Embed Size (px)
Citation preview

Pediatr Blood Cancer 2006;46:372–376
BRIEF REPORTImmune Thrombocytopenia Following Successful
Treatment of Cancer in Children
Victoria Price, MB, ChB,1 Chris Barnes, MB BS,1 Patricia Canning, RN,2
Victor Blanchette, MD,1 and Mark Greenberg, MD1*
INTRODUCTION
The dramatic improvement in the survival of childrenwith cancer has been a major breakthrough in pediatricmedicine over the last three decades. Current survival ratesin childhood cancer approach 75% and it is estimated that1 in 810 of individuals younger than 20 years of age aresurvivors of childhood cancer [1]. In the setting of in-creasing survival rates, the study of long-term effects oftreatment of childhood cancer has appropriately becomea major focus of recent research. Recognized adverselong-term effects have included deficits in growth,impaired intellectual function, endocrinopathies, reduc-tion in cardiac performance, and secondary malignancies[1]. Reconstitution of the immune system followingchemotherapy has also been well studied and a numberof reports demonstrate gross return of function of humoraland cellular components of the immune system within12 months of ceasing chemotherapy [2–4].
Immune thrombocytopenic purpura (ITP) is a wellcharacterized autoimmune disorder presenting as in-creased bruising and petechiae secondary to auto-antibodymediated platelet destruction. ITP occurs with anapproximate incidence in children of 4–5.3 per 100,000children [5,6]. Themajority of children with ITPwill havean acute self-limiting illness with complete platelet countrecovery. Chronic ITP is defined as a persistent plateletcount of less than 150� 109/L for longer than 6 monthsfrom the onset of illness and occurs in 5.3%–9.3% ofchildren with ITP [7]. The association of ITP occurring inchildren following successful treatment for childhoodcancer, excluding ITP associated with Hodgkin lym-phoma, has not previously been reported. Followingrecognition of the occurrence of ITP in a number ofchildren followed in a late effects clinic at the Hospital for
Sick Children, the presenting features, laboratory inves-tigations, and response to therapy of these children werereviewed. A review of the literature including possiblemechanisms for an increase in the incidence of ITP andother auto-immune conditions in children following treat-ment with cancer is presented.
CASE REPORTS
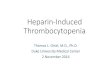
Table I demonstrates patient demographics and ITPcharacteristics.
Case 1
A 16-month-old boy with a localized endodermal sinustumor of the mediastinum was treated with surgicalresection and three cycles of chemotherapy consisting ofVP-16 (total dose 1,800 mg/m2), cisplatinum (total dose300 mg/m2), and bleomycin (90 mg/m2). Followingchemotherapy hewas deemed to be in complete remissionand complete blood counts (CBC) were repeatedlynormal. At 6.8 years of age, the patient presented withincreased bruising and petechiae following a viral illnesscharacterized by diarrhea. A CBC demonstrated isolatedthrombocytopenia (platelet count of 26� 109/L). Given
A predisposition to developing immunethrombocytopenia (ITP) has not been reportedin survivors of childhood cancer. We report acase series of childhood cancer survivors whodeveloped an isolated thrombocytopenia in thepresence of a normocellular bone marrow. Fivechildren, two with endodermal sinus tumorsand three with acute lymphoblastic leukemia,
developed ITP at a median of 4 years (range:0.2–8 years) after completion of therapy. Wesuggest the association of ITP in survivors ofchildhood malignancy may not be co-incidentalas chemotherapy may cause persistent immunedysfunction. Pediatr Blood Cancer 2006;46:372–376. � 2005 Wiley-Liss, Inc.
Key words: childhood cancer survivors; immune thrombocytopenia
� 2005 Wiley-Liss, Inc.DOI 10.1002/pbc.20341
——————1Department of Pediatrics, Division of Hematology/Oncology, The
Hospital for Sick Children, University of Toronto, Canada
2Department of Nursing, The Hospital for Sick Children, University of
Toronto, Canada
*Correspondence to: Dr. Mark Greenberg, Division of Hematology/
Oncology, The Hospital for Sick Children, 555 University Avenue,
Toronto, M5G 1X8. E-mail: [email protected]
Received 28 September 2004; Accepted 17 December 2004

the patients past history of malignancy and treatment withchemotherapy, a bone marrow examination was per-formed and showed a normocellular bone marrow withno dysplastic features and increased megakaryopoiesis,consistent with ITP. The patient was treated with in-travenous gammaglobulin (IVIG), which was followed byan improvement in the platelet count to 80� 109/L. Thefollowing 6 months were characterized by repeatedexacerbations of thrombocytopenia treated with a totalof five courses of corticosteroids. At the most recentfollow-up, 3 years following the first presentation withthrombocytopenia, the platelet count was normal.
