Embed Size (px)
Citation preview

Article ID: WMC001652 2046-1690
Immediate Memory Functioning and IntelligenceQuotients of 18-30 Years Age Group Using New DataDerived From the Benton Visual Retention Test:Applicability to Alzheimers Disease PatientsCorresponding Author:Dr. Simon B Thompson,Associate Professor, Psychology Research Centre , Bournemouth University, BH12 5BB - United Kingdom
Submitting Author:Dr. Simon B Thompson,Associate Professor, Psychology Research Centre , Bournemouth University, BH12 5BB - United Kingdom
Article ID: WMC001652
Article Type: Original Articles
Submitted on:01-Mar-2011, 03:50:51 PM GMT Published on: 02-Mar-2011, 07:08:49 PM GMT
Article URL: http://www.webmedcentral.com/article_view/1652
Subject Categories:GERIATRIC MEDICINE
Keywords:Alzheimers Disease,Benton Visual Retention Test; Correlation, Dementia, Immediate Memory;Intelligence Quotients, Memory, Normative Values, Wechsler, Younger Age Group
How to cite the article:Thompson S B, Gander J . Immediate Memory Functioning and Intelligence Quotients of18-30 Years Age Group Using New Data Derived From the Benton Visual Retention Test: Applicability toAlzheimers Disease Patients . WebmedCentral GERIATRIC MEDICINE 2011;2(3):WMC001652
Source(s) of Funding:
Source of funding: None.
Competing Interests:
Competing interests: None.
WebmedCentral > Original Articles Page 1 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Immediate Memory Functioning and IntelligenceQuotients of 18-30 Years Age Group Using New DataDerived From the Benton Visual Retention Test:Applicability to Alzheimers Disease PatientsAuthor(s): Thompson S B, Gander J
Abstract
The aim of this study was to create a normative dataset of performance scores for the Benton VisualRetention Test (BVRT) for individuals aged between18 and 30 years. Previously, no normative dataexisted for BVRT performance for this particular agegroup.The data collected examined the correlationbetween cognitive functioning as tested by theWeschler Adult Intelligence Scale III (WAIS III) andBVRT.The Hospital Anxiety and Depression Scale(HADS) was used as a screening process to gain acognitive profile of the sample population.Fiftyparticipants carried out the BVRT, WAIS III andHADS.The data collected were analysed using thePearson’s Correlation Co-efficient and resultsindicated a strong relationship between BVRTperformance across all three administrations and fullIQ. In addition, strong relationships were identifiedbetween Total Correct responses and Total Errorsscore with Verbal IQ and Performance IQ. However,no significant correlations were found between Anxietyand Depression levels and BVRT performance, thismay have been due to 90% of the sample being withina normal, healthy range.These findings suggest IQlevels are a strong indicator for BVRT performance.Furthermore, the development of a new set ofnormative data for the 18-30 year old age group, willallow the use of the BVRT as a clinical instrument toassess brain damaged and diseased individuals moreaccurately, particularly those diagnosed withAlzheimer’s disease.
Introduction
Individuals may suffer from impaired cognition as aresult of brain injury or brain disease. This could resultin the skills and abilities the individual had prior toinjury or disease onset, being significantly damaged orcompletely lost. Brain injury or disease can affect anypart of the brain and the impairment can be displayedin any cogni t ive ski l ls such as at tent ion,
communication, visual perception, and memory. Over1.4 million people per year, sustain brain injury andone of the most common age groups at risk are 15-19year olds. Brain disease affects a considerably largerpercentage of the population e.g. Alzheimer’s aloneexceeding 3 million each year (Fay, 2010) andParkinson affects 12,000 people each year in the UKalone (Parkinson’s disease Society, 2010).Most research investigating brain damage and diseasehas attempted to measure the extent of impairment onthe individual’s cognitive abilities. The Benton VisualRetention Test (BVRT) developed by Arthur L. Benton(Benton Sivan, 1992) is a widely used instrument,assessing individual’s visual perception, visualmemory and visuo-constructive abilities, for thisreason it is highly valued in clinical settings(Thompson, Ennis, Coffin & Farman, 2007; Thompson,2 0 1 1 ) . L e z a k ( 1 9 8 3 ) a n d m a n y o t h e rneuropsychologists through time often use figuredrawings to assess people's deficits because of theirsensitivity in detecting many types of cognitiveimpairments and diseases. This is the main strength ofthe BVRT. The BVRT has been used to assess braindisorders such as Attention-deficit hyperactivitydisorder (ADHD), Alzheimer’s disease, stroke patients,Bipolar disorder, Schizophrenia and many others.Marsh and Hirsch (2006) looked at the effectiveness ofdifferent neuropsychological tests and showed theBVRT to be significantly more effective in detectingdefective visual retention. They further recommendthat it is highly valuable for evaluating brain damagedor diseased patients.Tasks which are visual memory and visuo-spatial innature have often been included in many intelligencescales (Binet & Simon, 1908). However, thesesubtests were not an adequate measure of anyspecific visual-memory or visuo-spatial abilities and soArthur L. Benton designed his first edition of the BVRT(Benton, 1946). Since then revisions andimprovements have been made and the BVRT iscurrently in its Fifth Edition (Benton Sivan, 1992).There are many ways of detecting brain damage anddisease e.g. Tomography (fMRI, PET, CAT) is atechnique using gamma rays, ultrasound or x-rays to
WebmedCentral > Original Articles Page 2 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
obtain detailed images of areas inside the body. Whilstthese tests are effective in detecting physical damage,they cannot measure the amount of memory loss orcapacity to sustain attention. Neuropsychologicalinstruments have proven far more useful indetermining an individual’s cognitive function.Neuropsychological tests, such as the BVRT, are usedto analyse and interpret the individual’s responses tocognitive based tasks and compare performance tonormative data. The results of these tests allow thepsychologist to make inferences about what theindividual is able to do within his or her environment,by assessing their performance on the specific tasksrelative to how a cohort of healthy people within thesame age range performed on the same set of tasks.By identifying brain-behaviour relationships,treatments can be tailored to focus on the individual’sparticular strengths to compensate for their limitationsin cognitive functioning.In clinical settings the BVRT is often used as aninstrument to determine cognitive function in the olderpopulation that are more susceptible to brain diseasessuch as Alzheimer’s and Parkinson’s disease.Whereas, in educational fields the main focus of thetest has been to asses learning difficulties andattention disorders such as ADHD in young childrenup to early/mid teens. Currently there is a lack ofresearch assessing cognitive function in late teens andyoung adults, or the data needs updating (eg Benton,Eslinger & Damasio, 1981). The existing normativedata are based on children aged up to 15 and adultsover the age of 30. The importance of the BVRTremains highly valued and it is important to havenormative data to demonstrate the performance ofindividuals within this age group, thus providing a baseline comparison for patients that may suffer from braininjury or disease that affects their cognitive function(Thompson, 2002). Existing normative data are basedupon correlations with IQ levels as this has beenidentified as a key factor in BVRT performance(Arenberg, 1978; Le Carret, Rainville, Lechevallier,Lafont, Letenneur & Fabrigoule. 2003; Emdad &Sondgaard, 2006).Cognitive decline in older populationsSignificant correlations between performance andchronological age have been identified, and in earlydetection of brain disease such as Alzheimer’sconcerning the older population. Arenberg (1978)studied males that had received a high level ofeducation with a good economic status, and found agradual decline in BVRT performance from 20-80years of age, and an increased rate of number oferrors when completing the tasks from 60-70 and70-80 years of age. However as noted previously,
