Embed Size (px)
DESCRIPTION
Immunity: The New Priority for the Modern Patient. Kerry Bone Co-Founder and Director Research and Development MediHerb Adjunct Associate Professor, University of New England, Australia. The Immune Challenge. Modern epidemics, viruses jumping species Antibiotic-resistant bacteria - PowerPoint PPT Presentation
Citation preview

Immunity: The New Priorityfor the Modern Patient
Kerry BoneCo-Founder and Director Research and DevelopmentMediHerbAdjunct Associate Professor,University of New England, Australia

The Immune Challenge
• Modern epidemics, viruses jumping species
• Antibiotic-resistant bacteria
• High costs, long lead times for new antibiotic drugs
• Antibiotic-induced changes in human flora and the modern epidemic of Clostridium perfringens
• The rising incidence of atopic allergy, for example anaphylaxis to peanuts
• The rising incidence of many autoimmune diseases, including type 1 diabetes
• Immunosenescence2

Antibiotic Resistance
• According to the World Health Organization(March 2012), “Antimicrobial resistance threatens a return to the pre-antibiotic era”
• 440,000 new cases of multidrug-resistant tuberculosis (MDR-TB) emerge annually (150,000 deaths). MDR-TB reported in 64 countries to date
• Resistance to earlier generation antimalarial medicines is widespread in most malaria-endemic countries
http://www.who.int/mediacentre/factsheets/fs194/en/index/html 3

Antibiotic Resistance
• Many hospital-acquired infections are causedby highly resistant bacteria such as methicillin- resistant S. aureus (MRSA) and vancomycin-resistant enterococci(VRE)1
• In the US, more than 18000 peopledie each year (50 every day!) from MRSA2 and up to 30000 from antibiotic-resistant Clostridium3
1 http://www.who.int/mediacentre/factsheets/fs194/en/index/html2 Klevens RM et al. JAMA 2007; 298(15): 1763-17713 Tenover FC. http://www.hhs.gov/asl/testify/2008/06/t20080624e.html accessed July 4,
2012
4

The Post-Antibiotic Era
• Dr Margaret Chan, director general of WHO:“A post-antibiotic era means, in effect, an end to modern medicine as we know it. Things as common as Strep. throat or a child’s scratched knee could once again kill.We are losing our first-line antimicrobials. Replacement treatments are more costly, more toxic, need much longer durations of treatment, and may require treatment in intensive care units.”
http://www.who.int/dg/speeches/2012/amr_20120314/en/index.html access July 4 2012 5

Three Key Immune Herbs
• Echinacea angustifolia and/or Echinacea purpurea root, mainly for prevention and to counter immunosenescence
• Andrographis paniculata for acute viral or bacterial infections
• Astragalus membranaceus for chronically depleted immunity and supporting the immune system under adverse conditions, especially the immune cells themselves. Also for immunosenescence
6

My Favorite Herb• Echinacea root has much to offer the modern
naturopathic physician, but it is so confused and misunderstood
• There are a multitude of products using different species, plant parts and manufacturing methods
• A lack of consensus over what phytochemicals in Echinacea are responsible for its immune activity
• A rudimentary understanding of its exact mode of action on the immune system, but with intriguing new developments
• Many myths about how Echinacea should and should not be used
7

A Brief History of Echinacea
• Information about the therapeutic value of Echinacea first came from Native American tribes
• Their use of Echinacea was then adopted by the Eclectic physicians
• By 1921 Echinacea (specificallythe root of E. angustifolia) wasby far the most populartreatment prescribed byEclectic physicians
Wagner H. Z Phytother 1996; 17(2): 79-958

9
Lloyd JU. Echinacea angustifolia. Lloyd Brothers, Cincinnati, 1923. In: Bauer R, Wagner H. Echinacea: Handbuch für Ärzte, Apotheker und andere Naturwissenschaftler. WVG, Stuttgart, 1990, p 16.

