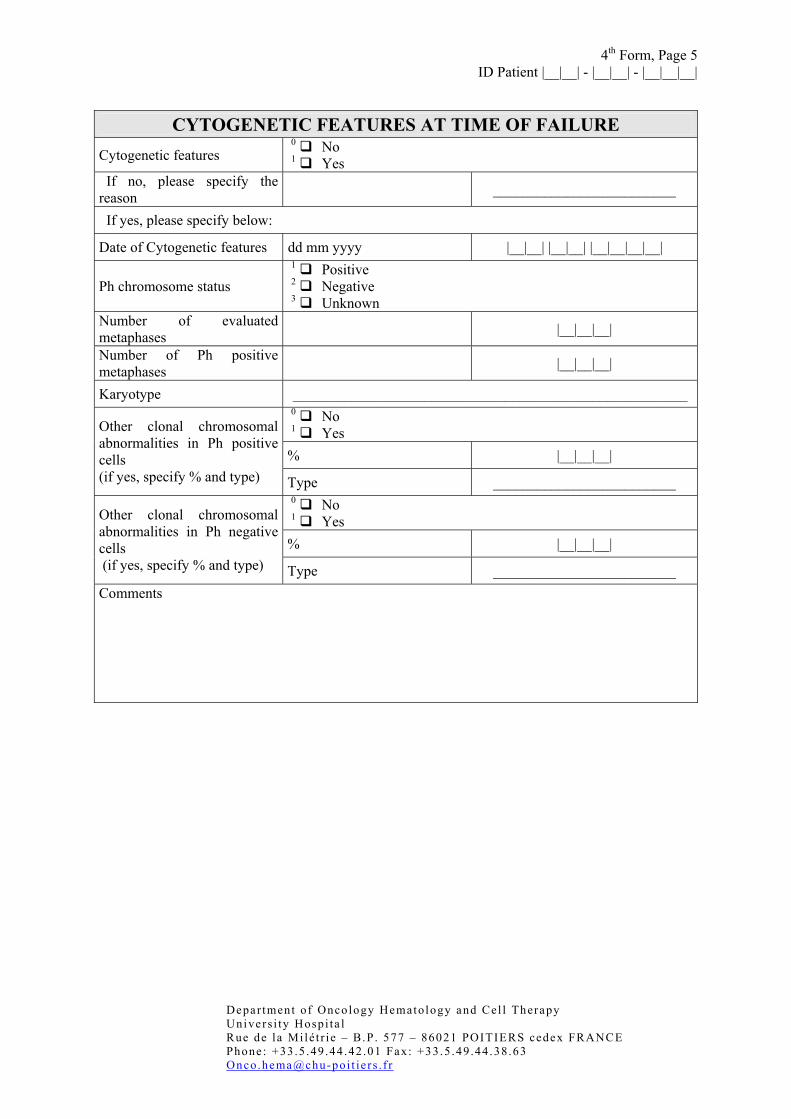
CYTOGENETIC FEATURES AT TIME OF FAILURE
Cytogenetic features 0 No 1 Yes
If no, please specify the reason _________________________
If yes, please specify below:
Date of Cytogenetic features dd mm yyyy |__|__| |__|__| |__|__|__|__|
Ph chromosome status 1 Positive 2 Negative 3 Unknown
Number of evaluated metaphases |__|__|__|
Number of Ph positive metaphases |__|__|__|
Karyotype ______________________________________________________ 0 No 1 Yes % |__|__|__|
Other clonal chromosomal abnormalities in Ph positive cells (if yes, specify % and type) Type _________________________
0 No 1 Yes % |__|__|__|
Other clonal chromosomal abnormalities in Ph negative cells (if yes, specify % and type) Type _________________________ Comments
4th Form, Page 6 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
F.I.S.H AT TIME OF FAILURE
FISH analysis 0 No 1 Yes
If no,
Technique failure 0 No 1 Yes
If yes
Date of F.I.S.H dd mm yyyy |__|__| |__|__| |__|__|__|__|
Number of evaluated nucleus |__|__|__| Number of BCR/ABL + nucleus |__|__|__|
Number of BCR/ABL + mitosis |__|__|__|
Deletion of genetic material on chromosome 9q+ (FISH)
0 No 1 Yes
Result ______________________________________________________ Comments

4th Form, Page 7 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
MOLECULAR BIOLOGY AT TIME OF FAILURE
Molecular biology analysis 0 No 1 Yes
If no, please specify the reason
_________________________
If yes, please specify below :
Date of analysis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Source of material 1 Peripheral blood 2 Bone marrow
Volume ml |__|__|__|
BCR-ABL transcript 1 Positive 2 Negative 3 Not done
Ratio BCR-ABL/ABL % |__|__|__| , |__|__|__|
Other control gene Please specify _________________________
Ratio BCR-ABL/other gene % |__|__|__| , |__|__|__|
