Embed Size (px)
Citation preview
The Christie NHS Foundation Trust
Immuno-Oncology ofRenal Cancer
Dr Fiona ThistlethwaiteConsultant Medical Oncologist and Honorary Senior Lecturer
The Christie NHS Foundation Trust and University of Manchester
•
The Christie NHS Foundation Trust
Disclosures
Advisory role
Nordic, BMS
Travel, accommodation, Expenses
Ipsen, BMS
Research collaborations
Adaptimmune
MedImmune
The Christie NHS Foundation Trust
Introduction• Renal cell carcinoma (RCC) accounts for
2-3% malignant diseases in adults
• 115,000 new cases in Europe in 2012
• Nephrectomy can be curative for earlystage disease but most patients developmetastatic disease
• 30% at diagnosis• 30% relapse
• RCC has long been recognized as apotential target for immunotherapy
• Observation that it is one of themost common tumour types toundergo spontaneous regression(Bumpus 1928)
The Christie NHS Foundation Trust
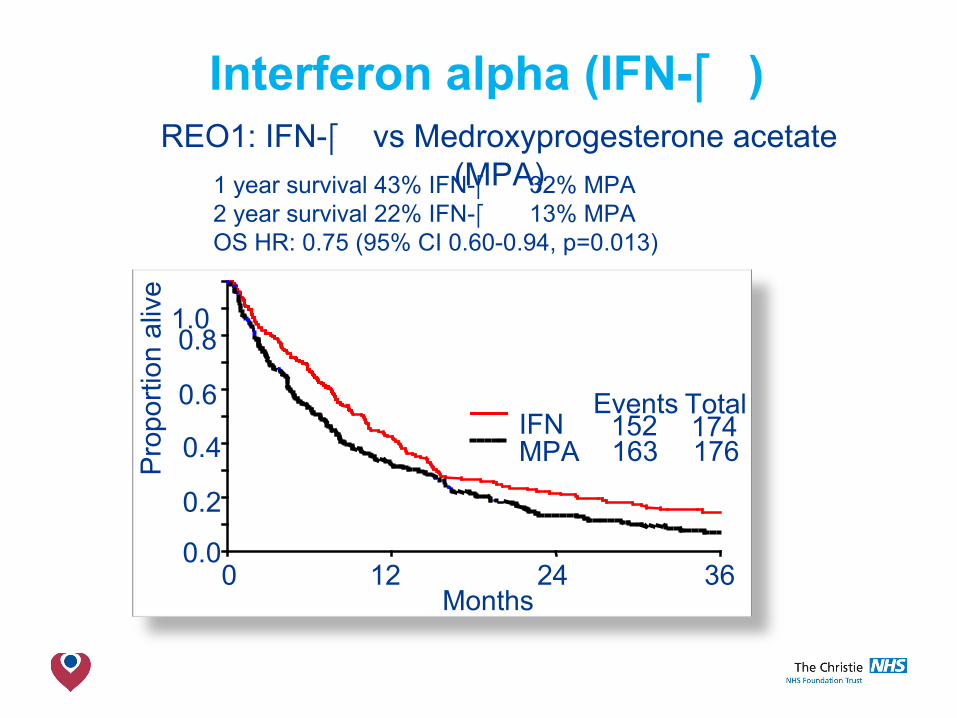
Interferon alpha (IFN- )
IFNMPA
Events Total152163
174176
0.0
0.2
0.4
0.6
0.8
Pro
port
ion
aliv
e 1.0
Months0 12 24 36
REO1: IFN- vs Medroxyprogesterone acetate(MPA)1 year survival 43% IFN- 32% MPA
2 year survival 22% IFN- 13% MPAOS HR: 0.75 (95% CI 0.60-0.94, p=0.013)
The Christie NHS Foundation Trust
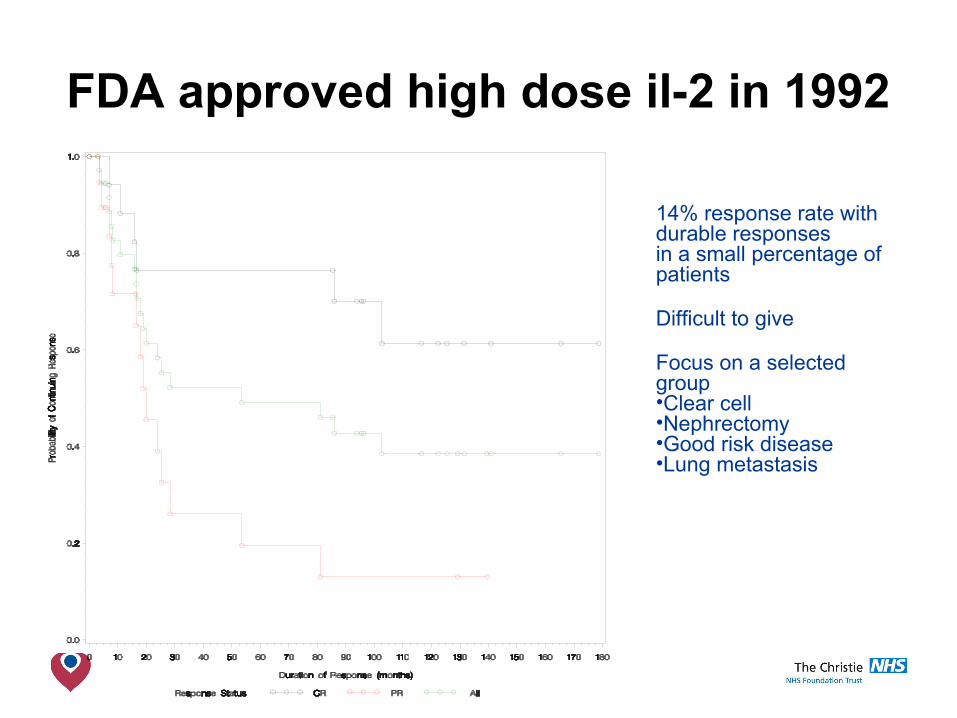
FDA approved high dose il-2 in 1992
14% response rate withdurable responses in a small percentage ofpatients
Difficult to give
Focus on a selectedgroup•Clear cell •Nephrectomy•Good risk disease•Lung metastasis
The Christie NHS Foundation Trust
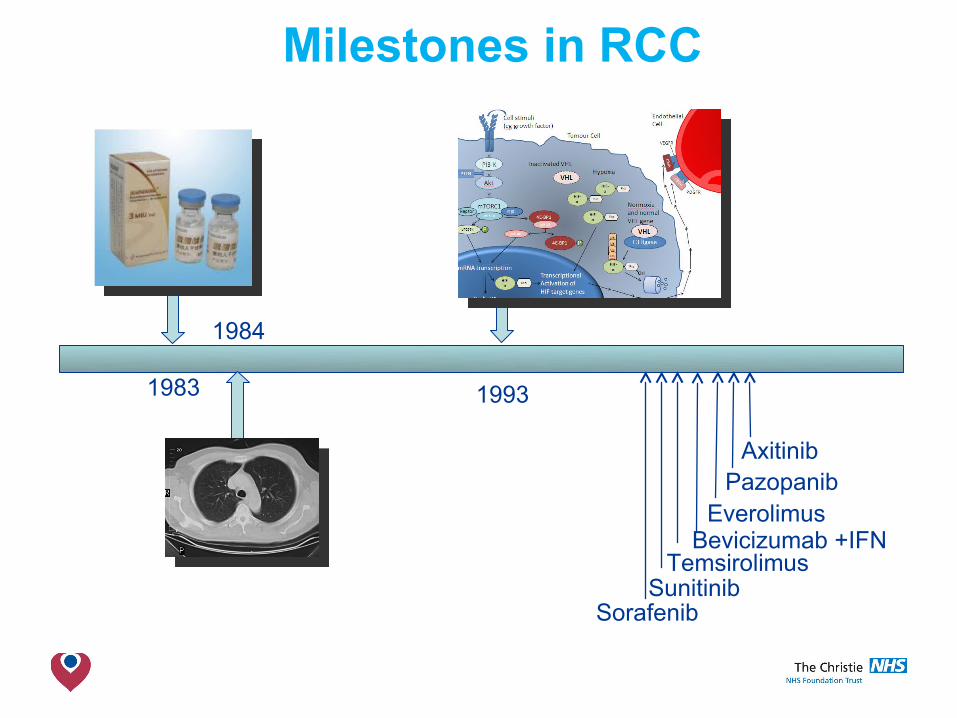
Milestones in RCC
1983
1984
1993
SorafenibSunitinib
PazopanibAxitinib
Everolimus
TemsirolimusBevicizumab +IFN
The Christie NHS Foundation Trust
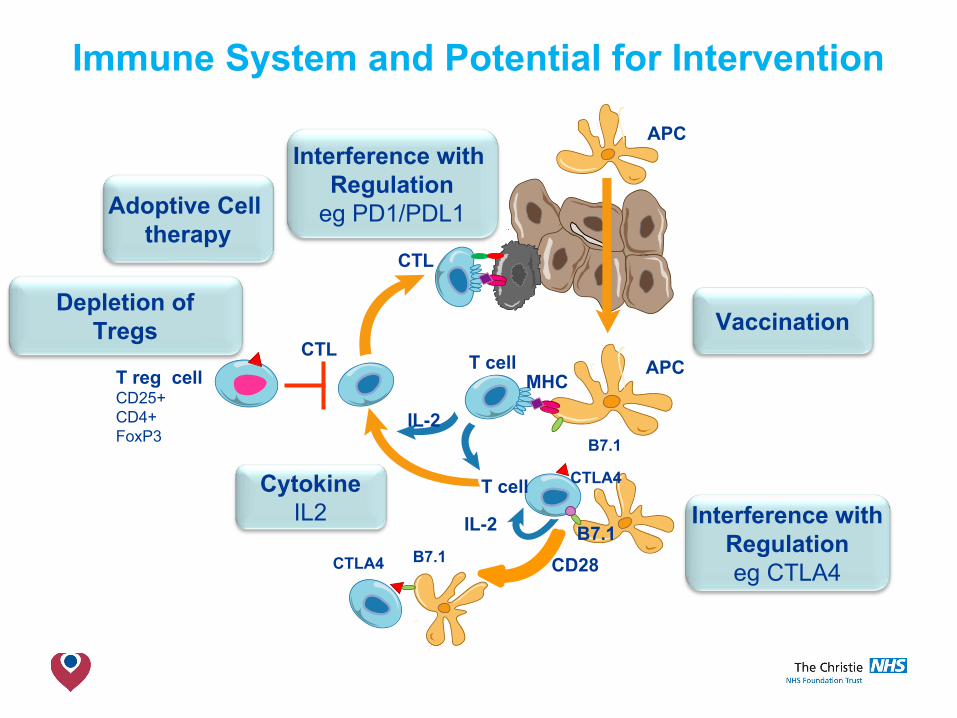
Immune System and Potential for Intervention
T reg cellCD25+CD4+FoxP3
CTL
APC
B7.1
CD28
T cell
T cell
CTLA4
B7.1
MHCAPC
CTL
IL-2
IL-2
CTLA4 B7.1
Vaccination
Interference withRegulationeg CTLA4
CytokineIL2
Depletion ofTregs
Interference with Regulation
eg PD1/PDL1Adoptive Cell therapy
The Christie NHS Foundation Trust
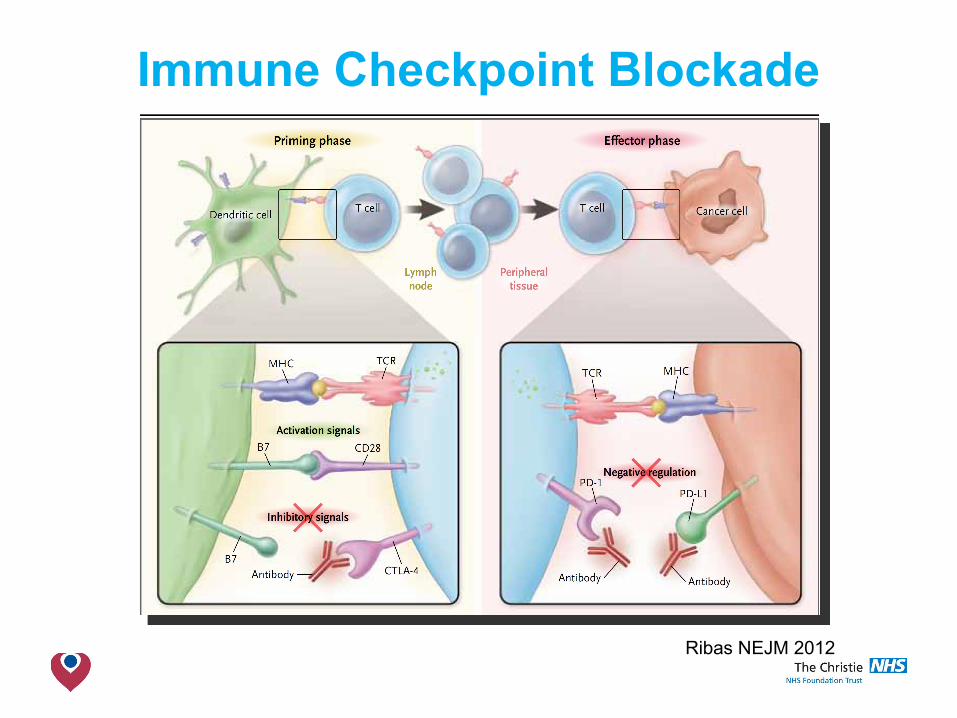
Immune Checkpoint Blockade
Ribas NEJM 2012
The Christie NHS Foundation Trust
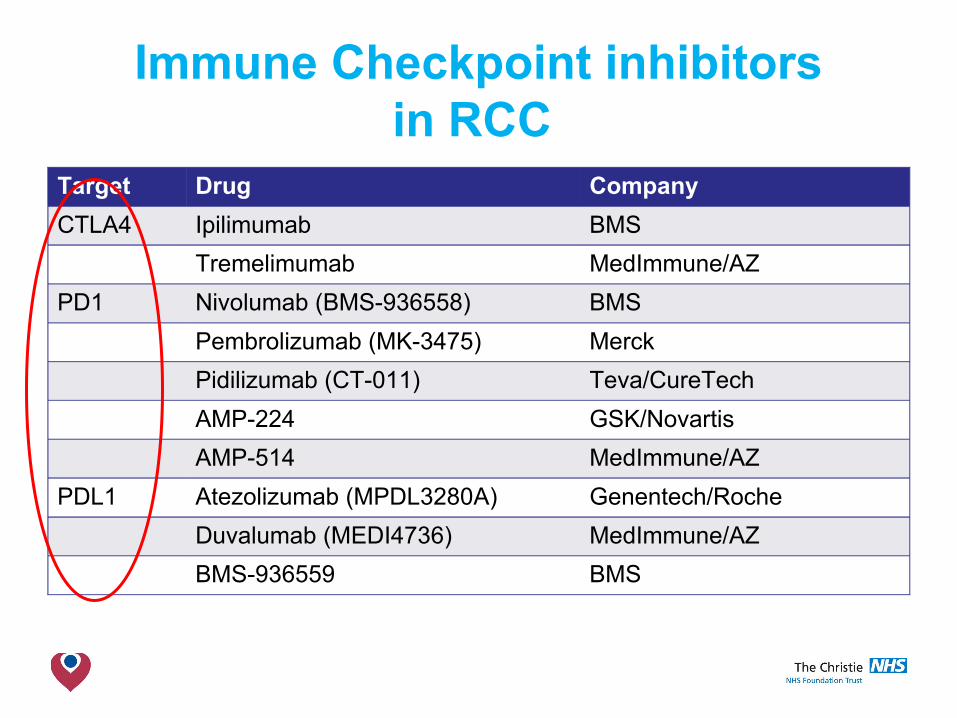
Immune Checkpoint inhibitorsin RCC
Target Drug Company
CTLA4 Ipilimumab BMS
Tremelimumab MedImmune/AZ
PD1 Nivolumab (BMS-936558) BMS
Pembrolizumab (MK-3475) Merck
Pidilizumab (CT-011) Teva/CureTech
AMP-224 GSK/Novartis
AMP-514 MedImmune/AZ
PDL1 Atezolizumab (MPDL3280A) Genentech/Roche
Duvalumab (MEDI4736) MedImmune/AZ
BMS-936559 BMS
The Christie NHS Foundation Trust
Immune Checkpoint inhibitorsin RCC
• ClinicalTrials.gov >450 trials of ‘immune agents’in RCC
• All stages of clinical development • Biomarker studies• Phase I-III• Combination studies
The Christie NHS Foundation Trust