• The Eclectics were responsible for Echinacea’s reputation as an immune herb and they used the root extracted in a high percentage of alcohol (lipophilic extracts or tinctures)
• They felt that the tingling (due to alkylamides) was the indicator of good quality
• In Europe during the 1930s the German herbalist Madaus introduced E. purpurea tops as a stabilized fresh juice (hydrophilic tincture)
• This eventually led to the investigation of polysaccharides as Echinacea active componentsBauer R, Wagner H. In Wagner H, Farnsworth NR eds. Economic and Medicinal Plant Research, Vol 5, Academic Press, London, 1991.
A Brief History of Echinacea
10

How the EclecticsUsed Echinacea Root
Abscesses DiphtheriaAlopecia DysenteryAnthrax EczemaAppendicitis EmpyemaBed sores Epidemic influenzaBee sting ErysipelasBoils, Carbuncles Exophthalmic goitreCancer FeversChicken-pox GangreneCholera GonorrheaChronic bronchitis ImpetigoChronic glandular indurations ImpotenceChronic malaria Intestinal indigestionChronic ulcerations Leg ulcersDiabetes mellitus Leucorrhea 11

How the EclecticsUsed Echinacea Root
Malaria SepticemiaMastitis, acute and chronic Small poxMeasles Snake biteMeningitis Spider bitePsoriasis SyphilisPuerperal infection TetanusPulmonary gangrene TonsillitisPurulent salpingitis Tubercular abscessesQuinsy Typhoid feverRabies Ulcerative stomatitisRenal hemorrhage Urethral infectionRespiratory catarrh VulvitisScarlet fever Wasp stingScorpion sting WoundsSeptic injuries 12

How the EclecticsUsed Echinacea Root
References for the previous slides• Felter HW, Lloyd JU. King’s American Dispensatory.
18th Edn, 3rd revision, Volume 1. First published 1905, reprinted Eclectic Medical Publications, Portland, 1983.
• Ellingwood F, Lloyd JU. American Materia Medica, Therapeutics and Pharmacognosy. 11th Edn. Naturopathic Medical Series: Botanical Volume 2. First published 1898, reprinted Eclectic Medical Publications, Portland, 1983.
13

How the EclecticsUsed Echinacea Root
Points of Note• The Eclectics often used quite high doses of
Echinacea root• They were not adverse to using Echinacea root
long-term• For example according to Ellingwood, Echinacea
was recommended for the following chronic conditions: cancer, chronic mastitis, chronic ulceration, tubercular abscesses, chronic glandular indurations and syphilis
• With regard to syphilis, Ellingwood writes: “The longest time of all cases yet reported, needed to perfect the cure, was nine months.”
Ellingwood F. American Materia Medica, Therapeutics and Pharmacognosy, EclecticMedical Publications, Portland, 1993.
14

Early Encounters withEchinacea: Real or Not?
• As a student at the Jacka’s Naturopathy clinic, Melbourne, Australia 1976
• As a herbal student, Tunbridge Wells, UK 1982
• At a US herbal trade show, 1987• Real Echinacea gives you “asthma”, 1988
15

Learning the Power ofReal Echinacea
• The Eclectic writings in King’s Dispensatory and Ellingwood, early 1990s
• Teaching Echinacea tonaturopathy undergraduatesand student feedback, early 1990s
• Feedback from patients andlearning the power of prevention,early 1990s
16

The Four Key Echinacea Myths
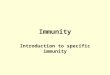
1. Echinacea can only be taken for short periods. Long-term use will wear out the immune system (tachyphylaxis)
2. The polysaccharides are the true active constituents, hence the root must be extracted with water, or better still use only the tops
3. Echinacea is the best herb to treat winter viral infections once they have occurred
4. Echinacea is dangerous in autoimmune disease
17

-40
-20
0
20
40
60
80
100
120
140
160
2 3 4 5 6 7 8 9 10 11
Echinacea
Placebo
Time(days)
Active or placebo3 x 30 drops per day
% Phagocytosis
Echinacea Root: Shortor Long-Term
Jurcic K et al. Z Phytother 1989; 10: 67-70 18

Problems with Polysaccharides
• Polysaccharides (PS) in Echinacea (tops or root) have received research attention as active components
• However, much of this research is in vitro and has been confounded by endotoxin (lipopolysaccharide) contamination of the samples used1
• The term “polysaccharide” is generic and includes starches and other potentially inert plant compounds, but these are often measured by the crude analytical techniques used
1 Tamta H et al. J Agric Food Chem 2008; 56(22): 10552-10556 19