Nested PCR 1 Positive 2 Negative 3 Not done
Level BCR-ABL transcript _________________________ 1 b2a2 2 b3a2 3 b2a3 4 b3a3 5 e1a2 6 b2a2 and b3a2 7 e6a2 8 e19a2 9 Others
Transcript
If others, please specify _________________________
HLA status
1 A 2 B 3 C 4 DR 5 DQ
Comments
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
5th Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patient
5th Form (a) Imatinib therapy
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
IMATINIB THERAPY Start of Imatinib dd mm yyyy |__|__| |__|__| |__|__|__|__|
1 400mg/day 2 600mg/day 3 800mg/day 4 Other
Administrated dose at the beginning of treatment
If other then please specify _________________________ 0 No 1 Yes Clinical trial If yes, please specify _________________________
Modification(s) of dose 0 No 1 Yes 1 Adverse event 2 Inefficacy 3 Dose error 4 Protocol 5 Other
Reason for modification(s)
If other, please specify _________________________ 1 400mg/day 2 600mg/day 3 800mg/day 4 Other or successive doses
New administrated dose(s)
If other, please specify _________________________
5th Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Period of modification
First occurrence dd mm yyyy |__|__| |__|__| |__|__|__|__|
Last occurrence dd mm yyyy |__|__| |__|__| |__|__|__|__|
Combination with other treatment
0 No 1 Yes
If yes, please specify 0 No 1 Yes If yes, please specify
Dose ____________________________
Period
From |__|__| |__|__| |__|__|__|__|
Cytarabine
To |__|__| |__|__| |__|__|__|__| 0 No 1 Yes If yes, please specify
Dose ____________________________
Period
From |__|__| |__|__| |__|__|__|__|
Interferon
To |__|__| |__|__| |__|__|__|__| 0 No 1 Yes Other If yes, please specify ____________________________
Comments
5th Form, Page 3 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
CONCOMITANT TREATMENT
Concomitant treatment 0 No 1 Yes