Case 2
A 4-year-old girl with an ovarian endodermal sinustumor, was treated with a unilateral salpingo-oophorect-omy, followed by three courses of chemotherapy consist-ing of VP-16 (total dose 1,800 mg/m2), cisplatinum (totaldose 300mg/m2), and bleomycin (90mg/m2). Chemother-apy was completed 3 months after the initial diagnosis. At12 years of age she presented with bruising and a plateletcount of 16� 109/L. The rest of the CBC analysis wasnormal. A bone marrow examination revealed a normo-cellular marrow with normal numbers of megakaryocytesand no evidence of dysplasia, consistentwith the diagnosisof ITP. There were no chromosomal abnormalities de-tected. Platelet antibodies (platelet associated immuno-globulins) were detected. She received corticosteroids andintravenous gamma globulin (IVIG) respectively withacute exacerbations of thrombocytopenia. The patientremained moderately thrombocytopenic for the following4 years. A repeat bone marrow examination 2 years afterpresenting with thrombocytopenia, demonstrated mildmegakaryocytic hyperplasia consistent with persistentimmune destruction of platelets. Six years after the initialdiagnosis of ITP, her platelet count normalized and hasremained stable.
Case 3
A 2.6-year-old female, diagnosed with acute lympho-blastic leukemia and treated with an in house BFM basedprotocol including: vincristine, L-asparginase (total dose94,000 U/m2), prednisone, dexamethasone, daunomycin,and adriamycin (total anthracycline dose 200 mg/m2),cyclophosphamide (total dose 3,000 mg/m2), metho-trexate (total dose 3,300 mg/m2), cytarabine (total dose1,800 mg/m2), 6 mercaptopurine, and 6 thioguanine. Shereceived intrathecal methotrexate for central nervoussystem (CNS) prophylaxis and did not receive radio-therapy. Four years after completion of chemotherapy, shepresented with bruising and petechiae. Her CBC showedan isolated thrombocytopenia (platelet count 28� 109/L).A bone marrow aspiration revealed a normocellularmarrow with megakaryocytic hyperplasia and no mor-T
ABLEI.
PatientDem
ographicsandIT
PCharacteristics
Patient
Diagnosis
Ageat
diagnosis
(years)
Treatment
Durationfrom
end
ofchem
otherapy
topresentationof
thrombocytopenia
(years)
Ageatdiagnosis
ITP(years)
Supplementalpositive
investigations
Treatment
Durationof
thrombocytopenia
(years)
1Endodermalsinustumor
1.3
CisplatinVP-16Bleomycin
5.5
6.8
None
IVIG
bcorticosteroids
0.5
2Endodermalsinustumor
4CisplatinVP-16Bleomycin
812
Antiplateletantibodies
IVIG
corticosteroids
>4
3ALLa
2.6
BFM
based
highrisk
protocol
410.2
None
IVIG
>8
4ALL
1.8
BFM
based
highrisk
protocol
12
16
None
IVIG
corticosteroids
splenectomy
0.2
5ALL
10.5
BFM
based
highrisk
protocol
0.2
13.3
Antiplateletantibodies"R
PCcNone
>4
aALL,acutelymphoblasticleukem
ia.
bIV
IG,intravenousgam
maglobulins.
cRPC,reticulatedplateletcount.
Immune Thrombocytopenia Following Chemotherapy 373

phological evidence of dysplasia, consistent with ITP. Theplatelet count increased to 142� 109/L after two doses ofIVIG (total dose 2 g/kg). All investigations for a secondarycause for chronic ITP including: antinuclear antibodies,rheumatoid factor, C3 and C4 levels, immunoglobulinlevels, and a direct Coombs’ test were negative. Althoughshe has not required treatment again, her platelet countremains below 150� 109/L. The most recent plateletcount was 111� 109/L, 8 years after her initial presenta-tion with acute ITP.
