Embed Size (px)
Citation preview
Journal of Investigative Surgery, 20:237–241, 2007Copyright ©c Informa Healthcare USA, Inc.ISSN: 0894-1939 print / 1521-0553 onlineDOI: 10.1080/08941930701481296
ORIGINAL RESEARCH
Immune Response to Small IntestinalSubmucosa (Surgisis) Implant in Humans:
Preliminary ObservationsLuca Ansaloni, MD, PaoloCambrini, MD, Fausto Catena,MD, Salomone Di Saverio, MD,Stefano Gagliardi, MD, FilippoGazzotti, MDUnit of General Surgery, Universityof Bologna, Sant’Orsola-MalpighiHospital, Bologna, Italy
Jason P. Hodde, MSCook Biotech Incorporated, WestLafayette, Indiana, USA
Dennis W. Metzger, PhDCenter for Immunology andMicrobial Disease, Albany MedicalCollege, Albany, New York, USA
Luigi D’Alessandro, MD, andAntonio Daniele Pinna, MDUnit of General Surgery, Universityof Bologna, Sant’Orsola-MalpighiHospital, Bologna, Italy
ABSTRACT Surgisis IHM is an acellular biomaterial derived from porcinesmall intestinal submucosa (SIS) that induces site-specific remodeling in theorgan or tissue into which it is placed. Previous animal studies have shownthat the graft recipient mounts a helper T type 2-restricted immune responseto the SIS xenograft without signs of rejection. The aims of this study were toevaluate the immune response to the SIS implant in a small series of humans andto examine the long-term clinical acceptance of the xenograft in these patients.Five consecutive male patients (mean age 56 years, range 34–68) who underwentinguinal hernioplasty with Surgisis IHM were assessed at 2 weeks, 6 weeks, and 6months after implant for SIS-specific, α-1,3-galactose (α-gal) epitope and type Icollagen specific antibodies. All five patients were also clinically assessed up to 2years for signs of clinical rejection, hernia recurrence, and other complications.All 5 patients implanted with Surgisis IHM produced antibodies specific for SISand α-gal with a peak between 2 and 6 weeks after implantation. By 6 months, allpatients showed decreasing levels of anti-SIS antibodies. Two patients developeda transient, mild local seroma that resolved spontaneously. None of the patientsshowed any clinical signs of rejection, wound infection, hernia recurrence, orother complications in the follow-up out to 2 years. Thus, this study showedthat in a small series of patients the SIS elicits an antibody response withoutclinical rejection of the xenograft and minimal postoperative complications.
KEYWORDS body wall, collagen, galactosyl-α(1,3)galactose epitope, extracellular matrix,inguinal hernioplasty, small intestinal submucosa
Surgisis IHM (Cook Biotech Inc., West Lafayette, IN) is an acellular extracel-lular matrix (ECM) biomaterial derived from porcine small intestinal sub-mucosa (SIS), which has been used extensively for repair of tendons and
ligaments, urinary bladder wall, dura mater, abdominal wall, and other tissues.When implanted, SIS appears to induce site-specific remodeling in the organ ortissue into which it is placed. It is currently approved and marketed for humanuse. SIS contains several types of collagen, glycoproteins (fibronectin, heparan
Address correspondence to Dr. LucaAnsaloni, Unit of General Surgery,University of Bologna,Sant’Orsola-Malpighi Hospital, ViaMassarenti 9, 40138, Bologna, Italy.(e-mail: [email protected]).
237
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mon
trea
l on
12/0
1/14
For
pers
onal
use
onl
y.

sulfate proteoglycan), glycosaminoglycans (hyaluronicacid, heparin, heparan sulfate, chondroitin sulfate Aand C, dermatan sulfate), and growth factors (ba-sic fibroblast growth factor-2 [FGF-2], transforminggrowth factor-β [TGF-β], vascular endothelial growthfactor [VEGF]) [1]. SIS also contains the galactosyl-α(1,3)galactose (Galα1–3Galβ1-(3)4GlcNAc-R) epi-tope, which in humans is a major cause of hyperacuterejection of porcine xenografts due to preexisting “natu-ral” antibodies [2]. Animal studies have shown that ani-mal recipients of SIS grafts mount an immune responseto the xenograft without signs of rejection [3,4].Theaims of this study were to evaluate the immune responseto SIS implant in a small sample of humans and to ex-amine in the long term the clinical acceptance of thegraft.
