-
8/7/2019 Immunotherapy for Infection (2)
1/75
IMMUNOTHERAPY FOR
INFECTION
Dr. Ashutosh Srivastava
Moderator- Prof. Janak kishore
1
-
8/7/2019 Immunotherapy for Infection (2)
2/75
Introduction
History
Agents Mode of action
2
-
8/7/2019 Immunotherapy for Infection (2)
3/75
INTRODUCTION & HISTORY
alteration in immune system in order to combat
diseases,
enhance the immunity e.g. in Cancer immunotheray
degrade it for control of self injuries. E.g. For
infectious diseases.
Emil Behring and Shibasaburo Kitasato in
1890 showed passive transfer of immunity withtetanus1.
3
-
8/7/2019 Immunotherapy for Infection (2)
4/75
In 1930, Maxwell Finland reported the clinical
experience from 1919 through 1929 at Boston
City Hospital, using equine serum to treat
pneumococcal pneumonia.
During the 1930s and 1940s, passive
immunotherapy, transfer of the agent of immunity
from an immunized donor to an unimmunized
recipient, was used to prevent or modify thecourse of measles
and hepatitis A1.
4
-
8/7/2019 Immunotherapy for Infection (2)
5/75
5
-
8/7/2019 Immunotherapy for Infection (2)
6/75
6
-
8/7/2019 Immunotherapy for Infection (2)
7/75
7
-
8/7/2019 Immunotherapy for Infection (2)
8/75
MECHANISMS OF ACTION OF AGENTS
Preventing entry Ab mediated ( polyvalent /monoclonal)
APC potentiation
Prevention of replication- drugs
Immune response regulation & inflammation I
mmunosuppressant Cytokine antagonist
Receptor antagonism (binding protein & antagonistic
peptides)
Tolerance induction
Lymphocyte destruction
Hematopoietic stem cell transplantation
Killing the pathogen/ infected cell ADCC
CMI enhancement
Cytokine induction
Transfer of Tc / NK cells
8
-
8/7/2019 Immunotherapy for Infection (2)
9/75
MODE OF ACTION
The ability to deliver massive amounts of antibodyrapidly and
repeatedly has promptedinvestigations of new clinical uses
ofIgpreparations, including new uses as anti-infectiveagents1 .
Polyvalent IVIg Activation of complement & cytokine
Fc receptor modulation
Idiotype antibody production
T & B cell activation
9
-
8/7/2019 Immunotherapy for Infection (2)
10/75
IMMUNOTHERAPIES
Vaccines
Adjuvants (nonspecific immune stimulant)
Passive Antibody
(IVIG, humanized Mabs/ immunotoxins)
Cytokines or cytokine antagonists
(anti-TNF, soluble cytokine receptors)
Co-stimulator or suppressor signaling
molecules (CTLA-4)
10
-
8/7/2019 Immunotherapy for Infection (2)
11/75
AGENTS contd.
Adoptive transfer of immune cells
Immune Tc cells
Lymphokine activated NK cells
Antagonist peptides
(inhibit specific T cells by blocking TcR)
Oral tolerance(ingestion of antigen induces suppressive
factors[TGF-]
11
-
8/7/2019 Immunotherapy for Infection (2)
12/75
AGENTS contd. immunosupressive
Corticosteroids
(block cellular infiltration, cytokine release, T
cellmaturation, etc.)
Azathioprine
(inhibit lymphocyte proliferation)
Cyclosporine
(inhibit IL-2 gene expression) Anti-lymphocyte serum
(causes lymphocyte destruction and removal)
12
-
8/7/2019 Immunotherapy for Infection (2)
13/75
AGENTS contd.