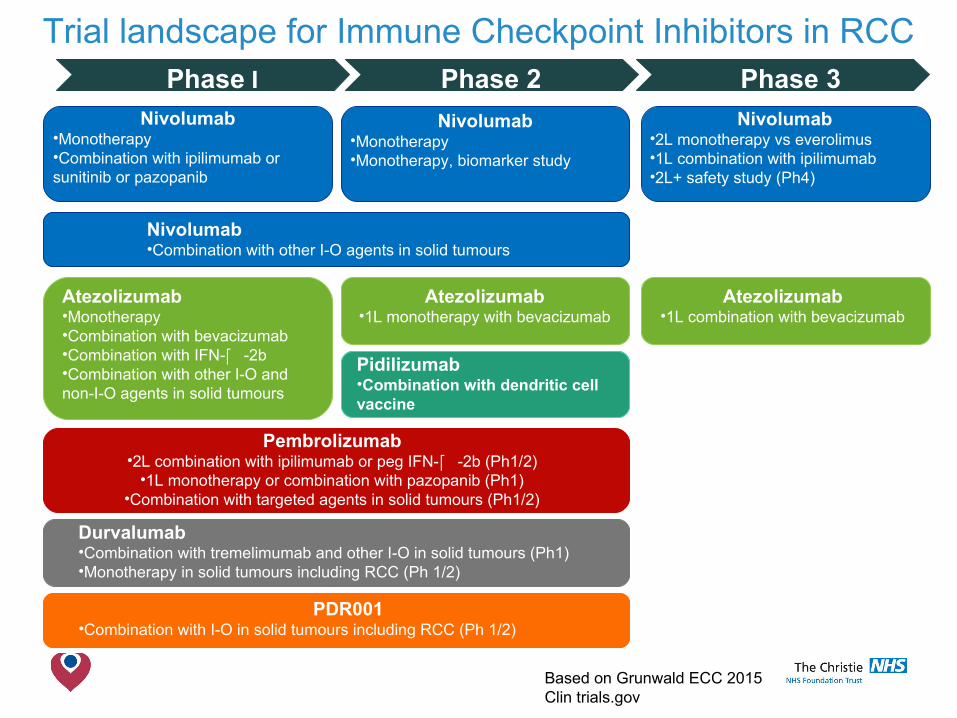
Trial landscape for Immune Checkpoint Inhibitors in RCC
Based on Grunwald ECC 2015Clin trials.gov
Phase I Phase 2 Phase 3Nivolumab
•Monotherapy•Combination with ipilimumab orsunitinib or pazopanib
Nivolumab•Monotherapy•Monotherapy, biomarker study
Nivolumab•2L monotherapy vs everolimus•1L combination with ipilimumab•2L+ safety study (Ph4)
Nivolumab•Combination with other I-O agents in solid tumours
Atezolizumab•Monotherapy•Combination with bevacizumab•Combination with IFN- -2b•Combination with other I-O and non-I-O agents in solid tumours
Atezolizumab•1L monotherapy with bevacizumab
Atezolizumab•1L combination with bevacizumab
Pidilizumab•Combination with dendritic cellvaccine
Pembrolizumab•2L combination with ipilimumab or peg IFN- -2b (Ph1/2)
•1L monotherapy or combination with pazopanib (Ph1)•Combination with targeted agents in solid tumours (Ph1/2)
Durvalumab•Combination with tremelimumab and other I-O in solid tumours (Ph1)•Monotherapy in solid tumours including RCC (Ph 1/2)
PDR001•Combination with I-O in solid tumours including RCC (Ph 1/2)
CheckMate 025: A randomized, open-label, phase III study ofnivolumab versuseverolimus in advancedrenal cell carcinoma
Padmanee Sharma, Bernard Escudier, David F. McDermott, Saby George, Hans J. Hammers, Sandhya Srinivas, Scott S. Tykodi, Jeffrey A. Sosman,
Giuseppe Procopio, Elizabeth R. Plimack, Daniel Castellano, Howard Gurney, Frede Donskov, Petri Bono, John Wagstaff, Thomas C. Gauler, Takeshi Ueda,
Li-An Xu, Ian M. Waxman, Robert J. Motzer, on behalf of the CheckMate 025 investigators
13
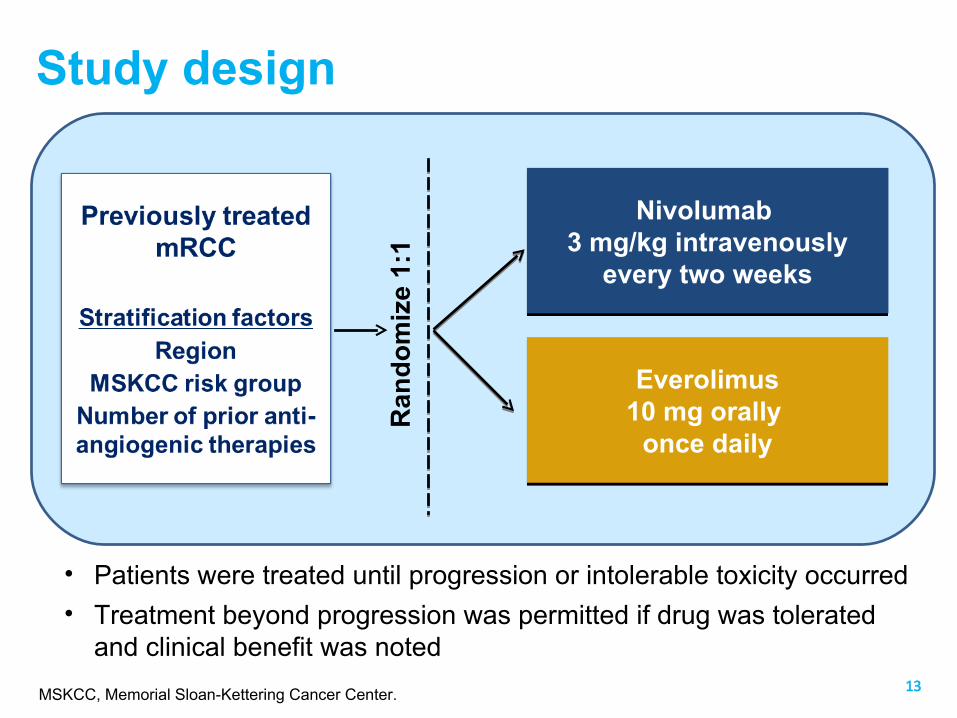
Study design
Nivolumab 3 mg/kg intravenously
every two weeks
Nivolumab 3 mg/kg intravenously
every two weeks
Everolimus10 mg orally
once daily
Everolimus10 mg orally
once daily
Ran
do
miz
e 1:
1
• Patients were treated until progression or intolerable toxicity occurred
• Treatment beyond progression was permitted if drug was toleratedand clinical benefit was noted
MSKCC, Memorial Sloan-Kettering Cancer Center.
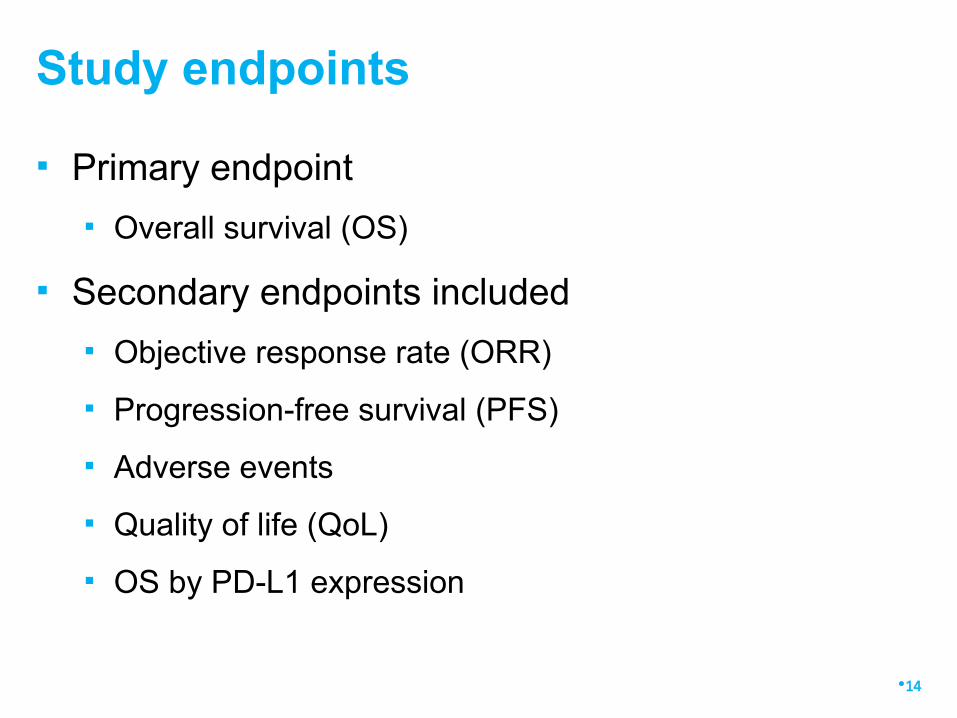
▪ Primary endpoint
▪ Overall survival (OS)
▪ Secondary endpoints included
▪ Objective response rate (ORR)
▪ Progression-free survival (PFS)
▪ Adverse events
▪ Quality of life (QoL)
▪ OS by PD-L1 expression
Study endpoints
•14
•15
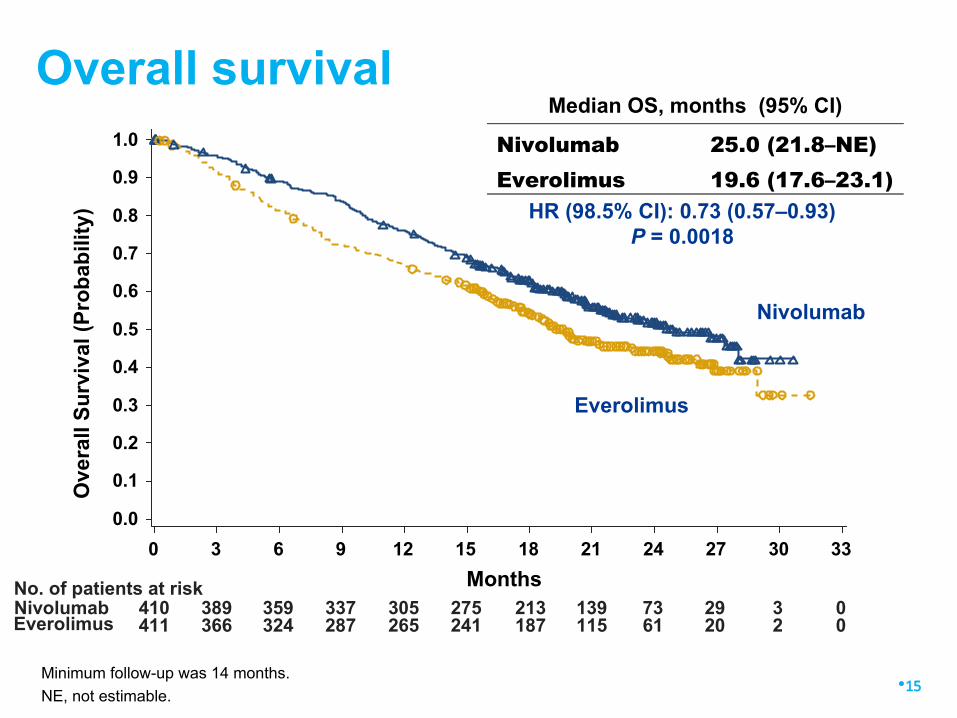
Overall survivalMedian OS, months (95% CI)
Nivolumab 25.0 (21.8–NE)Everolimus 19.6 (17.6–23.1)
HR (98.5% CI): 0.73 (0.57–0.93)P = 0.0018
0 3 6 129 15
Months
18 21 24 27 30 33
No. of patients at riskNivolumab 410 389 359 337 305 275 213 139 73 29 3 0
411 366 324 287 265 241 187 115 61 20 2 0Everolimus
0.0
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Ove
rall
Su
rviv
al (
Pro
bab
ility
)
Nivolumab
Everolimus
Minimum follow-up was 14 months.
