-
8/18/2019 Immunity 12
1/4
Journal of Clinical Virology 46 (2009) 161–164
Contents lists available at ScienceDirect
Journal of Clinical Virology
j o u r n a l h o m e p a g e : w w w . e l s e v i
e r . c o m / l o c a t e / j c v
Prevalence of influenza A and B antibodies in pregnant
women and their offspring
Peter Wutzler a, Ruprecht Schmidt-Ott b, Heike Hoyer c, Andreas
Sauerbreia,∗
a Institute of Virology and Antiviral Therapy,
Friedrich-Schiller University of Jena, Hans-Knoell-Straße 2, 07745
Jena, Germanyb GlaxoSmithKline, Theresienhöhe 11, 80339 Munich,
Germanyc Institute of Medical Statistics, Computer Sciences and
Documentation, Friedrich-Schiller University, Bachstraße 18, 07743
Jena, Germany
a r t i c l e i n f o
Article history:Received 5 December 2008
Received in revised form 24 June 2009
Accepted 24 June 2009
Keywords:
Influenza
Antibody prevalence
Placental antibody transfer
a b s t r a c t
Background: Influenza is associated with substantial
morbidity and mortality in pregnant women andneonates, but few
countriesoffer annualinfluenzavaccinationwith theinactivated
vaccine to all women
who are, or intend to become, pregnant.
Objectives: To provide seroepidemiological information on
influenza A and B antibodies in pregnant
women and their offspring in Germany.
Study design: Anti-influenza antibodies were determined
using commercially available enzyme-linked
immunosorbent assays (ELISA) on serum obtained from 209 women
and their newborns at delivery.
Results: Theprevalenceof antibodies against influenza A virus
was 93.8% [89.6–96.6%]in themothersand
96.7% [93.2–98.6%] in the newborns. The prevalence of antibodies
against influenza B virus was 42.1%
[35.3–49.1%] in themothers and78.5%[72.3–83.8%] in
theirnewborns, which wasa significant difference.
The antibody concentrations against both influenza A and
influenza B viruses were significantly lower in
mother than in their newborns.
Conclusions: Because of active placental transport of IgG
antibodies, neonates have higher prevalence
and/or concentrations of influenza A and B virus-specific
antibodies induced by natural infections than
their mothers. Considering these serological findings,
especially the lower prevalence of maternal anti-
body against influenza B virus, annual influenza vaccination may
improve the protection of pregnantwomen and their offspring against
influenza.
© 2009 Elsevier B.V. All rights reserved.
1. Background
The most significant respiratory infection that affects
pregnant
women with the risk of severe illness and death is
influenza.
Women of child-bearing age have increased exposure to young
children who have a high prevalence of infection during
influenza
epidemics.1 The rate of seasonal influenza infection during
the
secondand thirdtrimester isreported torange from 2%to 22%.2
Epi-
demiological studies during the past 25 years document
increasedrates of influenza in pregnant women compared with healthy
non-
pregnant women.3,4 Influenza-associated excess deaths among
pregnant women were documented during the pandemic “Spanish
Flu” of 1918–1919 and the pandemic “Asian Flu” of
1957–1958.5,6
Providing pregnant women withannual influenza vaccination is
considered the mosteffective public health intervention to
prevent
influenza during pregnancy. The American College of
Obstetri-
∗ Corresponding author. Tel.: +36 41 9395700; fax: +36 41
9395702.
E-mail address: [email protected] (A.
Sauerbrei).
cians and Gynecologists (ACOG), along with theCenters for
Disease
Control and Prevention, recommend that all women who are, or
intend to become, pregnant during the influenza season should
be
vaccinated with the inactivated influenza vaccine.7,8 In
Germany,
influenza vaccine is not recommended for pregnant women.9
Such
a policy would not only be beneficial for pregnant women,
but
their offspring might also be protected by placentally
transmit-
ted maternal antibodies during the first months of life.10
Influenza
in neonates and very young children is associated with
substan-tialmorbidity and occasionalmortality.11,12 R atesof
hospitalization
during the influenza season are highest in very young
children,
particularly those under 6 months of age, and in high-risk
elderly
patients.13,14
2. Objectives
The objective of this study was to provide information on
the
prevalence of influenza A and B antibodies in pregnant women
and
their offspring in selected populations in Germany.