MATERIALS AND METHODSPatients
Five consecutive male patients (mean: 56 years;range: 34–68 years) gave consent from a larger ethicscommittee-approved, randomized clinical trial involv-ing elective inguinal hernioplasty with Surgisis IHM[5] to provide blood samples for this investigation.Blood was collected at baseline, 2 weeks, 6 weeks, and6 months after implant and the serum was analyzed forα-1,3-galactose (α-gal)-specific, SIS-specific, and type Icollagen-specific antibodies. All five patients were alsoclinically assessed every 6 months up to 2 years for signsof clinical rejection (tissue necrosis, erythema, pain),hernia recurrence, and other complications.
Preparation of Tris Extract of SurgisisSurgisis was frozen at –80◦C and was pulverized un-
der liquid nitrogen to a fine particulate using a grindingmill. Fifty grams of powder was extracted for 24 h at 4◦Cin 500 mL of phophate-buffered saline (PBS) containing50 mM Tris-HCl (pH 7.4) and containing 10 mM N -ethylmaleimide, 1 mM phenylmethylsulfonyl fluoride(PMSF), and 5 mM benzamidine. The mixture was cen-trifuged at 12,000 × g and 4◦C for 20 min. Supernatantswere recovered; solid was discarded. Supernatants weredialyzed (MWCO 3000) extensively against deionizedwater (10 exchanges of 3 L each). Following dialysis, thesupernatants were frozen at –80◦C and lyophilized.
ELISA for Determination of α-gal-and SIS-Specific Antibodies
The ELISA technique for detecting α-gal-specific an-tibodies was a modification of the procedure reportedby Yang et al. [6] and previously reported by our group[4]. For the detection of SIS-reactive antibodies, theplates were coated at 4◦C overnight with 10 μg/mL ofTris extract in PBS from Surgisis (50 μl/well) and thentreated as described previously [4]. To ensure that allassays were functioning properly, pooled serum fromBALB/c mice immunized with 50 μg Tris extract of Sur-gisis in complete Freund’s adjuvant followed 28 dayslater by a booster injection of 50 μg Tris extract inincomplete Freund’s adjuvant was used as a positivecontrol, and preimmune serum from implanted micewas included as a negative control [3]. The results pre-sented are representative of at least two independentlyperformed assays.
ELISA for Collagen-ReactiveAntibodies
Immulon 2HB plates were coated with 5 μg/mLof porcine type I collagen (CI) and incubated at4◦C overnight. Plates were washed 3 times with0.05% Tween and blocked at 37◦C for 3 h with100 μL/well of 1% gelatin. A 1:20 serial dilution ofserum was added and incubated at 4◦C overnight.Plates were washed, and 50 μL/well of anti-mouse al-kaline phosphatase-conjugated total immunoglobulin(Ig) was added (Southern Biotech). Plates were incu-bated at 37◦C for 2 h, washed, and 50 μL/well of phos-phatase substrate was added for color development. Ab-sorbances were read at 405 nm.
Statistical AnalysisDescriptive statistics are expressed as means (SD),
and to compare preoperative and postoperative meansa paired-samples T -test was used. A p value < .05 wasconsidered to be statistically significant. The analyseswere done with SPSS version 13.0 (SPSS, Chicago).
RESULTSAll patients implanted with Surgisis IHM produced
antibodies specific for SIS (Figure 1). Patients 1 and 3had the highest antibody production in response to SISat 2 weeks after implantation, while patients 2, 4, and5 illustrated a peak of SIS-specific antibody production
L. Ansaloni et al. 238
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mon
trea
l on
12/0
1/14
For
pers
onal
use
onl
y.