NE, not estimable.
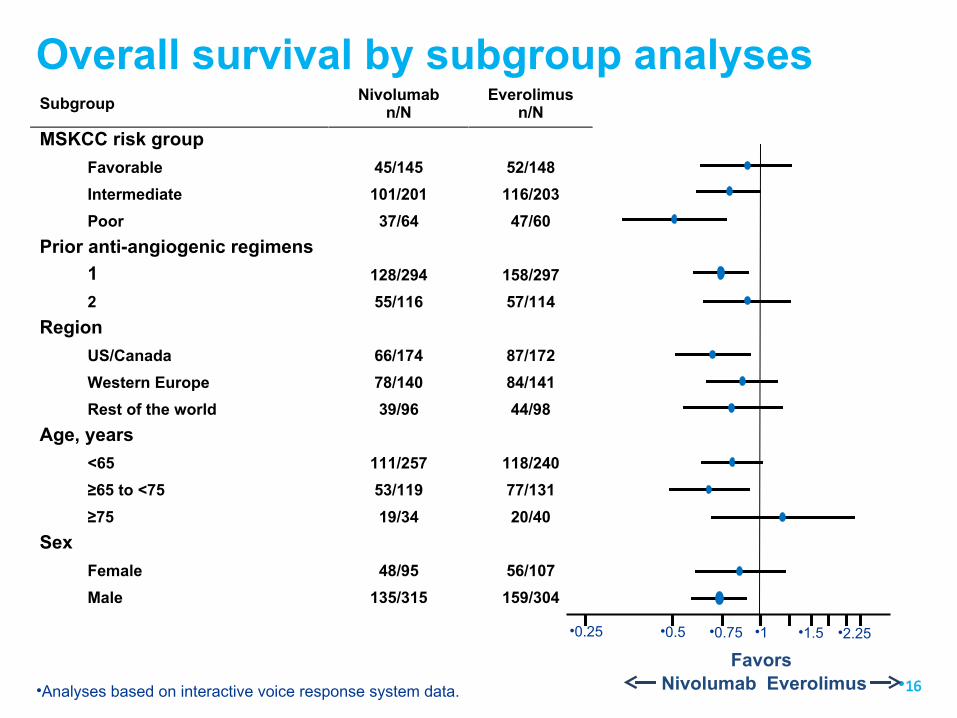
Overall survival by subgroup analysesSubgroup
Nivolumabn/N
Everolimusn/N
MSKCC risk group
Favorable 45/145 52/148
Intermediate 101/201 116/203
Poor 37/64 47/60
Prior anti-angiogenic regimens
1 128/294 158/297
2 55/116 57/114
Region
US/Canada 66/174 87/172
Western Europe 78/140 84/141
Rest of the world 39/96 44/98
Age, years
<65 111/257 118/240
≥65 to <75 53/119 77/131
≥75 19/34 20/40
Sex
Female 48/95 56/107
Male 135/315 159/304
•16Nivolumab
•0.25 •0.5 •0.75 •1.5 •2.25•1
EverolimusFavors
•Analyses based on interactive voice response system data.
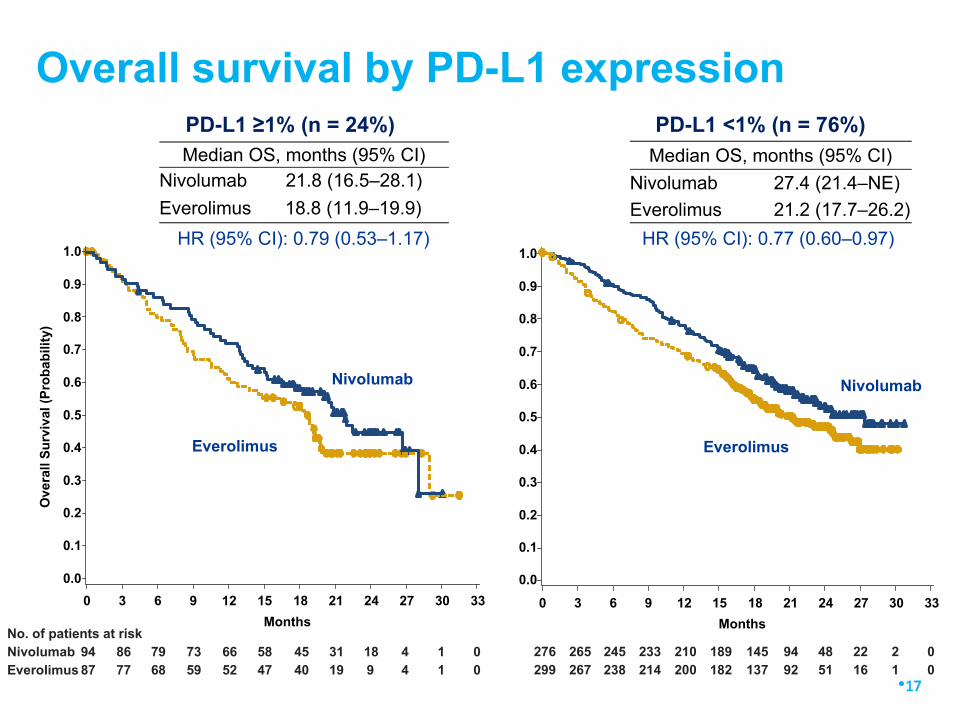
Overall survival by PD-L1 expressionPD-L1 <1% (n = 76%)
Median OS, months (95% CI)Nivolumab 21.8 (16.5–28.1)
Everolimus 18.8 (11.9–19.9)
No. of patients at riskNivolumab 94 86 79 73 66 58 45 31 18 4 1 0Everolimus 87 77 68 59 52 47 40 19 9 4 1 0
0.0
0 3 6 129 15
Months
18 21 24 27 30 33
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Ov
era
ll S
urv
ival
(P
rob
ab
ility
)
Nivolumab
Everolimus
PD-L1 ≥1% (n = 24%)
•17
Median OS, months (95% CI)
Nivolumab 27.4 (21.4–NE)
Everolimus 21.2 (17.7–26.2)
276 265 245 233 210 189 145 94 48 22 2 0299 267 238 214 200 182 137 92 51 16 1 0
Nivolumab
0 3 6 129 15
Months
18 21 24 27 30 33
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0.0
Everolimus
HR (95% CI): 0.79 (0.53–1.17) HR (95% CI): 0.77 (0.60–0.97)
•18
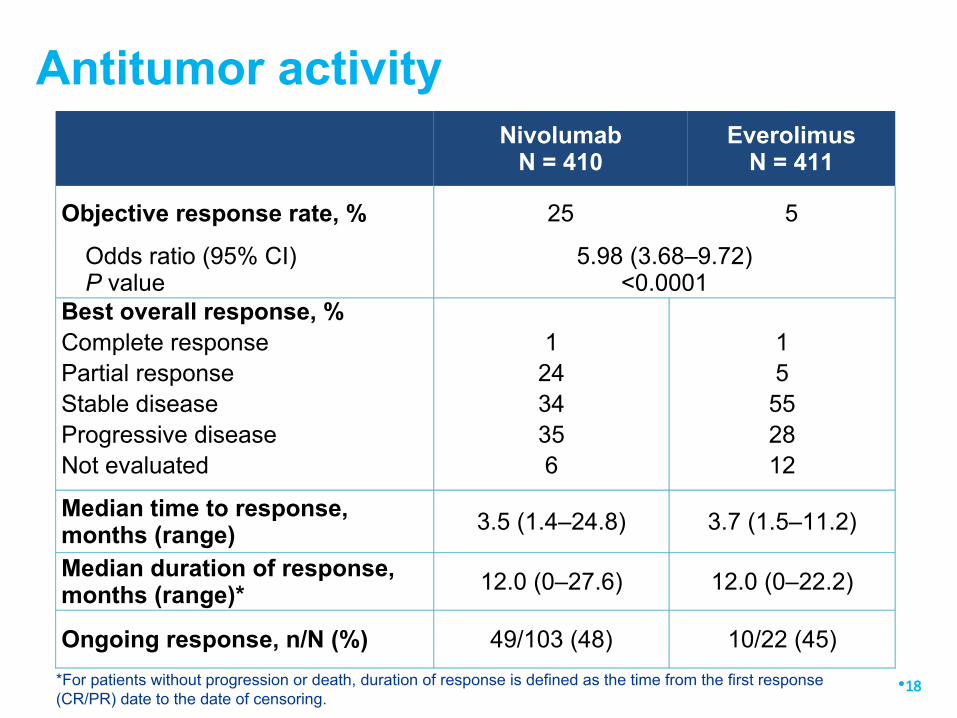
Antitumor activity
Nivolumab
N = 410Everolimus
N = 411
Objective response rate, % 25 5
Odds ratio (95% CI)P value
5.98 (3.68–9.72)<0.0001
Best overall response, %Complete responsePartial responseStable diseaseProgressive diseaseNot evaluated
1
2434356
15
552812
Median time to response,months (range)
3.5 (1.4–24.8) 3.7 (1.5–11.2)
Median duration of response,months (range)*
12.0 (0–27.6) 12.0 (0–22.2)
Ongoing response, n/N (%) 49/103 (48) 10/22 (45)
*For patients without progression or death, duration of response is defined as the time from the first response(CR/PR) date to the date of censoring.
•19
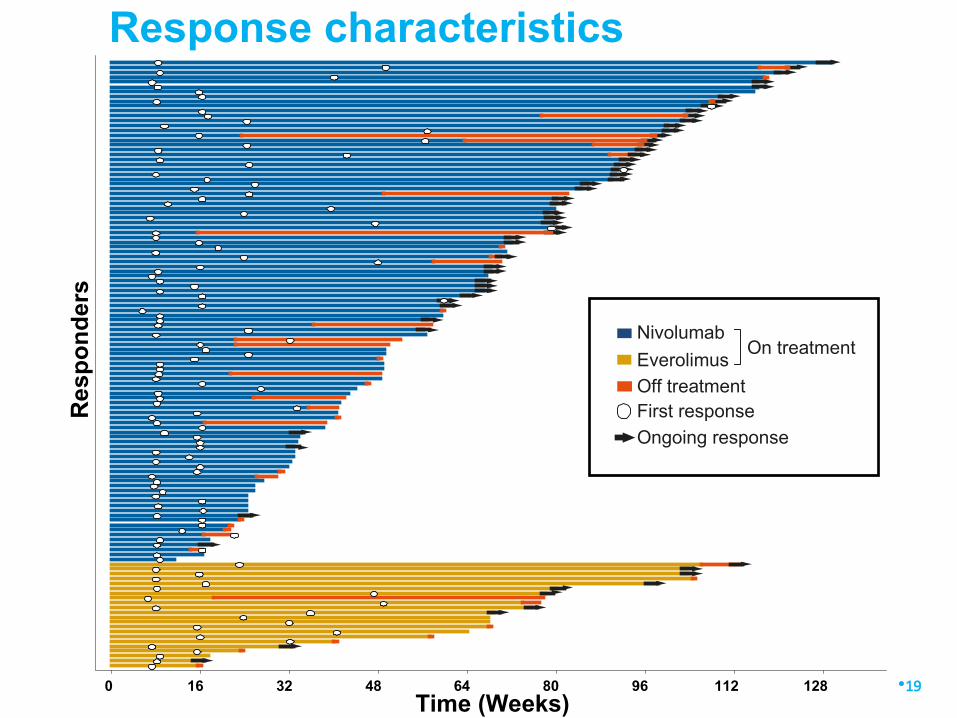
Response characteristics
0 16 32 6448 80
Time (Weeks)96 112 128
Re
spo
nd
ers
Ongoing response
First responseOff treatment
Nivolumab
EverolimusOn treatment
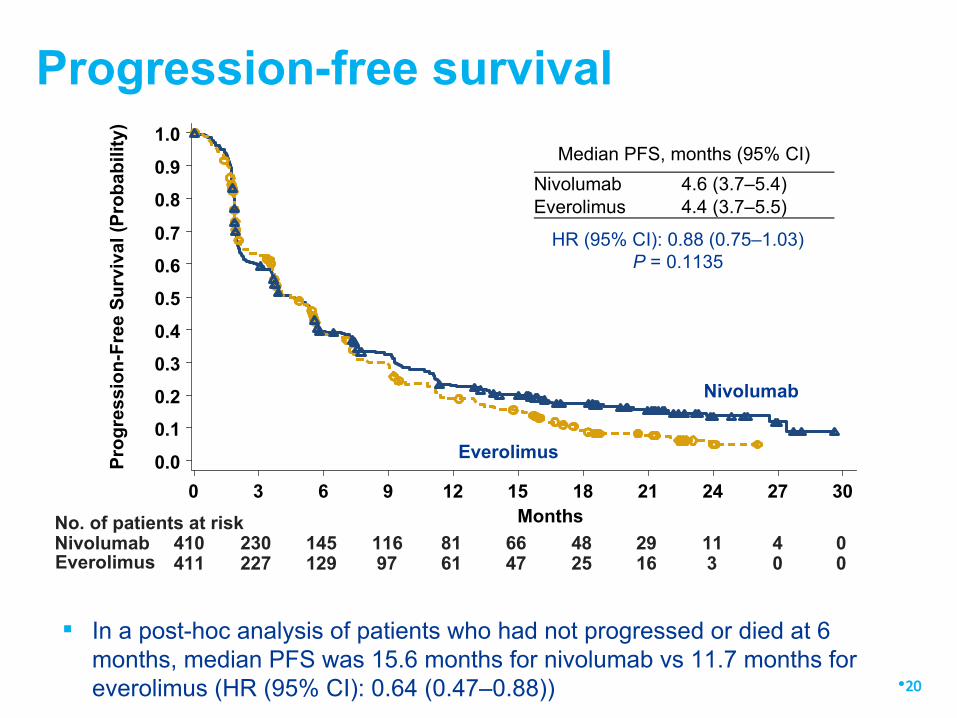
Progression-free survival
No. of patients at riskNivolumab 410 230 145 116 81 66 48 29 11 4 0Everolimus 411 227 129 97 61 47 25 16 3 0 0
0 3 6 129 15Months
18 21 24 27 30
0.0
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0P
rog
ress
ion
-Fre
e S
urv
ival
(P
rob
abili
ty)
Nivolumab
Everolimus
Median PFS, months (95% CI)
Nivolumab 4.6 (3.7–5.4)Everolimus 4.4 (3.7–5.5)
HR (95% CI): 0.88 (0.75–1.03)P = 0.1135
In a post-hoc analysis of patients who had not progressed or died at 6months, median PFS was 15.6 months for nivolumab vs 11.7 months foreverolimus (HR (95% CI): 0.64 (0.47–0.88)) •20
•21
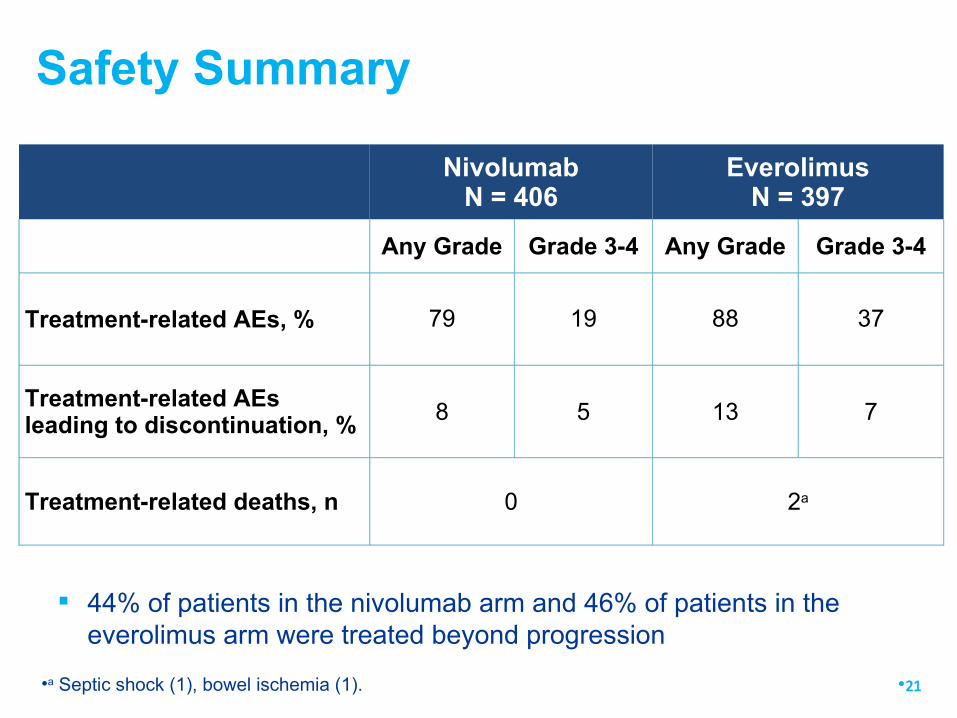
Safety Summary
NivolumabN = 406
EverolimusN = 397
Any Grade Grade 3-4 Any Grade Grade 3-4
Treatment-related AEs, % 79 19 88 37
Treatment-related AEsleading to discontinuation, % 8 5 13 7
Treatment-related deaths, n 0 2a
•a Septic shock (1), bowel ischemia (1).