1 Corticoids 2 Other
Name of molecule which can explain resistance or intolerance If other then please specify _________________________
From (dd mm yyyy) |__|__| |__|__| |__|__|__|__| Period or date of concomitant treatment To (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
1 Corticoids 2 Other
Name of molecule which can explain resistance or intolerance If other then please specify _________________________
From (dd mm yyyy) |__|__| |__|__| |__|__|__|__| Period or date of concomitant treatment To (dd mm yyyy) |__|__| |__|__| |__|__|__|__|
Comments
5th Form, Page 4 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
RESPONSE WITH IMATINIB
HEMATOLOGICAL RESPONSE
Chronic phase 0 No 1 Yes
Subsequent phase 0 No 1 Yes 0 No 1 Yes Complete hematological
response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
CYTOGENETIC RESPONSE
0 No 1 Yes
Any significant response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
0 No 1 Yes
Major Cytogenetic response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
0 No 1 Yes Complete Cytogenetic
response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
MOLECULAR RESPONSE
Date (dd mm yyyy) |__|__| |__|__| |__|__|__|__| Best response
Specify _____________________________ Comments
5th Form, Page 5 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patient
5th Form (b) Imatinib therapy at failure
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
IMATINIB THERAPY AT FAILURE 0 No 1 Yes If yes, please specify
Date (dd mm yyyy) |__|__| |__|__| |__|__|__|__| Discontinuation
Dose
1 400mg/day 2 600mg/day 3 800mg/day 4 Other
0 No 1 Yes If yes, please specify
Current dose at failure
1 400mg/day 2 600mg/day 3 800mg/day 4 Other
No discontinuation
Schedule dose after failure
1 400mg/day 2 600mg/day 3 800mg/day 4 Other
Comments