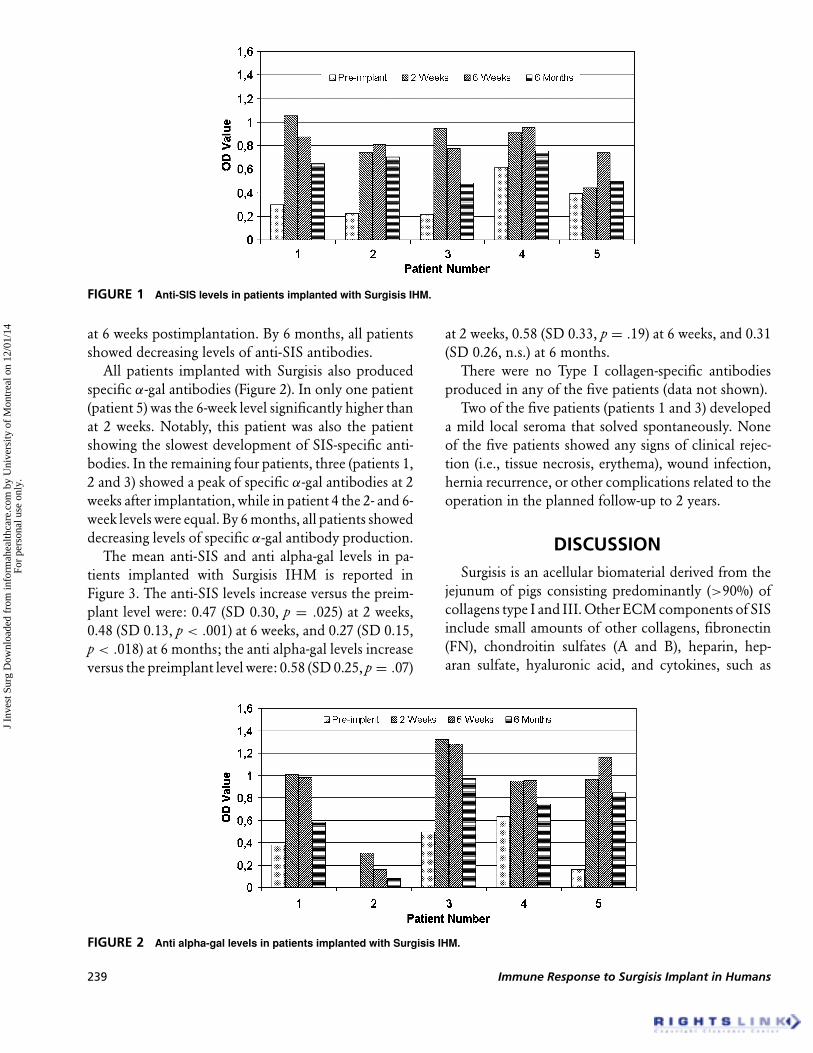
FIGURE 1 Anti-SIS levels in patients implanted with Surgisis IHM.
at 6 weeks postimplantation. By 6 months, all patientsshowed decreasing levels of anti-SIS antibodies.
All patients implanted with Surgisis also producedspecific α-gal antibodies (Figure 2). In only one patient(patient 5) was the 6-week level significantly higher thanat 2 weeks. Notably, this patient was also the patientshowing the slowest development of SIS-specific anti-bodies. In the remaining four patients, three (patients 1,2 and 3) showed a peak of specific α-gal antibodies at 2weeks after implantation, while in patient 4 the 2- and 6-week levels were equal. By 6 months, all patients showeddecreasing levels of specific α-gal antibody production.
The mean anti-SIS and anti alpha-gal levels in pa-tients implanted with Surgisis IHM is reported inFigure 3. The anti-SIS levels increase versus the preim-plant level were: 0.47 (SD 0.30, p = .025) at 2 weeks,0.48 (SD 0.13, p < .001) at 6 weeks, and 0.27 (SD 0.15,p < .018) at 6 months; the anti alpha-gal levels increaseversus the preimplant level were: 0.58 (SD 0.25, p = .07)
FIGURE 2 Anti alpha-gal levels in patients implanted with Surgisis IHM.
at 2 weeks, 0.58 (SD 0.33, p = .19) at 6 weeks, and 0.31(SD 0.26, n.s.) at 6 months.
There were no Type I collagen-specific antibodiesproduced in any of the five patients (data not shown).
Two of the five patients (patients 1 and 3) developeda mild local seroma that solved spontaneously. Noneof the five patients showed any signs of clinical rejec-tion (i.e., tissue necrosis, erythema), wound infection,hernia recurrence, or other complications related to theoperation in the planned follow-up to 2 years.
DISCUSSIONSurgisis is an acellular biomaterial derived from the
jejunum of pigs consisting predominantly (>90%) ofcollagens type I and III. Other ECM components of SISinclude small amounts of other collagens, fibronectin(FN), chondroitin sulfates (A and B), heparin, hep-aran sulfate, hyaluronic acid, and cytokines, such as
239 Immune Response to Surgisis Implant in Humans
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mon
trea
l on
12/0
1/14
For
pers
onal
use
onl
y.