44% of patients in the nivolumab arm and 46% of patients in theeverolimus arm were treated beyond progression
•22
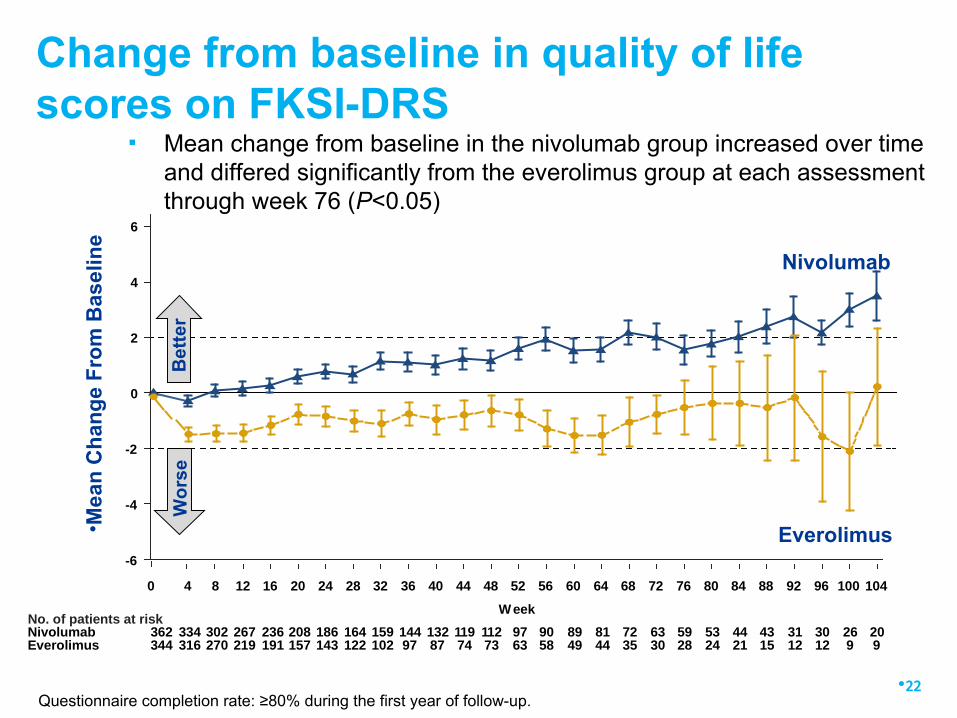
Change from baseline in quality of lifescores on FKSI-DRS
Questionnaire completion rate: ≥80% during the first year of follow-up.
• Mea
n C
han
ge
Fro
m B
asel
ine
Nivolumab
Everolimus
40 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100 104
Week
-6
0
-4
-2
2
4
6
No. of patients at riskNivolumab 362 334 302 267 236 208 186 164 159 144 132 119 112 97 90 89 81 72 63 59 53 44 43 31 30 26 20Everolimus 344 316 270 219 191 157 143 122 102 97 87 74 73 63 58 49 44 35 30 28 24 21 15 12 12 9 9
Wo
rse
Bet
ter
▪ Mean change from baseline in the nivolumab group increased over timeand differed significantly from the everolimus group at each assessmentthrough week 76 (P<0.05)
▪ CheckMate 025 met its primary endpoint, demonstratingsuperior OS with nivolumab versus everolimus (25.0 vs19.6 months)
▪ This is the only phase III trial to demonstrate a survivaladvantage in previously-treated patients with mRCC versusstandard therapy
▪ Nivolumab was associated with fewer grade 3 and 4treatment-related AEs compared to everolimus andimprovement in QOL
▪ ORR 25% vs 6 % but CR rate low at only 1% in each arm
•23
Conclusions (1)
▪ Practice changing for 2nd line therapy forRCC
▪ Still many unanswered questions forimmunotherapy in RCC▪ Checkpoint inhibitor drugs▪ Other immunotherapy approaches
What is the impact of Checkmate 025?
•24
▪ Checkpoint inhibitors in1st line therapy?▪ Combination therapy?▪ Treatment beyond progression?▪ Next generation targets?
Unanswered questions for checkpointinhibitor drugs in RCC
•25
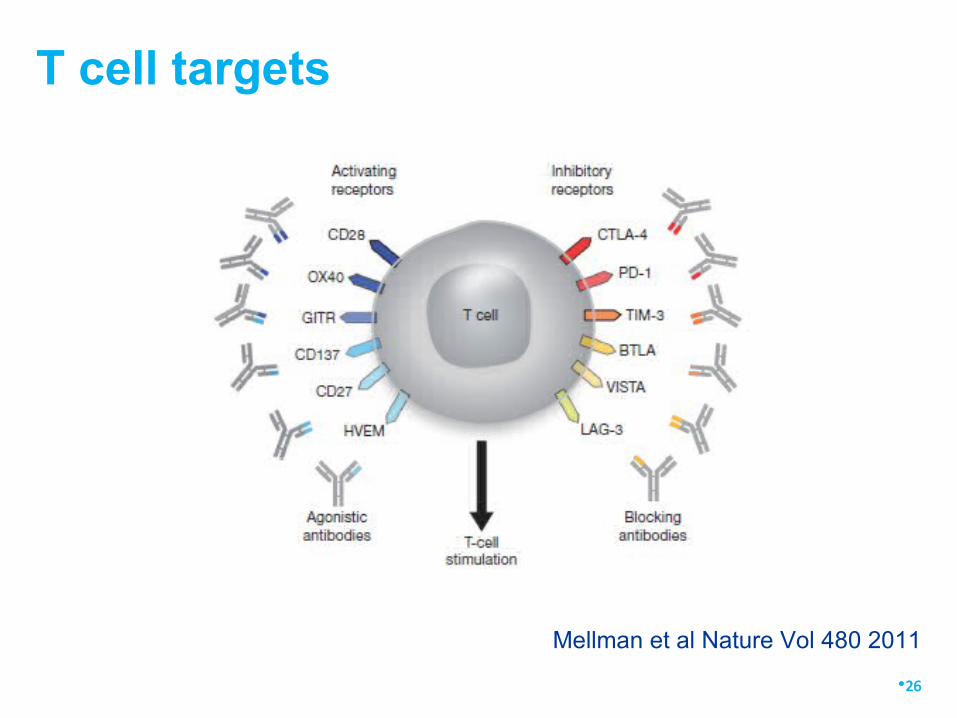
T cell targets
•26
Mellman et al Nature Vol 480 2011
▪ Checkpoint inhibitors in 1st line therapy?▪ Combination therapy?▪ Treatment beyond progression?▪ Next generation targets?▪ Immunotherapy biomarkers in RCC?▪ What about patients who do not respond?▪ How long to continue checkpoint inhibitors?▪ What about the adjuvant setting?
Unanswered questions for checkpointinhibitor drugs in RCC
•27
▪ Checkpoint inhibitors in1st line therapy?▪ Combination therapy?