5th Form, Page 6 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patient
5th Form (c) Treatment before Imatinib therapy
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
TREATMENT BEFORE IMATINIB THERAPY Treatment before Imatinib therapy
0 No 1 Yes
If yes, please specify below:
Drug: _________________________
Dose: _________________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug: ______________________
Dose: ______________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug : ______________________
Dose: ______________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
5th Form, Page 7 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Drug: ______________________
Dose: ______________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Comments
5th Form, Page 8 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
RESPONSE WITH PRE-TREATMENT
HEMATOLOGICAL RESPONSE
Chronic phase 0 No 1 Yes
Subsequent phase 0 No 1 Yes 0 No 1 Yes Complete hematological
response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
CYTOGENETIC RESPONSE 0 No 1 Yes
Any significant response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
0 No 1 Yes
Major Cytogenetic response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
0 No 1 Yes Complete Cytogenetic
response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
MOLECULAR RESPONSE
Date (dd mm yyyy) |__|__| |__|__| |__|__|__|__| Best response
Specify _____________________________ Comments
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
6th Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patient
6th Form Adverse events
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
ADVERSE EVENTS Adverse effects 0 No
1 Yes
Effects / symptom _________________________
During the treatment 0 No 1 Yes
Date dd mm yyyy |__|__| |__|__| |__|__|__|__|
Intensity (grade)