Case 4
A male infant, presented at age 1.8 years with acutelymphoblastic leukemia. He was treated according to thein house BFM-based chemotherapy protocol described incase 3 without high dose methotrexate, but including theadditionof cranial irradiation (1,800cGY).At age16yearshe presented with bruising and petechiae. He had a severethrombocytopenia (platelet count 15� 109/L) and thebone marrow aspiration showed a normocellular marrow,no dysplastic features and megakaryocytic thrombocyto-penia consistent with acute ITP. Despite receiving twocourses of prednisone and IVIG, his platelet count did notincrease and a month after his initial presentation withacute ITP, he underwent a splenectomy with subsequentimprovement in platelet count, and has not required anyfurther treatment.
Case 5
A female patient, diagnosed at age 10.5 years withacute lymphoblastic leukemia and treated with the above-mentioned BFM-based in house leukemia protocol in-cluding cranial irradiation, presented with an isolatedthrombocytopenia at completion of treatment. The throm-bocytopeniawas not severewith the platelet count rangingbetween 80� 109/L–100� 109/L. The reticulated plate-let count (RPC) was elevated at 3.60 (range: 1.00–1.50)and anti-platelet IgG antibodies were present. As she hadpersistent thrombocytopenia, she underwent two bonemarrow examinations over a 3 year period. Both con-firmed a normocellular bone marrow with no dysplasticfeatures and the presence of megakaryocytes, compatiblewith ITP. Further investigations for a secondary cause ofITP were negative and included anti nuclear antibodies,C3, C4, and immunoglobulin levels as well as a directCoombs’ test. As this was an asymptomatic, mild throm-bocytopenia, she did not receive any treatment.
DISCUSSION
We report five children who developed ITP, at a medianage of 12 years (range: 6.8–16 years), and a median of4 years (range: 0.2–8 years) after completion of cancertherapy. The number of patients presenting to the Hospital
for Sick Children for management of malignancy over thelast decade is approximately 2,500. As this is a case series,no formal statistical analyses can be made. Nonetheless,three of these children had chronic ITP, resulting in aprevalence of chronic ITP which appears to be higher thanthat reported in healthy Swedish children in which theprevalence of chronic ITP was 4.6 in 100,000 children [8].Several important biases preclude statistical comparisonof the prevalence of ITP following childhood cancer in thisreport to that in otherwise healthy children. For example,approximately 1/3 of children with cancer will not survivethe cancer diagnosis, thus decreasing the observed pre-valence of ITP. By contrast, survivors of cancer are anattuned population, particularly to signs and symptoms ofbleeding, which may increase the proportion of childrenwith moderate ITP presenting with clinical complaints,compared to healthy children in whom the diagnosis maynever come to the attention of a health care professional.
There are a number of reports of ITP occurring in adultpatients following successful treatment for malignancy.Jillela et al. [9] provide a report of a 58-year-old femalefollowing autologous hematopoietic cell transplantationas treatment for breast carcinoma. The patient respondedto treatment including corticosteroids and IVIG. In thesame report a review of six reported cases of auto-immunethrombocytopenia following autologous transplantationis provided. The age of these cases ranged from 16 to50 years of age. Four of the cases were treated for acutemyeloid leukemia and two cases were treated forlymphoblastic lymphoma. In all three patients wherelong-term follow-up was available the thrombocytopeniaresolved. Ustun et al. [10] report ITP occurring in a 40-year-old female while being treated for breast cancer. Theauthors review six reported cases of ITP occurring inpatients with metastatic breast cancer and conclude theassociation is likely to be co-incidental. There are severalreports of ITP developing in patients with Hodgkinlymphoma who are in remission [11] and for the purposeof this report, will not be included in the discussion.