Unanswered questions for checkpointinhibitor drugs in RCC
•28
•29
•30
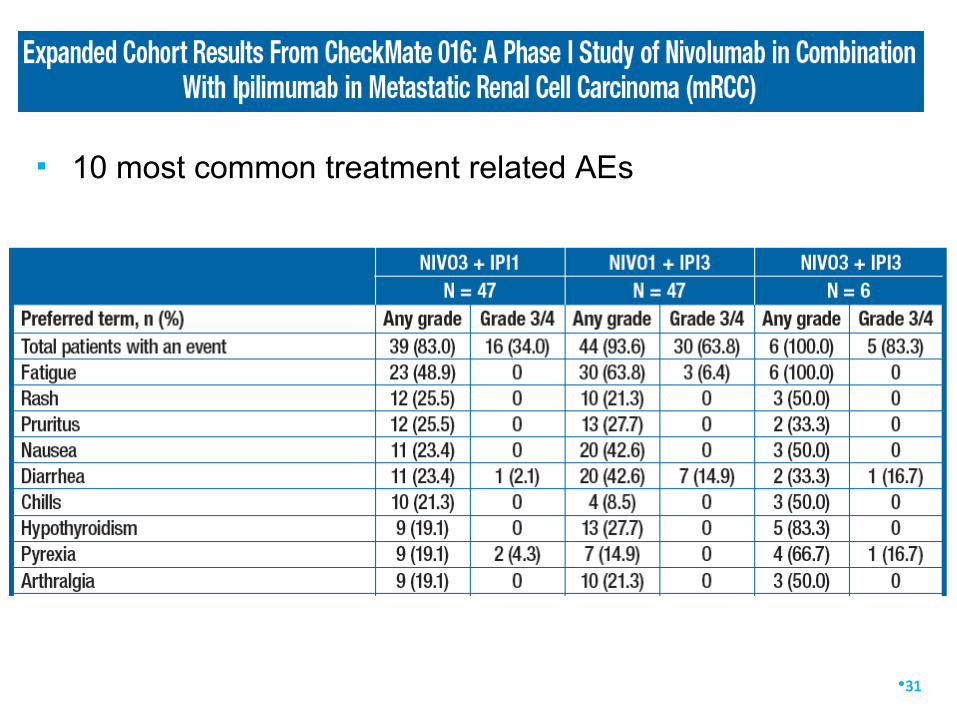
▪ 10 most common treatment related AEs
•31
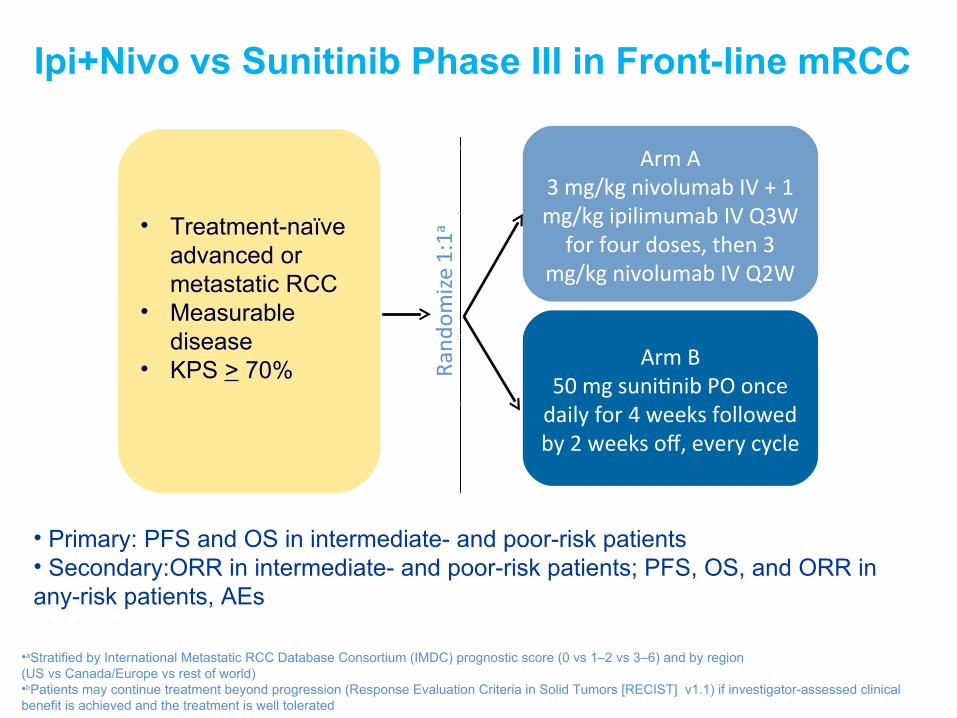
Ipi+Nivo vs Sunitinib Phase III in Front-line mRCC
•32
•aStratified by International Metastatic RCC Database Consortium (IMDC) prognostic score (0 vs 1–2 vs 3–6) and by region (US vs Canada/Europe vs rest of world)•bPatients may continue treatment beyond progression (Response Evaluation Criteria in Solid Tumors [RECIST] v1.1) if investigator-assessed clinicalbenefit is achieved and the treatment is well tolerated
• Treatment-naïveadvanced ormetastatic RCC
• Measurabledisease
• KPS > 70%
Arm A3 mg/kg nivolumab IV + 1mg/kg ipilimumab IV Q3W
for four doses, then 3mg/kg nivolumab IV Q2W
Arm B50 mg sunitnib PO once
daily for 4 weeks followedby 2 weeks of, every cycle
• Primary: PFS and OS in intermediate- and poor-risk patients• Secondary:ORR in intermediate- and poor-risk patients; PFS, OS, and ORR inany-risk patients, AEs
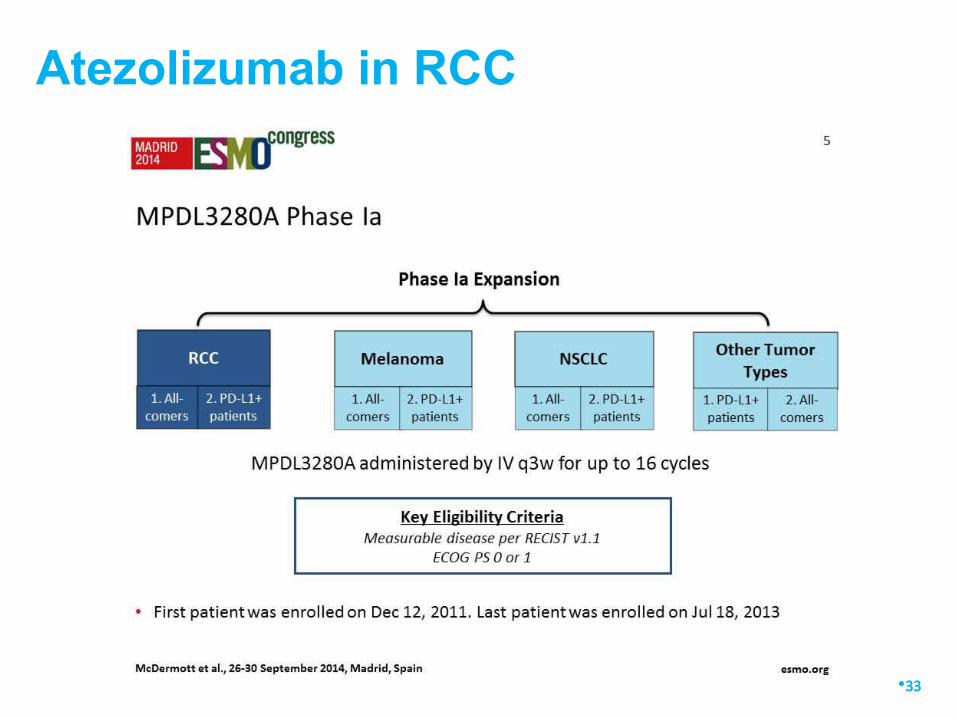
Atezolizumab in RCC
•33
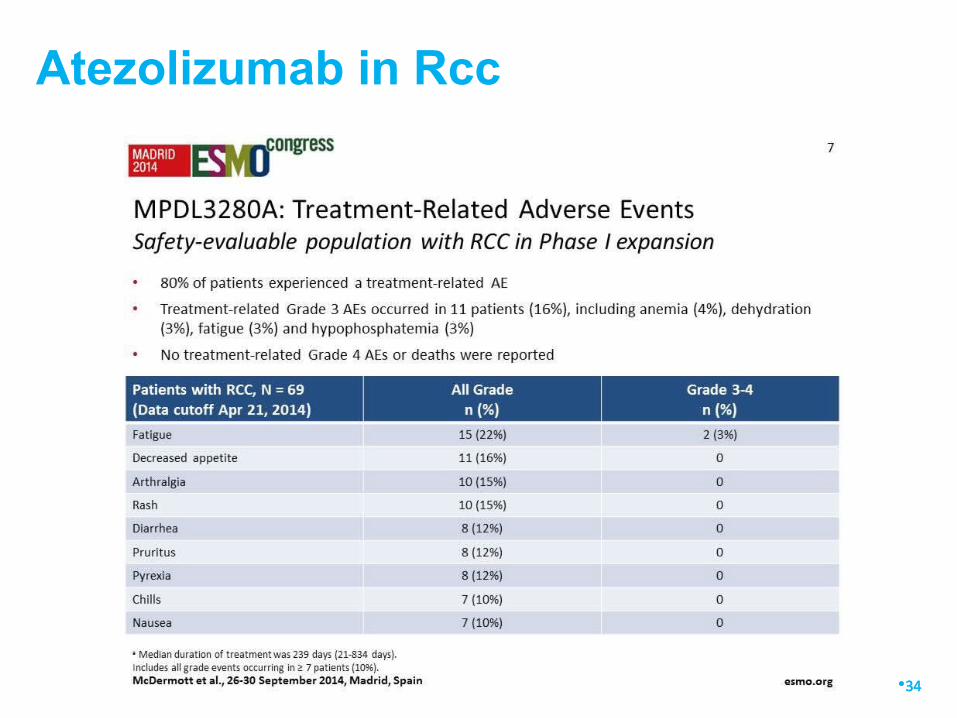
Atezolizumab in Rcc
•34
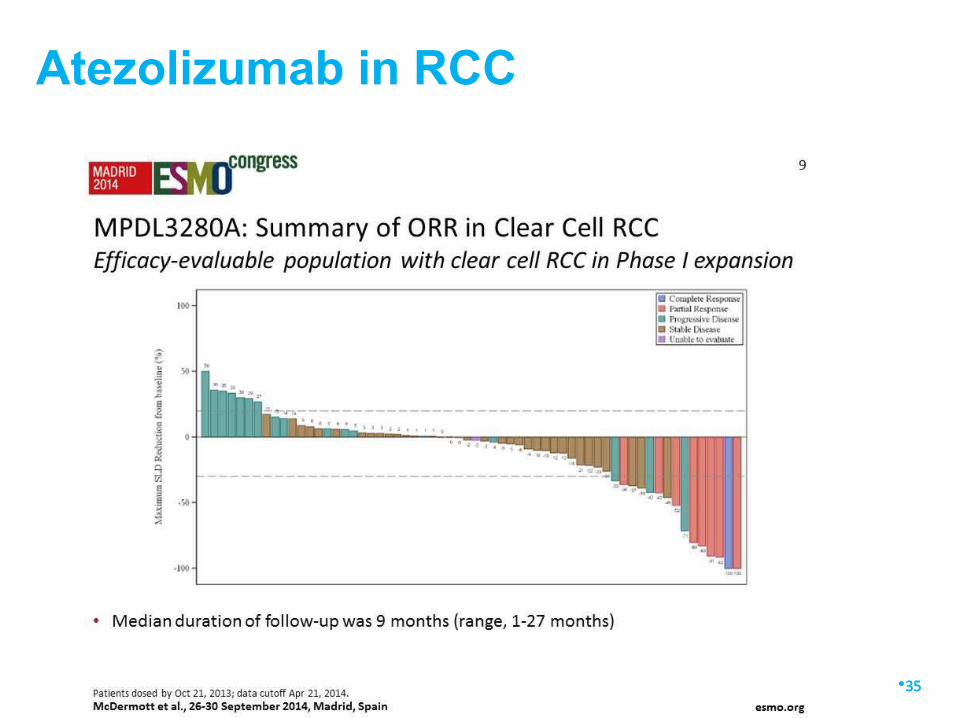
Atezolizumab in RCC
•35
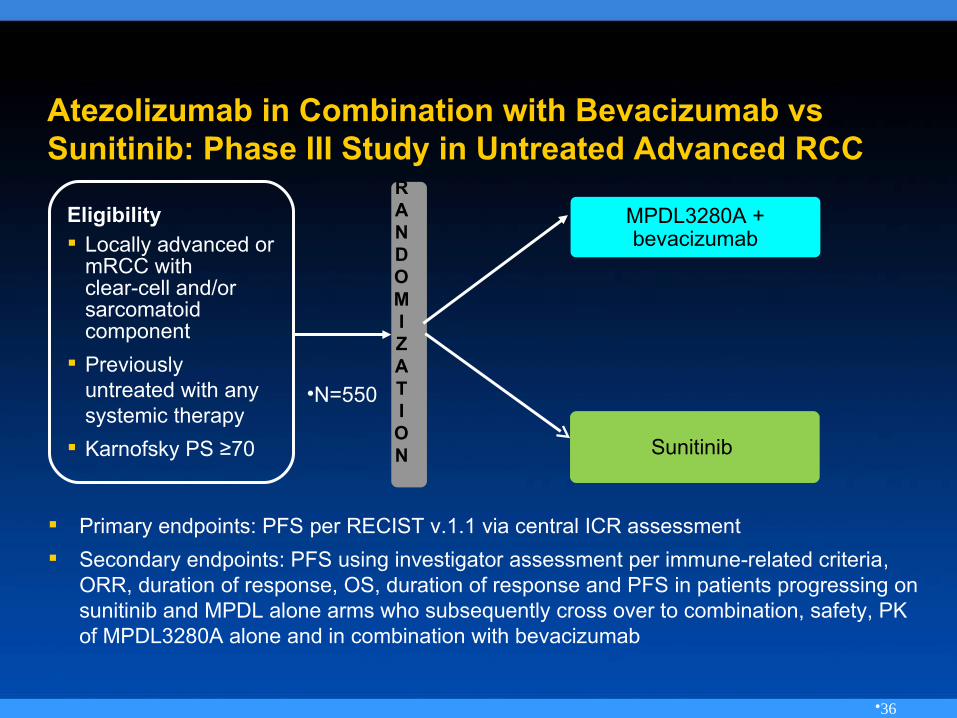
Atezolizumab in Combination with Bevacizumab vsSunitinib: Phase III Study in Untreated Advanced RCC
Primary endpoints: PFS per RECIST v.1.1 via central ICR assessment
Secondary endpoints: PFS using investigator assessment per immune-related criteria,ORR, duration of response, OS, duration of response and PFS in patients progressing onsunitinib and MPDL alone arms who subsequently cross over to combination, safety, PKof MPDL3280A alone and in combination with bevacizumab
Eligibility Locally advanced or
mRCC with clear-cell and/orsarcomatoidcomponent
Previouslyuntreated with anysystemic therapy
Karnofsky PS ≥70
MPDL3280A +bevacizumab
RANDOMIZATION
•N=550
Sunitinib
•36
▪ What about 1st line therapy?▪ Combination therapy?▪ Treatment beyond progression?
Unanswered questions for checkpointinhibitor drugs in RCC
•37
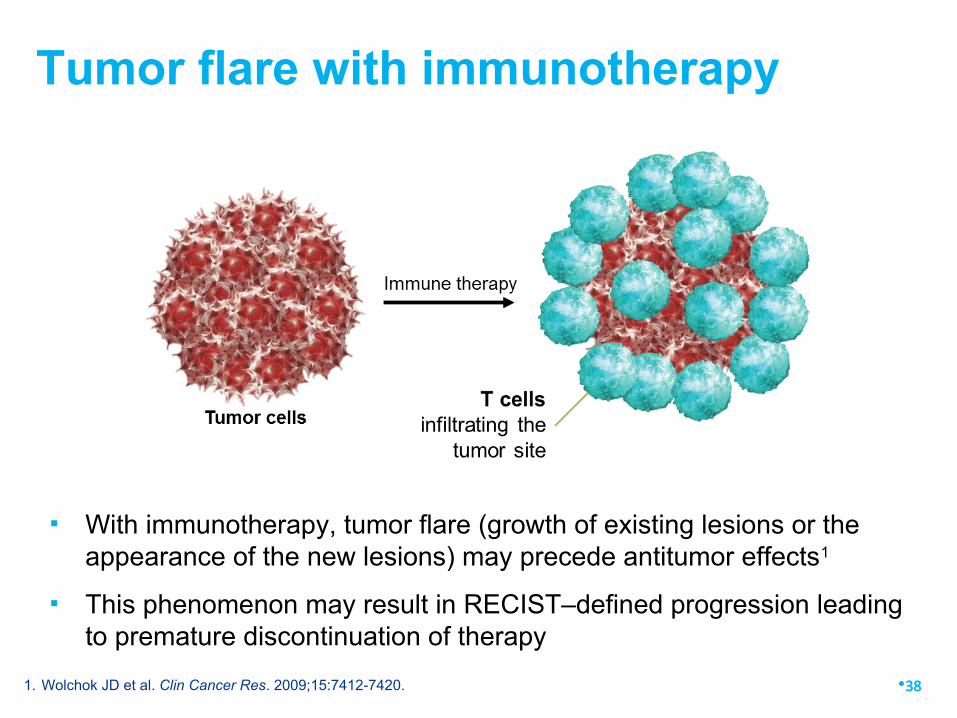
▪ With immunotherapy, tumor flare (growth of existing lesions or theappearance of the new lesions) may precede antitumor effects1
▪ This phenomenon may result in RECIST–defined progression leadingto premature discontinuation of therapy
Tumor flare with immunotherapy
•381. Wolchok JD et al. Clin Cancer Res. 2009;15:7412-7420.
