Embed Size (px)
Citation preview
Atoms for better health care
Immunodiagnosis of parasiticinfectionsTools are evolving to help control diseases afflicting over 900 million people
by John B. Castelino
Parasitic infections are one of the world's majorcauses of human illness and suffering. Manifestations ofdisease range from the fevers of malaria to physicaldeformities, such as "river blindness" and elephantia-sis, resulting from infections by certain filarial worms.Parasitic diseases lower the productivity of the humanwork force, and some of the apathy encountered inregions where these diseases are endemic may bedirectly traced to such infections. In the extreme, deathresults, either as a direct consequence of the parasiticinfection or from viral, bacterial, nutritional or otherdiseases to which the body, weakened by the ravages ofparasitic infections, succumbs.
There is a growing acceptance of the importance ofhealth and quality of life in socio-economic develop-ment. Hence, increased international interest has beenfocused on research in the diseases of the tropics, nota-bly by the Special Programme on Research and Trainingin Tropical Diseases of the United Nations DevelopmentProgramme (UNDP), the World Bank, and the WorldHealth Organization (WHO). Five of the six diseasesselected for attention in the Special Programme are
Mr Castelino is a staff member in the Agency's Division of Life
Sciences.
caused by parasites — filariasis, leishmaniasis, malaria,schistosomiasis, and trypanosomiasis.
Despite this focus, the prevalence of parasitic infec-tions appears to remain high. Some 250 million personshave filariasis; a similar number, schistosomiasis; some400 million people live in malarial regions, with 50 mil-lion cases of malaria each year resulting in about onemillion deaths. The extension of development projects— such as irrigation and resettlement schemes — and thegrowing density of human populations in the tropics canbe expected to further worsen the situation unless effec-tive measures to control parasitic infections areimplemented.
So that control measures may be implemented, thereis a clear need for techniques that diagnose clinical infec-tions. Such techniques also are needed to study theepidemiology of the infection, i.e., the pattern of trans-mission in the community, and the detection of personswho have had the infection in the past or who are carry-ing the infection with few, if any, clinical signs ofdisease.
Classically, diagnosis has been based on microscopicexamination for parasites or their eggs in stool, urine,blood, or biopsy material. But for both diagnosis andepidemiology this approach is viewed increasingly as
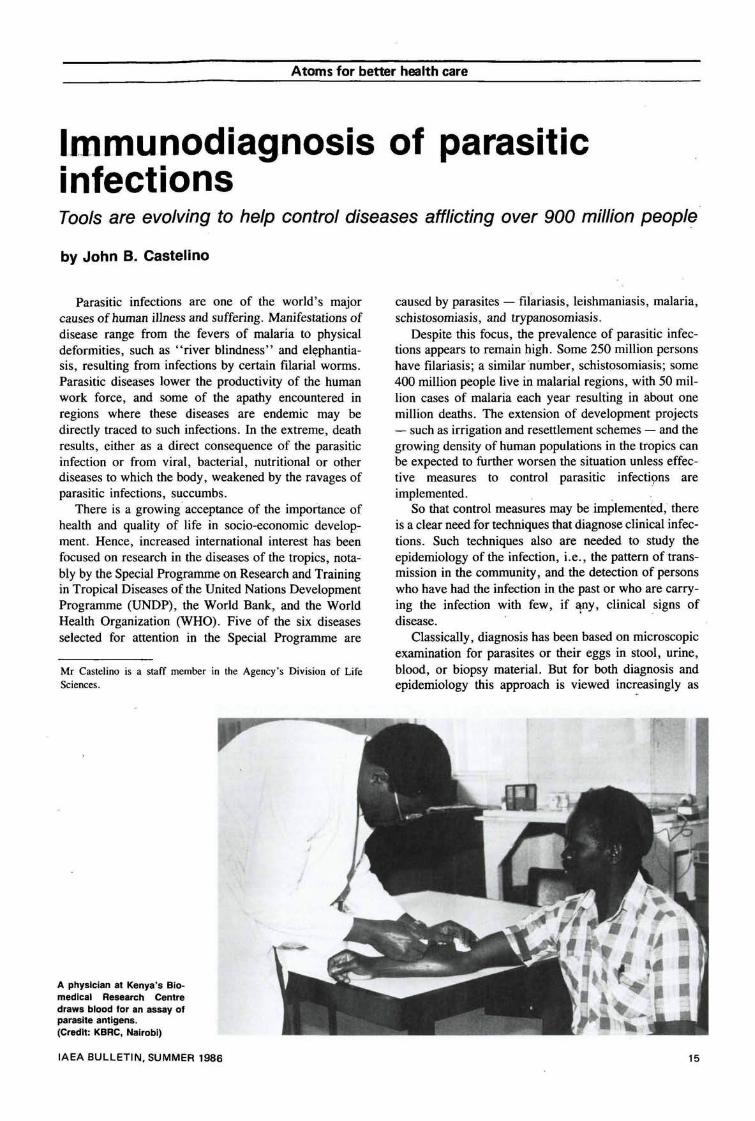
A physician at Kenya's Bio-medical Research Centredraws blood for an assay ofparasite antigens.(Credit: KBRC, Nairobi)
IAEA BULLETIN, SUMMER 1986 15

Atoms for better health care
impractical. This is particularly so when few, if any,parasites or their eggs are available in body fluids orstool for examination, such as in low intensity of infec-tion, in the early incubation period, in the late chronicstages of the infection, or in infections such as thosecaused by filarial worms in which the parasites may bepresent in body fluids only at certain times of the day.
Tools for diagnosis