research has indicated significant correlationsbetween intelligence and BVRT performance, and sothese findings may only be representative ofindividuals with advanced levels of education. Theresearch of Seo and colleagues (2007), offered furthersupport to these findings. They looked at the BVRTperformance of an educationally diverse elderlypopulation on the BVRT and found that both age andeducation play a role in non-verbal memory andreconstructive abilities. Both older age and lowereducational levels related to poorer performance onthe BVRT. Poitrenaud and Clement (1965) carried outa similar study on a culturally diverse population; thefindings support those of Seo and colleagues (2007).The BVRT Manual (fifth edition) provides normativedata which demonstrates a significant relationshipbetween chronological age and BVRT performance; aprogressive increase from 8 to 15 years of age(Benton Sivan, 1992). Performance begins toprogressively decline through the fifties; a drop ofabout 1 point in mean number of correct score, then afurther 2 points in the sixties. Benton concluded thatperformance on the BVRT declines significantly afterthe age of 60 years and inter-individual variabilityc o r r e s p o n d i n g l y i n c r e a s e s . V a r i o u sneuropsychologists have researched into whatchanges occur within the brain that results in cognitivedecline. It has been found that it may be as a result ofa loss of synapses within circuits of the hippocampusand also a decrease in metabolic activity in theentorhinal cortex which is the major input and output ofthe hippocampus. Leon (2001) found that in normalindividuals, the level of metabolic activity in theentorhinal cortex can predict the amount of cognitivedecline over the next 3 years.Alzheimer’s disease and other brain diseasescommonly affecting the older populations have beenstudied in some depth to understand the contributionof the disease to further impairment of the individual’scognitive abilities. Alzheimer’s in particular, ischaracterised by progressive brain deterioration andimpaired memory and other mental abilities. An articleby Amieva and colleagues (2005) reported a 9 yearcognitive decline prior to the onset of dementia, withsignificantly low performances on the BVRT even inthe early years, which progressively declined furtherwith time. It is however, important to note inlongitudinal studies, such as this, other factors thatmay be responsible for the change need to be takeninto account. Thompson, MacDonald and Coates(2001) carried out a study in which they found, using abattery of neuropsychological tests including the BVRT,significant improvement on performance in bothvisuo-spatial and visual memory tests after 16 weeks
WebmedCentral > Original Articles Page 3 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
of Aricept treatment used to improve the symptoms ofAlzheimer’s.Netherton and colleagues (1989) used the BVRT tostudy patients with Parkinson’s Disease, thesepatients showed an increase in figural reproductionerrors between test periods spaced six months apart,the control group however showed no increase inerrors over this time and fewer errors in general.Poitrenaud and Barrere (1973) looked at 46 middleaged individuals who had been either referred forneuropsychological testing or who had reported havingexperienced mental difficulties. The study involved abattery of five tests, one of which was the BVRT. Ofthe 46 patients, 31 performed normally and 15performed defectively. Five years later the sample wasassessed again. Subsequent testing showed that ofthe 46, 30 were diagnosed as mentally intact and 16diagnosed with dementia. Of the 16 patientsdiagnosed with dementia, 14 were from the original 15that performed badly. The Rey Auditory-VerbalLearning Test, another of the other five battery tests,and the BVRT accounted for 93% of the correctprediction rate and individually showing 85% predictiveaccuracy.Brain damage and disease in younger populationsDisorders of a visuo-spatial nature are particularlyprevalent after damage to the posterior parietal lobe,such as unilateral neglect. Balint’s syndrome andconstructional apraxia patients often have similarlesions within this region. Vilkki (1989) studied braindamaged patients with lesions to the anterior andposterior areas of the brain. He showed subjects withanterior lesions made significantly more perseverationerrors (figure in previous design replicated inreconstruction of following design) than subjects withposterior lesions, with both left and right hemispheresof the brain. Petris (1981) compared performance onthe BVRT of brain damaged patients to controlpatients. Patients with brain disease produced ahigher average percentage of omission errors (28%) -single figure of a design being completely omitted orno recognisable attempt was made to reconstruct thefigure - than the control group (14%), and higherfrequency of s ize errors (2.7% vs. 0.3%)(Reconstruction wrongly sized), yet made lessperseveration errors than the control group (33% vs.42%). Benton Sivan (1992) concluded that omissionerrors and size errors are particularly prominent inpatients with cerebral disease. Damage locatedtoward the front of the brain tends to result in the mostsevere problems associated with attention andconcentration, which could explain the omission andsize errors found.The BVRT has been used in adults and younger
individuals that have suffered from strokes andpost-traumatic stress. By using the BVRT they havefound a cognitive decline due to the impact of traumaon hippocampal functioning, which affects memory.Emdad and Sondegaard (2006) studied PostTraumatic Stress Disorder (PTSD) patients byassessing intelligence levels using the RavenStandard Progression Matrices (RSPM) (seeThompson, 2000; 2001; 2006; 2010), and visualmemories using the BVRT. In comparison to thecontrol group, the PSTD patients demonstrated astrong negative correlation between the BVRT andRSPM. PSTD patients showed poor short term,non-verbal memory, and these deficits were related toindividual’s intelligence. However the same resultswere not found in the control group, where comparabledifferences in RSPM score showed no significantrelationship to performance on the BVRT.In the younger population, the use of the BVRT inassessing learning difficulties in children and youngadults has been extremely important in theimprovement of their abilities and assessing theirprogress. Dige and Maarh (2008) studied patients withdifferent levels of ADHD. Using the BVRT, they wereable to show ADHD patients performed considerablypoorer in such tests, and the more severe the case ofADHD the higher the amount of errors.Park (2008) looked at Schizophrenic patients and thenature of visual recall and recognition through the useof the BVRT, she found that patient’s performancewas widely variable in visual memory and there wasno significant difference between recall andrecognition. From looking at research into the affectsof these brain diseases and the use of the BVRT as aclinical instrument, it is clear to understand its value inthis field. The BVRT appears to tap into a uniquecombination of skills that are characterised by bothshort-term memory and psychomotor abilities. TheBVRT not only records where errors are made inresponses, but also the different types of errors beingmade, this allows for assessment of qualitative as wellas quanti tat ive patterns to faci l i tate morecomprehensive interpretation. For exampleRobinson-Whelen (1992) reported a significantdifference between controls and patients with mild tomoderate levels of dementia, specifically in thenumber of omission errors that were made. Baum,Edwards, Yonan and Storandt (1996) also foundspecific associations between test errors andAlzheimer’s patients.Affects of mood disorders on cognitionAnxiety and Depression are known disorders that canimpact performance on many cognitive based tasks(Eysenck, 1997, p.8). Such that if individuals are
WebmedCentral > Original Articles Page 4 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
feeling anxious or depressed this may significantlyaffect their performance. Anxiety suggests thatindividuals may be tense, restless and have troubleconcentrating on the current task at hand. Similarsymptoms may be found in individuals that aredepressed; fatigue, difficulty concentrating and lack ofmotivation will affect performance and so how theyperform on a given task will not be an accuratemeasure of how they would usually perform had theybeen in a calm, relaxed, healthy state. Especially inmedical practice, it is very important to ensure thatpossible mood disorders such as depression andanxiety are not influencing a patient’s performance.Weems and colleagues (2007) found certain cognitiveerrors demonstrated specific associations with anxietysymptoms. Findings from Ellis and colleagues (2008)further support this, and showed mild anxiety wasassociated with better cognition, where more severeanxiety was associated with worse cognition.Several studies have indicated that sufferers of severedepression may experience impairment in motivation,attention, and concentration. This is related to poorBVRT performance, however not as significantly assuch illnesses as Dementia (Crookes & McDonald,1972; Birch & Davidson, 2007). Research into theeffects of less severe levels of Depression is yet to becompleted and therefore the current findings areinconclusive.Intelligence and cognitive abilitiesIn a vast amount of research on cognitive abilities amajor factor has been intelligence. As educationallevels increase so does performance on tests such asthe BVRT, and so higher IQ scores suggest bettercognitive skills. In the early 19th century, the conceptof intelligence was widely debated. David Wechslerviewed intelligence as a multidimensional responseconstruct, one that manifests itself in many forms, notonly as a global entity, but as a collection of specificabilities. Weschler concluded that intelligence is the‘’capacity of the individual to act purposefully, to thinkrationally and deal effectively with his environment’’(Weschler, 2002).Le Carret and colleagues (2003) carried out researchinto how educational levels influence visual workingmemory using the BVRT on elderly individuals. Theyfound that higher levels of intelligence resulted inbetter performance but as a result of better executiveabilities rather than visual discrimination skills. Theyconcluded that higher levels of education meantindividuals were able to use more efficient strategies.The Normative standard section of the BVRT statesthat performance on all three administrations for thethree forms correlates substantially with intelligencelevel (Benton Sivan, 1992). Correlation coefficients for
the stated age groups claim to average from 0.46 to0.71. All published normative data collected andexplained in the manual are described on the basis ofthe relationships between intellectual level andchronological age with BVRT performance.