1 1 2 2 3 3 4 4 11 Low 12 Moderate 13 High
In relation with the therapy 0 No 1 Yes 2 Not applicable
Follow-up
1 Recovery 2 No complete recovery 3 Sequelae 4 Death 5 Other
Gravity 0 No 1 Yes
Frequency _________________________
6th Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
1 Any 2 Medical treatment 3 Hospitalization 4 Other
Action
If other then please specify _________________________
Effects / symptom _________________________
During the treatment 0 No 1 Yes
Date dd mm yyyy |__|__| |__|__| |__|__|__|__|
Intensity (grade)
1 1 2 2 3 3 4 4 11 Low 12 Moderate 13 High
In relation with the therapy 0 No 1 Yes 2 Not applicable
Follow-up
1 Recovery 2 No complete recovery 3 Sequelae 4 Death 5 Other
Gravity 0 No 1 Yes
Frequency _________________________ 1 Any 2 Medical treatment 3 Hospitalization 4 Other
Action
If other then please specify _________________________ Comments
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
7th Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Imatinib Failure Patients
7th Form Therapeutic decision after failure
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
TREATMENT AFTER FAILURE Imatinib ongoing 0 No
1 Yes If No, please specify
Date of Discontinuation dd mm yyyy |__|__| |__|__| |__|__|__|__|
Dose
1 400mg/day 2 600mg/day 3 800mg/day 4 Other
New treatment 0 No 1 Yes
If yes then please specify
Drug: _________________________
Dose: _________________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug: _________________________
Dose: _________________________
7th Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug: _________________________
Dose: _________________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug: _________________________
Dose: _________________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug: _________________________