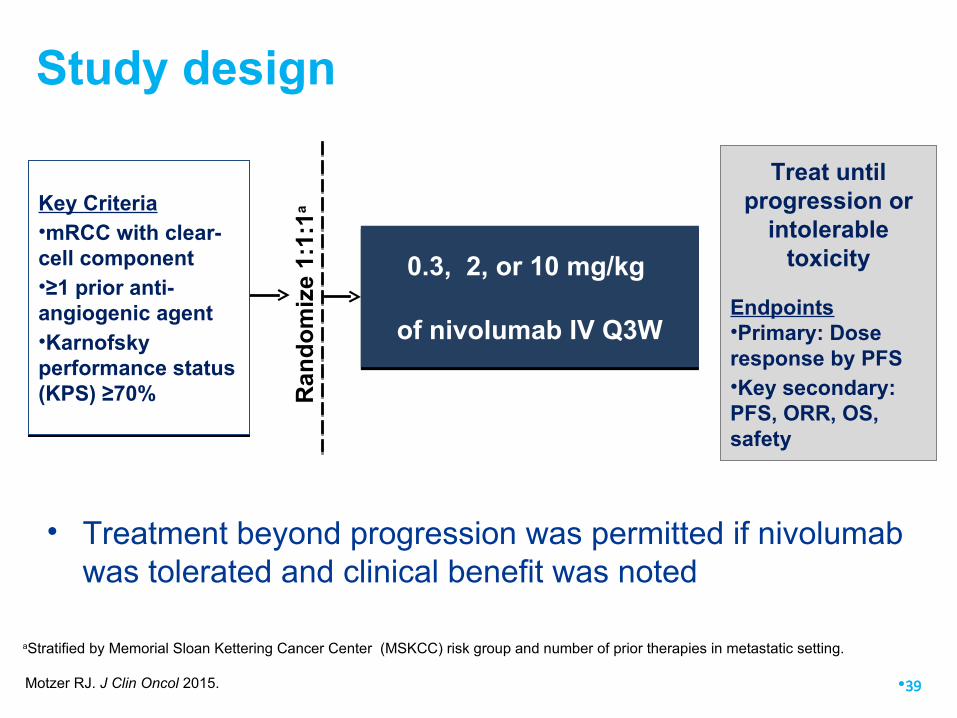
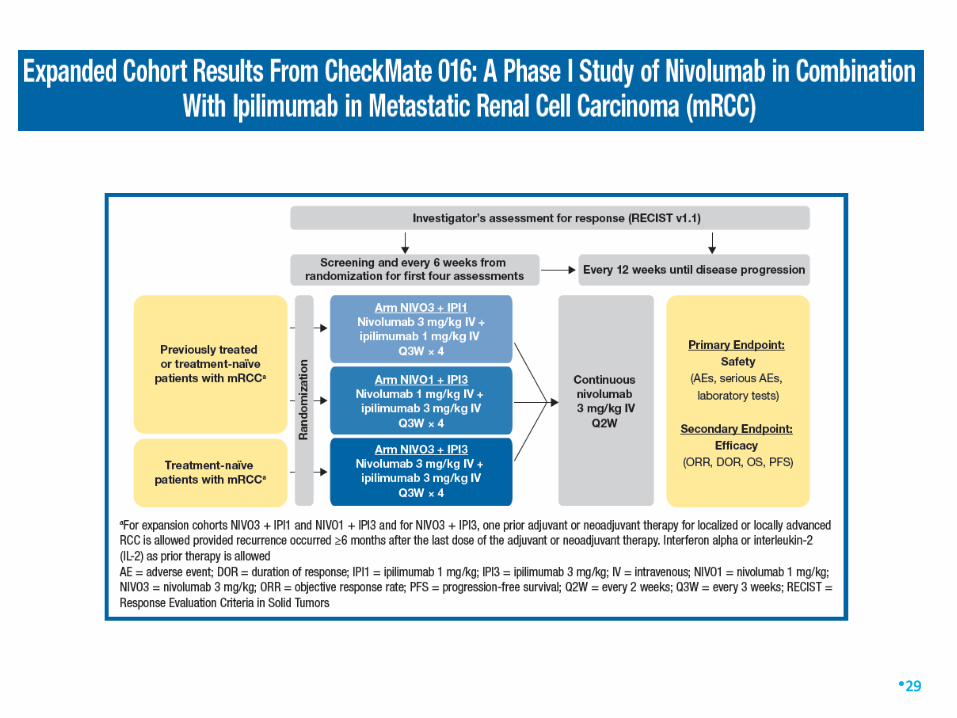
Study design
aStratified by Memorial Sloan Kettering Cancer Center (MSKCC) risk group and number of prior therapies in metastatic setting.
0.3, 2, or 10 mg/kg
of nivolumab IV Q3W
0.3, 2, or 10 mg/kg
of nivolumab IV Q3WR
an
do
miz
e 1:
1:1aKey Criteria
•mRCC with clear-cell component•≥1 prior anti-angiogenic agent •Karnofskyperformance status(KPS) ≥70%
Key Criteria•mRCC with clear-cell component•≥1 prior anti-angiogenic agent •Karnofskyperformance status(KPS) ≥70%
Treat untilprogression or
intolerabletoxicity
Endpoints•Primary: Doseresponse by PFS•Key secondary:PFS, ORR, OS,safety
•39
• Treatment beyond progression was permitted if nivolumabwas tolerated and clinical benefit was noted
Motzer RJ. J Clin Oncol 2015.
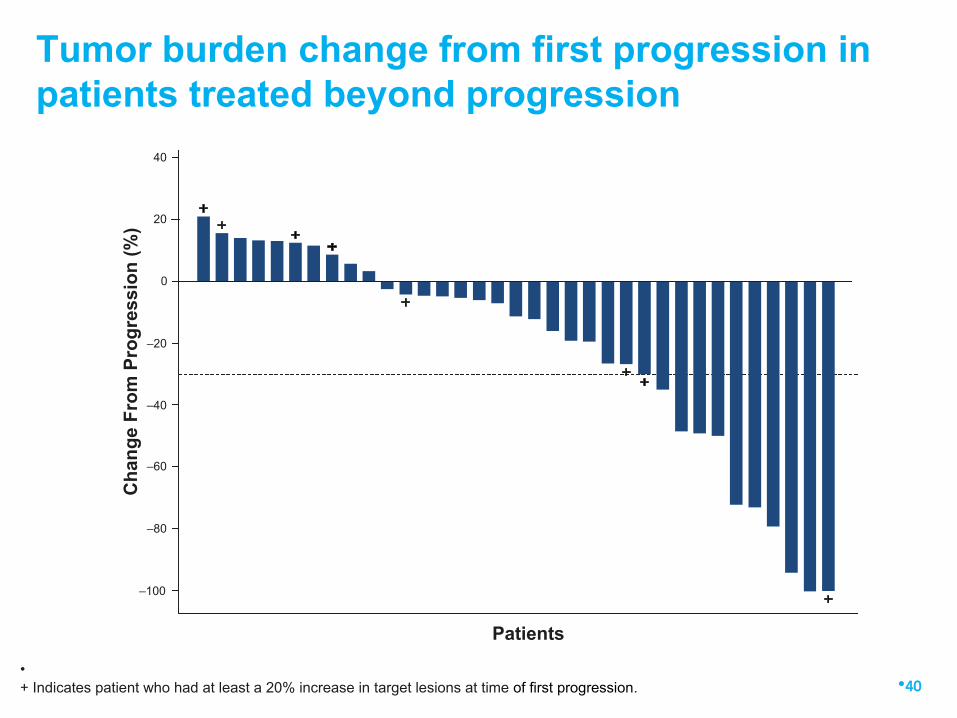
Tumor burden change from first progression inpatients treated beyond progression
•40
Patients
40
20
–20
–40
–60
–80
–100
0
Ch
ang
e F
rom
Pro
gre
ssio
n (
%)
•+ Indicates patient who had at least a 20% increase in target lesions at time of first progression.
The Christie NHS Foundation Trust
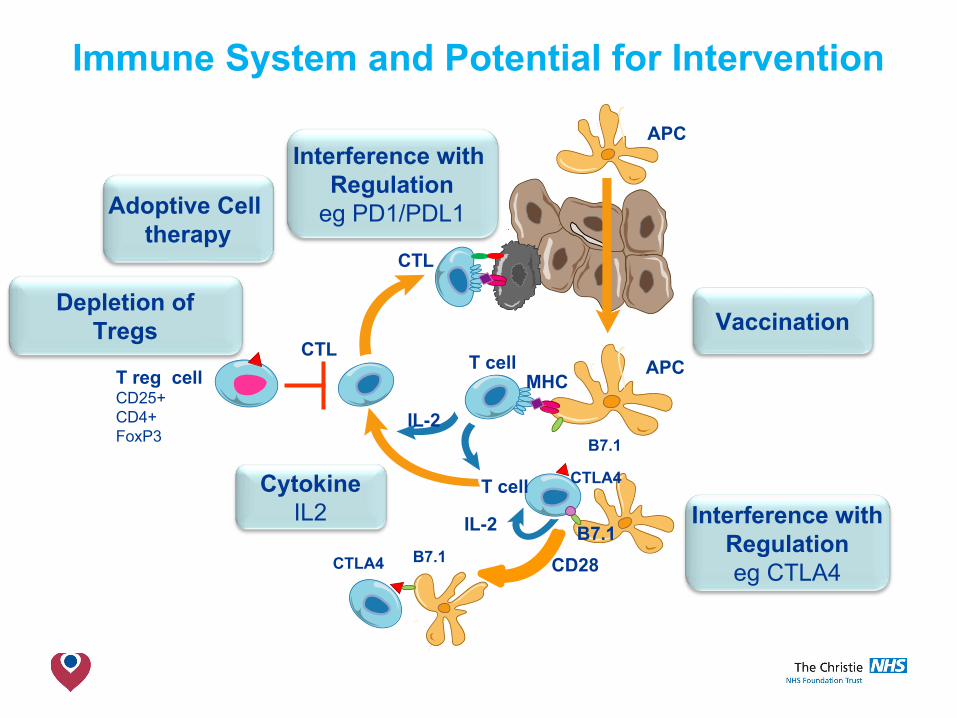
Immune System and Potential for Intervention
T reg cellCD25+CD4+FoxP3
CTL
APC
B7.1
CD28
T cell
T cell
CTLA4
B7.1
MHCAPC
CTL
IL-2
IL-2
CTLA4 B7.1
Vaccination
Interference withRegulationeg CTLA4
CytokineIL2
Depletion ofTregs
Interference with Regulation
eg PD1/PDL1Adoptive Cell therapy
The Christie NHS Foundation Trust
Other approaches• Vaccination
• Autologous/allogeneic RCC vaccination• Dendritic cell vaccines• Heat Shock protein vaccines• Peptide (eg IMA901 Immatics NCT01265901)• DNA/RNA viral vaccines (eg TroVax NCT00397345)
• T cell therapy• Depletion of Treg (Thistlethwaite Can Immunol Immunother 2008)
• CAR/TCR
• TIL
An open-label, randomized, phase 3 studyinvestgatng IMA901 multpeptde cancer vaccinein combinaton with sunitnib vs. sunitnib alone as
frst-line therapy for metastatc RCC
B. Rini1, A. Stenzl2, R. Zdrojowy3, M. Kogan4, M. Shkolnik5, S. Oudard6, S. Weikert7, S. Bracarda8, S. Crabb9, J. Bedke2, J. Ludwig10, D. Maurer10, R.