Anti-CD3 & Anti CD4
(T cell destruction)
Cytotoxic drugs and ionizing radiation
(block cell proliferation, lymphopoiesis)
13
-
8/7/2019 Immunotherapy for Infection (2)
14/75
14
-
8/7/2019 Immunotherapy for Infection (2)
15/75
AGENTSAgents Rationale Status
Monoclonal Antibodies or Toxins Against T or B Cells
Anti-CD3 and T cell murine
monoclonal antibody (OKT3)
Inhibit T cell function;
induce T cell lymphopenia
FDA approved - ofcar iac an renal allograft
rejection
Diphtheria toxin-IL2 fusion protein Kills activated T cells FDA
approved for GVHD an transplant
repertoire; understudy to kill T regulatory cell
to embrace tumor vaccine efficacy
Humanized anti-CD3 monoclonal
antibody (hOKT3 gamma-1)
Eliminates auto-reactive T
cells
Human study underway in ype I ia etes,
psoriasis
Humanized anti-CD25 (IL-2R)
monoclonal antibody (daclizumab)
Eliminates activated T cells FDA approved for GVHD; studies
underway in
ulcerative colitis
Anti-CD40 ligand (CD154)
monoclonal antibody
Inhibit CD40-CD40 ligand ;
induces T cell tolerance
In primate trials for prevention of renal
allograft rejection
Humanized anti-CD20 (anti-B cell)
monoclonal antibody (rituximab)
Eliminates autoreactive B
cells
Human study underway for treatment of
AN A+ vasculitis
Humanized anti-IgE monoclonal
antibody (omalizumab)
Block allergy causing IgE Human study underway for allergy
(Hay
fever, allergic rhinitis)
15
-
8/7/2019 Immunotherapy for Infection (2)
16/75
Agents Rationale Status
Cytokines and Cytokine Inhibitors to Inhibit Immune Responses
and Inflammation
Anti-TNF- monoclonal antibody;humanized mouse chimeric
MAb, infliximab, fully humanized
MAb, adalimumab
Inhibit TNF- FDA approved for RA, Crohn's colitis(infliximab);
rheumatoid arthritis
(adalimumab)
Recombinant TNF-receptor-Ig
fusion protein (etanercept)
Inhibit TNF- FDA approved for RA, juvenile
rheumatoid arthritis, psoriasis
Recombinant IL-1 receptor
antagonist (IL-1Ra) (anakinra)
Inhibit IL-1
and -
FDA approved for rheumatoid arthritis
Soluble T Cell Molecule
Soluble CTLA-
4 protein
Inhibit CD28-B7-1 and B7-2
interactions; induces tolerance to
organ grafts; inhibit autoimmune T
cell reactivity in autoimmune
diseases
In trials for preventingGVHD in
BMT and for treatment of
psoriasis and systemic lupus
erythematosus
16
-
8/7/2019 Immunotherapy for Infection (2)
17/75
Agents Rationale Status
Intravenous Immunoglo in
IVIg Reticuloendothelial cell blockage;
complement inhibition; regulation ofidiotype/anti-idiotype
antibodies;
modulation of cytokine production;
modulation of lymphocyte production
FDA approved for Kawasaki's isease an I P;
treatment of GVHD, multiple sclerosis,myasthenia gravis, G S, an
chronic
inflammatory emyelinating polyneuropathy
supported by clinical trials
ytokines for Immune Reconstitution
IL-2 Induce proliferation of peripheral
memory CD4+ and CD8+ T cells
In trial for treatment of HIV infection
IL-7 Induce renewed thymopoiesis Under consideration for
treatment of disease
associated with cell eficiency
Hematopoietic Stem ell ransplantation
Hematopoietic stem
transplantation for immune
reconstitution
Remove pathologic
autoreactive immune system
and replace with less
autoreactive immunity
In clinical trials for systemic lupus
erythematosus, multiple sclerosis,
an sclero erma
17
-
8/7/2019 Immunotherapy for Infection (2)
18/75
CONSIDERATIONS
Need of therapy- mode? When?
Route of administration
Safety, dose Trials & diseases covered
Marketing & cost estimation
Future trend
18
-
8/7/2019 Immunotherapy for Infection (2)
19/75
NEED OF THERAPY
Prophylactic
Vaccination
Immunomodulation e.g. probiotics
Therapeutic
Rational of therapy
Population involved
19
-
8/7/2019 Immunotherapy for Infection (2)
20/75
USE OF POLYVALENT IVIG
20
-
8/7/2019 Immunotherapy for Infection (2)
21/75
RATIONAL OF THERAPY
conditions limitations
sis, m lidiosis,
s domonas / n mococcal
inf ction, T tc.
ndotoxins l ading to IC, T , m ltir sistant
HCV Poor tol ranc , costly, Genoty e dependent, no vaccine
H V Rec rrence of latent, high viral load, no vaccine, co
infection
with HIV
CMV Rec rrence of latent, high viral load, no vaccine
EBV Rec rrence, high viral load, no vaccine or therapy
HIV Virologic response b t not imm nologic, no vaccine
RSV No vaccine, significant infection
H5N1 Navepopulation, no vaccine
Fungal invasion Poor T cell immunity & PMN function, drug
toxicity & poor
bioavailability of drugs at site
Parasitic infections Limited drug options, drug resistance, no
vaccines, drug
toxicity,
General Immune incompetencee.g. BMT 21
-
8/7/2019 Immunotherapy for Infection (2)
22/75
POPULATION INVOLVED
Immunocompromised patients e.g. CGD. 10 disorder
Chronically infected persons e.g. HCV, HIV
Failure of available drug options e.g. TB, RSV, EBV
Multiple & complex ongoing therapy e.g. HAART
Poor immunologic response e.g. HIV
Research purposes.