Method
RationaleThe aim of this study is to gain a set of normative datafor performance on the BVRT for individuals agedbetween 18 and 30 years of age. Currently nonormative data exists for BVRT performance for thisparticular age group. The BVRT is an essentialinstrument in clinical research when studying patientswith brain disease or brain damage. However, for anaccurate assessment of an individual’s BVRTperformance, a set of normative data for that specificage range for comparison must exist. Furthermore,this study aims to look at the correlation betweencognitive functioning (as tested by the WAIS III andIQ’s) and BVRT scores for this age group, todetermine if a significant relationship exists betweenIQ and BVRT performance as has been observed inother age groups previously studied.MaterialsBenton Visual Retention TestBenton designed his first edition of the BVRT in 1946(Benton, 1946). After reviewing limitations andweaknesses, reviews have been made, a first revisionwas made in 1955 (Benton, 1955), and furtherrevisions in 1963 (Benton, 1963) and 1974 (Benton,1974). Each time, a new set of normative data havebeen produced for various age groups. Each revisionhas enhanced the use of the BVRT in clinical practiceand research.The BVRT has 3 similar forms of task C, D and E,each consisting of 10 designs containing one or morefigures. There are 4 methods of administration A, B, Cand D. Clinical investigators have devised noveladministrations of the BVRT to answer specificresearch questions. For the purpose of this study,administrations A, B and D will be used to see howhealthy 18 – 30 year olds perform with timeconstrictions and delays outlined below.Administration A – Participant views each design for10 seconds and then immediately reproduces thedesign from memory.Administration B – (serves as a comparison for theamount of time needed to process each stimulus).Participant views each design for 5 seconds andimmediately reproduces the design form memory.Administration D – (requires examinees to retain the
WebmedCentral > Original Articles Page 5 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
percept for a brief period of time). Participant viewseach design for 10 seconds, after a delay of 15seconds, is then asked to reproduce design frommemory.WAIS III David Wechsler designed the first edition of theWeschler Adult Intelligence Scale in 1939 (Weschler,1939). Weschler observed certain attributes which canaccount for the overall variance of intelligence; theseinclude basic human motivations, attitudes andpersonality traits, such as persistence, goal awarenessand enthusiasm. The WAIS reflects an individual’soverall ability, where the subtests look at such skills asabstract reasoning, perceptual skills, verbal skills andspeed processes. Since 1939, revisions have beenmade, to allow for changes in social and culture era,the WAIS is now in its third edition (Weschler, 2002).The Wechsler Adult Intelligence Scale consists of 14subtests. When restricted by time, it is possible tofollow the short form WAIS III, which still remains farsuperior to many other intelligence scales available(Weschler, 2002). For the purpose of this study theshort form of WAIS III will be used. The scoringprocess involves the conversion of raw scores intoscaled scores which provide 3 levels of IQ;Performance IQ, Verbal IQ and Full Scale IQ.Hospital Anxiety and Depression ScaleThe HADS is a self screening questionnaire firstdesigned in 1983 by Snaith and Zigmond, based on anitem analysis of a longer list of items given to patientsattending an out-patient clinic (Snaith & Zigmond,1983). The Anxiety scale was based on ‘feelings oftension’, ‘tendency to unnecessarily worry’ and‘apprehensive anticipation’. The Depression Scale wasbased on ‘enjoyment of usual activities’, ‘retention of asense of humour’, ‘depressed mood’ and ‘optimisticattitude’.The HADS is a Questionnaire consisting of 14questions, 7 for anxiety and 7 for depression, eachscoring 0-3 points per item. In this study the HADS isused as a screening technique in order to gain acognitive profile of the sample population. For thisreason the aim is to use participants that score ateither a normal (0-7), mild (7-10) or moderate (11-14)level for both Anxiety and Depression. A score of 15 orhigher suggests possible presence of a mood disorderwhich may interfere with the rest of the study. Experimental hypothesesBased on existing research the hypotheses for thisstudy include:H1 There will be a significant relationship between FullIQ and Total Errors score and Total Correct responseson the BVRT. H2 There will be a significant relationship between Full
IQ and Total Errors score and Total Correct responsesacross the three administrations A, B and D. H3 Both Performance IQ and Verbal IQ will besignificantly correlated with Total Errors score andTotal Correct responses. H4 There will be a significant relationship betweenTotal Errors Score and Total Correct responses andAnxiety and Depression score on the HADS. Study designThis study will look at the interactions betweenPerformance on the BVRT and IQ Levels. A Pearsonproduct-moment correlation coefficient was used toanalyse the relationship between Total Errors score,and Total Correct responses under the 3administrations A,B and D of the BVRT, together with:Full IQPerformance IQVerbal IQA Pearson product-moment correlation coefficientanalysed the relationship between Total Errors score,and Total Correct responses under the 3administrations of the BVRT (A, B and D) andDepression and Anxiety scores on the HADS.In order to determine if age or gender had anysignificant influence on the data collected, a 3 x 2unrelated ANOVA was implemented to investigate asignificant difference in performance on the BVRTbetween genders and age groups. The firstIndependent variable (IV) was gender, which had twolevels; Males and Females. The second independentvariable was age group, and was split into 3 levels;18-20 (mode = 19, median = 19), 21-23 (mode = 21,median = 21) and 24-27 (mode = 26, median = 26).The dependent variables were Total Errors score andTotal Correct responses.ParticipantsA sample of 50 undergraduate BournemouthUniversity students took part in the study; they wererecruited on a volunteer basis. 14 male and 36 femalefirst, second and third year students took part in thestudy. The age range was between 18-30 years old,with the mean age being 22. The sample wasrecruited via emails to students, and through theuniversity study program SONA, this allows first andsecond year students to view the available studies inwhich they can participate with the incentive of gainingresearch experience which is mandatory for theiruniversity course. All participants were British Citizensliving in the United Kingdom with English as their firstlanguage. All participants came from similarsocio-economic and educational backgrounds. Allparticipants were psychologically assessed using theHADS self-screening questionnaire to ensure theywere within the healthy range.
WebmedCentral > Original Articles Page 6 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
ProcedurePrior to the commencement of the study, ethicsapproval was obtained from the BournemouthUniversity Research & Ethics Committee (11.11.2009)to clarify that the study adhered to all ethicalguidel ines. Two computer laborator ies atBournemouth University were booked for 10 sessions,participants were seen for 2 hour sessions over aperiod of 2 weeks; two sessions each Monday, one oneach Tuesday, one on each Wednesday and one oneach Thursday. Five Participants took part in eachsession allowing for confounding variables to becontrolled and for the efficiency of the running of theexperiment within the time allocated. Each participantentered the 1st Lab and sat at individual desksseparated by partitions to ensure there were nointeractions between participants. In front of eachparticipant was a study information sheet, participantinformation sheet, consent Form, HADS questionnaire,WAIS response booklet and 3 BVRT responsebooklets.On commencement of the study the experimenterexplained in full what the study involved, the order inwhich it would be carried out and the aim of theresearch. Participants were asked to read the studyinformation sheet, and given the opportunity to askany questions or to withdraw themselves from thestudy. Once everything was made clear, participantswere asked to fill in the Participant Information sheetand read and sign the Consent Form. When all formswere completed, they were then asked to turn to theHADS Questionnaire. The experimenter instructedparticipants to read each statement and report theirimmediate response to each item without spending toomuch time making long thought-out replies. Allcompleted forms were then collected and the first testwas ready to be administered.The BVRT was displayed on the projector screen atthe front of the lab. The procedure and requirementsof the test were explained using the standardisedexplanation for each administration. The participantscompleted the three administrations which were timedusing a stopwatch by the experimenter. Once theBVRT was completed the three response bookletswere then collected in.The WAIS III Short Form Administration was thenexplained to the participants using the standardisedexplanation in the WAIS III Administration Manual.Eight subtests were carried out en masse toparticipants, the two remaining subtests required oneon one examination and each participant was calledinto the second lab one at a time to carry them out.Once all participants had completed all tests, theywere fully debriefed on every aspect of the study and
again offered the opportunity to ask any questions orwithdraw themselves and any information they hadgiven from the study. They were also informed thatresults were available for collection from theresearchers.