Mendrzyk10, A. Mahr10, J. Fritsche10, T. Weinschenk10, H. Singh10, A. Kirner10, C. Reinhardt10, T. Eisen11
•1Cleveland Clinic Taussig Cancer Center, Cleveland, USA; 2University of Tuebingen, Tuebingen, Germany; 3Wroclaw MedicalUniversity, Wroclaw, Poland; 4Rostov State Medical University of Roszdrav, Rostov-on-Don, Russia; 5Russian Scientfc Centerof Radiology and Surgery Technologies, St. Petersburg, Russia; 6Hopital Europeen Georges Pompidou, Paris, France; 7Vivantes
Humboldt Clinic, Berlin, Germany; 8Ospedale San Donato, Arezzo, Italy; 9Southampton General Hospital, Southampton, UK;10immatcs biotechnologies GmbH, Tuebingen, Germany; 11University of Cambridge, Cambridge, UK
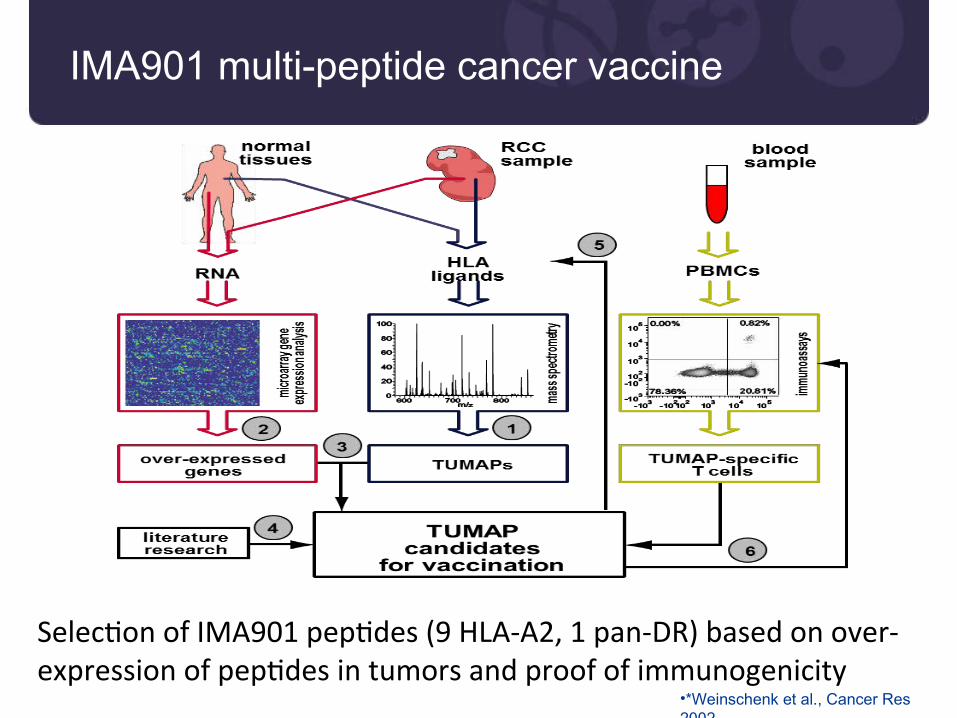
IMA901 multi-peptide cancer vaccine
Selecton of IMA901 peptdes (9 HLA-A2, 1 pan-DR) based on over-expression of peptdes in tumors and proof of immunogenicity
•*Weinschenk et al., Cancer Res2002
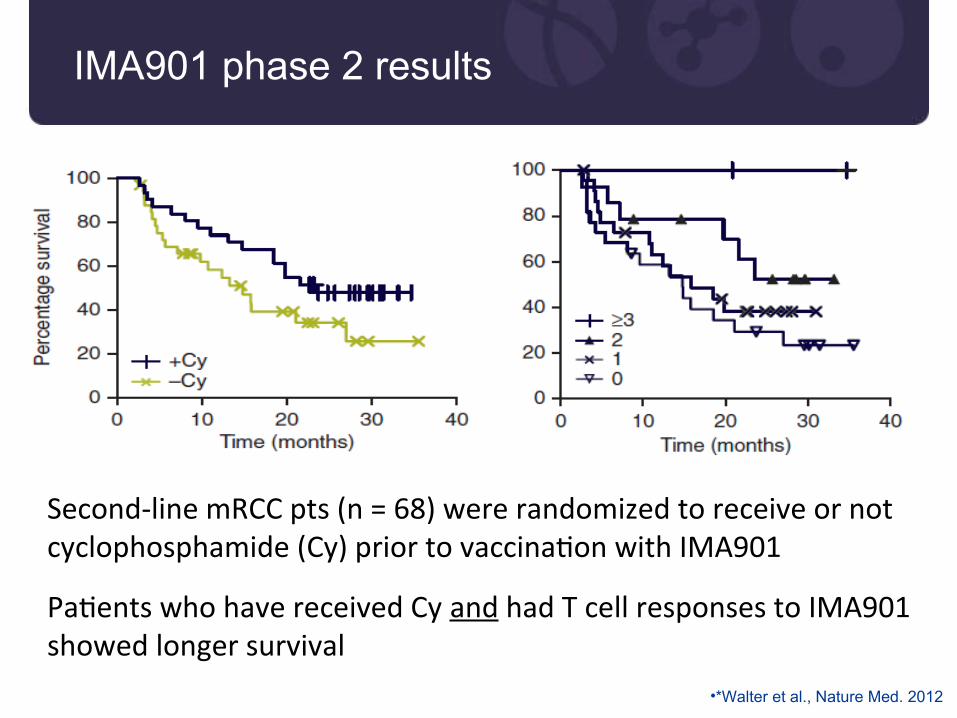
IMA901 phase 2 results
Second-line mRCC pts (n = 68) were randomized to receive or notcyclophosphamide (Cy) prior to vaccinaton with IMA901
Patents who have received Cy and had T cell responses to IMA901showed longer survival
•*Walter et al., Nature Med. 2012
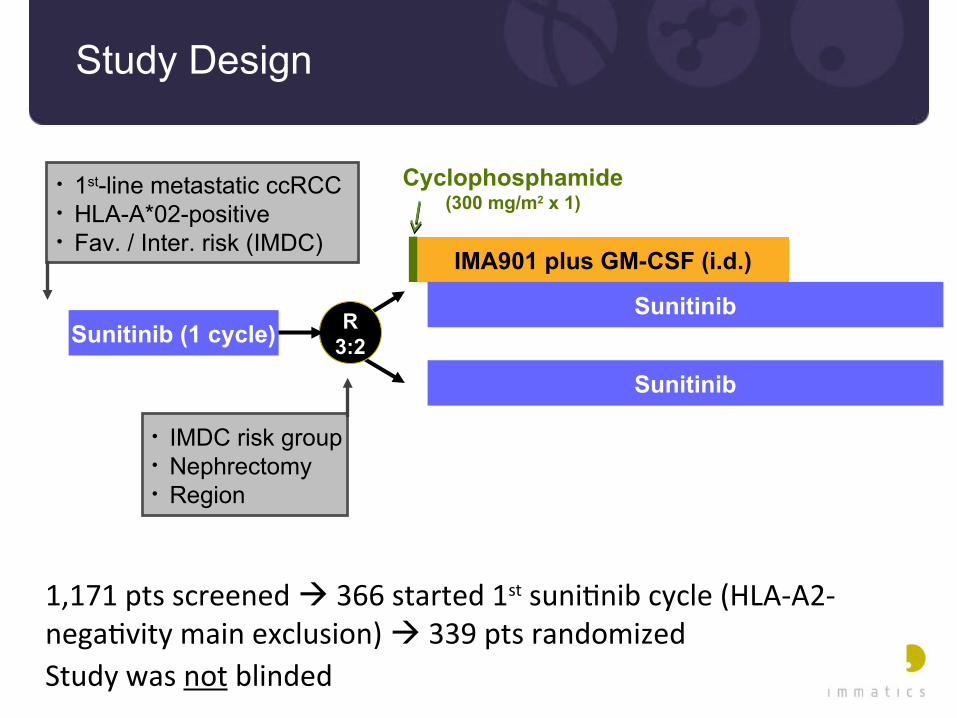
Study Design
1,171 pts screened 366 started 1st sunitnib cycle (HLA-A2-negatvity main exclusion) 339 pts randomized
Study was not blinded
IMA901 plus GM-CSF (i.d.)
R3:2
Sunitinib
Cyclophosphamide(300 mg/m2 x 1)
SunitinibSunitinib (1 cycle)
• IMDC risk group• Nephrectomy• Region
• 1st-line metastatic ccRCC• HLA-A*02-positive• Fav. / Inter. risk (IMDC)
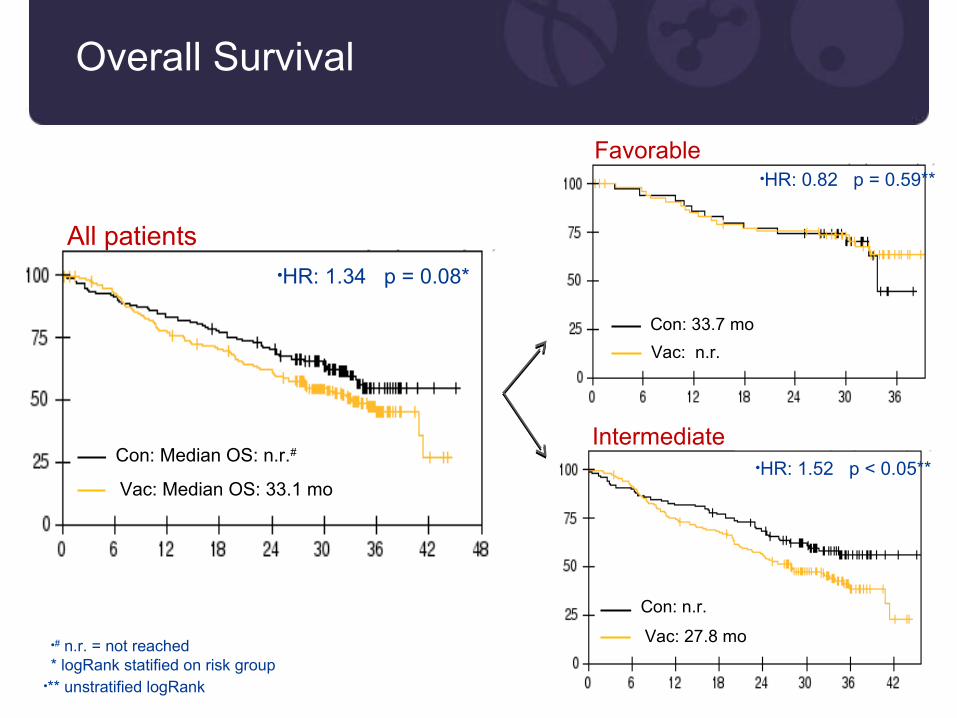
Overall Survival
•# n.r. = not reached* logRank statified on risk group
•HR: 1.34 p = 0.08*
Con: Median OS: n.r.#
Vac: Median OS: 33.1 mo
All patients
Con: 33.7 mo
Vac: n.r.
•HR: 0.82 p = 0.59**
Favorable
Con: n.r.
Vac: 27.8 mo
•HR: 1.52 p < 0.05**
Intermediate
•** unstratified logRank
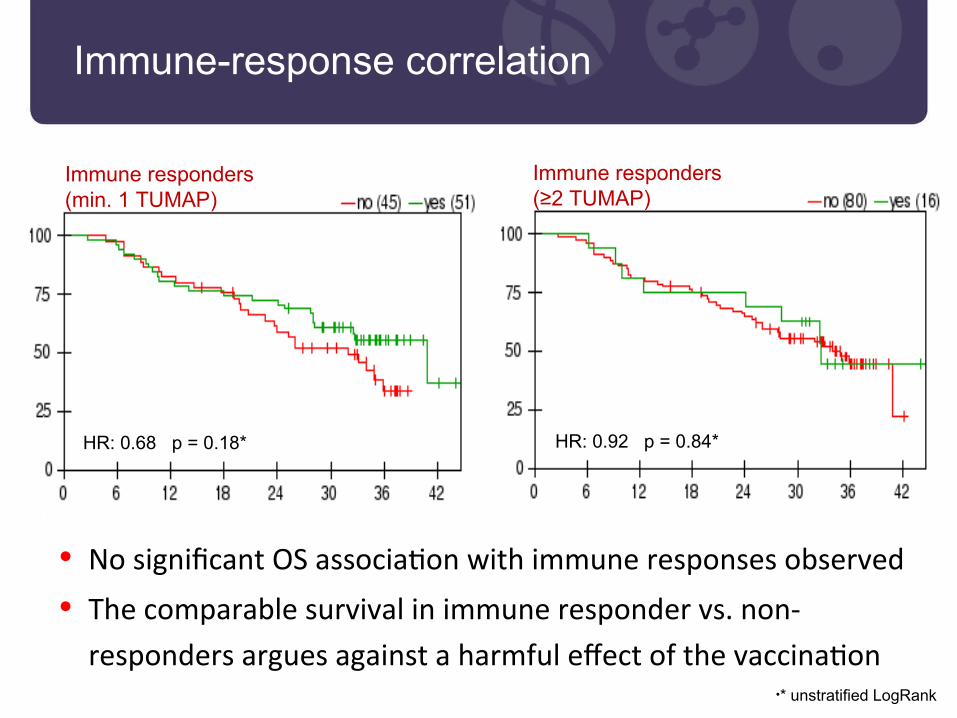
Immune-response correlation
• No signifcant OS associaton with immune responses observed
• The comparable survival in immune responder vs. non-
responders argues against a harmful efect of the vaccinaton•* unstratified LogRank
Immune responders(≥2 TUMAP)
HR: 0.92 p = 0.84*
Immune responders(min. 1 TUMAP)
HR: 0.68 p = 0.18*
Summary and Conclusions
• No improvement of OS when adding IMA901 to 1st line sunitnib
• An overall favorable safety profle of IMA901 was confrmed
• IMA901 with sunitnib resulted in impaired immune responses
• Specifc T cells with 3-fold lower frequency compared to phase 2
