Embed Size (px)
Citation preview
Immature Myocardium & Fetal Circulation
Seoul National University Hospital
Department of Thoracic & Cardiovascular Surgery
Fetal Circulation
• Is adapted to a special situation
• Depends on placenta for O2/nutrients
• Is rarely overloaded, but if overloaded little reserve
Fetal Circulation
Parallel circulation (combined output)
Communications between R and L heart
Pulmonary circulation is redundant
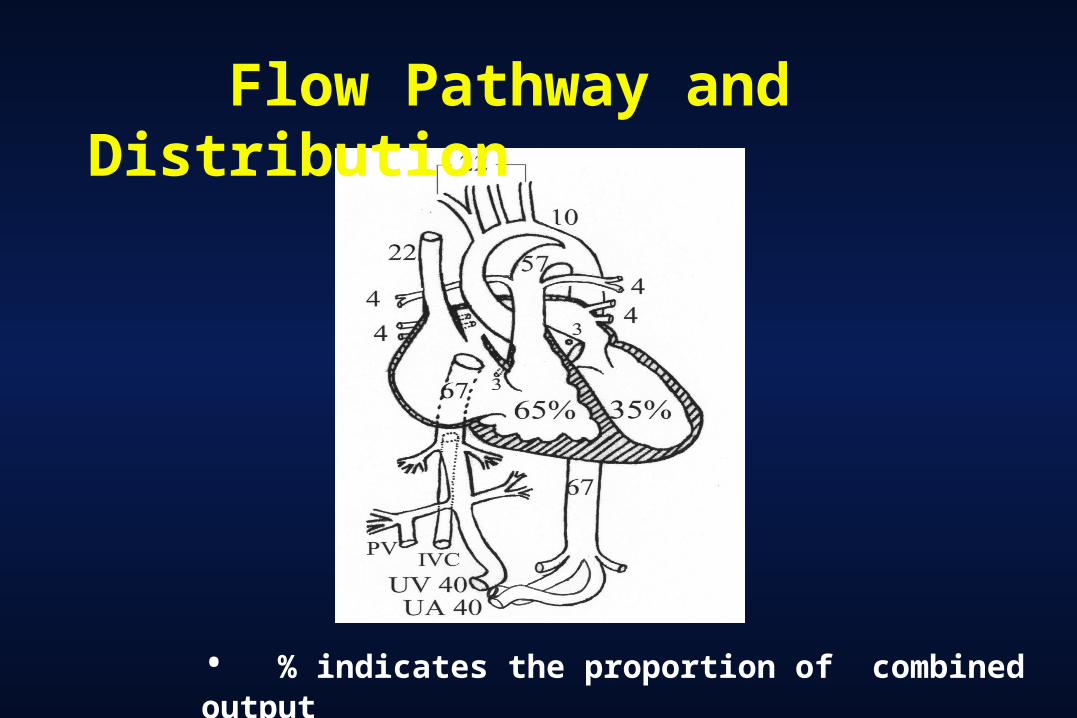
Flow Pathway and Distribution
• % indicates the proportion of combined output
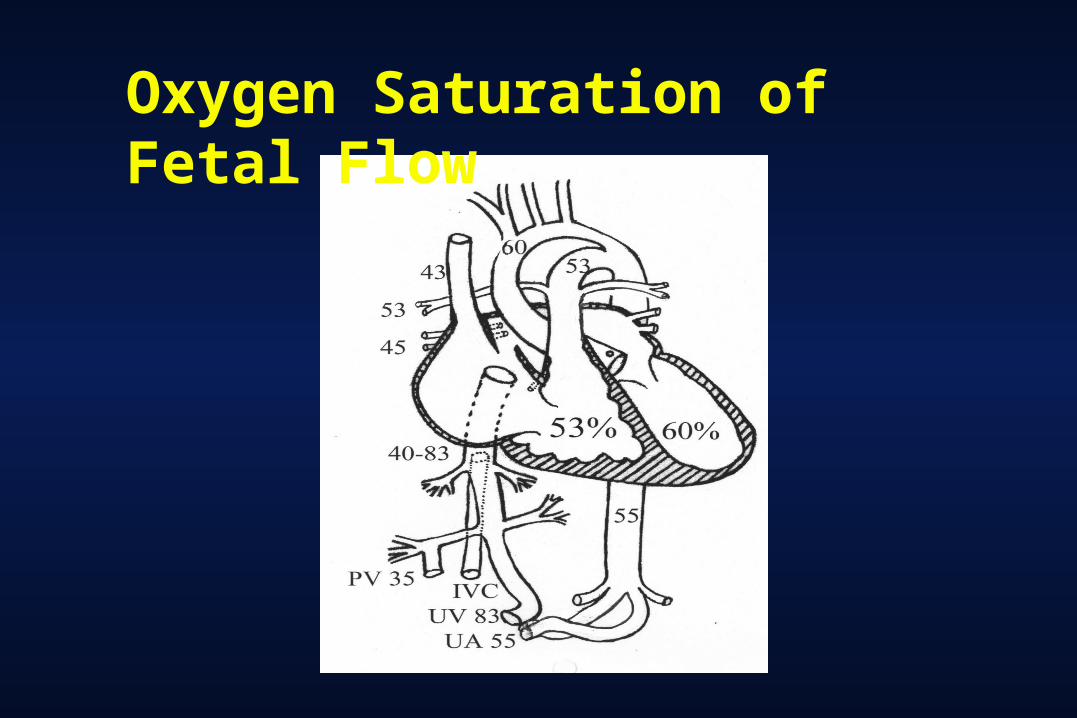
Oxygen Saturation of Fetal Flow
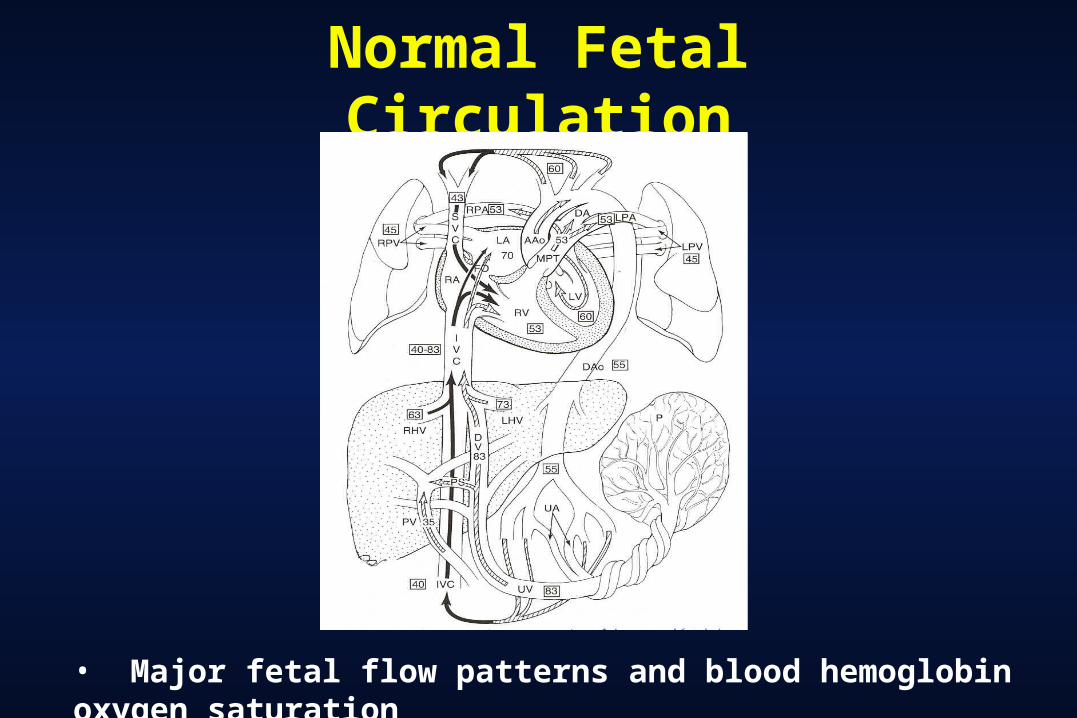
Normal Fetal Circulation