Four of the five children in this series presented withclinical ITP, and only one (case 5) was diagnosed onfollow up CBCs. Although we recognize that conclusionscannot be drawn from such a small cohort, it is interestingthat the three patients who developed a chronic course(case nos. 2, 3, 5)were female and their ageswere 12, 10.2,and 13.3 years, respectively. Predictors for the develop-ment of chronic ITP in children include older age(>10 years) at onset and female sex [12]. In the case ofchronic ITP, it is suggested that a secondary cause beactively excluded [13]. Investigations that should be con-sidered include screening for systemic lupus erythematosus(antinuclear antibody, antiphospholipid antibody), dys-gammaglobulinemia/agammaglobulinemia (quantitativeimmunoglobulin levels, specific antibody titres), and otherautoimmune diseases (direct Coombs’ test, thyroid func-
374 Price et al.

tion tests). A secondary cause could not be identified inany of the patients who developed chronic ITP, which begsthe question as towhether their exposure to chemotherapymay have predisposed them to a chronic course.
The exact pathogenic mechanism for development ofITP is not fully known. The immunopathogenesis is knownto involve the formation of auto-antibodies directedagainst platelets leading to Fc receptor mediated phago-cytosis by the reticuloendothelial system [14] but thecontrol mechanisms leading to the development of anti-bodies directed against platelet antigens are not fullyunderstood. There is, however, evidence to suggest thatT-cell lymphocytes are critical in the development of auto-immune thrombocytopenia. T-cells of patients withchronic ITP have been shown to secrete interleukin-2 inresponse to normal platelet antigens [15]. Furthermore,abnormal clonal T-cells have been shown to accumulatein the peripheral blood of patients with auto-immunethrombocytopenia [16]. A link between T-cells and B-cells in the pathogenesis of ITP is suggested by the findingthat anti-platelet antibody producing splenic B-cells inpatients with acute ITP have undergone somatic mutation[17]. Somatic mutation is a strictly T-cell mediated pro-cess. There are a number of studies demonstrating per-sistent immune abnormalities in children recovering fromchemotherapy [2,4,18–20]. Lasting immune abnormal-ities include defects with respect to previous infections orvaccinations, reduced number of CD8þ T-cell lympho-cytes and abnormalities in immunoglobulin subclasses.We are unable to provide any laboratory-based data toexplain why survivors of childhood cancer might bepredisposed to develop auto-immune thrombocytopenia.It should also be noted that even currently available toolsto assess the integrity of the immune response are limitedand may not detect subtle abnormalities. Potentially,subtle persistent immune abnormalities following chemo-therapy may predispose survivors of childhood cancer todevelop auto-immune conditions including auto-immunethrombocytopenia.
The presentation of thrombocytopenia in a child whohas previously been treated for malignancy requiresdifferentiation between suppression of bone marrowproduction secondary to therapy and peripheral destruc-tion of platelets related to or independent of therapy.Exclusion of recurrence of the malignancy or the devel-opment of therapy-relatedmyelodysplasia (MDS) or acutemyeloid leukemia (AML) is the most important priorityand urgent bone marrow examination is warranted. In thepresent series none of the patients had morphologicalevidence of bone marrow dysplasia. Alkylating agents,topoisomerase II inhibitors, and radiation are risk factorsfor the development of therapy-related MDS/AML [21].Characteristically, there is a latency period of 5–7 years inpatients who develop alkylating agent related MDS/AMLand a preleukemic/myelodysplastic phase often precedes
overt leukemia by months to years. Patients who developleukemia following exposure to topoisomerase II inhibi-tors, present with a shorter latency period (1–3 years) andan overt AML with no preceding dysplastic phase [21].Investigations thatwould support a diagnosis ofMDSoverITP in such patients include an increased mean corpus-cular volume (MCV) in the absence of vitamin B12 andfolate deficiencies and an increased percentage of HbFon hemoglobin electrophoresis. Cytogenetic studies areessential for the evaluation of a child with suspectedMDS, with the most common abnormalities being mono-somy 7, þ8, and þ21. Furthermore, MDS with þi(12p)has been reported after successful treatment of germ celltumors [22].