Problems with Polysaccharides
• Hence commercial Echinacea products claiming quantified levels of PS should be viewed with considerable caution
• Research has found that true polysaccharides are extremely difficult to extract from Echinacea (top or root) and they are unstable in the harvested dried plant
• Ethanol strengths 40% or higher cannot extract the PS from Echinacea, while less than 4% of PS1 and 17% of PS2 was extracted by hot water from any dried plant partStuart DL et al. Optimisation of polysaccharides in processed Echinacea purpurea. RIRDC Publication No. 04/118, 2004. 20

Problems with Polysaccharides
• PS are common to all plants, being components of plant cell walls
• PS are large molecules with limited bioavailability
• The Eclectics never gave EchinaceaPS to patients, since they onlyused high ethanol extracts
21

Echinacea Root:What is Active?
• Echinacea root extracted with alcohol mainly contains alkylamides and caffeic acid derivatives
• Herbal in vitro research is meaningless if the extracts being tested do not contain bioavailable phytochemicals
• What is active must be bioavailable, what is bioavailable must be active: the model of undertaking all quality research on herbs
• But subsequent clinical proof of activity of any product optimized to these phytochemicals is paramount
22

Echinacea Root: Pharmacokinetics
Study Design:11 healthy individuals Age: 18 to 26 yearsBMI: 19 to 30Blood samples takenover 12 hours
Dose:4 Echinacea root tablets as a single dose
23

What Compounds WereFound in Bloodstream
• No caffeic acid conjugates• No caffeic acid conjugate degradation products• No alkylamide degradation products• No polysaccharides
The only compounds identified in human plasma were alkylamides from the Echinacea ingested, at approximately the same ratio as the initial product tested
Matthias A, Addison RS, Penman KG, Bone KM et al. Life Sci 2005; 77: 2018-2029 24

Echinacea - Liquid vs Solid Dose Pharmacokinetics
0
50
100
150
200
0 60 120 180 240 300 360
Time (m in)
Die
ne
(ng
/mL
pla
sma)
Matthias A, Addison RS, Agnew L, Bone KM et al, Phytomedicine 2007; 14(9): 587-590
25

Liver First Pass Metabolism• The pharmacokinetic study suggested that
alkylamides were being degraded by the liver on first pass after absorption in the GIT
• When liver decomposition of alkylamides was investigated a surprisingfact was found
• Some alkylamides inE. angustifolia aredegraded at a slowerrate and protect otheralkylamides (found inE. angustifolia and E. purpurea) from degrading
26

Enhancing Bioavailability
• 2-ene protects the 2,4-diene
• increasing amounts of 2-ene alkylamide gives less degradation of the 2,4-diene
0
20
40
60
80
100
0 20 40 60 80
Time (min)
% O
rigi
nal [
247]
0.000.050.501.262.085.00
Matthias A, Gillam EMJ, Penman KG, Bone KM et al. Chem Biol Interact 2005; 155: 62-70 27

What Do Echinacea Alkylamides Do?
• Exert anti-inflammatory effects• Some bind strongly to cannabinoid receptors• Others may inhibit breakdown of endogenous
cannabinoids• Possibly upregulate dendritic cell maturation• Possibly responsible for positive effects on
natural killer (NK) cell function and numbers and increased white cell phagocytic activity seen in several in vivo studies
• Possibly responsible for effects on heat shock proteins seen in human studiesBone KM, Mills SY. Principles and Practice of Phytotherapy: Modern Herbal Medicine.Elsevier, UK. 2nd Edition, In press.
28

Cannabinoid Receptors
• CB1 receptors are highly localized in the central nervous system (CNS) and are believed to primarily modulate behavior
• CB2 receptors predominate inimmune tissues outside theCNS, especially the spleen,and are believed to modulateimmune function
• Echinacea alkylamides mainlybind to CB2 receptors
Ralevic V. Cannabinoid modulation of peripheral autonomic and sensory neurotransmission. Eur J Pharmacol 2003; 472(1-2): 1-21 29

CB2 Binding of Alkylamide Isomers
Isomer Ki CB2 (nM) ZZ 57 ± 8.5 ZE 9044 ± 2985 EZ 4535 ± 711 EE > 100000
Matovic N, Matthias A, Gertsch J, Bone KM et al. Org Biomol Chem 2007; 5(1): 169-174
Using alkylamides supplied from Australia it has been found that the tetraene isomers vary in terms binding to CB receptors, with the ZZ isomer showing a higher affinity than anandamide
Alkylamides from other plants do NOT bind to CB2
30