One of the body's defenses against parasites is itsimmunological system. On or in parasites, and in theirsecretory or excretory products, are many proteins.Against some of these (antigens), the body is capable ofgenerating other complex protein molecules (antibodies)that neutralize the antigens by binding to them. Tech-niques that measure these antibodies or antigens providealternative tools for diagnosis. This method of diagno-sis, which uses the immunological binding reactionbetween antibodies and antigens, is termed immunodiag-nosis and the assays for measuring these antibodies orantigens, immunoassays.
During the 1960s, there was a recognition of the roleof immunoassays in the study of parasitic infections. Itwas seenjhat they had a place not only in the researchlaboratory but also in the field for immunodiagnosis andepidemiology. The most commonly used techniqueswere based on the reaction between antibodies and anti-gens that resulted in a visible agglutinated or precipitatedproduct. These techniques were found to be useful, butin some cases they lacked sensitivity. More recently,immunoassays that use reagents labelled with radio-nuclides, enzymes, or fluorescent substances havebecome popular because of their potentially high sensi-tivity in the detection of antigens and antibodies.
Radioimmunoassays (RIAs) and related procedurescould provide alternative diagnostic means to the classi-cal parasitological tests. The new assays should becheap, rapid, technically simple, and well adapted to thedemands of large-scale epidemiological surveys,particularly for evaluating the effects of the variousnational and international schemes of control.
The need for immunological tests is particularly greatin assessing the effectiveness of chemotherapy and indetecting infections in which few parasites are availablefor microscopic examination. The available tests forantibody detection appear to be poor in this respect.However, measurement of antibodies has the advantageof providing indications of the immune response of theinfected host. In those infections where specific antibod-ies are clearly involved in immune defense, as in malariaand schistosomiasis, immunoassays for antibodies canallow identification of protective responses. This may bean important clue to the strategy of research forimmunological control of parasitic infections.
Measurement of parasite antigens is a recent alterna-tive to antibody detection, and several research groupsare developing assay systems, often based on labelledantibodies. It now appears feasible to measure levels of
antigens released by parasites in host serum and urine,and through collaborative programmes the IAEA hashelped in the evaluation of such tests.
With the availability of enzyme and fluorochrometracers, consideration needs to be given to the choice oftracers. Radionuclide tracers provide easy quantitationof the antibody or antigen being measured. Moreover,because of the low non-specific signal in radioactivitymeasurements, radionuclide tracers are valuable particu-larly in the developmental stages of antigen detectionassays. Once the assay has been established, non-isotopic labels such as enzymes are equally suitable forroutine use. Indeed, such tracers offer advantages inmany circumstances with the result that radionuclidesmay play a diminishing role in the field.