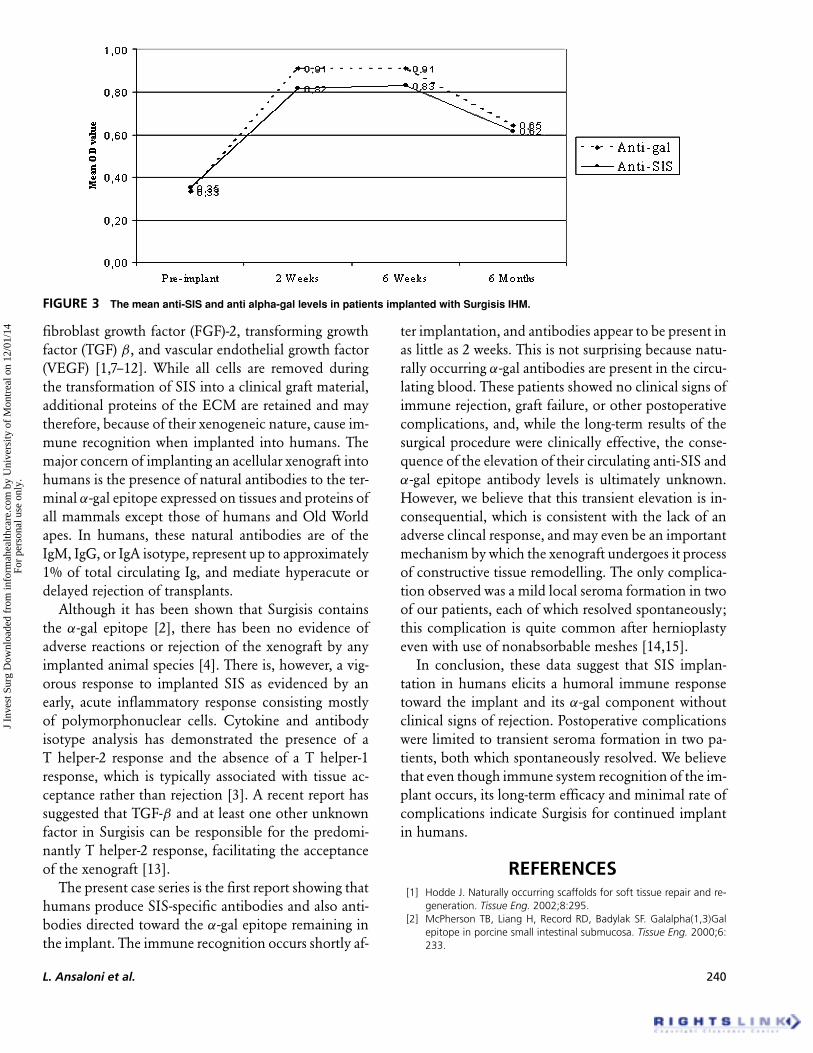
FIGURE 3 The mean anti-SIS and anti alpha-gal levels in patients implanted with Surgisis IHM.
fibroblast growth factor (FGF)-2, transforming growthfactor (TGF) β, and vascular endothelial growth factor(VEGF) [1,7–12]. While all cells are removed duringthe transformation of SIS into a clinical graft material,additional proteins of the ECM are retained and maytherefore, because of their xenogeneic nature, cause im-mune recognition when implanted into humans. Themajor concern of implanting an acellular xenograft intohumans is the presence of natural antibodies to the ter-minal α-gal epitope expressed on tissues and proteins ofall mammals except those of humans and Old Worldapes. In humans, these natural antibodies are of theIgM, IgG, or IgA isotype, represent up to approximately1% of total circulating Ig, and mediate hyperacute ordelayed rejection of transplants.
Although it has been shown that Surgisis containsthe α-gal epitope [2], there has been no evidence ofadverse reactions or rejection of the xenograft by anyimplanted animal species [4]. There is, however, a vig-orous response to implanted SIS as evidenced by anearly, acute inflammatory response consisting mostlyof polymorphonuclear cells. Cytokine and antibodyisotype analysis has demonstrated the presence of aT helper-2 response and the absence of a T helper-1response, which is typically associated with tissue ac-ceptance rather than rejection [3]. A recent report hassuggested that TGF-β and at least one other unknownfactor in Surgisis can be responsible for the predomi-nantly T helper-2 response, facilitating the acceptanceof the xenograft [13].
The present case series is the first report showing thathumans produce SIS-specific antibodies and also anti-bodies directed toward the α-gal epitope remaining inthe implant. The immune recognition occurs shortly af-
ter implantation, and antibodies appear to be present inas little as 2 weeks. This is not surprising because natu-rally occurring α-gal antibodies are present in the circu-lating blood. These patients showed no clinical signs ofimmune rejection, graft failure, or other postoperativecomplications, and, while the long-term results of thesurgical procedure were clinically effective, the conse-quence of the elevation of their circulating anti-SIS andα-gal epitope antibody levels is ultimately unknown.However, we believe that this transient elevation is in-consequential, which is consistent with the lack of anadverse clincal response, and may even be an importantmechanism by which the xenograft undergoes it processof constructive tissue remodelling. The only complica-tion observed was a mild local seroma formation in twoof our patients, each of which resolved spontaneously;this complication is quite common after hernioplastyeven with use of nonabsorbable meshes [14,15].