22
-
8/7/2019 Immunotherapy for Infection (2)
23/75
PREREQUISITE BEFORE THERAPY
Exact diagnosis & co morbid conditions.
Full natural disease course
pathogenesis & molecular cross talk Immunological response
of human to agent
Suitable animal model & experiments
Clinical trials outcome
23
-
8/7/2019 Immunotherapy for Infection (2)
24/75
BACTERIAL IMMUNOTHERAPY
24
-
8/7/2019 Immunotherapy for Infection (2)
25/75
INTRAVENOS HYPERIMMUNE GLOBULIN
USED IN CLINICAL TRIALS FOR
INFECTIOUS DISEASES1
Pseudomonas aeruginosa
Cytomegalovirus
Grup B streptococus , J-5 Antiendotoxin*
Pneumococcal/ Haemophilus influenzae
Re Antiendotoxin*
* failed
25
-
8/7/2019 Immunotherapy for Infection (2)
26/75
GN SEPSIS
several anti-J-5 monoclonal antibodies are
evaluated in clinical trials1.
Role of polyvalent IVIG requires multicentre
RCT as contradicting results of various
studies2.
26
-
8/7/2019 Immunotherapy for Infection (2)
27/75
FOR TREATMENT OF BURKHOLDERIA
PSEUDOMALLEI1
gamma interferon (IFN-) very low doses ofIFN-
and ceftazidime elicited strong synergistic
inhibition1.
G-CSF was not effective when it was combined
with ceftazidime for the treatment ofB.
pseudomalleiinfection2.
27
-
8/7/2019 Immunotherapy for Infection (2)
28/75
S. AUREUS TSS.
ClassificationEffect on exotoxin at subgrowth inhibitory
concentrations
-lactam
Glycoprotein
Lipopepetide NA
Macrolide
Lincosamide
Oxazolidinone
Streptogramin NA
Aminoglycoside
Tetracycline
Sulfonamide NA
28
-
8/7/2019 Immunotherapy for Infection (2)
29/75
S. AUREUS
Reagent Mechanisms of action Supporting evidence
GML Inhibit growth of S.aureus
Delay the production of
exoproteins
Immunomodulation effects on
mammalian cells via membrane
stabilization
In vitro: GML reduces the production of
proinflammatory cytokines and chemokines by
epithelial cells in response to S. aureus and purified
TSST-1
In vivo: GML, as 5% vaginal gel, prevents lethality in
rabbits challenged vaginally with purified TSST-1
Tampon coated with GML reduces S. aureus growth,
exotoxin production and vaginal IL-8 secretion
Hemoglobin
subunit inhibitors
Target two-component and
quorum sensing systems to inhibit
exoprotein production [87]
In vitro: mixtures of and hemoglobin (1 g/ml)
inhibit S. aureus exoproteins[87]
In vivo: TSST-1 and -toxin were only detected in
tampon sections containing little or no menstrual
blood, despite the high bacterial counts [86]
V peptides (SEB
antagonists)
A synthesized immunoglobulin-
like peptide competes with the
particular TCR binding site to
prevent SEB-mediated T-cell
activation and lethality in rabbits
intravenously administered with
SEB [88]
In vivo: rabbits injected with V protein (dose 32.5
g/kg) survived through endotoxin enhancement
model of TSS[88]
The protective capacity of the V agent was 2000-
times greater than that ofIVIG
29
-
8/7/2019 Immunotherapy for Infection (2)
30/75
BacterialtargetPutativerolein
virulence
Proposedstrategy
(product/company)Trialconclusion
Capsule
polysaccharide
(CP5 and CP8)
Avoidance of
phagocytosis
Active immunization
(StaphVAX/Nabi)
Vaccine efficacy (57%) only last up to 40 weeks after
immunization in end-stage
renal disease (ESRD) hemodialysis patients (n = 1804). However,
no significant
protection was detected against bacteria in a confirmatory
follow-up trial (n = 3600)
Human polyclonal
antiserum(Altastaph/Nabi)
No reduction in preventing Staphylococcus aureus bacteremia in
very low-birth
weight (
-
8/7/2019 Immunotherapy for Infection (2)
31/75
MDR TUBERCULOSIS
low-dose Recombinant Human Interleukin-2 in
combination with multidrug chemotherapy1.