Nevertheless, radionuclide tracers will not disappear.The cost of sophisticated equipment for measuring non-isotopic tracers is not lower than that of radioactivitycounters, and radionuclide counting equipment isalready widely available. The expertise developed by theAgency over the years in immunoassays usingradionuclides is immediately relevant to other tracers,and it will continue to play a role not only in developingsensitive assays but also in transferring the technology toless advanced Member States.
Radioimmunoassay: Important role
The basic immunoassay principles were establishedsome 30 years ago in studies on binding of radiolabelledinsulin to antibodies to insulin (anti-insulin antibodies).*The basis for the RIA was laid by the observation thatlabelled insulin can be displaced by unlabelled insulin inthe assay. The competition between the labelled andunlabelled insulin to bind to anti-insulin antibodies (theoutcome of which is predictably dependent on the rela-tive concentrations of the different reagents) led to theevolution of competitive binding assays. These havebeen used in a variety of situations for quantitation ofsubstances present in trace quantities in body fluids.
Immunoassays using an immunological reagent (anti-body or parasite antigen) and a radionuclide, an enzyme,or a fluorochrome, have a potential to play an importantrole in immunodiagnosis and epidemiology. Their sensi-tivity is high, they use minute amounts of parasite anti-gens or patient sera, they are applicable to large-scalesurveys, and they have the ability to yield quantitativeresults.
Objectives in immunodiagnosis
The objective of research in immunodiagnosis ofparasitic infections is to develop rapid, cheap, and tech-nically easy tests that can be used in epidemiological sur-veys to evaluate the effects of various national orinternational schemes of control in areas where parasiticinfections are endemic. It should provide tests that have
* S.A. Berson, R.S. Yallow, A. Bauman, M.A. Rothschild, andK. Newerly, Journal of Clinical Investigation 35 (1956).
IS IAEA BULLETIN, SUMMER 1986
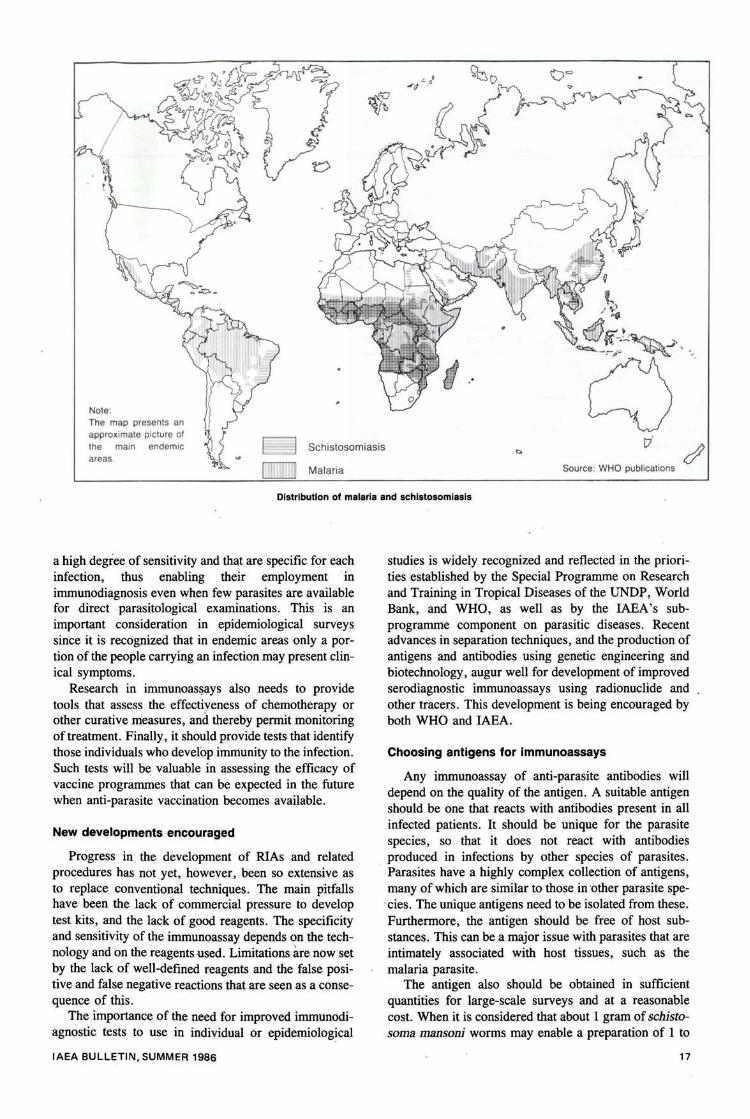
Note:The map presents anapproximate picture ofthe main endemicareas.