Dose: _________________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Drug: _________________________
Dose: _________________________
Period of administration
From dd mm yyyy |__|__| |__|__| |__|__|__|__|
To dd mm yyyy |__|__| |__|__| |__|__|__|__|
Experimental drug 1 0 No 1 Yes
Comments
1 If you don’t wish to specify the name of drug then, check experimental drug
7th Form, Page 3 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
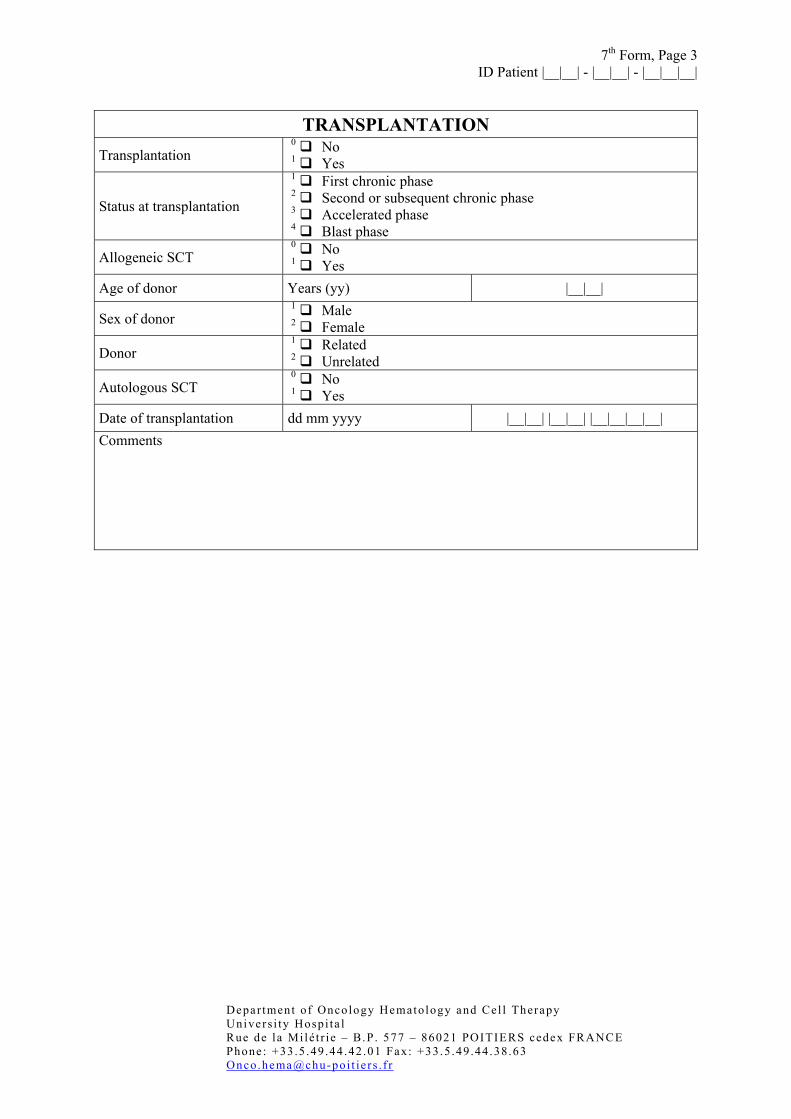
TRANSPLANTATION
Transplantation 0 No 1 Yes
Status at transplantation
1 First chronic phase 2 Second or subsequent chronic phase 3 Accelerated phase 4 Blast phase
Allogeneic SCT 0 No 1 Yes
Age of donor Years (yy) |__|__|
Sex of donor 1 Male 2 Female
Donor 1 Related 2 Unrelated
Autologous SCT 0 No 1 Yes
Date of transplantation dd mm yyyy |__|__| |__|__| |__|__|__|__| Comments
7th Form, Page 4 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
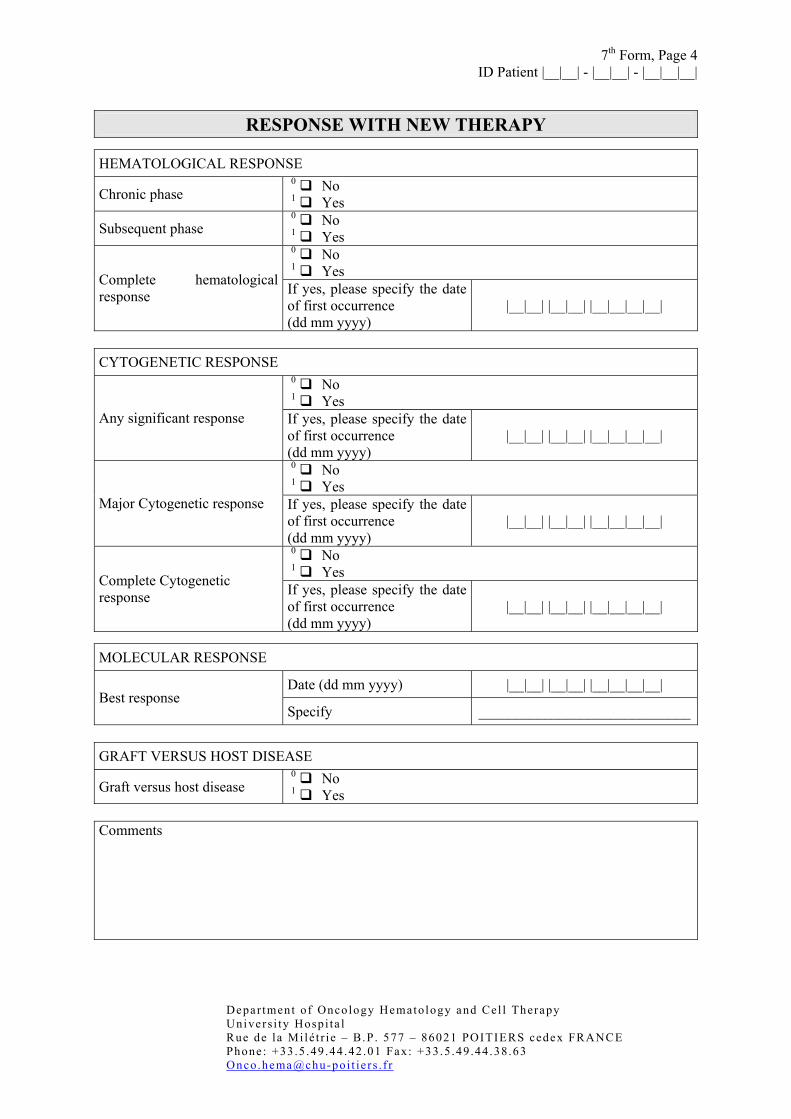
RESPONSE WITH NEW THERAPY
HEMATOLOGICAL RESPONSE
Chronic phase 0 No 1 Yes
Subsequent phase 0 No 1 Yes 0 No 1 Yes Complete hematological
response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
CYTOGENETIC RESPONSE
0 No 1 Yes
Any significant response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
0 No 1 Yes
Major Cytogenetic response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
0 No 1 Yes Complete Cytogenetic
response If yes, please specify the date of first occurrence (dd mm yyyy)
|__|__| |__|__| |__|__|__|__|
MOLECULAR RESPONSE
Date (dd mm yyyy) |__|__| |__|__| |__|__|__|__| Best response
Specify _____________________________ GRAFT VERSUS HOST DISEASE
Graft versus host disease 0 No 1 Yes
Comments
EUROPEAN REGISTRY OF CHRONIC MYELOGENOUS LEUKEMIA PATIENTS IN FAILURE AFTER IMATINIB THERAPY
By European Leukemia Net
CML WP4
8th Form, Page 1 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