Results
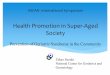
Statistics50 participants took part in the study; their full IQ’sranged from 90 to 155 with an average of 118 andstandard deviation of 16.1. The average of TotalCorrect responses (on all 3 administrations) were20.34 with a standard deviation of 4.36, the averagetotal number of errors made was 16.80, with astandard deviation of 9.98. The average score of theHADS was 3.94 for Depression with a standarddeviation of 3.59 and 3.88 for Anxiety with a standarddeviation of 3.22. SPSS 18 was used for statisticalanalysis of the data (Illustrations 1 - 4).Hypothesis 1A Pearson product-moment correlation coefficient wascomputed to assess the relationship between Full IQand Total Errors score and Total Correct responses onthe BVRT (Illustration 4). There was a significantcorrelation between Full IQ and Total Correctresponses, r = 0.001, n = 50, p = 0.440. There was asignificant correlation between Full IQ and Total ofErrors Score, r = 0.000, n = 50, p = - 0.484. BothVariables; Total Correct responses and Total ErrorsScore demonstrate a strong relationship which issignificant at a level of pThe scatter plot demonstrates a steep decline in theTotal Errors score as individual’s Full IQ increases,illustrating a strong negative correlation. Also, a fewanomalies can be seen within the error scores, 7participants error scores appear to be significantlylarger compared to the rest of the data group. TheTotal Correct responses incline at a milder rate as FullIQ increases and remain more consistent; a strongpositive correlation is clearly demonstrated.Hypothesis 2A Pearson product-moment correlation coefficient wascomputed to assess the relationship between Full IQand Total Errors score and Total Correct responsesacross the three administrations A, B and D:There was a significant correlation between Full IQand Error score Administration A (mean = 5.06), r =0.006, n = 50, p = -.384Error score Administration B (mean = 7.00), r = 0.003,n = 50, p = -.411Error score Administration D (mean = 4.74), r = 0.009,
WebmedCentral > Original Articles Page 7 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
n = 50, p = -.364Correct responses Administration D (mean = 7.36), r =0.005, n = 50, p = .391These relationships are significant at a level of pCorrect responses Administration A (mean = 7.14), r =0.032, n = 50, p = .303Correct responses Administration B (mean = 5.84), r =0.026, n = 50, p = .315These correlations are significant at a pA scatter plot summarises these results (Illustration 5).Illustration 6 demonstrates the spread of correctresponses across the 3 administrations. It is clear thatfor administrations A, B and D, correct responses aresignificantly positively correlated with Full IQ scores.Similarly, I l lustrat ion 7 demonstrates howadministrations A, B and D error scores aresignificantly negatively correlated with Full IQ.Hypothesis 3A Pearson product-moment correlation coefficient wascomputed to assess the relationship between bothPerformance IQ and Verbal IQ and Total Errors scoreand Total Correct responses. Performance IQ wassignificantly correlated with Total Correct responses, r= 0.001, n = 50, p = .457. Performance IQ was alsosignificantly correlated with Total Errors score, r =0.001, n = 50, p = -.464. Verbal IQ was alsosignificantly correlated with Totals r of Errors score, r =0.003, n = 50, p = -.417. These relationships aresignificant at a level of pIn Illustration 8, the relationships are demonstratedfurther through the gradient of the regression lines.Again the spread of Total Correct responses is moreevenly spread in comparison to Total Error scores forboth VIQ and PIQ. For PIQ the regression linesappear more closely related (Illustration 8).Hypothesis 4A Pearson product-moment correlation coefficient wascomputed to assess the relationship between Anxietyand Depression scores on the HADS and TotalCorrect responses, and Total Errors score on theBVRT. No significant correlations were found betweenAnxiety and Correct response score, r = 0.434, n = 50,p = -0.113, or between Anxiety and Errors score, r =0.435, n = 50, p = .113. No significant correlationswere found between Depression and Total Correctresponses, r = 0.112, n = 50, p = 0.228, or betweenDepression and Total Errors score, r = 0.116, n = 50, p= -.255.3 x 2 unrelated ANOVA for gender and ageA 3 x 2 unrelated ANOVA was carried out to identifyany significant effects age and gender had on correctresponses. The first IV was Age, there were 3 levels;18-20 (mean correct responses = 19.32), 21-23 (21.33)and 24-27 (21.4). The second IV was Gender which
had 2 levels; male (22.21) and female (19.61). Themain affects for Gender and Age were not significant.A 3 x 2 unrelated ANOVA was carried out to identifyany significant effects age and gender had on numberof errors made. The first IV was Age, there were 3levels; 18-20 (mean error score = 18.84), 21-23 (15.06)and 24-27 (14.30). The second IV was Gender whichhad 2 levels; male (11.78) and female (18.75). Themain effects for Age were not significant. However themain effects for Gender were significant; F(1,50) =4.178, P< 0.05 (P=0.047).Although a significant difference has been found, thesample collected only represented 14 males comparedto 36 females. This questions the validity of thesefindings, as the sample may not represent a fairnumber of each gender.Summary BVRT resultsIllustrations 10 - 12, demonstrate the expected BVRTperformance scores for 18-30 year old individualsdepending on IQ score grouping, for eachadministration A, B and D). The way in which they aretabularised are based upon how existing Normativedata are recorded in the BVRT Manual (Benton Sivan,1992). Illustration 13 summarises FIQ, Correct andError scores of the BVRT for each participant.
Discussion
Firstly, the results obtained from the study providesupport for Hypothesis 1. There was a significantpositive correlation between IQ Score and TotalCorrect Responses on the BVRT. There was also asignificant negative correlation between IQ Score andTotal Errors score on the BVRT. By correlating theresults of the two tests in a scatter plot (Illustration 6),the strength of relationships of these significantcorrelations can be further understood. The LinearRegression line for errors shows a steeper decline incomparison to the incline in correct responses,suggesting that there may be a slightly strongerrelationship between IQ and errors made than IQ andcorrect responses. These results strongly suggest thatIQ level is in some way related to our visual perception,visual memory and visuo-constructive abilities. A lowerIQ suggests that the individual’s ability to perform wellin such tests is weaker. Based on this study,Hypothesis 1 was accepted.Hypothesis 2 predicted that IQ would be significantlycorrelated with Total Correct responses and TotalErrors made across all administrations of the BVRT.The data collected supported this Hypothesis, andpositive correlations were found between IQ and Total
WebmedCentral > Original Articles Page 8 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Correct responses for A, B and D, and negativecorrelations between IQ and Total Errors score madeon A, B and D. Illustrations 6 and 7 help to furtherunderstand the relationships identified. From the linearregression lines it is clear that all administrations havestrong relationships with IQ Level. For both Errors andCorrect Scores the line shows a steeper decline (inerrors), and more gentle incline (in correct responses)for administration B. This would suggest that theparticipants had more difficulty in reconstructingimages when they were only able to view the imagefor 5 seconds prior to drawing it. Statistical analysisrevealed that although they were still significant at alevel of pIt was expected that both Verbal IQ (VIQ) andPerformance IQ (PIQ) would be significantly correlatedwith the Total Correct responses and Total Errorsscore on the BVRT. Again, significant correlationswere found, both PIQ and VIQ was positivelycorrelated with Total Correct responses, andnegatively correlated with the Total Errors made.Illustrations 8 and 9 demonstrate the strength of therelationships through the gradient of the regressionlines. Another observation which was very interestingwas the mean average of participants VIQ’s (110.2)was much lower than the mean average of participantsPIQ’s (127.4).VIQ is assessed by 7 of the 14 subsections of theWAIS, it is indicative of an individual’s ability to workwith abstract symbols, verbal memory skills, andfluency abilities. PIQ is assessed by the other 7subsections, and is indicative of an individual’s abilityto work with concrete situations, to integrateperceptual stimuli with motor responses andvisuo-spatial ability. As visuo-spatial ability is also partof what is being assessed in the BVRT, this couldexplain the strong relationship identified. In clinicalsettings if PIQ is significantly higher than VIQ, it maybe suggestive of a learning disability, autism or mentalretardat ion, they may also have dif f icul tyunderstanding auditory directions and putting theminto practice. In the case of the current study it may bea reflection of their educational backgrounds or degreetype. On the basis of these results Hypothesis 3 wasaccepted.Finally, the strength of relationship between Anxietyand Depression Scores on the HADS and TotalCorrect responses and Total Error scores on theBVRT was tested. There were no significantcorrelations between Anxiety and Depression Scoreswith performance on the BVRT. Of the 50 participantsonly 7 were classified as above normal levels ofDepression and only 2 above Mild levels. Even lessscored above Normal levels of Anxiety, 2 were
classified as Mild and 3 Moderate. However, as theHADS was being used to gain a Cognitive Profile ofthe sample, it was the initial aim to only haveparticipants scoring in low levels of Anxiety andDepression to ensure that this did not interfere withtheir performance. Of the few that did score slightlyabove healthy levels, there was no significant effect ontheir performance on the BVRT. Based on thisevidence the Null Hypothesis was retained and theAlternative Hypothesis 4 was rejected.Although a significant difference was found betweenmales and females performance, the sample collectedonly represented 14 males compared to 36 females.This may question the validity of these findings, as thesample may not be representative of each gender andso it is not possible to further generalise this to thepopulation.When looking at the BVRT results it is clear that themost common errors that were made were DistortionErrors, these are inaccurate reproductions of a singlefigure of a design. On average participants madebetween 2 to 3 Distortion errors on administrations Aand D, for administration B the average was 3-4 errors.The second most common errors were Omission andAddition Errors, an omission error can be classified bya single figure of a Design being completely omitted orno recognisable attempt was made to reconstruct thefigure. An Addition Error in contrast would be when anadditional figure present in the reconstructed designwhich could not be scored as a Perseveration orDistortion Error.On average participants made between 1 and 2Omission errors for administration A, B and D.Misplacements and Rotations were the next mostcommonly made errors, Size and Perseverationserrors were far less common. Administration Bresulted in the least amount of correct responses andthe most amounts of errors made. Almost 100 moreerrors in total for the 50 participants were made inadministration B as compared to administration A, andover 100 in comparison to administration D. Of the 50participants, irrespective of IQ, an average of 7-8correct scores for both administrations A and D wasfound as compared to 5-6 for administration B. Thesefindings further indicate that the sample population of18 to 30 year old individuals struggled most when onlyviewing the image for a brief period of time, suggestingthat to fully absorb an image 5 seconds is notadequate.By looking at the standard deviation (SD) we can seehow the data was distributed across the samplepopulation. The data appears to be equally distributedacross Administrations for correct responses, with thelargest being 2.02 for administration D. Total Correct