31
-
8/7/2019 Immunotherapy for Infection (2)
32/75
-
8/7/2019 Immunotherapy for Infection (2)
33/75
HCV INFECTION
a new albumin-conjugated IFN- (albIFN-). ableto extend its
half-life up to 6 days allowing it to beadministered once every 2-4
weeks.
consensus interferon (CIFN). an un-naturallyoccurring
recombinant type I interferon derivedfrom the alignment of a
variety of differentnaturally occurringIFN- subtypes. Initial
studies
have shown that CIFN is able to exert a ten- to100-fold
antiviral, antiproliferative and gene-inductive activities
33
-
8/7/2019 Immunotherapy for Infection (2)
34/75
HCV INFECTION
Toll-like Receptor Agonists- CPG 10101 and
isatoribine
CPG 10101 is a synthetic oligodeoxynucleotide
TLR9 agonist 2- Th1 induction- more emphasis on
cancer therapy.
Isatoribine, a TLR7 agonist3 stopped due to safety
concern
34
-
8/7/2019 Immunotherapy for Infection (2)
35/75
-
8/7/2019 Immunotherapy for Infection (2)
36/75
NEWER APPROACHES
36
-
8/7/2019 Immunotherapy for Infection (2)
37/75
CMV
limiting the load of latent viral genome should alsoreduce the
risk of virus recurrence & Antiviral CD8T cells prevented CMV
disease and accelerated
the resolution of productive infection3
. a preemptive CD8 T-cell immunotherapy of CMV
disease is in clinical trials1.
Generation of specific T cells by CMV peptide-
pulsed dendritic cells or genetically modifiedAPCs2, 4, 5
37
-
8/7/2019 Immunotherapy for Infection (2)
38/75
CMV CONTD.
treated eight patients with antiviral-resistantCMV reactivation,
and who had a CMV-
seropositive donor2 using Tc cells.
vaccine3 description Status
Towne Live attenuated Used in prim. Boost with DNA vaccine
gB Recombinant,
soluble
Phase II complete in healthy, Phase I in
Tx pt.
Canarypoxpp65
Live single cycleexpression
Phase I
Pp65, gB DNA plasmid Phase I
AlphaVax Alphavirus vector
with gB pp65
Phase I
38
-
8/7/2019 Immunotherapy for Infection (2)
39/75
FOR HSV
Agonist to TLR 3 & 7, have been used
transientlyeffective.
imiquimod (Aldara), an imidazoquinoline amine
analog to guanosine and a TLR7 agonist the cocirculation of HIV
has provided a great
challenge for researchers and healthcareproviders to develop
HSV-2 therapies that either
do not increase HIV-1 susceptibility or replication,or
simultaneously protect against both infections1.
39
-
8/7/2019 Immunotherapy for Infection (2)
40/75
HSV contd..
In recent Phase III clinical trials of a recombinantglycoprotein
D vaccine, approximately 74%prevention of genital HSV disease was
observed
but only in women seronegative for both serotypesof HSV1.
TLR-mediated immunomodulation and vaccinesconjugated to TLR
agonists enhance resistance to
genital HSV-2 infections but additional work isrequired to
dissect their impact on HIV-1infections.
40
-
8/7/2019 Immunotherapy for Infection (2)
41/75
EBV
Adoptive transfer of T cells in trials.
41
-
8/7/2019 Immunotherapy for Infection (2)
42/75
FOR HIV
how should we treat patients who respond
virologically but not immunologically?
A study by Katlama and colleagues, in France
suggests that interleukin-2 (IL-2) may be an
option1. still do not know whether an IL-2-
induced CD4+ cell increase will prove clinically
beneficial.
42
-
8/7/2019 Immunotherapy for Infection (2)
43/75
Interleukin-7 is currently in clinical trials to treat
cancer and infection with hepatitis C virus and
HIV.
immunotherapy will probably be tailored to the
individual patient on the basis of specific
laboratory or clinical findings.
43
-
8/7/2019 Immunotherapy for Infection (2)
44/75
RSV
Mortality 50% if treated with ribavirin in
posttransplant pt. & pt. on chemotherapy.
Lack of effective vaccine
RSV immunoglobulin (RSVIG) asimmunoprophylaxis in high
risk1.