Schistosomiasis
Malaria Source: WHO publications
Distribution of malaria and schistosomiasis
a high degree of sensitivity and that are specific for eachinfection, thus enabling their employment inimmunodiagnosis even when few parasites are availablefor direct parasitological examinations. This is animportant consideration in epidemiological surveyssince it is recognized that in endemic areas only a por-tion of the people carrying an infection may present clin-ical symptoms.
Research in immunoassays also needs to providetools that assess the effectiveness of chemotherapy orother curative measures, and thereby permit monitoringof treatment. Finally, it should provide tests that identifythose individuals who develop immunity to the infection.Such tests will be valuable in assessing the efficacy ofvaccine programmes that can be expected in the futurewhen anti-parasite vaccination becomes available.
New developments encouraged
Progress in the development of RIAs and relatedprocedures has not yet, however, been so extensive asto replace conventional techniques. The main pitfallshave been the lack of commercial pressure to developtest kits, and the lack of good reagents. The specificityand sensitivity of the immunoassay depends on the tech-nology and on the reagents used. Limitations are now setby the lack of well-defined reagents and the false posi-tive and false negative reactions that are seen as a conse-quence of this.
The importance of the need for improved immunodi-agnostic tests to use in individual or epidemiological
studies is widely recognized and reflected in the priori-ties established by the Special Programme on Researchand Training in Tropical Diseases of the UNDP, WorldBank, and WHO, as well as by the IAEA's sub-programme component on parasitic diseases. Recentadvances in separation techniques, and the production ofantigens and antibodies using genetic engineering andbiotechnology, augur well for development of improvedserodiagnostic immunoassays using radionuclide andother tracers. This development is being encouraged byboth WHO and IAEA.
Choosing antigens for immunoassays
Any immunoassay of anti-parasite antibodies willdepend on the quality of the antigen. A suitable antigenshould be one that reacts with antibodies present in allinfected patients. It should be unique for the parasitespecies, so that it does not react with antibodiesproduced in infections by other species of parasites.Parasites have a highly complex collection of antigens,many of which are similar to those in other parasite spe-cies. The unique antigens need to be isolated from these.Furthermore, the antigen should be free of host sub-stances. This can be a major issue with parasites that areintimately associated with host tissues, such as themalaria parasite.