Alkylamides and Anandamide
Anandamide: an endogenous cannabinoid
NHCH3
CH3
O
CH3
Z,Z tetraene alkylamide from Echinacea
NHOH
O
CH3
31

CB2 Activation: Subtle but Profound
• A lipophilic extract of E. purpurea strongly stimulated TNF mRNA synthesis in peripheral monocytes in vitro
• TNF mRNA was upregulated (around 8-fold) by the Echinacea extract over a time-span of 24 hours, but the constituent protein level (of TNF) was not changed
• However, LPS-stimulated TNF production was potently modulated by Echinacea, with inhibition (around 40%) during the first 20 hours, and a subsequent prolongation of TNF production
Gertsch J, Schoop R, Kuenzle U et al. FEBS Letters 2004; 577(3): 563-56932

• These effects were produced by the interaction of Echinacea alkylamides with the CB2 receptors on the monocytes
• The results of this study suggest that Echinacea works more as a facilitator of the immune response. In resting monocytes it prepares them for a quicker response by inducing TNF mRNA
• However, in overstimulated monocytes (as in the case of LPS) it first reduces, but then extends their response in terms of TNF production
CB2 Activation: Subtle but Profound
33

Echinacea: A Miracle Herb?• In an extraordinarily entitled paper:
“Echinacea: a Miracle Herb against Aging and Cancer?”, Canadian scientist Dr Sandra Miller reviewed her research on Echinacea, specifically Echinacea purpurea root1
• In healthy young adult mice, oral doses of Echinacea purpurea root (0.45 mg per 25 g body weight, similar to human dose rates) stimulated NK cell production by bone marrow in the first 7 days which resulted in significantly higher levels (around 25% more) of NK cells in the spleen by 2 weeks2
1 Miller SC. eCAM 2005; 2(3): 309-3142 Sun LZ-Y, Currier NL, Miller SC. J Altern Complement Med 1999; 5: 437-446
34

Echinacea Boosts NK Cells• In addition, the ‘helper’ or accessory cells
for NK cells, the monocytes, were also increased by 25%
• The Echinacea treatment influenced no other white blood cell counts
• Polysaccharides, even by injection, were not responsible for this effect
• Dr Miller feels that alkylamides are largely responsible for the effect (personal communication)
• This research tends to shift the focus for Echinacea to innate immunity and emphasizes its preventative roleCurrier NL, Lejtenyi D, Miller SC. Phytomedicine 2003; 10: 145-153
35

Echinacea Reverses Agingof Innate Immunity
• NK cells decline in number and function with age and this is thought to be one factor behind the increase of various cancers with age
• Experiments conducted in healthy, elderly mice found that 2 weeks of oral doses of Echinacea returned NK cell numbers in bonemarrow and spleen to the levels ofyoung adults and also resurrectedthe functional capacity (target cellbinding, lysis) of these cells1
1 Currier NL, Miller SC. Exp Gerontol 2000; 35: 627-639 36

Echinacea Reverses Agingof Innate Immunity
• On this result Dr Miller writes1:“These observations appear to apply uniquely to this herb since we could never rejuvenate the NK cell-mediated component of the immune system in elderly mice by any of the other typical NK cell enhancers….”
• In addition for mice fed Echinacea purpurea root from 7 weeks of age to 13 months lifespan was significantly extended compared to controls2
1 Miller SC. eCAM 2005; 2(3): 309-3142 Brousseau M, Miller SC. Biogerontology 2005; 6: 157-163 37

Heat Shock Proteins
• Heat shock proteins (HSPs) are molecular chaperones that bind to large proteins to facilitate their folding (during synthesis) and to prevent mis-folding (after synthesis)
• While basal levels of HSPs exist within cells, they are further induced by temperature shock or other stressors
• They act to protect cells from protein denaturation and possible death under hostile conditions
• Certain HSPs within immune cells also appear to facilitate the immune response (antigen presentation) 38