1386-6532/$ – see front matter © 2009 Elsevier B.V. All rights
reserved.
doi:10.1016/j.jcv.2009.06.024
http://www.sciencedirect.com/science/journal/13866532http://www.elsevier.com/locate/jcvmailto:[email protected]://localhost/var/www/apps/conversion/tmp/scratch_5/dx.doi.org/10.1016/j.jcv.2009.06.024http://localhost/var/www/apps/conversion/tmp/scratch_5/dx.doi.org/10.1016/j.jcv.2009.06.024mailto:[email protected]://www.elsevier.com/locate/jcvhttp://www.sciencedirect.com/science/journal/13866532
-
8/18/2019 Immunity 12
2/4
162 P. Wutzler et al. / Journal of Clinical Virology 46
(2009) 161–164
3. Study design
3.1. Subjects and serum samples
Allhealthywomenwho delivered at theDistrict Hospital Rudol-
stadt, German federal state Thuringia, between January 1999
and
January 2000, and their healthy newborn infants agreed to
be con-
secutively enrolled in this study. At delivery, the women and
their
offspring were clinicallyhealthyand routine laboratory
parameters
were normal. Two hundred and nine women aged between 17 and
40 years (mean 26.1 years, standard deviation, SD 4.3) and
their
offspring were included in this study. One hundred and
eighty-
nine (89.0%) infants were delivered spontaneously; 13 (6.2%)
by
caesarean section; and 10 (4.8%) by vacuum extraction, at
gesta-
tional age of 34–42 weeks (mean 39.8 weeks, SD 1.3). Data on
maternal occupation and history of influenza immunization
were
not available. Blood samples were taken from all women at
the
time of delivery and from the umbilical cord of the neonates by
the
gynaecologist shortly after birth. Contamination of newborn
blood
withmaternalblood wasavoided.Maternaland newborn serawere
obtained without delay by centrifugation and stored in aliquots
of
0.5 mlat−20 ◦C forseveral yearsunderequal conditions that
would
not lead to concentration of the infant samples. Informed
consent
was obtained from the parents of the infants.
3.2. Serological testing
The Influenza Virus A IgG ELISA (no. INFG0290, lots
INFAG-023
and INFAG-27) and Influenza Virus B IgG ELISA (no. INFG0300,
lots
INFBG-024 and INFBG-29) manufactured by NovaTec Immundi-
agnostica (Dietzenbach, Germany) were used for qualitative
and
semi-quantitative antibody testing. The micro-titration strip
wells
were pre-coated with influenza virus type-specific antigens
con-
sisting of matrix proteins and nucleoproteins of influenza A
virus
strain Texas 1/77 (H3N2) and influenza B virus strain Hong
Kong
5/72, respectively. Testing of sera was carried out according to
the
manufacturer’s instructions. In short, sera diluted 1 in 100
were
incubated with antigen-coated wells, washed, and incubated
with
horseradish peroxidase-labeled anti-human IgG. The wells
were
then washed, after which they were incubated with
tetramethyl-
benzidine substrate; sulfuric acid was added to stop the
reaction.
Plateswere read photometrically at 450and 620nm. Samples
were
considered positive if the absorbance value was higher than
10%
above the cut-off. Negative samples had an absorbance value
lower
than 10% below the cut-off. Samples with an absorbance value
less
10% above or below the cut-off were regarded as equivocal.
By
using the arbitrary units “NovaTec Units” (NTU), a relative
quan-
titation within the test was possible. The NTU was calculated
with
the following formula:
mean absorbance× 10
cut-off = [NovaTec Units = NTU]
The cut-off was defined by the manufacturer as 10 NTU; posi-
tive sera contained>11 NTUand negative sera correspondedto
NTU
levels of
-
8/18/2019 Immunity 12
3/4
P. Wutzler et al. / Journal of Clinical Virology 46 (2009)
161–164 163
Table 2
Distribution of qualitativeIgG antibody againstinfluenza B virus
(IBV) in newbornscompared withtheir mothers. The numbers represent
the absolute numbers of newborns
tested negative, positive or equivocal for IBV antibodies.
Percentages are given in parenthesis.
Antibodies against IBV of mothers Antibodies against IBV of
newborns Summary
Negative Positive Equivocal
Negative 29 (13.9%) 40 (19.1%) 11 (5.3%) 80 (38.3%)
Positive 2 (1.0%) 86 (41.2%) 0 (0%) 88 (42.1%)
Equivocal 3 (1.4%) 38 (18.2%) 0 (0%) 41 (19.6%)
Summary 34 (16.3%) 164 (78.5%) 11 (5.3%) 209 (100%)
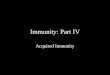
Fig. 1. Boxplotof
IgGantibodyconcentration[NovaTec-Units,NTU] againstinfluenza
A virus(IAV)and influenzaB virus(IBV) inmothers(m)andnewborns
(n)at thetime
of deliveryshowingmedian, 25thand 75thpercentile, minimum,
maximum and/or
outliers (values >1.5 inter-quartile range from the end of
the box).