In conclusion, these data suggest that SIS implan-tation in humans elicits a humoral immune responsetoward the implant and its α-gal component withoutclinical signs of rejection. Postoperative complicationswere limited to transient seroma formation in two pa-tients, both which spontaneously resolved. We believethat even though immune system recognition of the im-plant occurs, its long-term efficacy and minimal rate ofcomplications indicate Surgisis for continued implantin humans.
REFERENCES[1] Hodde J. Naturally occurring scaffolds for soft tissue repair and re-
generation. Tissue Eng. 2002;8:295.[2] McPherson TB, Liang H, Record RD, Badylak SF. Galalpha(1,3)Gal
epitope in porcine small intestinal submucosa. Tissue Eng. 2000;6:233.
L. Ansaloni et al. 240
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mon
trea
l on
12/0
1/14
For
pers
onal
use
onl
y.

[3] Allman AJ, McPherson TB, Badylak SF, Merrill LC, Kallakury B, Shee-han C, Raeder RH, Metzger DW. Xenogeneic extracellular matrixgrafts elicit a TH2-restricted immune response. Transplantation.2001;71:1631.
[4] Raeder RH, Badylak SF, Sheehan C, Kallakury B, Metzger DW. Nat-ural anti-galactose alpha1,3 galactose antibodies delay, but do notprevent the acceptance of extracellular matrix xenografts. TransplImmunol. 2002;10:15.
[5] Ansaloni L, Catena F, D’Alessandro L. Prospective randomized,double-blind, controlled trial comparing Lichtenstein’s repair of in-guinal hernia with polypropylene mesh versus Surgisis gold softtissue graft: Preliminary results. Acta Biomed Ateneo Parmense.2003;74(Suppl 2):10.
[6] Yang YG, deGoma E, Ohdan H, Bracy JL, Xu Y, Iacomini J, ThallAD, Sykes M. Tolerization of anti-Galalpha1–3Gal natural antibody-forming B cells by induction of mixed chimerism. J Exp Med.1998;187:1335.
[7] Hodde JP, Badylak SF, Brightman AO, Voytik-Harbin SL. Gly-cosaminoglycan content of small intestinal submucosa: Abioscaffold for tissue replacement. Tissue Eng. 1996;2:209.
[8] Voytik-Harbin SL, Brightman AO, Kraine MR, Waisner B, Badylak
SF. Identification of extractable growth factors from small intestinalsubmucosa. J. Cell Biochem. 1997;67:478.
[9] McPherson TB, Badylak SF. Characterization of fibronectin derivedfrom porcine small intestinal submucosa. Tissue Eng. 1998;4:75.
[10] Hodde JP, Hiles MC. Bioactive FGF-2 in sterilized extracellular matrix.Wounds. 2001;13:195.
[11] Hodde JP, Record RD, Liang HA, Badylak SF. Vascular endothelialgrowth factor in porcine-derived extracellular matrix. Endothelium.2001;8:11.
[12] Badylak SF. Xenogeneic extracellular matrix as a scaffold for tissuereconstruction. Transpl Immunol. 2004;12:367.
[13] Palmer EM, Beilfuss BA, Nagai T, Semnani RT, Badylak SF, vanSeventer GA. Human helper T cell activation and differentiationis suppressed by porcine small intestinal submucosa. Tissue Eng.2002;8:893.
[14] Sakorafas GH, Halikias I, Nissotakis C, Kotsifopoulos N, Stavrou A,Antonopoulos C, Kassaras GA. Open tension free repair of inguinalhernias; the Lichtenstein technique. BMC Surg. 2001;1:3.
[15] Yamamoto S, Maeda T, Uchida Y, Yabe S, Nakano M, Sakano S,Yamamoto M. Open tension-free mesh repair for adult inguinal her-nia: Eight years of experience in a community hospital. Asian J Surg.2002;25:121.
241 Immune Response to Surgisis Implant in Humans
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mon
trea
l on
12/0
1/14
For
pers
onal
use
onl
y.









![Porcine vesical acellular matrix graft of tunica albuginea for penile … · 2016-08-26 · sue [2, 3]. The acellular matrix, using urinary tract tis-sue or small intestinal submucosa](https://img.pdfslide.net/doc/110x75/5f9142224c3f14202461bc23/porcine-vesical-acellular-matrix-graft-of-tunica-albuginea-for-penile-2016-08-26.jpg)