Heat Shock Proteins
• Extracellularly, HSPs appear to act like cytokines (as “moonlighting proteins”) and can modulate immune responses
39Chen T, Cao X. Eur J Immunol 2010; 40(6): 1541-1544Henderson B. Cell Biochem Funct 2010; 28(1): 1-14

Echinacea Root and HSPs• In an open-label pilot trial, 11 healthy volunteers
were evaluated at baseline (day 1) and on day 15 after consuming 2 Echinacea root tablets/day (standardized to 4.4 mg alkylamides) for 14 days1
• Echinacea root markedly enhanced (by about 50%) the increase in white cell heat shock protein (hsp70) expression after mild heat shock (p=0.029)
• White cell counts were mildly increased (p=0.043) and there was a preventative effect against free radical induced erythrocyte hemolysis (p=0.006)
1 Agnew LL et al. J Clin Pharm Ther 2005; 30(4): 363-369 40

Echinacea Root and HSPs• A follow-up open-label trial in 24 healthy
volunteers used the same design, except the Echinacea root dose was twice the above1
• While Echinacea did not significantly change basal hsp70 expression in lymphocytes, it increased CD4, CD8 and NK cell stress-induced hsp70 expression
• The effect was most marked in NK cells (p<0.05)• This implies that Echinacea root may play a role
in activating and protecting the immune system via HSPs when the body encounters a challenge, such as a virus
1 Agnew L et al. Planta Med 2010; 76(12): P629, 135441

The Four Key Echinacea Myths
1. Echinacea can only be taken for short periods. Long-term use will wear out the immune system (tachyphylaxis)
2. The polysaccharides are the true active constituents, hence the root must be extracted with water, or better still use only the tops
3. Echinacea is the best herb to treat winter viral infections once they have occurred
4. Echinacea is dangerous in autoimmune disease
42

Echinacea Root for the Common Cold
• In a large and well-designed US trial, the impact of taking Echinacea root shortly after common cold onset was investigated
• The active intervention was10.2 g of dried Echinacearoot during the first 24 h,and then 5.1 g/day for thenext 4 days
• Primary outcomes assessedwere global severitythroughout the illness and duration of infection
Barrett B, Brown R, Rakel D et al. Ann Intern Med 2010; 153(12): 769-777
43

No Pill Group
Unblinded Echinacea
Group
Blinded Placebo Group
Blinded Echinacea
Group
Whole Group
Participants (n) 173 181 176 183
Median global severity
220 195 206 193
Median duration (d)
6.42 6.16 6.87 6.34
Herbs within 24 h
Participants (n) 80 97 79 95
Median global severity
221 177 199 196
Median duration (d)
6.66 6.15 6.38 6.0744
Echinacea Root for the Common Cold
Barrett B, Brown R, Rakel D et al. Ann Intern Med 2010; 153(12): 769-777

Prevention is Better Than Cure
• In a study presented by the late Dr Anna Macintosh at the 1999 Convention of the American Association of Naturopathic Physicians, an Echinacea root formulation was compared against a herbal adaptogenic formulation and a placebo in the prevention of winter colds over a 90-day period1
• The trial recruited 260 medical students who were under stress from their studies
• The placebo group averaged an infection rate of 10%, whereas this dropped to as low as 2% by day 70 (p=0.013) in the Echinacea group
1 McIntosh A et al. AANP Convention, Coeur d’ Arlene, 1999.45

Echinacea and Long-haul Flights• A randomized, double blind, placebo-controlled
clinical trial was undertaken with 175 participants travelling return from Australia to North America, Europe or Africa for 1 to 5 weeks
• Active tablets each contained extract from 1.275 g Echinacea root (4.4 mg alkylamides)
• Priming dose was 2/day, travel dose was 4/day and dose when ill was 6/day
• The placebo group exhibited significantly higher average respiratory infection symptom score (around double) compared with the Echinacea group (p<0.05) after return from travelTiralongo E et al. Evid Based Complement Alternat Med 2012; 2012: 417267
46

Echinacea Root and Air Travellers
47Tiralongo E et al. Evid Based Complement Alternat Med 2012; 2012: 417267