The antigen also should be obtained in sufficientquantities for large-scale surveys and at a reasonablecost. When it is considered that about 1 gram of schisto-soma mansoni worms may enable a preparation of 1 to
IAEA BULLETIN, SUMMER 1986 17
Atoms for better health care
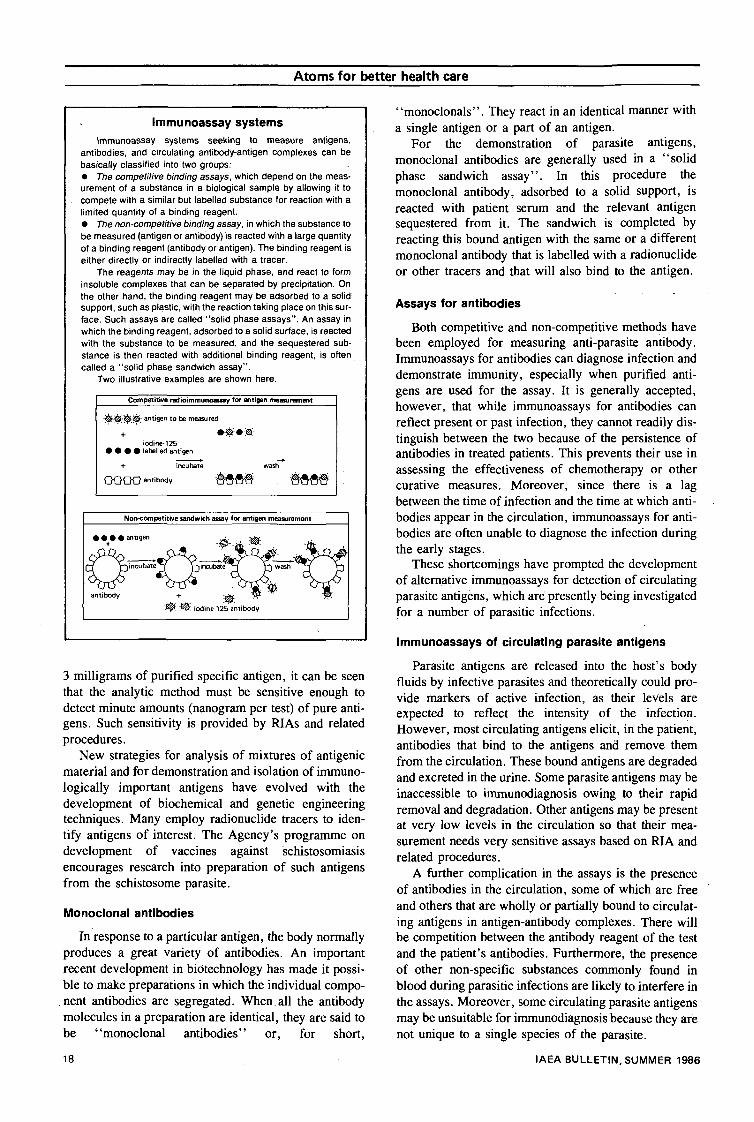
Immunoassay systemsImmunoassay systems seeking to measure antigens,
antibodies, and circulating antibody-antigen complexes can bebasically classified into two groups:• The competitive binding assays, which depend on the meas-urement of a substance in a biological sample by allowing it tocompete with a similar but labelled substance for reaction with alimited quantity of a binding reagent.• The non-competitive binding assay, in which the substance tobe measured (antigen or antibody) is reacted with a large quantityof a binding reagent (antibody or antigen). The binding reagent iseither directly or indirectly labelled with a tracer.
The reagents may be in the liquid phase, and react to forminsoluble complexes that can be separated by precipitation. Onthe other hand, the binding reagent may be adsorbed to a solidsupport, such as plastic, with the reaction taking place on this sur-face. Such assays are called "solid phase assays". An assay inwhich the binding reagent, adsorbed to a solid surface, is reactedwith the substance to be measured, and the sequestered sub-stance is then reacted with additional binding reagent, is oftencalled a "solid phase sandwich assay".
Two illustrative examples are shown here.
Competitive radioimmunoatsay for antigen measurement
H&r'$r$.- antigen to be measured
iodine-125• • • • labelled antigen
O O O O antibody
Non-competitive sandwich assay for antigen measurement
• • • • antigen
antibody
iodine-125 antibody
3 milligrams of purified specific antigen, it can be seenthat the analytic method must be sensitive enough todetect minute amounts (nanogram per test) of pure anti-gens. Such sensitivity is provided by RIAs and relatedprocedures.
New strategies for analysis of mixtures of antigenicmaterial and for demonstration and isolation of immuno-logically important antigens have evolved with thedevelopment of biochemical and genetic engineeringtechniques. Many employ radionuclide tracers to iden-tify antigens of interest. The Agency's programme ondevelopment of vaccines against schistosomiasisencourages research into preparation of such antigensfrom the schistosome parasite.