WebmedCentral > Original Articles Page 9 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
responses has a standard deviation of 4.36. For Errorscores however the distribution seems more widelyspread, for administration A the SD = 3.55, for B =4.23 and D = 4.73, overall error scores had an SD of9.98. This suggests that there may be certain factorswhich influence individual’s susceptibility to errorsrather than just the administration of the test. For TotalErrors score, participants ranged from 1 (with an IQ of125) and 41(with an IQ of 95).During the study significant correlations were identifiedbetween Full Scale IQ’s and performance on theBVRT for administrations A, B and D. This addsfurther support for a vast amount of existing literatureon this relationship. Carret and colleagues (2003)carried out a study to investigate how educationallevels influence visual working memory using theBVRT on elderly individuals. They found that higherlevels of intelligence did result in better performance;these findings coincide with the data collected in thecurrent study, which demonstrates the same findingsfor a younger age group of 18 to 30 year olds.Emdad and Sondegaard (2006) looked at intelligencelevels and BVRT performance on Post TraumaticStress Disorder (PTSD) patients. They found thatdespite comparable differences in levels of intelligence,this had no significant relationship with performanceon the BVRT on the control group. However with thePSTD group, they found deficits in short term memoryand non-verbal memory, these were directly related tointelligence. Emdad and Sondegaard’s study suggestthat intelligence only influences performance if it isrelated to the specific deficits identified by BVRTperformance. Whereas the current study providesconvincing evidence to suggest that in healthy 18-30year olds, significant correlations could be foundbetween IQ and BVRT performance. The participantsused in Emdad and Sondegaard’s study were of anolder age group and only 20 control participants tookpart, this might explain the difference in findings.Ellis and colleagues (2008) found that mild anxietywas associated with better cognition, when severityincreased, performance went down. This study foundno correlation between anxiety score on the HospitalAnxiety and Depression Scale (HADS) andperformance on the BVRT. However, 45 of the 50participants in the study all scored at a normal healthylevel and no participants scored above a moderatelevel. Therefore it cannot be concluded from this studythat Anxiety levels do not influence BVRT performance.The Normative standards for clinical use ofadministration A, was based on Benton (1963) lookingat over 600 individuals mainly in and out patients of ahospital in Iowa. According to this existing data, anindividual aged between 15 and 49 with an IQ of
95-109 should obtain a correct score of 8 onadministration A and with an IQ of 110 or highershould obtain a correct score of 9. According to thedata collected in the current study, an individual withan IQ score of 110 or above should obtain a correctscore of 7 or 8.Furthermore, the existing data suggests an individualwhose IQ is between 90 and 94 will have an errorscore of 4, from 95 – 104 an error score of 3, 105 –109 an error score of 2 and 110 and above an errorscore of 1. The data in the current study has foundslightly different margins, an individual whose IQ is 95or below may have an error score of 10, between96-110 an error score of 5 or 6, and 111 or higher anerror score of between 3 and 5. The slight difference indata could be due to the existing data being quitedated, in current times people may be educated to ahigher level which might affect the correct or errorscores.The Normative standards for individuals aged 60 andyounger for administration B, according to the manual,are based on performance in administration A, minus1 point for correct scores. These data were based onthe research of Von Kerekjarto (1961). The relation forerror scores between the two administrations has notyet been reported. A similar pattern was found in thisstudy, correct scores were on average one point lessfor each IQ range. What is interesting to observe in thepresent study is that the number of errors madeincreases by a larger amount. For individuals whoseIQ’s are between 96 and 110, error score is estimatedto be 7 or 8 compared to 5 or 6 for A, and 95 andbelow, is 13 or 14 compared to 10.Data collected lead to the conclusion that normaladults aged 60 years and younger perform as well inadministration D as they do on administration A.Administration D involves a short delay of 15 secondsafter viewing an image for 10 seconds, beforeconstructing the design on paper; this meant retainingan image for a brief period of time. This wasdeveloped in order to identify participants with braindisease who would perform even normally or mildlydefective on other administrations.Vakil and colleagues (1989) found correlations of 0.54for correct scores and 0.65 for error scores and sodifferences in performance, in either direction, may beencountered. Severe impairments in the delayconditions suggest a defect in memory storagecapacity; however superior performance has not yetbeen examined. It may be that the delay conditionallows individuals time to fully construct the design intheir mind, which would be beneficial for someone whohas slowed information processing abilities. As of yet,data collected for administration D has not been
WebmedCentral > Original Articles Page 10 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
adequate for routine clinical use. The present studyproduced findings that represent a similar pattern tothat found in the existing literature, what is interestingto note is a total of 128 Distortion errors for the 50participants were made in administration A, comparedto 107 in administration D. This is a significantly lowersum suggesting the delay resulted in fewer distortionerrors, still no other significant differences were foundfor any other types of errors.Methodological issuesAccording to the Handbook of normative data forneuropsychological assessment, (Mitrushina & Boone2005, p.400) 7 key criteria were deemed to beadequate for evaluating the studies on the BVRT.These include Composition Description and AgeIntervals, Educational Levels, IQ levels, Specificationof Test Version and Data Reporting, all of which havebeen clarified and controlled for. The 7th criterion isnumber of participants. The results of the presentstudy may be restricted by the number of participantsthat were used in the sample. Although 50 participantsis considered a desirable sample size, the smaller thesample the more influenced by individual differences itmay be, therefore 50 may not be a representativedepiction of the entire population of 18 to 30 year oldindividuals.The results obtained were significant; it may bebeneficial to repeat the study on a larger sample whichmay have more validity when generalising to the largerpopulation. Also only 14 of the participants were malesand 36 were females, in addition 25 of the participantswere between 18 and 20 and the other 25 ranged from21-27. A more varied sample of ages and equallydivided sample of males and females may offer furthervalidity. The results of the present study offer furthersupport for a large amount of existing literature, and soin future research the same findings would beexpected.Another possible limitation may be that the study wascarried out on groups of 5 participants at a time.Although they were separated by partitions thepresence of others may have interfered with theirperformance on the tasks. For example, when fillingout the Hospital Anxiety and Depression ScaleQuestionnaire they may have been worried that othersmay see how they were filling it in and not have beenhonest. Also as the HADS is a self-screeningquestionnaire, this may have also meant that theiranswers were dishonest possibly due to a fellowstudent carrying out the study despite ful lconfidentiality of the data.However, research has indicated that the HADS isvalid as a screening technique for cognitive profiles.When completing the WAIS III, they may not have paid
their full attention to the task at hand, and possiblybeen discouraged if others were answering questionsmore promptly and easily. In future research wheretime constraints are not an issue, the study could becarried out on an individual basis, therefore eliminatingthe distraction of the presence of others.The study was particularly time consuming, thus mayhave lead to participants experiencing boredom andfatigue, this may have contributed to the variation insome levels of the data. This could be the cause oflarger standard deviations in some parts of the data,such as the vast range in IQ scores or Error scores onthe BVRT. Timing was an issue for both theresearcher and participants, who were all alsostudents under pressure from deadlines and vastworkloads. To spread the study over a number of dayswhen the participants are not in a time of increasedstress and workload, with distractions on their mind,this may add further validity to the study.Implications for future researchThe development of this set of normative data for thisnew age group, 18 to 30 year olds, will greatly aid inthe advance of the use of the BVRT as an instrumentin clinical fields. The BVRT can now be used on braindamaged patients or patients suffering from braindiseases within this younger age group to accuratelymeasure the extent of damage to their visualperception, visual memory and visuo-constructiveabilities.Future research can now accurately assessperformance of neuro-psychologically impairedindividuals within this new age group, suffering fromsuch disorders as Post Traumatic Stress andSchizophrenia, on the BVRT, by comparing to this newset of normative data. This can then be used forcomparison against that of existing literature on otherage groups to see how age may affect the extent ofimpairment of these cognitive skills. In addition,individuals with learning disabilities and ADHD cannow be assessed to investigate the possibilities ofprogress or decline with age into early adulthood, nowthat a set of normative data exists for this age range.
Conclusion
In conclusion to this study a new set of NormativeData has been collected for the new age group of 18 –30 year olds. With this development in BVRT research,clinical applications can benefit from these findingswhen looking at patient’s with brain damage or thosesuffering from a brain disease within this age group.The findings are consistent with the normativestandards stated in the BVRT fifth edition manual for
WebmedCentral > Original Articles Page 11 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
older age groups in that a significant relationship wasfound between BVRT performance and IQ levels.Higher IQ levels are associated with betterperformance on the BVRT, suggesting that the moreintellectually advanced an individual, the moreenhanced their visual perception, visual memory andvisuo-constructive abilities. These new findingsprovide reliable data which can be used to assess thecognitive abilities of the younger age group (18-30year olds), they also suggest that performance on theBVRT may be slightly different to that suggested inprevious research. This may be because the existingdata is slightly outdated, changes may have occurred,which have influenced cognitive processing, also inthe current study only a small cohort of people tookpart with a low male to female ratio.In addition to existing research, the findings of thisstudy can now be applied in new settings. Thisyounger age group (18-30 year olds) are one of themost likely to sustain brain injury. Also, Post traumaticstress disorder (PTSD), and symptoms of manymental psychiatric disorders often begin to appearwithin this age range. By using the BVRT as aninstrument to measure their performance on cognitivetasks, new research can discover the impact of suchtraumas on this younger age group. Finally this newset of normative data provides support to currentresearch that IQ level is a strong indicator of BVRTperformance; this aids the interpretation of results forneuro-psychologically impaired individuals.