The Four Key Echinacea Myths
1. Echinacea can only be taken for short periods. Long-term use will wear out the immune system (tachyphylaxis)
2. The polysaccharides are the true active constituents, hence the root must be extracted with water, or better still use only the tops
3. Echinacea is the best herb to treat winter viral infections once they have occurred
4. Echinacea is dangerous in autoimmune disease
48

Echinacea and Autoimmunity• The caution for Echinacea in autoimmunity
was based on theoretical grounds and the few isolated adverse events hardly provide reasonable grounds for a contraindication
• Mice with autoimmune diabetes did not show adverse effects when fed Echinacea purpurea root1
• In a controlled clinical trial, patients with autoimmune uveitis were able to reduce their time on prednisone when given Echinacea purpurea2
• The role of immune herbs in autoimmunity will be revisited later in this seminar
1 Delorme D, Miller SC. Autoimmunity 2005; 38(6): 453-4612 Neri PG et al. J Ocul Pharmacol Ther 2006; 22(6): 431-436
49

Echinacea: Conclusions and Recommendations
Preferred Preparations and Key Quality Markers•The preferred parts of Echinacea to use are the roots of E. angustifolia combined with E. purpurea•The alkylamides are the important quality marker compounds (even active constituents) and MUST be present in adequate quantities•Doses must be adequate: at least 2.5 g of a root combination per day (temporarily to ward off infection) 50

Echinacea: Conclusions and Recommendations
The Mode of Action• Alkylamides are bioavailable, importantly tablet
and liquid preparations are equipotent if appropriately formulated
• Alkylamides in E. angustifolia help inhibit the rapid liver breakdown of alkylamides from E. purpurea
• Echinacea root boosts innate immunity with continued use and modulates immune activity during an acute phase response
• Mechanisms are complex but probably involve (among others) CB2 agonism and HSP induction
51

Echinacea: Conclusions and Recommendations
Best Clinical Practice• Echinacea root is better used as a preventative
for infections, although traditionally it does have a role for resolving chronic infections
• Long-term use of Echinacea root is in fact not only beneficial, it is necessary for its full immune effects
• There is no reason why Echinacea root should be contraindicated in autoimmune disease, in fact it may be beneficial (see later in this seminar)
52

Andrographis and Winter Infections
• Two systematic reviews of the role of Andrographis in the clinical management of upper respiratory tract infections have been published
• In one review, 7 double blind, controlled trials (n=896) that met inclusion criteria for evaluation of efficacy were considered
• All trials scored at least 3(out of a maximum of 5)for methodological qualityon the Jadad scale
53

Andrographis and Winter Infections
• Collectively, the data suggested that Andrographis was superior to placebo in alleviating the subjective symptoms of uncomplicated upper respiratory tract infection. There was also preliminary evidence of a preventative effect
• Adverse events reported followingthe herb administration weregenerally mild and infrequent1
• In the second review, 433 patientsfrom 3 trials were included in themeta-analysis
1 Coon JT, Ernst E. Planta Medica 2004; 70(4): 293-298
54

Andrographis and Winter Infections
• Andrographis either alone or in combination with Eleutherococcus was more effective than placebo in the treatment of uncomplicated acute upper respiratory tract infection1
• Doses used were typically upto 1000 mg/day of extract(about 6 g of herb) delivering50 to 60 mg/day andrographolides
1 Poolsup N, Suthisisang C, Prathanturarug S et al. J Clin Pharm Ther 2004; 29(1): 37-45
55

Andrographis and Autoimmunity
• A 14-week randomized, double blind, placebo-controlled clinical trial in 60 patients examined the impact of a 75% ethanolic extract of Andrographis (300 mg/day corresponding to 3 g of herb and containing 90 mg of andrographolides) in active rheumatoid arthritis1
• All trial patients were given methotrexate and were allowed to take prednisone or chloroquine in stable doses if already prescribed
1 Burgos RA, Hancke JL, Bertoglio JC et al. Clin Rheumatol 2009; 28(8): 931-946
56

Andrographis and Autoimmunity
• Compared with baseline there were significant improvements observed in the Andrographis group by week 14
• However, compared with the placebo group these changes in RA were not statistically significant
57