Megakaryocytic hyperplasia consistent with increasedperipheral destruction of platelets may be an unexpectedfinding in this setting and is a diagnosis of exclusion. Thereis evidence that platelet production may be impaired inITP; one possiblemechanismbeing antiplatelet antibodiesbinding to megakaryocytes in the bonemarrow [23,24]. Invitro studies support this concept showing that humanmegakaryocyte colony formation is inhibited and in thepresence of certain antiplatelet antibodies there is reducedexpansion of megakaryocyte progenitors [25,26]. How-ever, despite evidence of reduced platelet production inITP, the number of megakaryocytes in the bone marroware usually normal or increased [27]. This is in contrast toa hypoplastic bone marrow, evaluated by bone marrowbiopsy, that would be expected secondary to chemo-therapy or certain viral infections (e.g., parvovirus B19,Epstein–Barr virus, human herpes virus 6, cytomegalo-virus, and human immunodeficiency virus). In support ofan increased peripheral destruction of platelets, a reticulat-ed platelet count (RPC) may be helpful as an increasedpercentage is a direct measure of young platelets andindicates increased platelet turnover. Megakaryocytosisassociated with an increased percentage of reticulatedplatelets indicates the origin of thrombocytopenia isperipheral destruction. The limitation of this test lies inthe fact that the reticulated platelet percentagemay only beelevated when the platelet count is below 60� 109/L [28].Ideally a platelet antibody assay should assist in dis-criminating between antibody-mediated thrombocytope-nia and other causes of thrombocytopenia. Despite manydifferent techniques being devised for themeasurement ofplatelet antibodies, available tests lack sufficient sensitiv-ity and specificity to be a useful tool as positive antibodytests have been reported in patients with non-immunethrombocytopenias [29]. For this reason, the AmericanSociety of Hematology deemed platelet-antigen specificantibody assays unnecessary in the routine evaluation ofchildhood ITP [30].
We report five cases of presumed auto-immune throm-bocytopenia occurring in survivors of childhood malig-nancy. There is no definitive evidence for an increased
Immune Thrombocytopenia Following Chemotherapy 375

incidence of autoimmune thrombocytopenia occurringfollowing chemotherapy. However, the number of caseswe present relative to the number of patients follow-ed in our pediatric oncology late effects clinic, combinedwith our understanding of the immune basis of ITP andthe finding of persistent immune function abnormalitiesin children following chemotherapy suggest the associa-tion of ITP in survivors of childhood malignancy may notbe co-incidental. In addition to the routine investiga-tion and management of thrombocytopenia in this con-text, a thorough assessment of immune function includingevaluation of T-cell subsets may increase our under-standing of the immuno-pathogenesis of autoimmunethrombocytopenia.
ACKNOWLEDGMENT
The authors wish to thank Dr. Yigal Dror for his criticalreview of the article.
REFERENCES
1. Hewitt M, Weiner SL, Simone JV, editors. The epidemiology of
childhood cancer. In: Childhood cancer survivorship improving
care and quality of life. Washington, DC: The National Academies
Press; 2003. 35p.
2. Alanko S, Pelliniemi TT, Salmi TT. Recovery of blood lympho-
cytes and serum immunoglobulins after treatment of solid tumors
in children. Pediatr Hematol Oncol 1994;11:33–45.
3. Alanko S, Salmi TT, Pelliniemi TT. Recovery of natural killer cells
after chemotherapy for childhood acute lymphoblastic leukemia
and solid tumors. Med Pediatr Oncol 1995;24:373–378.
4. Mustafa MM, Buchanan GR, Winick NJ, et al. Immune recovery
in children with malignancy after cessation of chemotherapy.
J Pediatr Hematol Oncol 1998;20:451–457.
5. Lilleyman JS. Management of childhood idiopathic thrombocyto-
penic purpura. Br J Haematol 1999;105:871–875.
6. Zeller B, Helgestad J, Hellebostad M, et al. Immune thrombo-
cytopenic purpura in childhood in Norway: A prospective,
population-based registration. Pediatr Hematol Oncol 2000;17:
551–558.
7. Kuhne T, Buchanan GR, Zimmerman S, et al. A prospective com-
parative study of 2,540 infants and children with newly diagnosed
idiopathic thrombocytopenic purpura (ITP) from the Interconti-
nental Childhood ITP Study Group. J Pediatr 2003;143:605–608.
8. Hedman A, Henter JI, Hedlund I, et al. Prevalence and treatment
of chronic idiopathic thrombocytopenic purpura of childhood in
Sweden. Acta Paediatr 1997;86:226–227.
9. Jillella AP, Kallab AM, Kutlar A. Autoimmune thrombocytopenia
following autologous hematopoietic cell transplantation: Review
of literature and treatment options. BoneMarrow Transplant 2000;
26:925–927.