44
-
8/7/2019 Immunotherapy for Infection (2)
45/75
FOR H5N1
specific equine anti-H5N1 IgGs from horses
vaccinated with inactivated H5N1 virus, and
then obtained the F(ab')2 fragments by
pepsin digestion ofIgGs1.
On mice model. Fit to human trial.
45
-
8/7/2019 Immunotherapy for Infection (2)
46/75
FUNGAL IMMUNOTHERAPY
46
INTERFERON Gamma IMMUNOTHERAPY FOR INVASIVE
-
8/7/2019 Immunotherapy for Infection (2)
47/75
INTERFERON-Gamma IMMUNOTHERAPY FOR INVASIVE
FUNGAL INFECTIONS IN KIDNEY TRANSPLANT PATIENTS1
in nonneutropenic solid organ transplant patients
T cell-mediated immune defects are becoming anincreasingly
important risk factor for IFIs.
compared to standard approaches, the accelerated cureof life
threatening, disseminated IFIs with 6 weeks of
combination antifungal drug therapy andIFN-immunotherapy saved
lives, retained allograft function
and led to substantial cost savings in this small
patientgroup.
In 2005,published the case report of a renal transplantpatient
in whom disseminated cryptococcal disease wascured only after the
addition of recombinant IFN-therapy.
human IFN-, 200 g subcutaneously; 3/week 47
-
8/7/2019 Immunotherapy for Infection (2)
48/75
Notably, a patient with disseminated (includingcerebral)
aspergillosis (mortality 90%) and apatient with disseminated
(including cerebral)
O. gallopavum infection (mortality previously100%) were
cured.
Intranasal Granulocyte-Macrophage Colony-Stimulating Factor
Reduces the Aspergillus
Burdeninan Immunosuppressed MurineModel of Pulmonary
Aspergillosis1.
48
-
8/7/2019 Immunotherapy for Infection (2)
49/75
FOR P. JEROVACII1
Anti-P. carinii hyperimmune serum was highly
effective at reducing the number of P. Jerovacii
organisms in early, intermediate, and advanced
stages of PCP and was capable of increasing
the mean life expectancy.
On SCID mice.
49
-
8/7/2019 Immunotherapy for Infection (2)
50/75
PARASI I RAPY
50
-
8/7/2019 Immunotherapy for Infection (2)
51/75
FOR VISCERAL LEISHMANIASIS
Modulation of T-Cell Costimulation
injection of agonist anti-CD40 monoclonal
antibody (MAb) induced killing of60% of
parasites within liver macrophages, stimulated
gamma interferon (IFN-) secretion, and
enhanced mononuclear cell recruitment and
tissue granuloma formation. anti-CD40 and anti-CTLA-41.
51
-
8/7/2019 Immunotherapy for Infection (2)
52/75
LEISAHMANIA .
immunotherapy with cytokines (interleukin-12
and interferon-).
The frequency of asymptomatic
infections needs to identify the deficiencies in
the host or the parasite-induced responses that
predispose phenotypically normal persons to
progressive disease.
52
-
8/7/2019 Immunotherapy for Infection (2)
53/75
CRYPTOSPORIDIOSIS
Anti-CSL MAb 3E2 had the highest protective
activity of all Mabs, reducing infection levels by
62 to 92%. 3E2 combined with anti-GP25-200
MAb 3H2 and anti-P23 MAb 1E10 conferred
significant additive protection over that
provided by the individual MAbs and reduced
infection levels by 86 to 93%
53
-
8/7/2019 Immunotherapy for Infection (2)
54/75
TRYPANOSOMA CRUZI
DNA Vaccines in Mice
54
-
8/7/2019 Immunotherapy for Infection (2)
55/75
BONE MARROW TRANSPLANTATION
IGIV, 500 mg per kilogram weekly1, from 7 to90 days after
transplantation, the incidence ofgram negative septicemia and viral
infections
was reduced substantially in the globulinprophylaxis group.
the incidence of interstitial pneumonitis wasconsiderably
reduced by the globulin
prophylaxis, as was that of graftversus- hostdisease for
patients older than 20 years.
55
-
8/7/2019 Immunotherapy for Infection (2)
56/75
SAFETY
56
-
8/7/2019 Immunotherapy for Infection (2)
57/75
SAFETY
Drawbacks of polyclonal immunoglobulin therapy1
1. High dosage required
2. Safety of plasma-derived product
3. Product standardization
4. Product availability
monoclonal antibodies contain foreign protein and cansensitize
human recipients.
dilemma pertaining to monoclonal antibodies of any
source is the potential for anti-idiotypic antibodyformation.