• Major fetal flow patterns and blood hemoglobin oxygen saturation
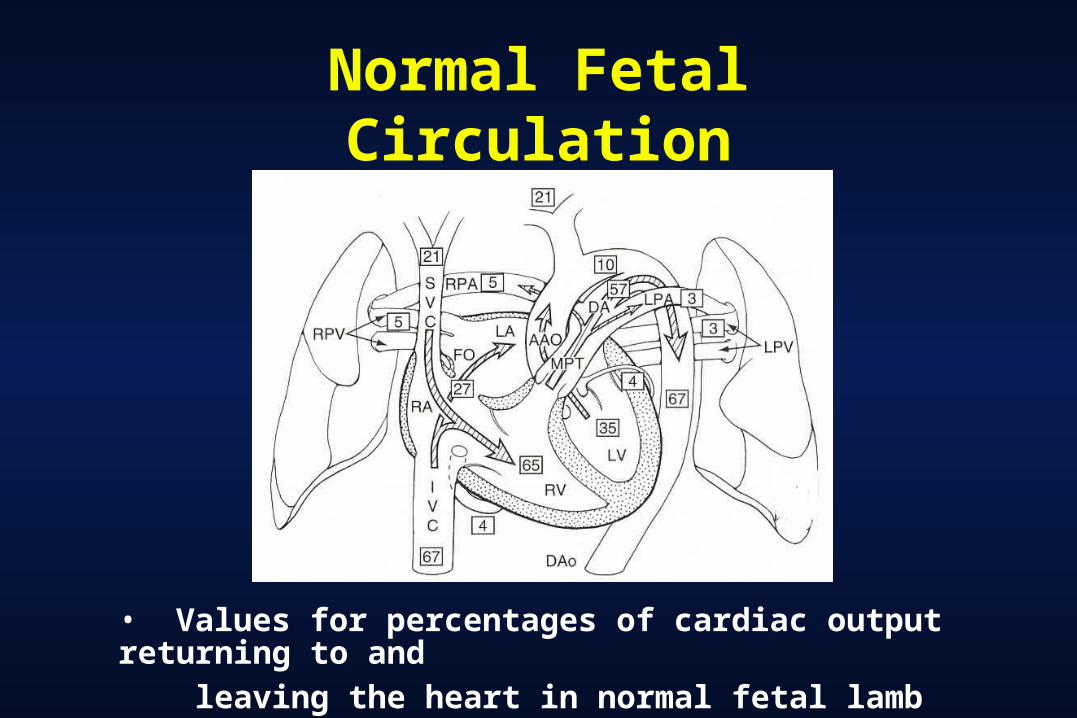
Normal Fetal Circulation
• Values for percentages of cardiac output returning to and
leaving the heart in normal fetal lamb
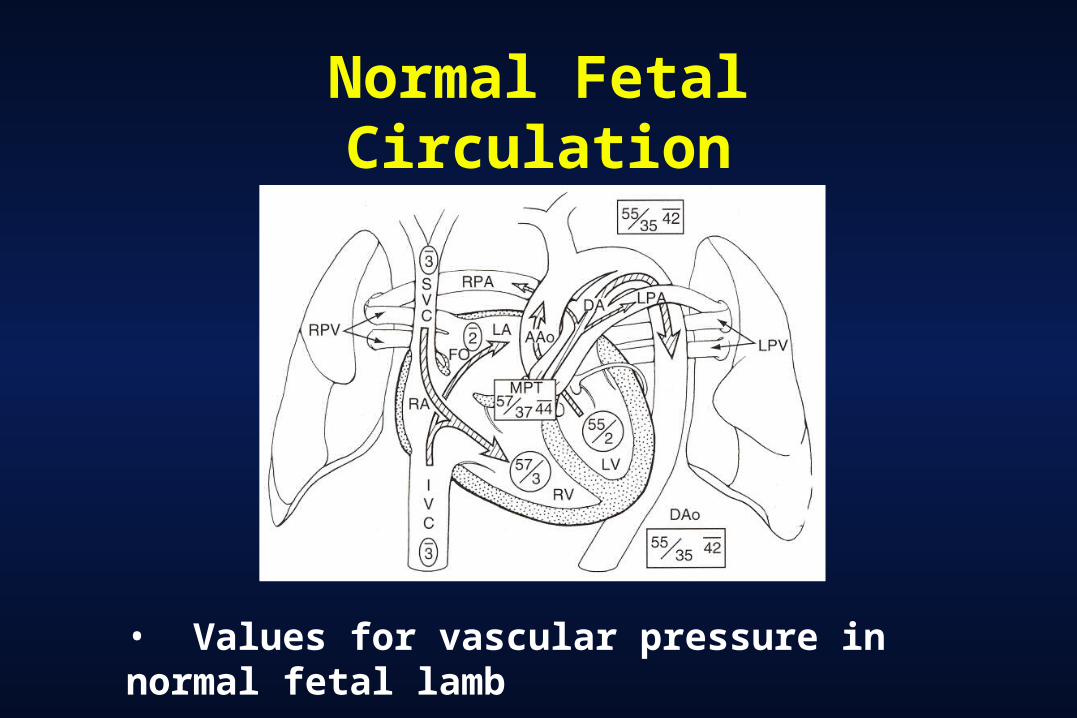
Normal Fetal Circulation
• Values for vascular pressure in normal fetal lamb
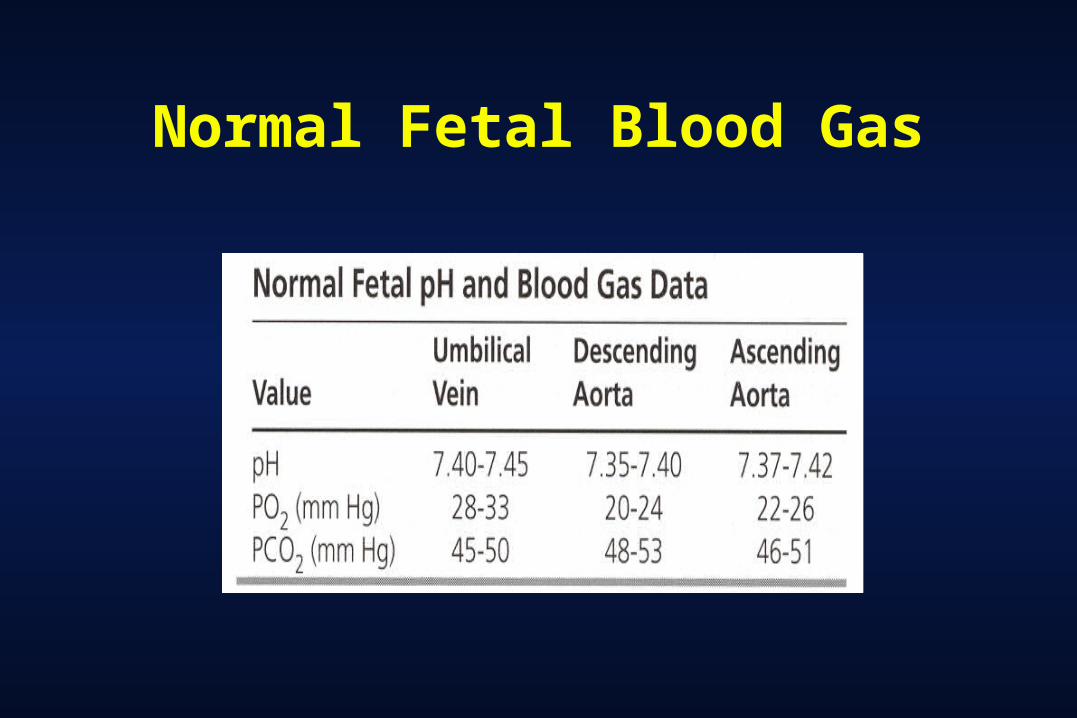
Normal Fetal Blood Gas
Transitional Circulation and CHD
• As circulation separates, TGA can not supply enough oxygen to the body
• Obstructed pathway in either side hardly tolerate
right : PA or critical PS in any CHD
left : Aortic atresia or critical AS, IAA, COA
mitral atresia + small PFO; obstructed TAPVR
Transitional Circulation