10. Ustun C, Dainer P, Hendricks L, et al. Association of breast cancer
and immune thrombocytopenic purpura. South Med J 2002;95:
1335–1337.
11. Bradley SJ, Hudson GV, Linch DC. Idiopathic thrombocytopenic
purpura in Hodgkin disease: A report of eight cases. Clin Oncol
1993;5:355–357.
12. Robb LG, Tiedeman K. Idiopathic thrombocytopenic purpura:
Predictors of chronic disease. Arch Dis Child 1990;65:502–
506.
13. Blanchette V, Carcao M. Approach to the investigation and man-
agement of immune thrombocytopenic purpura in children. Semin
Hematol 2000;37:299–314.
14. Cines D, Blanchette V. Immune thrombocytopenia purpura. N Eng
J Med 2002;346:995–1008.
15. Semple JW, Freedman J. Increased antiplatelet T helper lympho-
cyte reactivity in patients with autoimmune thrombocytopenia.
Blood 1991;78:2619–2625.
16. Shimomura T, Fujimura K, Takafuta T, et al. Oligoclonal accumu-
lation of T cells in peripheral blood from patients with idiopathic
thrombocytopenic purpura. Br J Haematol 1996;95:732–737.
17. Roark JH, Bussel JB, Cines DB, et al. Genetic analysis of
autoantibodies in idiopathic thrombocytopenic purpura reveals
evidence of clonal expansion and somatic mutation. Blood 2002;
100:1388–1398.
18. Alanko S, Salmi TT, Pelliniemi TT. Recovery of blood T-cell
subsets after chemotherapy for childhood acute lymphoblastic
leukemia. Pediatr Hematol Oncol 1994;11:281–292.
19. Kantar M, Cetingul N, Kansoy S, et al. Immune deficiencies
following cancer treatment in children. J Trop Pediatr 2003;49:
286–290.
20. Smith S, Schiffman G, Karayalcin G, et al. Immunodeficiency in
long-term survivors of acute lymphoblastic treated with Berlin–
Frankfurt–Munster therapy. J Pediatr 1995;127:68–75.
21. Rund D, Ben-Yehuda D. Therapy-related leukemia and myelodys-
plasia: Evolving concepts of pathogenesis and treatment. Hema-
tology 2004;9:179–187.
22. Christodoulou J, Schoch C, Schnittger S, et al. Myelodysplastic
syndrome (RARS)withþi(12p) abnormality in a patient 10months
after diagnosis and successful treatment of a mediastinal germ cell
tumor (MGCT). Ann Hematol 2004;83:386–389.
23. Ballem PJ, Segal GM, Stratton JR, et al. Mechanisms of throm-
bocytopenia in chronic auto-immune thrombocytopenic purpura:
Evidence of both impaired platelet production and increased
platelet clearance. J Clin Invest 1987;80:33–40.
24. McMillan R, Luiken GA, Levy R, et al. Antibodies against
megakaryocytes in idiopathic thrombocytopenic purpura. JAMA
1978;239:2460–2462.
25. Takahashi R, Sekine N, Nakatake T. Influence of monoclonal
antiplatelet glycoprotein antibodies on in vitro human megakar-
yocyte colony formation and proplatelet formation. Blood 1999;
15:1951–1958.
26. Chang M, Nakagawa PA, Williams SA, et al. Immune thrombo-
cytopenic purpura (ITP) plasma and purified ITP monoclonal
autoantibodies inhibit megakaryocytopoiesis in vitro. Blood 2003;
102:887–895.
27. Louwes H, Zeinali Lathori OA, Vellenga E, et al. Platelet kinetic
studies in patients with idiopathic thrombocytopenic purpura. Am J
Med 1999;106:430–434.
28. Saxon BR, Mody M, Blanchette VS, et al. Reticulated platelet
counts in the assessment of thrombocytopenic disorders. Acta
Paediatr Suppl 1998;424:65–70.
29. Winiarski J. Measurement of platelet antibodies: Where do we
stand? Acta Paediatr Suppl 1988;424:51–53.
30. George JN, Woolf SH, Raskob GE. Idiopathic thrombocytopenic
purpura: Aguideline for diagnosis andmanagement of children and
adults. American Society of Hematology. Ann Med 1998;30:
38–44.
376 Price et al.