References
1. Amieva, H., Jacqmin-Gadda, H., Orgogozo, J., LeCar re t , N . , He lmer , C . , Le tennuer , L . ,Berberger-Gateau, P., Fabrigoule, C. & Dartiques, J.,2005. The 9 year cognitive decline before dementia ofthe Alzheimer’s type: A prospective population-basedstudy. Brain A journal of Neurology, 133(2), 1-9.2. Arenberg, D., 1978. Differences and changes withage in the Benton Visual Retention Test. Journal ofGerontology, 33, 534-540. Available from:http://geronj.oxfordjournals.org/content/33/4/534.full.pdf+html [Accessed on November 1st 2009]3. Baum, C., Edwards, D., Yonan, C., & Storandt, M.,1996. The relation of neuropsychological testperformance to performance of functional tasks indementia of the Alzheimer type. Archives of ClinicalNeuropsychology, 11(1),69-75.4. Benton, A. L., 1946. A visual retention test forclinical use. New York: The Psychological Corporation.5. Benton, A. L., 1955. Revised Visual Retention Test:Clinical and experimental applications. Iowa City:
State University of Iowa.6. Benton, A. L., 1963. Revised Visual Retention Test:Clinical and experimental applications (3rd ed.). NewYork: The Psychological Corporation.7. Benton, A.L., 1974. Revised Visual Retention Test:Clinical and experimental applications (4th ed.). SanAntonio, TX: The Psychological Corporation.8. Benton, A.L., Eslinger, P. J., & Damasio, A. R.,1981. Normative observations on neuropsychologicaltest performances in old age. Journal of clinicalNeuropsychology, 3, 33-42.9. Benton Sivan, A., 1992. Benton Visual RetentionTest. 5th ed. San Antonio: The PsychologicalCorporation.10. Binet, A., & Simon, TH., 1908. Le development del’intelligence chez les enfants [The development ofintelligence in children]. L’Annee Psychologique, 14,1-94.11. Birch, L. S., & Davidson, K. M., 2007. Specificity ofautobiographical memory in depressed older adultsand its relationship with working memory and IQ.British Journal of Clinical Psychology, 46(2), 175-186.12. Crookes, T. G., & McDonald, K. G., 1972. Benton’sVisual Retention Test in differentiation of depressionand early dementia. American Journal of MentalDeficiency, 72, 96-99.13. Dige, N., & Maarh, E., 2008. Memory tests insubgroups of adult attention deficit hyperactivityreveals simultaneous capacity deficit. Intern. J.Neuroscience 118: 569-591. Informa Healthcare USA,Inc.14. Ellis, J. M., Comijs, H., Rijmen, F., Jonker, C., &Beekman, A. F., 2008. Anxiety symptoms andcognitive performance in later life: Results from thelongitudinal aging study Amsterdam. Aging and MentalHealt, 12(4), 517-52315. Emdad, R., & Sondergaard, H.P. 2006. GeneralIntelligence and short-term memory impairments inPost Traumatic Stress Disorder patients. Journal ofMental Health, 15(2), 205-216.16. Eysenck, M. W., 1997. Anxiety and Cognition: AUnified Theory. East Sussex : Psycholgy Press Ltd.17. Fay, L., 2010. Alzheimer’s Disease Facts andFigures 2010. Brain Fitness for Life. Available from:http://www.brainfitnessforlife.com/alzheimers/alzheimers-disease-2010-facts-figures/ Accessed: 30.01.2010.18. Le Carret, N., Rainville, C., Lechevallier, N., Lafont,S., Letenneur, L., & Fabrigoule, C., 2003. Influence ofeducation on the Benton Visual Retention Testperformance as mediated by a strategic searchcomponent. Brain and Cognition, 53(2), 408-411.19. Leon, M. J., 2001. Prediction of cognitive decline innormal elderly subjects. The National Academy ofSciences, 98(19), 10966–10971.
WebmedCentral > Original Articles Page 12 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
20. Lezak, M. D., 1983. Neuropsychologicalassessment (2nd ed.) New York: Oxford UniversityPress.21. Marsh, G. G., & Hirsch, S. H., 2006. Effectivenessof two tests of visual retention. Journal of ClinicalPsychology, 38, 115-118.22. 1989. Changes in the performance of parkinsonianpatients and normal aged on the Benton VisualRetention Test. Exp Aging, Res, 15(1-2),13-823. Park, J. J., 2008. Pattern of Performance on theBenton Visual Retention Test in Schizophrenicpatients diagnosed with research diagnostic criteria.Dissertation Abstracts International: Section B: TheSciences and Engineering, 68(10-B), 6976.24. Parkinson’s Disease Society, 2010. London:Parkinson's Disease Society of the United Kingdom.A v a i l a b l e f r o m :http://www.parkinsons.org.uk/default.aspx Accessed:30.01.2010.25. Petris, L., 1981. Il Visual Retention Testnell’Esame della Conoscenza Visiva. Firenze:Organizzazioni Speciali.26. Poitrenaud, J., & Clement, F., 1965. Ladeterioration physiologique dans le Test de RetentionVisuelle de Benton: Resultats obtenus par 500 sujetsnormaux. Psychologie Francaise, 10, 359-368.27. Robinson-Wheelen, S., 1992. Benton VisualRetention Test performance among normal anddemented older adults. Neuropsychology, 6(3), 1992,261-269.28. Seo, E. H., Lee, D. Y., Choo, I. H., Youn J. C., KimK. W., Jhoo, J. H., Suh, K. W., Paek, Y. S., Jun, Y. H.& Woo, J. I., 2007. Performance on the Benton Visualretention Test in an Educationally Diverse ElderlyPopulation. The Journals of Gerontology Series B:Psychological sciences and Social Sciences, 62,191-193.29. Snaith, R.P., & Zigmond, A.S. 1983. 1992. 1994.Hospital Anxiety and Depression Scale (HADS). ACTAPsychiatrica Scandanavica, 67, 361 – 370. NelsonPublishing Company Ltd. London.30. Thompson, S.B.N., 2000. The Central ExecutiveSystem in people with Down’s syndrome anddementia. Clinical Gerontologist, 21(3), 3-32.31. Thompson, S.B.N., 2001. Assessing dementia inDown’s syndrome: a comparison offive tests. Clinical Gerontologist, 23(3/4), 3-19.32. Thompson, S.B.N. MacDonald. J., & Coates, T.D.2001. Improving Visual Memory with Aricept(Donepezil Hydrochloride, E2020) in Mild-to-ModerateAlzheimer’s disease. Clinical Gerontologist, 24(1/2),55-73.33. Thompson, S.B.N., 2002. Memory decline,Alzheimer’s disease and vascular dementia: the
clinical picture. The Journal of Cognitive Rehabilitation,20(2), 12-18.34. Thompson, S.B.N., 2006. Dementia and memory:a handbook for students and professionals. Aldershot:Ashgate.35. Thompson, S.B.N., Ennis, E., Coffin, T., & Farman,S., 2007. Design and evaluation of a computerisedversion of the Benton Visual Retention Test.Computers in Human Behavior, 23, 2383-2393.36. Thompson, S.B.N., 2010. Advancing knowledgeinto the clinical assessment of dementia. PhD, Schoolof Design, Engineering & Computing, Department ofPsychology, Bournemouth University.37. Thompson, S.B.N., 2011 Psychology of trauma:clinical reviews, case histories, research. Portsmouth:Blackwell-Harvard-Academic.38. Vilkki, J., 1989. Perseveration in memory forfigures after frontal lobe lesion. Neuropsychologia, 27,1101-1104.39. Wechsler, D., 1939. Weschler-BellevueIntelligence Scale. New York: The PsychologicalCorporation.40. Wechsler, D., 2002. WAIS-III. WMS-III. TechnicalManual. New York: The Psychological Corporation.41. Weems., C.F., Costa, N.M., Watts, S.E., Taylor,L.K., & Cannon, M.F., 2007. Cognitive errors, anxietysensitivity, and anxiety control beliefs: their unique andspecific associations with childhood anxiety symptoms.Behaviour Modification, 31(2), 174-201.