SD 5.1 NTU). Gestational age did not significantly influence
IgG
concentrations against influenza B virus in the infants ( p
= 0.314).However, newborns who were delivered by vacuum
extraction
(n = 10) had significantly lower antibody concentrations (11.4
NTU,
SD 5.4NTU) than newborns who were delivered spontaneously
(n = 189, 14.5NTU, SD 5.0NTU) or by caesarean section (n =
13;
14.5NTU, SD 6.1 NTU) ( p = 0.046). Figs. 1 and 2
demonstrate the dis-
tribution of IgG antibody concentrations against influenza A
and
influenza B virus in the mothers and newborns at the time of
birth.
5. Discussion
Thehemagglutination inhibition(HI) assay andthecomplement
fixation (CF) test are used routinely for quantitation of
influenza
virus-specific serumantibodies.15 However,
theseassaysarelabori-
ous, difficult to incorporate into automatic procedures, and
requirea readily available source of appropriate erythrocytes.
ELISAs mea-
suring virus-specific serum IgG antibodies are more sensitive
than
the HI or the CF assay.16–18 Thus, they are more suitable for
the
determination of prevalence of antibodies against influenza A
and
influenza B viruses. Furthermore, since the matrix and
nucleopro-
tein antigens used in these ELISAs are highly conserved
within
both the influenza A and influenza B viruses,19–21 we could
detect
antibodies induced by influenza A and B viruses circulating
dur-
ing the last few years without subtype-specific assay. The
ELISA
assays do not require the annual adjustment of the viral
anti-
gen preparations and are not affected by antibodies induced
by
hemagglutinin antigens of split influenza vaccines that are
used
currently in Germany. A limitation is that quantitative
results
cannot be calibrated in the absence of an international
stan-
Fig. 2. Boxplot of mother–newborn pair differences of IgG
antibody concentration
[NovaTec-Units, NTU] against influenza A virus (IAV) and
influenza B virus (IBV) at
thetimeof deliveryshowingmedian,25thand75thpercentile,minimum,
maximum
and/or outliers (values >1.5 inter-quartile range from the
end of the box).
dard. Thus, the arbitrary NovaTec Units were used. Even
though
antibodies to influenza virus matrix and nucleoprotein
antigensmay not contribute to protection, they indicate the
presence of
subtype-independent T cell-mediated protection22 and may be
informative for the development and application of a new
live
attenuated influenza vaccine inducing both humoral and
cellular
immunity.
In thepresent study,the prevalenceof theanti-influenza B
virus-
specific antibodies was significantly greater in neonates than
in
their mothers. In addition, the antibody concentrations against
the
influenza A virus as well as the influenza B virus were
significantly
higher in newborns than in their mothers. The mean
newborn-to-
mother ratios between cord and maternal blood were between
1.2
and 1.5 for antibodies against influenza A virus and between
1.3
and 1.7 for antibodies against influenza B virus. These data
suggest
active placental transfer of maternal influenza virus-specific
IgGduring the third trimester of pregnancy. Apart from the
quantita-
tive differences, theprevalence of influenza B antibodyin
newborns
supports this hypothesis. As shown in Table 2, 11 sera
from new-
borns whose mothers were seronegative had equivocal results
and
38 newbornswhosemothershad equivocal results tested
antibody-
positive. Thus, a higher prevalence of antibodies in the cord
blood
sera can be the consequence of actively transported antibodies
if
maternalconcentrationswere below thedetectable assay levels.
No
significant association of antibody concentration with
gestational
age was found for either influenza virus A or B. This is most
likely
because only 10 out of 209 babies were born at a gestational age
of
≤37 weeks and only 3 after
-
8/18/2019 Immunity 12
4/4
164 P. Wutzler et al. / Journal of Clinical Virology 46
(2009) 161–164
their offspring, but has been reported for antibodies to
measles,
mumps, rubella, parainfluenza and varicella-zoster viruses, as
well
astetanusantitoxin, diphtheriaantitoxinandanti-Bordetella
pertus-
sis antibodies.23–28 Specific receptor-mediated binding of
the Fc
portion of IgG at the maternal surface of the placenta has
been
considered part of the mechanism involved in neonatal
antibody
levels.29 Why newborns who were delivered by vacuum extrac-
tionhad significantly lower antibodylevels
thanneonatesdelivered
spontaneously or by caesarean section cannot be explained.