• Dramatic changes in circulation at the moment of birth and onwards :
Air breadth - lung expansion - Rp ↓ -
Qp ↑ - LA pressure ↑ - PFO ↓
P O2 ↑ - ductus arteriosus and venosus ↓
Obliteration of placental circulation - Rs ↑ -
IVC pressure ↓ - PFO ↓
Congenital Heart Disease in Fetus
• Often silent :
TGA : has little effect
HLHS : RV is slightly overloaded
PA + IVS : no effect at all
• When CHD causes volume overload, heart fails and hydrops ensues
Neonatal Circulation and CHD
Neonatal circulation
Potential of increased Rp
Potential of atrial communication
Compliance of two ventricles is nearly equal
CHD and neonatal circulationVSD, PDA : usually not symptomatic
ASD : usually not symptomatic
Neonatal Circulatory Physiology
1. Decreased compliance of fetal & neonatal right
& left ventricle
2. Decreased capacity for peripheral vasodilation
3. Decreased capacity for response to volume load
due to diminished preload reservoir
Characteristics of Immature Myocardium
1. Greater tolerance to hypoxia & normothermic ischemia in experimental study
1) greater capacity for anaerobic glycolysis 2) greater buffering capacity 3) decreased ATP flux secondary to lower levels of 5-
nucleotidase2. Less tolerant to ischemia based on the duration of ischemia
at the onset of contracture or intracellular accumulation of sodium and calcium, but recovery of pump function was not assessed by several reports.