WebmedCentral > Original Articles Page 13 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
NoAge
Sex PIQ VIQ FIQ
HADSDepression
HADSAnxiety
BVRTCorr-A
BVRTCorr-B
BVRTCorr-D
BVRTErr-Total
BVRTErr-A
BVRTErr-B
BVRTErr-D
BVRTErr-Total
1 19 M 130 122 128 8 1 9 8 7 24 1 1 6 82 20 F 146 123 136 2 0 9 8 8 25 1 4 2 73 19 F 105 106 100 8 2 7 6 0 13 9 7 0 164 21 F 130 104 116 9 2 8 6 10 24 3 6 0 95 21 F 117 99 107 4 0 8 7 7 22 4 8 6 186 20 F 109 112 111 6 2 9 6 7 22 9 5 4 187 20 F 113 102 107 11 4 6 6 6 18 11 7 7 258 25 F 138 140 144 4 0 8 6 7 21 2 5 3 109 26 M 128 119 126 7 3 8 7 6 21 2 4 6 1210 21 F 110 99 104 0 0 4 3 6 13 11 16 9 3611 22 F 142 114 128 5 2 8 5 8 21 4 12 4 2012 18 F 144 102 120 2 0 10 5 7 22 0 6 6 1213 20 F 121 89 102 3 4 7 5 6 18 6 9 4 1914 21 M 155 127 147 10 5 7 7 8 22 4 3 4 1115 21 F 109 106 108 8 3 8 8 10 26 3 2 0 516 22 F 119 102 110 3 0 10 7 9 26 0 4 1 517 21 F 113 122 120 7 2 8 6 9 23 3 4 1 818 21 F 146 123 136 6 0 9 9 8 26 2 2 2 619 20 F 109 114 112 6 3 10 7 7 24 0 7 7 1420 24 M 130 95 110 2 2 8 5 9 22 4 13 3 2021 26 F 132 123 130 4 1 7 3 5 15 5 13 18 3622 19 F 130 100 113 3 1 5 4 7 16 7 12 5 2423 27 M 155 122 149 0 3 9 7 6 22 2 4 4 1024 25 F 125 100 111 3 0 4 6 10 20 8 5 0 1325 26 M 153 133 145 1 3 9 8 10 27 3 2 0 526 27 M 155 151 155 6 2 7 9 9 25 5 2 1 827 22 F 130 114 122 2 7 6 4 8 18 7 8 2 1728 20 F 146 112 128 2 2 8 6 10 24 2 5 0 729 21 F 155 107 130 3 12 6 4 8 18 7 10 2 1930 18 M 150 140 149 1 3 6 6 9 21 6 4 2 1231 26 F 136 125 134 0 11 8 4 8 20 2 10 3 1532 27 F 132 107 119 3 11 8 4 9 21 3 10 1 1433 19 M 117 107 112 1 5 7 7 6 20 6 4 5 1534 19 F 142 107 122 6 6 8 10 10 28 3 0 0 335 22 M 155 102 125 6 11 9 10 10 29 1 0 0 136 18 F 146 92 113 14 7 7 4 10 21 5 9 0 1437 20 F 146 115 130 1 4 6 4 9 19 9 13 1 2338 19 M 107 114 112 0 2 8 6 6 20 2 8 5 1539 20 M 109 97 102 4 4 9 4 6 19 1 8 3 1240 19 F 138 96 113 6 5 5 3 7 15 16 14 7 3741 19 M 119 110 114 0 4 8 6 8 22 3 6 10 1942 18 F 125 100 111 3 7 6 5 8 19 6 7 6 1943 23 F 105 93 98 1 9 5 6 3 14 9 8 18 3544 19 F 91 91 90 2 4 3 2 6 11 11 20 9 4045 20 F 90 91 90 3 5 6 6 6 18 7 8 10 2546 19 F 98 93 95 3 8 4 3 4 11 12 12 17 4147 19 F 117 112 115 0 2 3 4 4 11 8 9 16 3348 18 F 105 97 100 1 7 7 7 8 22 5 5 3 1349 22 F 104 106 105 2 7 7 8 6 21 6 3 10 1950 23 M 144 133 142 0 6 5 5 7 17 7 6 4 17
Illustrations
Illustration 1
WAIS III, HADS and BVRT scores
WebmedCentral > Original Articles Page 14 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
BVCoA
BVCoB
BVCoD
BVCoTot
BVErA
BVErB
BVErD
BVErTo
DisC
DisD
DisE
OmC
OmD
OmE
PD
PE
SzC
SzD
SzE
RoC
RoD
RoE
MC
MD
M E
9 8 7 24 1 1 6 8 0 0 1 0 0 0 0 0 1 0 3 0 0 1 0 1 1
9 8 8 25 1 4 2 7 0 3 1 0 0 0 0 0 0 0 0 0 0 0 1 1 1
7 6 0 13 9 7 0 16 3 2 0 4 1 0 0 0 0 0 0 0 0 0 2 4 08 6 10 24 3 6 0 9 2 1 0 0 0 0 0 0 0 0 0 0 1 0 1 4 08 7 7 22 4 8 6 18 2 3 4 0 0 0 0 0 0 2 0 0 1 0 2 2 2
9 6 7 22 9 5 4 18 2 3 4 2 1 0 0 0 1 0 0 0 0 0 0 1 0
6 6 6 18 11 7 7 25 7 5 3 2 0 0 1 1 0 0 0 1 0 1 1 1 2
8 6 7 21 2 5 3 10 2 3 0 0 0 0 0 0 0 0 0 0 0 0 0 2 3
8 7 6 21 2 4 6 12 1 3 1 1 0 0 0 0 0 0 1 0 0 0 0 1 4
4 3 6 13 11 16 9 36 5 8 1 3 5 2 0 0 2 0 3 0 0 2 1 3 18 5 8 21 4 12 4 20 1 3 3 1 7 0 0 0 0 0 0 0 0 0 2 2 1
10 5 7 22 0 6 6 12 0 2 2 0 1 3 0 0 0 0 0 0 2 1 0 1 07 5 6 18 6 9 4 19 4 6 1 1 1 0 0 0 0 0 0 1 0 2 0 2 17 7 8 22 4 3 4 11 2 1 0 2 1 3 0 0 0 0 0 0 0 1 0 1 08 8 10 26 3 2 0 5 2 1 0 0 0 0 0 0 0 0 0 0 1 0 1 0 0
10 7 9 26 0 4 1 5 0 2 0 0 0 0 0 0 0 0 0 0 0 0 0 2 1
8 6 9 23 3 4 1 8 2 2 1 0 2 0 0 0 0 0 0 1 0 0 0 0 0
9 9 8 26 2 2 2 6 0 2 0 0 0 0 0 0 1 0 0 0 0 0 1 1 2
10 7 7 24 0 7 7 14 0 3 2 0 1 4 0 0 0 1 0 0 1 0 0 1 1
8 5 9 22 4 13 3 20 2 4 3 0 0 0 1 0 0 0 0 2 2 0 0 6 07 3 5 15 5 13 18 36 2 6 9 1 3 5 0 0 0 0 1 0 2 1 1 2 25 4 7 16 7 12 5 24 2 6 3 0 2 0 0 0 0 0 0 4 1 0 1 3 29 7 6 22 2 4 4 10 1 1 3 1 0 0 0 0 0 0 0 0 1 0 0 2 14 6 10 20 8 5 0 13 5 3 0 0 0 0 1 0 0 0 0 1 1 0 2 0 09 8 10 27 3 2 0 5 2 1 0 0 0 0 0 0 0 0 0 1 0 0 0 1 0
7 9 9 25 5 2 1 8 3 1 1 1 0 0 0 0 0 0 0 1 0 0 0 1 0
6 4 8 18 7 8 2 17 5 5 2 1 2 0 0 0 0 1 0 1 0 0 0 0 0
8 6 10 24 2 5 0 7 1 1 0 1 3 0 0 0 0 0 0 0 1 0 0 0 0
6 4 8 18 7 10 2 19 4 5 1 0 2 1 0 0 0 0 0 2 3 0 1 0 0
6 6 9 21 6 4 2 12 3 1 1 2 0 1 2 0 0 0 0 1 1 0 0 0 08 4 8 20 2 10 3 15 0 3 2 1 2 1 0 0 0 0 0 1 3 0 0 2 08 4 9 21 3 10 1 14 1 5 1 2 1 0 0 0 0 0 1 0 0 0 3 07 7 6 20 6 4 5 15 3 1 1 1 1 0 0 0 0 1 1 1 1 1 1 0 28 10 10 28 3 0 0 3 2 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 09 10 10 29 1 0 0 1 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0
7 4 10 21 5 9 0 14 4 6 0 0 0 0 0 0 0 0 0 0 1 0 1 2 0
6 4 9 19 9 13 1 23 6 6 1 0 0 0 0 0 0 0 0 2 2 0 1 5 0
8 6 6 20 2 8 5 15 0 4 2 1 4 0 0 1 0 0 0 0 0 1 1 0 1
9 4 6 19 1 8 3 12 0 3 2 1 1 0 1 0 0 0 0 0 2 1 0 1 0
5 3 7 15 16 14 7 37 7 8 4 9 3 1 1 0 0 0 0 0 1 0 0 1 28 6 8 22 3 6 10 19 2 1 4 0 3 0 0 0 0 0 2 0 2 0 1 0 46 5 8 19 6 7 6 19 4 4 2 1 2 4 0 0 0 0 0 1 1 0 0 0 05 6 3 14 9 8 18 35 6 2 8 0 4 8 0 0 0 0 0 2 1 0 1 1 23 2 6 11 11 20 9 40 5 7 5 4 11 3 1 0 0 0 0 0 0 0 2 1 16 6 6 18 7 8 10 25 4 4 6 1 1 1 0 0 0 0 1 1 0 1 1 3 1
4 3 4 11 12 12 17 41 7 6 10 3 5 3 0 0 0 0 1 2 0 2 0 1 1
3 4 4 11 8 9 16 33 3 4 6 1 2 5 0 0 1 0 1 1 0 1 2 3 3
7 7 8 22 5 5 3 13 4 2 0 1 0 1 0 0 0 0 1 0 1 0 0 2 1
7 8 6 21 6 3 10 19 2 2 6 2 1 1 0 0 0 0 1 2 0 2 0 0 0
5 5 7 17 7 6 4 17 3 4 1 0 1 1 0 0 0 0 0 3 0 1 1 1 1 7.1
4 5.84 7.36 20.34 5.06 7 4.74 16.8 2.6 3.2 2.2 1 1.5 1.1 0.2 0 0.1 0.1 0.3 0.7 0.7 0.4 0.6 1.4 0.9
357 292 368 778 253 350 237 492 128 159 107 50 75 49 8 2 7 5 16 35 33 19 29 71 44
Illustration 2
Means and totals for BVRT correct, error and visuospatial scores
WebmedCentral > Original Articles Page 15 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
N 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
RawRaw
RawRaw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw Raw
PC 16 15 10 19 18 8 18 17 14 13 19 11 11 24 10 15 10 17 13 15 19 16 22 17 19
DS 58 75 57 64 72 68 47 75 58 93 92 94 64 102 65 72 87 70 61 67 59 70 63 57 53
S 24 24 25 17 15 14 22 29 24 17 22 23 14 23 25 19 23 27 17 13 23 12 23 17 27
Bl 55 59 44 55 33 38 49 55 56 42 53 53 59 62 50 37 44 54 45 53 56 46 65 54 64
Ar 14 18 14 14 13 17 12 18 19 10 18 13 9 19 15 11 19 16 15 8 19 15 20 17 18
Mat 21 22 18 21 20 20 14 22 19 16 19 19 19 13 18 22 16 24 17 17 21 21 23 23 25
DSp 20 20 16 18 17 19 9 26 14 16 12 14 14 24 11 16 18 14 20 12 12 16 15 16 25
Inf 22 20 13 12 8 18 18 18 15 13 21 14 8 17 16 12 18 20 21 19 24 11 23 12 18
PA 19 19 10 16 12 13 15 18 20 4 17 20 16 17 10 13 10 19 12 19 15 19 22 12 17