Andrographis and Autoimmunity
• A randomized, double blind trial (n=108) was conducted at five centers in Shanghai to compare a standardized extract of Andrographis with the nonsteroidal anti-inflammatory drug mesalazine(4.5 g/day, in slow release form) in patients with mildly to moderately active ulcerative colitis (confirmed by colonoscopy)1
• Treatment with Andrographis extract demonstrated similar efficacy to mesalazine but with fewer adverse events
1 Tang T, Targan SR, Li ZS et al. Aliment Pharmacol Ther 2011; 33(2): 194-20258

Astragalus and Immunity
• In an open, randomized clinical trial, 115 patients with leucopenia received a high dose of a concentrated Astragalus preparation (equivalent to 30 g/day of Astragalus) or a low dose (equivalent to 10 g/day) over a period of 8 weeks
• There was a significant rise of average white blood cell (WBC) counts in both groups after treatment (p<0.001)
• The average WBC count for the high-dose group was significantly higher than for the low-dose group (p<0.05)
Weng XS. Chung Kuo Chung Hsi I Chieh Ho Tsa Chih 1995; 15(8): 462-46459

Astragalus and Cancer Therapy
• A meta-analysis of 34 randomized clinical trials involving patients with non-small-cell lung cancer treated with platinum-based chemotherapy and Astragalus-based Chinese herbs suggested a benefit from the combination1
• Most trials involved formulas featuring Astragalus, but two were of Astragalus alone. The herbs were administered by injection in around one third of the trials
1 McCulloch M, See C, Shu XJ et al. J Clin Oncol 2006; 24(3): 419-43060

Astragalus and Cancer Therapy
• 12 trials measuring such outcomes reported significantly lower mortality rates after 12 months when Astragalus was combined with chemotherapy (risk ratio 0.67)
• 9 studies reported significantly lower mortality rates after 24 months when Astragaluswas combined with chemotherapy(risk ratio 0.73)
• Most of the studies included wereof low methodological quality
61

Astragalus and Cancer Therapy
• A Cochrane review identified four relevant trials where a decoction of Astragalus and a formulation featuring Astragalus was combined with chemotherapy in patients with colorectal cancer
• Chemotherapy-induced nausea, vomiting, and leucopenia were all decreased by concomitant administration of Astragalus decoction, and immune function was improved
• The trials were of low quality, suggesting larger, more rigorous trials are needed to confirm these results
Taixiang W, Munro AJ, Guanjian L. Cochrane Database Syst Rev (1):CD004540, 200562

Astragalus and Autoimmunity
• A US group of doctors described 2 separate cases (published 3 years apart) of complete remission of idiopathic membranous nephropathy (IMN, probably autoimmune in origin) after therapy with Astragalus
• The first case described a 77-year-old woman with nephrotic syndrome secondary to IMN who was largely unresponsive to conventional treatments. After beginning Astragalus (15 g/day as part of the formulation Shen-Yan Siwei Pian) there was a marked decrease in proteinuria
Ahmed MS, Hou SH, Battaglia MC et al. Am J Kidney Dis 2007; 50(6): 1028-103263

Astragalus and Autoimmunity• Nephrotic syndrome recurred after a
temporary cessation of the formulation, with complete remission after its reintroduction
• Remission persisted even after stopping the herbal treatment
• The second case was a 63-year-old man with nephrotic syndromedue to IMN who took 15 g/dayAstragalus on its own1
1 Leehey DJ, Casini T, Massey D. Am J Kidney Dis 2010; 55(4): 772 64

Overall Conclusions
• The post-antibiotic era is coming• Immune herbs have much to offer the modern
patient and if used in appropriate doses of quality preparations can achieve dramatic results
• The main value of Echinacea root is as a preventative, and its informed use can be practice building
• Astragalus and Andrographis also have important roles, the latter for acute infections and the former for chronically depressed immunity 65

Echinacea Research Collaborators
University of Queensland research groups • Prof Istvan Toth • Dr JJ De Voss• Dr E Gillam • Prof R Dickenson and Prof W HooperSouthern Cross University research groups • A/Prof D Leach • Prof S Meyers University of New England research group • Prof K Watson Swiss Federal Institute of Technology • Dr J GertschUniversity of Wisconsin • Dr Bruce Barrett 66

Acknowledgments with Thanks
Echinacea research team•A/Prof Reg Lehmann•Dr Anita Matthias•Dr Kerry Penman
Contribution to presentation•Berris Burgoyne ND
67