Since
only 10 newborns delivered by vacuum extraction were
included
in this study, theanalysis of different factors that could have
biased
this result is not possible.
The high prevalence of influenza A virus-specific antibodies
in pregnant women suggests high incidence of recent
infection.
Depending on the persistence of ELISA antibodies, theseresults
cor-
respond to the epidemiological situation in 1999 and 2000
when
the sera included in this study were taken from the mothers
and
their newborns. During these seasons, there was a moderate
activ-
ityof influenzaA viruses ofthe subtype H3N2 inGermany.30,31
Since
women at child-bearing agehaveincreased exposureto
youngchil-
dren who have higher infection rates of influenza than
adults,32,33
it is likely that these women have an increased risk of
becoming
infected with influenza. However, this does not apply to
women
having theirfirst child. Theconsequenceof
thehighantibodypreva-lence of pregnant women is that nearly all
neonates also acquired
antibodies. In the case of influenza, passive immunity is
important
sincecurrentlyavailable influenza vaccines arenot
indicatedbelow
6 months of age.
In contrast, there was a lower prevalence of maternal
antibody
against influenza B virus, which also reflects the
epidemiological
data reported in 1999 and 2000 in Germany. Whereas one third
of all isolated influenza viruses could be classified as
influenza B
viruses in 1999, only a few influenza B virus isolates were
obtained
in the following season.30,31,34 This would lead to a relatively
low
number of booster infections caused by the influenza B virus
dur-
ing these seasons. Although less common and usually
associated
with lower mortalitythaninfluenza A, influenza B
cancausesignifi-
cant morbidityand mortalityin neonates and other
children.11,35,36Offering influenza vaccine to pregnant women, who
will deliver
during influenza season, may potentially reduce the frequency
and
severity of this neonatal disease.
Conflict of interest
There are no competing interests.
Ethical approval
The work has been approved by the Ethical Committee of the
University of Jena (Germany) and subjects gave informed
consent
to the work.
Acknowledgments
This work was supported by grants of the GlaxoSmithKline
GmbH & Co. KG, Munich, Germany.
References
1. Englund JA. Maternal immunization with inactivated influenza
vaccine: ratio-nale and
experience. Vaccine 2003;21:3460–4.
2. Griffiths PD, Ronalds CJ, Heath RB. A prospective study of
influenza infectionsduring pregnancy. J Epidemiol Community
Health 1980;34:124–8.
3. MulloolyJP,BarkerWH, Nolan TF. Riskof acute
respiratorydiseaseamongpreg-nant women during influenzaA epidemics.
Public Health Rep 1986;101:205–11.
4. Neuzil KM, Reed GW, Mitchel EF, Simonsen L, Griffin MR.
Impact on influenzaon acute cardiopulmonary hospitalizationsin
pregnant women. Am J Epidemiol1998;148:1094–102.
5. HarrisJW. Influenzaoccurring in pregnant women: statistical
study of thirteenhundred and fifty
cases. JAMA 1919;72:978–80.
6. Freeman DW, Barno A. Deaths fromAsian influenzaassociated
withpregnancy. Am J Obstet Gynecol 1959;78:1172–5.
7. ACOG Committee on Obstetric Practice. ACOG Committee Opinion.
Influenzavaccinationand treatmentduring pregnancy. Obstet Gynecol
2004;104:1125–6.
8. Centersfor DiseaseControl andPrevention. Preventionand
control ofinfluenza.Recommendations of the Advisory Committee on
Immunization Practice.
MMWR 2007;56:1–54.9. Robert Koch-Institut. Empfehlungen der
Ständigen Impfkommission (STIKO)
am Robert Koch-Institut/Stand: Juli 2007. Epidemiol
Bull 2007;30:267–86.10. Zaman K, Roy E, Arifeen SE, Rahman M,
Raqib R, Wilson E, et al. Effective-
ness of maternal influenza immunization in mothers and
infants. N Engl J Med2008;359:1555–64.
11. Munoz FM. Influenza virus infection in infancy and early
childhood. Paediatr Respir Rev 2003;4:99–104.
12. Yusuf K, Soraisham AS, Fonseca K. Fatal influenza B virus
pneumonia ina preterm neonate: case report and review of the
literature. J Perinatol2007;27:623–5.
13. Glezen WP, Decker M, Perrotta DM. Survey of underlying
conditions of per-sonshospitalizedwith acute respiratory disease
during influenzaepidemics inHouston, 1978–1981. Am Rev Respir
Dis 1987;136:550–5.
14. Glezen WP, Greenberg SB, Atmar RA, Piedra PA, Couch RB.
Impact of respi-ratory virus infections on persons with chronic
underlying conditions. JAMA2000;283:499–505.