Co 18 17 16 17 18 17 16 25 26 17 18 13 13 18 16 19 21 25 17 18 27 18 22 13 23
Sum 267 289 223 253 226 232 220303
265
241 291
274 227 319 236 236 266 286 238 241 275 244 298 238 289
PVIQ 122 123 106 104 99 112 102140
119 99 114
102 89 127 106 102 122 123 114 95 123 100 122 100 133
PPIQ 130 146 105 130 117 109 113138
128
110 142
144 121 155 109 119 113 146 109 130 132 130 155 125 153
PFIQ 128 136 100 116 107 111 107144
126
104 128
120 102 147 108 110 120 136 112 110 130 113 149 111 145
Illustration 3
WAIS III raw scores
WebmedCentral > Original Articles Page 16 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
Raw
22 18 13 19 17 19 17 13 21 9 19 18 8 8 11 12 13 15 11 5 14 11 6 11 20
76 53 77 75 72 71 50 50 66 83 67 65 64 60 72 58 71 79 74 69 42 69 73 55 63
28 22 23 18 25 26 25 26 18 17 16 21 17 13 16 18 13 13 15 9 17 20 17 19 31
64 55 59 49 63 50 56 51 59 64 62 49 25 40 57 50 38 13 28 36 33 44 45 29 61
16 18 16 17 19 18 17 11 18 16 7 18 17 16 12 18 14 6 6 11 10 14 13 12 16
24 19 23 20 24 17 22 19 20 21 17 25 17 20 18 20 20 11 7 10 11 12 7 17 21
23 16 13 16 24 16 13 18 15 16 16 17 19 12 13 18 17 14 10 16 17 21 16 16 19
26 11 18 11 22 20 19 16 12 17 14 20 21 16 15 18 17 18 18 8 11 13 10 16 21
22 19 19 17 18 20 19 18 15 21 21 19 18 13 21 17 20 18 11 8 17 20 18 17 18
32 22 20 20 24 25 14 13 19 9 12 15 14 12 33 10 10 19 17 17 9 18 13 18 21
333 253 281 262 308 282 252 235 263 273 251 267 220 210 268 239 233 206 197 189 181 242 218 210 291
151 114 112 107 140 125 107 107 107 102 92 115 114 97 96 110 100 93 91 91 95 112 97 106 133
155 130 146 155 150 136 132 117 142 155 146 146 107 109 138 119 125 105 91 90 98 117 105 104 144
155 122 128 130 149 134 119 112 122 125 113 130 112 102 113 114 111 98 90 90 93 115 100 105 142
Illustration 4
WAIS III raw scores (continued)
WebmedCentral > Original Articles Page 17 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Illustration 5
Relationship between BVRT scores and WAIS III FIQ
WebmedCentral > Original Articles Page 18 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Illustration 6
Relationship between BVRT errors scores across administrations A, B, D and WAIS III FIQ
WebmedCentral > Original Articles Page 19 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Illustration 7
Relationship between BVRT correct scores across administrations A, B, D and WAIS III FIQ
WebmedCentral > Original Articles Page 20 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Illustration 8
Relationship between BVRT scores and WAIS III VIQ
WebmedCentral > Original Articles Page 21 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Illustration 9
Relationship between BVRT scores and WAIS III PIQ
WebmedCentral > Original Articles Page 22 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Administration A Aged 18 – 30 Years of Age
Estimated IQ ScoreEstimated Number
Correct Score
Estimated Number
Error Score
141 and above 7-8 4-5
126 - 140 7-8 3-4
111 - 125 7-8 5
96 - 110 7-8 5-6
95 and below 4-5 10
Illustration 10
Expected BVRT scores for administration A derived from estimated IQ
WebmedCentral > Original Articles Page 23 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Administration B Aged 18 – 30 Years of Age
Estimated IQ ScoreEstimated Number
Correct Score
Estimated Number
Error Score
141 and above 6-7 3-4
126 - 140 5-6 7-8
111 - 125 5-6 6-7
96 - 110 6 7-8
95 and below 3-4 13-14
Illustration 11
Expected BVRT scores for administration B drived from estimated IQ
WebmedCentral > Original Articles Page 24 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
Administration D Aged 18 – 30 Years of Age
Estimated IQ ScoreEstimated Number
Correct Score
Estimated Number
Error Score
141 and above 8 2-3
126 - 140 7-8 4-5
111 - 125 7-8 4-5
96 - 110 6-7 5-6
95 and below 5-6 12
Illustration 12
Expected BVRT scores for administration D derived from estimated IQ
WebmedCentral > Original Articles Page 25 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
FIQ
Correct Responses Error scores
A B D A B D P Number90 3 2 6 11 20 9 44
90 6 6 6 7 8 10 4595 4 3 4 12 12 17 46
Average 4.333333 3.666667 5.333333 10 13.33333 1298 5 6 3 9 8 18 43100 7 6 0 9 7 0 3100 7 7 8 5 5 3 48102 7 5 6 6 9 4 13102 9 4 6 1 8 3 39
104 4 3 6 11 16 9 10105 7 8 6 6 3 10 49107 8 7 7 4 8 6 5
107 6 6 6 11 7 7 7
108 8 8 10 3 2 0 15110 10 7 9 0 4 1 16110 8 5 9 4 13 3 20
Average 7.166667 6 6.333333 5.75 7.5 5.333333111 9 6 7 9 5 4 6
111 4 6 10 8 5 0 24111 6 5 8 6 7 6 42112 10 7 7 0 7 7 19112 7 7 6 6 4 5 33
112 8 6 6 2 8 5 38
113 5 4 7 7 12 5 22113 7 4 10 5 9 0 36113 5 3 7 16 14 7 40114 8 6 8 3 6 10 41
115 3 4 4 8 9 16 47116 8 6 10 3 6 0 4119 8 4 9 3 10 1 32120 10 5 7 0 6 6 12
120 8 6 9 3 4 1 17122 6 4 8 7 8 2 27122 8 10 10 3 0 0 34125 9 10 10 1 0 0 35
Average 7.166667 5.722222 7.944444 5 6.666667 4.166667
126 8 7 6 2 4 6 9128 9 8 7 1 1 6 1128 8 5 8 4 12 4 11
128 8 6 10 2 5 0 28130 7 3 5 5 13 18 21130 6 4 8 7 10 2 29130 6 4 9 9 13 1 37
134 8 4 8 2 10 3 31
136 9 8 8 1 4 2 2
136 9 9 8 2 2 2 18Average 7.8 5.8 7.7 3.5 7.4 4.4
142 5 5 7 7 6 4 50144 8 6 7 2 5 3 8
145 9 8 10 3 2 0 25
147 7 7 8 4 3 4 14149 9 7 6 2 4 4 23149 6 6 9 6 4 2 30155 7 9 9 5 2 1 26
Average 7.285714 6.857143 8 4.142857 3.714286 2.571429
Illustration 13
FIQ and BVRT scores across all participants
WebmedCentral > Original Articles Page 26 of 27

WMC001652 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 10:01:46 AM
DisclaimerThis article has been downloaded from WebmedCentral. With our unique author driven post publication peerreview, contents posted on this web portal do not undergo any prepublication peer or editorial review. It iscompletely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscriptbut also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions beforesubmitting any information that requires obtaining a consent or approval from a third party. Authors should alsoensure not to submit any information which they do not have the copyright of or of which they have transferredthe copyrights to a third party.
Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater tothe needs of an individual patient. The web portal or any content(s) therein is neither designed to support, norreplace, the relationship that exists between a patient/site visitor and his/her physician. Your use of theWebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harmthat you may suffer or inflict on a third person by following the contents of this website.
WebmedCentral > Original Articles Page 27 of 27