• No clear associaton of (weak) T cell responses with clinical outcome
• Immune responses need to be signifcantly improved before
further development of IMA901 is indicated
The Christie NHS Foundation Trust
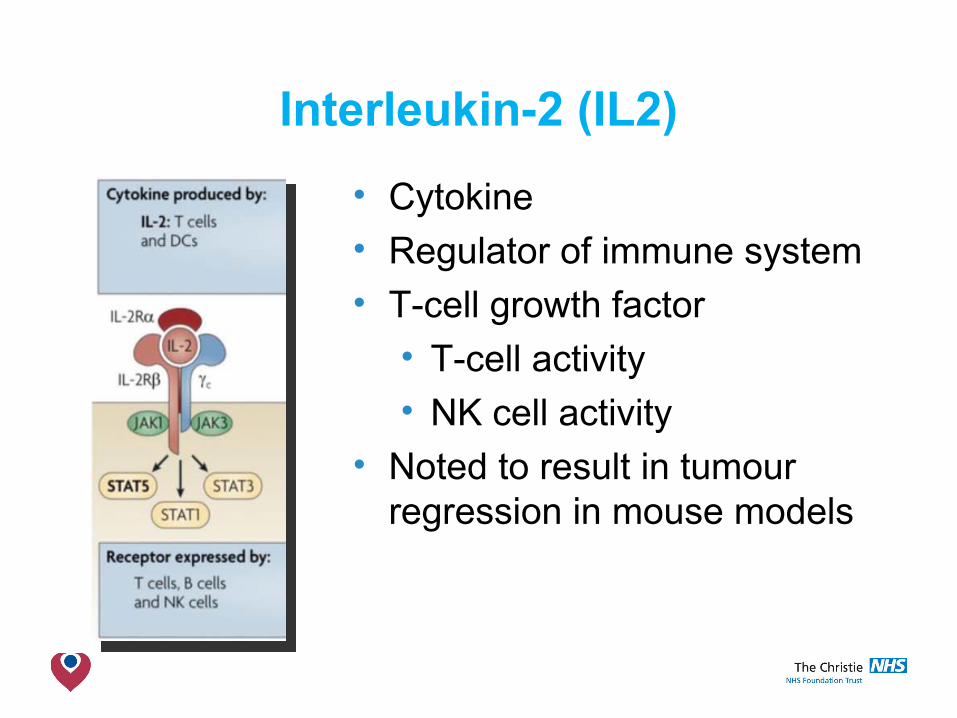
Interleukin-2 (IL2)
• Cytokine• Regulator of immune system• T-cell growth factor
• T-cell activity• NK cell activity
• Noted to result in tumourregression in mouse models
The Christie NHS Foundation Trust
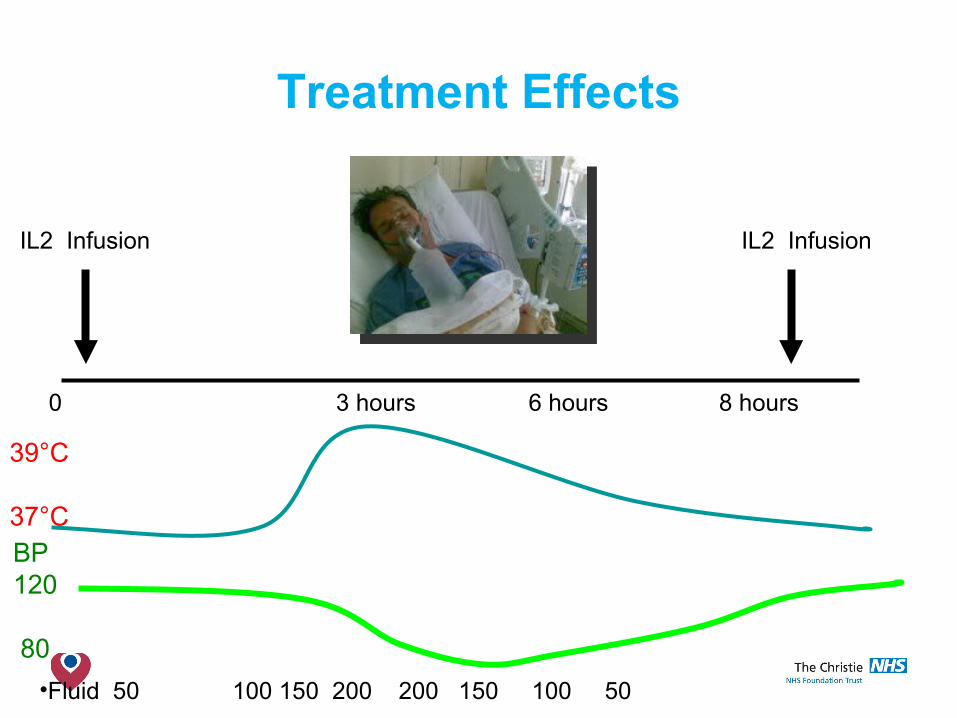
Treatment Effects
0 3 hours 6 hours 8 hours
IL2 Infusion
39°C
37°CBP120
80
•Fluid 50 100 150 200 200 150 100 50
IL2 Infusion
The Christie NHS Foundation Trust
HD IL2 toxicities• Fever• Hypotension• Tachycardia• Malaise
• Capillary leak syndrome• Oliguria• Nausea/vomiting• Diarrhoea• Thrombocytopenia
• Thyroid dysfunction• Arrhythmias• Myocarditis• Transaminitis• Confusion/hallucinations
The Christie NHS Foundation Trust
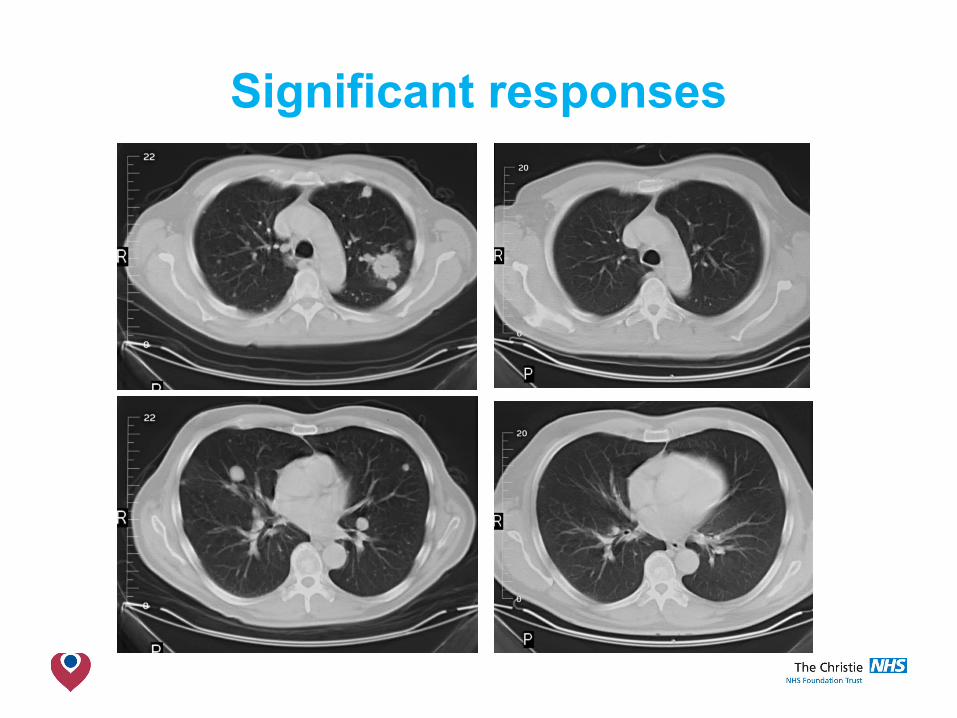
Significant responses
The Christie NHS Foundation Trust
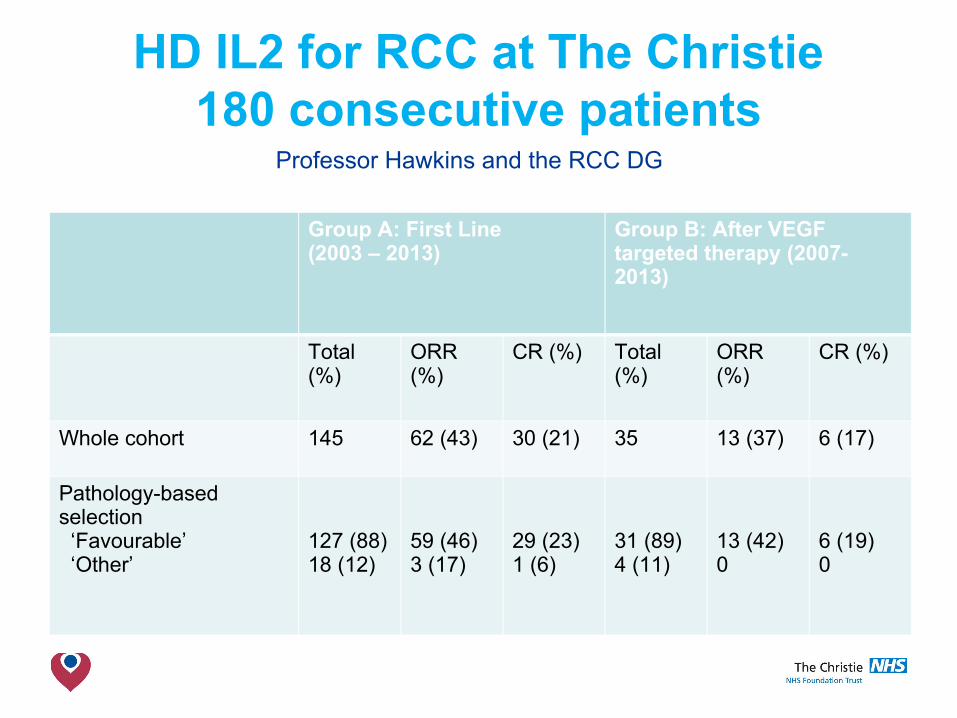
HD IL2 for RCC at The Christie180 consecutive patients
Group A: First Line (2003 – 2013)
Group B: After VEGFtargeted therapy (2007-2013)
Total(%)
ORR(%)
CR (%) Total(%)
ORR(%)
CR (%)
Whole cohort 145 62 (43) 30 (21) 35 13 (37) 6 (17)
Pathology-basedselection ‘Favourable’ ‘Other’
127 (88)18 (12)
59 (46)3 (17)
29 (23)1 (6)
31 (89) 4 (11)
13 (42)0
6 (19)0
Professor Hawkins and the RCC DG
The Christie NHS Foundation Trust
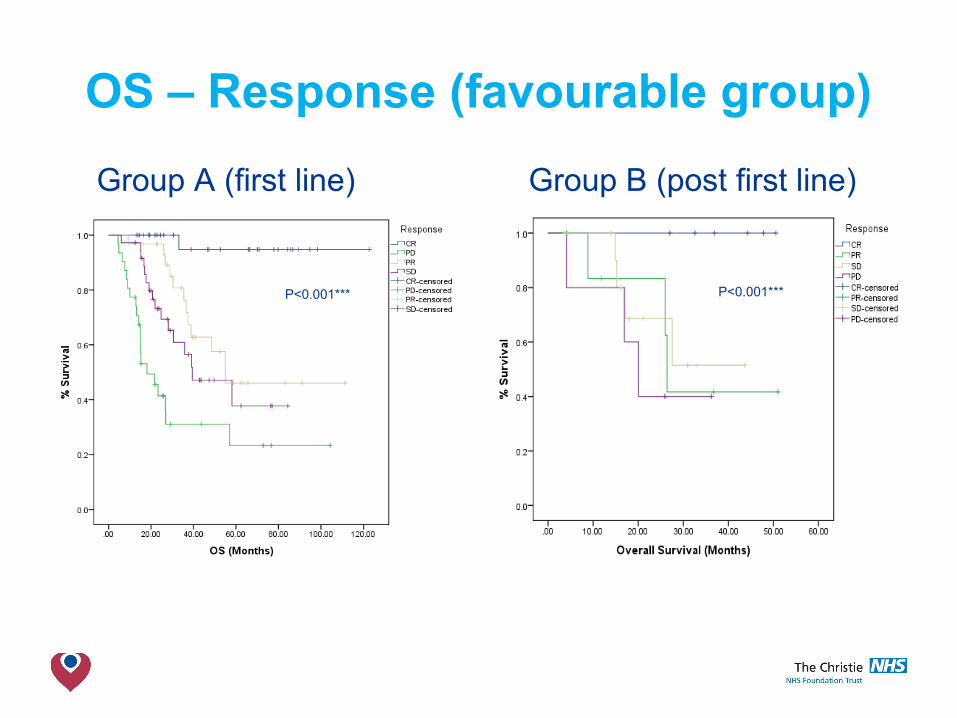
OS – Response (favourable group)
Group A (first line) Group B (post first line)
P<0.001*** P<0.001***
The Christie NHS Foundation Trust
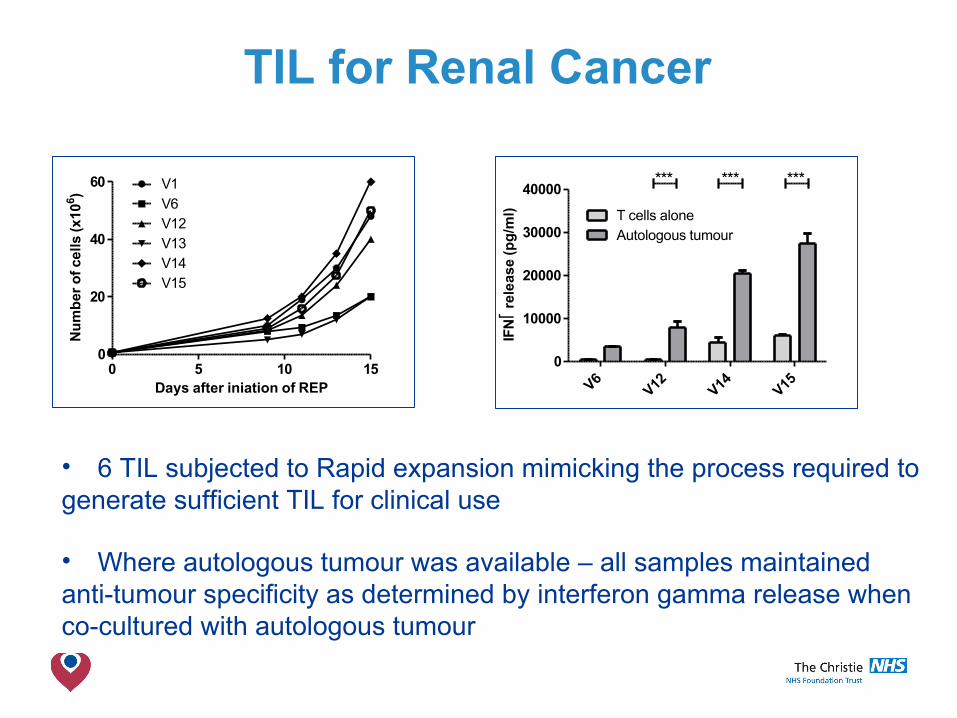
TIL for Renal Cancer
0 5 10 150
20
40
60 V1V6V12V13V14V15
Days after iniation of REP
Nu
mb
er o
f ce
lls (
x106 )
0
10000
20000
30000
40000
T cells aloneAutologous tumour
*** *** ***
IFN
rele
ase
(pg
/ml)
• 6 TIL subjected to Rapid expansion mimicking the process required to generate sufficient TIL for clinical use
• Where autologous tumour was available – all samples maintained anti-tumour specificity as determined by interferon gamma release when co-cultured with autologous tumour
The Christie NHS Foundation Trust
Conclusions• Renal cancer is at the centre of the
immunotherapy for cancer revolution• Still searching for the Holy Grail of maximum
durable response rate, with limited toxicities• HDIL2 in RCC can achieve the former but at the
cost of the later• Checkpoint inhibitors are shaping the future of
mainstream treatment for RCC• How they will be combined together/with
cytokines/with small molecues/Tcell therapyremains to be defined