3. Compromised secondary to cyanosis, volume or pressure overload with associated ventricular hypertrophy & subendocardial ischemia in clinical setting
Normal Neonatal Myocardium
Characteristics of normal myocardium• Myocardial structure Myocytes are smaller cells with single nuclei than adult and less contractile materials(30%) than adult(60%), more water, less collagen, more noncontractile protein. Small volume of mitochondria, rudimentary sarcoplasmic reticulum, fewer myofibrils, absence of T-tubules, organization of immature muscle cells in random
• Function Velocity of shortening is less. Less compliant myocardium due to increased amount of noncontractile cellular element in immature myocardium
Normal Neonatal Myocardium
• Response to hypoxia Increased ability to tolerate periods of anoxia due to increased glyc
ogen storage and glycolytic acitivity
• Response to ischemia Increased resistance to ischemia , but first 3-8 days of life
Early onset of irreversibly injured myocardium than mature myocardium.
More reperfusion injury, but rapid recovery without irreversible injury than mature myocardium
• Decreased clear ability of lactate production and with stress caused by underlying cardiac disease, which causes high morbidity & mortality.
Structure of Neonatal Myocardium
1. Stiffer due to more water, less collagen, more contractile
protein
2. Smaller cells with single nuclei, poorly developed
intercalated disks, greater mitotic activity, fewer mature
mitochondria, and fewer myofibrils
3. Greater storage of glycogen, enhanced rate of anaerobic
glycolytic ATP production
4. Calcium homeostasis is different & more dependent on
external calcium
Metabolism of Neonatal Myocardium
• Preference for glucose & glycogen over free fatty acid as energy substrates and greater concentration of glycogen in the heart • Enhanced anaerobic glycolytic ATP production capacity t
hat may represent adaptation to relative O2 deprivation during fatal condition
• Significant difference in calcium metabolism (1) Amount of calcium within cardiac cell of neonate is significantly less than that of adult. (2) Decreased ability of immature sarcoplasmic reticulum to accumulate calcium ---- the strength of contraction can be increased in neonate by increasing in extracellular calcium
Neonatal Myocardial Management
Trend of management In 1990
Equal split in the preference for crystalloid vs. blood
cardioplegic solutions
In 1995 Trend toward the use of blood based solutions, with only
20% using crystalloid solutions
Neonatal Cardiac Surgery
Potential for damage duing surgery
1. Preischemic stage Hypothermia
2. Ischemic stageCalcium content
Magnesium
Single vs. multidose
3. Postischemic stage
Myocardial Protection vs. Injury
• The surgical treatment of complex congenital heart
defects in the neonate requires controlled conditions
with unimpaired exposure in a bloodless, immobile
operative field.
• The cost one pays to obtain such exposure, however,
is a period of ischemic insults to myocardium.
Effect of Hypothermia
The term, cooling contracture, rapid cooling contra
cture refers to as marked increase in resting in resp
onse to sudden decrease in temperature.
(activation of myofilaments by the release of calciu
m from intracellular stores)
Damage at Ischemic Stage1. Calcium content
o Optimal calcium concentration(?)o Calcium paradox in acalcemic solutionso PH, Na, duration of ischemia, effects(?)
-> Reduction in the ionized level of this cation in the cardioplegic solution results in better myocardial recovery
2. Magnesiumo Magnesium help maintain a negative resting membrane potential and
competitively inhibits sarcolemmal calcium influx o Superior functional recovery with solution containing magnesium in
blood perfused neonatal rabbit model o Optimal concentration is 16 mmol/l citrate calcium level temperature
3. Single-dose vs. multidose o No advantage with multiple administration
o More evident detrimental effects at infusion temperatures below 20oC and with increasing frequency of administration
Damage at Postischemic Stage
After early reperfusion, the postischemic myocardial functional alternation may ensue
Intervention aimed at the reduction of reperfusion-mediated injury
1. substrate enhancement & ionic modification
2. free radical scavenging
3. leucocyte depletion
4. reduction in perfusion pressure and temperature
Protocols for Neonatal Myocardial Protection (I)
Preischemic phase
A. Moderate hypothermic (25~28oC) continuous CP bypass,
with intermittent periods of low flow (50ml/kg/min)
B. Ionized calcium level in the range of 0.5~0.6 mmol/l
* fresh frozen plasma (citrate)
C. Gas flows are adjusted to maintain PCO2 level at
40~45 mmHg during cooling phase
Protocols for Neonatal Myocardial Protection (II)
Ischemic phase
A. 2:1 blood : crystalloid formulation (Hct 5%)
B. Alkalotic cardioplegic solutions may not be a as effe
ctive in the neonatal heart
C. Initial infusion is at or above room temperature bu
t is cooled to 10oC
Protocols for Neonatal Myocardial Protection (III)
Postischemic phaseA. Bypass flow rate is reduced to 50% & temperature
20~25oC for several minutes.
B. Ionized level of calcium are not normalized until
myocardial activity has returned.