15. Rothbarth PH, Groen J, Bohnen AM, de Groot R, Osterhaus AD.
Influenza virusserology—a comparative study. J Virol
Methods 1999;78:163–9.
16. Julkunen I, Pyhälä R, Hovi T. Enzyme immunoassay, complement
fixation andhemagglutination inhibition tests in the diagnosis of
influenza A and B virusinfections.Purified hemagglutininin
subtype-specific diagnosis. J VirolMethods1985:75–84.
17. Koskinen P, Vuorinen T, Meurman O. Influenza A and B virus
IgG and IgMserology by enzyme immunoassays. Epidemiol
Infect 1987;99:55–64.
18. Voeten JT, Groen J, van Alphen D, Claas EC, de Groot R,
Osterhaus AD, et al.Use of recombinant nucleoproteins in
enzyme-linked immunosorbent assaysfor detection of virus-specific
immunoglobulin A (IgA) and IgG antibodies ininfluenza virus A- or
B-infected patients. J Clin
Microbiol 1998;36:3527–31.
19. Londo DR, Davis AR, Nayak DP. Complete nucleotide sequence
of the nucleo-protein gene of influenza B virus. J
Virol 1983;47:642–8.
20. Watanabe S, Imai M, Ohara Y, Odagiri T. Influenza B virus
BM2 protein is trans-ported throughthe trans-Golgi networkas
anintegral membrane protein. J Virol2003;77:10630–7.
21. Tompkins SM, Zhao ZS, Lo CY, Misplon JA, Liu T, Ye Z, et al.
Matrix protein 2vaccination and protection against influenza
viruses, including subtype H5N1.Emerg Infect
Dis 2007;13:426–35.
22. Cinatl Jr J, Michaelis M, Doerr HW. The threat of avian
influenza A (H5N1). PartIV. Development of vaccines. Med
Microbiol Immunol 2007;196:213–25.23. SatoH,Albrecht P,
ReynoldsDW, StagnoS, Ennis FA.Transferof measles,mumps,
and rubella antibodies from mother to infant. Am J Dis
Child 1979;133:1240–3.
24. Asano Y, Hiroishi Y, Itakura N, Hirose S, Kajita Y, Suga S,
et al. Placental trans-fer of IgG subclass-specific antibodies to
varicella-zoster virus. J Med Virol1988;26:1–6.
25. Wilczynski J, Lukasik B. Transplacental transfer of
antibodies to some respira-tory viruses. Acta Microbiol
Pol 1994;43:347–58.
26. Malek A, Sager R, SchneiderH. Transportof proteins acrossthe
human placenta. Am J Reprod Immunol 1998;40:347–51.
27. Sauerbrei A, Groh A, Bischoff A, Prager J, Wutzler P.
Antibodiesagainst vaccine-preventable diseases in pregnant women
and their offspring in Eastern part of Germany. Med
Microbiol Immunol 2002;190:167–72.
28. Sauerbrei A, Wutzler P. Placental boost to varicella-zoster
antibodies in thenewborn. J Perinat
Med 2002;30:345–8.
29. Friden BE, Makiya R, Nilsson BM, Holm S, Stigbrand TI. The
human placen-tal immunoglobulin G receptor and immunoglobulin G
transport. Am J Obstet
Gynecol 1994;171:258–63.30. Robert Koch-Institut.
Influenza/ARE: Einschätzung der Saison 1998/99. Epi-
demiol Bull 1999;18:131–3.31. Robert Koch-Institut.
Vorbereitungauf die Influenza: Start der Impfaktion. Epi-
demiol Bull 2000;37:295–7.32. Heikkinen T, Booy R, Campins
M, Finn A, et al. Should healthy children be
vaccinated against influenza? A consensus report of summits of
independentEuropean vaccination experts. Eur J
Pediatr 2006;165:223–8.
33. Wutzler P. Influenza-Schutzimpfung—Wo steht Deutschland?
Dtsch MedWochenschr 2006;131:453–7.
34. Robert Koch-Institut. Influenza—aktuelle Situation.
Epidemiol Bull 2000;6:49.
35. Troendle JF, Demmler GJ, Glezen WP, Finegold M, Romano MJ.
Fatal influenza Bvirus pneumonia in pediatric
patients. Pediatr Infect Dis J 1992;11:117–21.
36. van den Dungen FA, van Furth AM, Fetter WP, Zaaijer HL, van
Elburg RM. Fatalcase of influenza B virus pneumonia in a preterm
neonate. Pediatr Infect Dis2001;20:82–4.