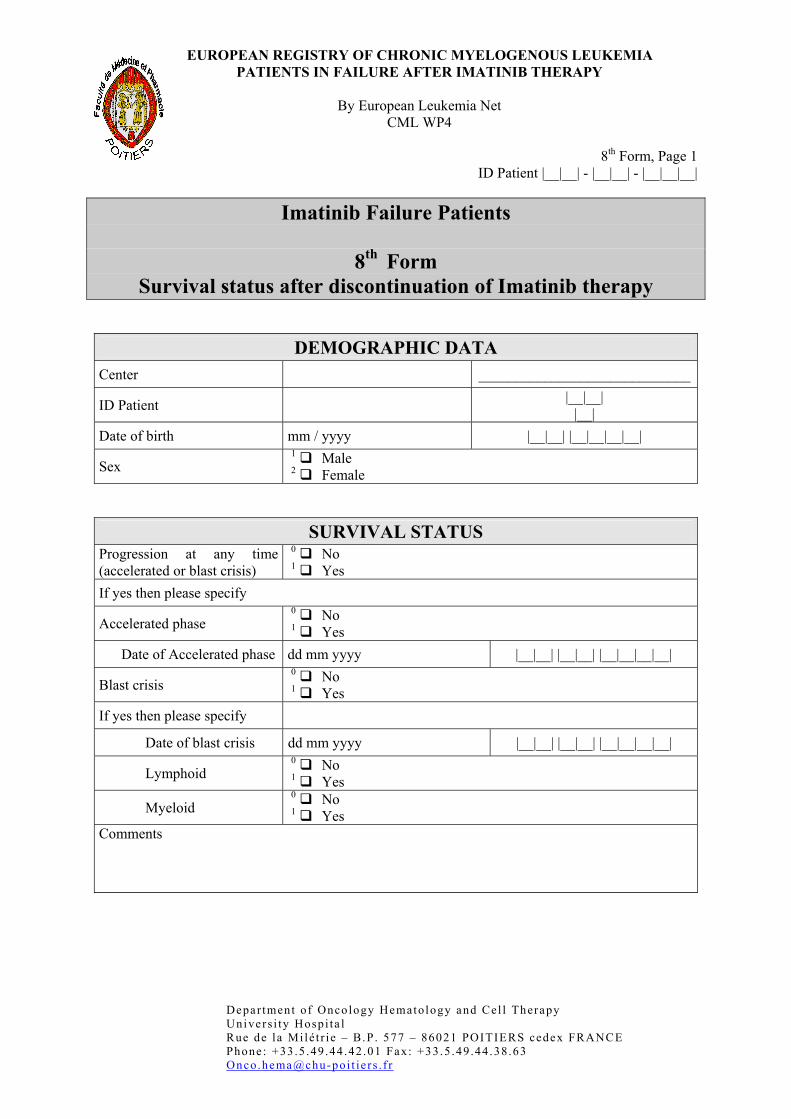
Imatinib Failure Patients
8th Form Survival status after discontinuation of Imatinib therapy
DEMOGRAPHIC DATA Center _____________________________
ID Patient |__|__| |__|
Date of birth mm / yyyy |__|__| |__|__|__|__|
Sex 1 Male 2 Female
SURVIVAL STATUS Progression at any time (accelerated or blast crisis)
0 No 1 Yes
If yes then please specify
Accelerated phase 0 No 1 Yes
Date of Accelerated phase dd mm yyyy |__|__| |__|__| |__|__|__|__|
Blast crisis 0 No 1 Yes
If yes then please specify
Date of blast crisis dd mm yyyy |__|__| |__|__| |__|__|__|__|
Lymphoid 0 No 1 Yes
Myeloid 0 No 1 Yes
Comments
8th Form, Page 2 ID Patient |__|__| - |__|__| - |__|__|__|
Depar tment of Oncology Hematology and Cel l Therapy Univers i ty Hospi ta l Rue de la Mi lé t r ie – B.P . 577 – 86021 POITIERS cedex FRANCE Phone : +33 .5 .49 .44 .42 .01 Fax: +33.5 .49 .44 .38.63 Onco.hema@chu-poi t ie r s . f r
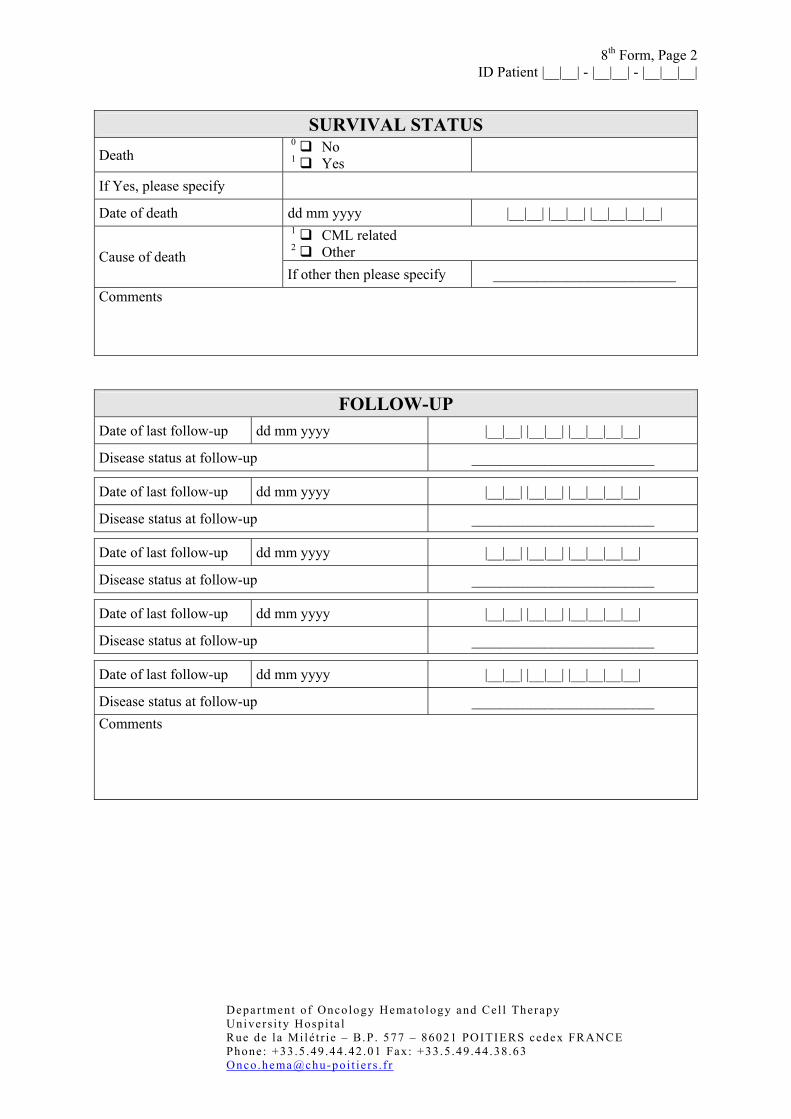
SURVIVAL STATUS
Death 0 No 1 Yes
If Yes, please specify
Date of death dd mm yyyy |__|__| |__|__| |__|__|__|__| 1 CML related 2 Other Cause of death If other then please specify _________________________
Comments
FOLLOW-UP Date of last follow-up dd mm yyyy |__|__| |__|__| |__|__|__|__|
Disease status at follow-up _________________________
Date of last follow-up dd mm yyyy |__|__| |__|__| |__|__|__|__|
Disease status at follow-up _________________________
Date of last follow-up dd mm yyyy |__|__| |__|__| |__|__|__|__|
Disease status at follow-up _________________________
Date of last follow-up dd mm yyyy |__|__| |__|__| |__|__|__|__|
Disease status at follow-up _________________________
Date of last follow-up dd mm yyyy |__|__| |__|__| |__|__|__|__|
Disease status at follow-up _________________________ Comments





