Monoclonal antibodies
In response to a particular antigen, the body normallyproduces a great variety of antibodies. An importantrecent development in biotechnology has made it possi-ble to make preparations in which the individual compo-nent antibodies are segregated. When all the antibodymolecules in a preparation are identical, they are said tobe "monoclonal antibodies" or, for short,
"monoclonals". They react in an identical manner witha single antigen or a part of an antigen.
For the demonstration of parasite antigens,monoclonal antibodies are generally used in a "solidphase sandwich assay". In this procedure themonoclonal antibody, adsorbed to a solid support, isreacted with patient serum and the relevant antigensequestered from it. The sandwich is completed byreacting this bound antigen with the same or a differentmonoclonal antibody that is labelled with a radionuclideor other tracers and that will also bind to the antigen.
Assays for antibodies
Both competitive and non-competitive methods havebeen employed for measuring anti-parasite antibody.Immunoassays for antibodies can diagnose infection anddemonstrate immunity, especially when purified anti-gens are used for the assay. It is generally accepted,however, that while immunoassays for antibodies canreflect present or past infection, they cannot readily dis-tinguish between the two because of the persistence ofantibodies in treated patients. This prevents their use inassessing the effectiveness of chemotherapy or othercurative measures. Moreover, since there is a lagbetween the time of infection and the time at which anti-bodies appear in the circulation, immunoassays for anti-bodies are often unable to diagnose the infection duringthe early stages.
These shortcomings have prompted the developmentof alternative immunoassays for detection of circulatingparasite antigens, which are presently being investigatedfor a number of parasitic infections.
Immunoassays of circulating parasite antigens
Parasite antigens are released into the host's bodyfluids by infective parasites and theoretically could pro-vide markers of active infection, as their levels areexpected to reflect the intensity of the infection.However, most circulating antigens elicit, in the patient,antibodies that bind to the antigens and remove themfrom the circulation. These bound antigens are degradedand excreted in the urine. Some parasite antigens may beinaccessible to immunodiagnosis owing to their rapidremoval and degradation. Other antigens may be presentat very low levels in the circulation so that their mea-surement needs very sensitive assays based on RIA andrelated procedures.
A further complication in the assays is the presenceof antibodies in the circulation, some of which are freeand others that are wholly or partially bound to circulat-ing antigens in antigen-antibody complexes. There willbe competition between the antibody reagent of the testand the patient's antibodies. Furthermore, the presenceof other non-specific substances commonly found inblood during parasitic infections are likely to interfere inthe assays. Moreover, some circulating parasite antigensmay be unsuitable for immunodiagnosis because they arenot unique to a single species of the parasite.
18 IAEA BULLETIN, SUMMER 1986
Atoms for better health care
IAEA's co-ordinated research programmeThe Agency's programme on immunodiagnosis is focused on
three parasitic infections — filariasis, malaria, and schistosomia-sis. Filariasis can be difficult to diagnose because the symptomsare often confused with those for other diseases. Moreover, theworms causing the infection may not produce the larvae whosepresence in the circulation forms the basis for diagnosis by classi-cal microscopic examination of a specimen of the patient's blood.Similar problems, although less acute, may also be presentedduring low chronic infections with malaria and schistosome para-sites or following incomplete cure of such infections.
The Agency's programme encourages the development ofimmunoassay methods that effectively detect and measure para-site antigens in blood, serum, and urine. It provides a frameworkfor collaborative research through which monoclonal antibodiesproduced against specific parasite antigens are screened forimmunodiagnostic potential using serum and urine from infectedand uninfected persons in endemic areas. Those monoclonalantibodies found to be suitable are then used in immunodiagnos-tic assays and related procedures to assess the applicability ofthe systems in endemic areas. Encouraging results are beingobtained through this programme.
Schistosomiasis
In schistosomiasis, a number of monoclonal antibodies withimmunodiagnostic potential have been produced by participantsin the programme: the University of Leiden, Netherlands; theInstitut Pasteur at Lille, France; and the Walter and Eliza HallInstitute for Medical Research at Melbourne, Australia. Some ofthese antibodies have been employed in sandwich assays wherethe same antibody is used for the solid phase and as the labelledantibody. These antibodies are unique for schistosomes. Theantibody can detect schistosome antigens in either the serum orthe urine of infected patients. This is an interesting result sinceurine collection is easier in epidemiological surveys than bloodsampling. Moreover, urine assays can be expected to circumventthe problem of interference by rheumatoid factors, immune com-plexes, and anti-parasite and anti-antibodies that are frequentlypresent in patient sera.
Filariasis and malaria
Several monoclonal antibodies have also been prepared atLille and Melbourne against filarial worms. The sandwich assay,using a combination of two such antibodies, will detect filarialantigens in patient sera. As in schistosomiasis, the accuracy ofthe test is better in urine samples since no overlap is found ininfected patients and in endemic controls.
In malaria, several monoclonal antibodies have been pre-pared at Mahidol University at Bangkok, Thailand and, in prelimi-nary evaluation, one of these has been shown to have a goodpotential for diagnosing malaria.
In addition to immunodiagnosis of parasitic infections in man,the Agency has a programme on monitoring malaria vectors.There are still gaps in our knowledge of the relative roles thatdifferent species of mosquitoes play in transmitting malaria.
The Agency's programme encourages the use of immunoas-says that can identify malaria sporozoites, the infective stages ofthe malaria parasite, in the salivary glands of mosquitoes. Theprogramme employs a monoclonal antibody that binds tosporozoite antigens. The antibody was prepared at the New YorkUniversity Medical Centre in the USA, and is used in a sandwichassay. In preliminary evaluation in Gambia, Burkina Faso, andMali, the assay has shown a good potential for large-scale fieldapplication. The assay can be expected to replace the classicalmicroscopical examination of salivary glands of freshly killedmosquitoes for assessing the presence of malaria sporozoites,since the sandwich assay is more rapid and can be performed ondry specimens of mosquitoes that have been stored for severalmonths. It allows the identification of the malaria species and pro-vides objective quantitative estimates of the sporozoite load. Thepersistence of malaria, especially in Africa, despite decades ofimplementing control strategies based on insecticides, reinforcesthe need for such an assay system that can be expected todevelop a better understanding of the dynamics and epidemiol-ogy of malaria.
Finally, the Agency has a programme that encourages theapplication of radiation techniques to immobilize anti-parasiteantibodies onto solid supports for use in immunoassays. Anti-schistosome antibodies provided by the Pasteur Institute, Lille,France, have been successfully immobilized onto polymer sup-ports by the Japan Atomic Energy Research Institute at Takasaki,Japan, and the Centre for Bio-engineering at the University ofWashington, USA. The immobilized antibody is stable at ambienttemperatures and retains much of its immunodiagnostic potency.
"Dip sticks" for the field
Epidemiological surveys involving collection of blood andurine for immunodiagnosis of infections are often carried out inareas far from a laboratory. The survey team spends several dayscollecting the samples before returning with these to a centrallaboratory for processing. This delay presents the problem ofkeeping the samples under refrigeration to avoid their deteriora-tion. The Agency's programme seeks to develop "dip sticks" forthose infections such as schistosomiasis, in which the uniqueparasite antigen present in the urine or serum is heat stable. Thedip sticks would be plastic strips with a stable antibody polymer-ized at one end that could be reacted with the urine or blood inthe field to sequester the antigen. The strip would then be driedand returned to a central laboratory for the immunoassay usingenzyme, fluorochrome, or radionuclide tracers.
Participants in an IAEA co-ordinated research pro-gramme are learning to usethe sandwich assay fordetecting malaria sporozoi-tes in mosquitoes. Trainingwas at the New York Univer-sity Medical Centre with par-ticipants from Nigeria,Kenya, Thailand, Egypt,Sudan, Mali, Sierra Leone,Netherlands, and the USA.
IAEA BULLETIN, SUMMER 1986 19