Anti-id antibodies may neutralize the activityof the monoclonal if
used in a prolonged fashion.
57
-
8/7/2019 Immunotherapy for Infection (2)
58/75
Isolated y-globulin preparations tend to form small
aggregates
spontaneously and these can lead to severe anaphylactic
reactions when administered intravenously, on account of
theirability to aggregate platelets and to activate complement
and
generate C3a and C5a anaphylatoxins. For this reason, the
material were injected intramuscularly1.
Preparations free of aggregates are available, and separatepools
with raised antibody titers to selected organisms such as
vaccinia, herpes zoster, tetanus and perhaps rubella would
be
available soon.
Four Cases of Disseminated Mycobacterium bovis Infection
FollowingIntravesical BCGInstillation for Treatment of
Bladder
Carcinoma2 .
58
-
8/7/2019 Immunotherapy for Infection (2)
59/75
HUMANIZED MONOCLONAL ANTIBODIES
Use of mouse monoclonal antibodies for immunotherapyin humans is
limited by immune responses in humans
against the foreign mouse antibody proteins.
Complementarity determining regions (CDR) of mouse
monoclonal antibodies can be grafted onto theframework of a
human immunoglobulin. Recombinant
antibodies are less immunogenic and induce less allergic
reactions.
59
-
8/7/2019 Immunotherapy for Infection (2)
60/75
60
-
8/7/2019 Immunotherapy for Infection (2)
61/75
IL- 12 AS AGENT
has adjuvant activity when it is co delivered withDNA vaccines.
systemic IL-12 therapy has beenlimited by high levels of
toxicity.
The activity was greater with the single polypeptidescIL-12. An
antigen-specific cellular response (i.e.,secretion of Th1
cytokines, IL-2, and IFN-) elicitedby a recombinant L. lactis
straindisplaying a cellwall-anchored human papillomavirus type 16
E7
antigen was dramatically increased bycoadministration with an L.
lactis strain secretingIL-12 protein.
61
-
8/7/2019 Immunotherapy for Infection (2)
62/75
EFFICACY
efficacy of immunotherapy was dependent
upon two conditions.
First, an accurate microbiologic diagnosis,
including serotyping, was necessary. And
second, therapy had to be administered early in
the course of infection.
62
-
8/7/2019 Immunotherapy for Infection (2)
63/75
FUTURE TRENDS
63
-
8/7/2019 Immunotherapy for Infection (2)
64/75
64
SUMMARY OF CHIMPANZEE IMMUNIZATION AND
-
8/7/2019 Immunotherapy for Infection (2)
65/75
SUMMARY OF CHIMPANZEE IMMUNIZATION AND
CHALLENGE STUDIES FOR HCV1
Vaccine Immune response Challenge results
Recombinant gpE1/gpE2 in
oil/water adjuvants
Humoral immune response
induced in chimpanzees
Five out of seven chimpanzees showed
sterilizing immunity againsthomologous HCV challenge
DNA prime followed by protein
boost (E1, E2, core and NS3)
Humoral and cellular
immune responses induced
in chimpanzees
One out of two cleared infection
following heterologous challenge
Recombinant gpE1/gpE2 Humoral and cellular
immune responses inchimpanzees
The only chimpanzee studied became
persistently infected
DNA prime-adenoviral boost (core,
E1, E2, NS3-NS5)
Humoral and cellular
immune responses in
chimpanzees
Two out of six did not proceed to
chronic infection upon slightly
heterologous HCV challenge, one had
sterilizing immunity; one resolved
infection
Adenoviral prime-DNA boost (NS3-NS5)
Induced cellular immuneresponses in chimpanzees
Four out of five resolved infection uponheterologous
challenge
DNA prime-MVA boost (core, E1,
E2 andNS3)
Humoral and cellular
immune responses in
chimpanzees
Three out of four became chronically
infected upon homologous challenge
Recombinant HCV virus-like
particles (core, E1 and E2)
Cellular immune responses
and weak humoralresponses in chimpanzees
Two out of four HCV RNA negative 2
years following homologous challenge65
-
8/7/2019 Immunotherapy for Infection (2)
66/75
THERAPEUTIC HCV VACCINES
InnoVac- (recom inant gpE1)-Humoral and cellular immune
responses induced in both healthy and chronically
infected individuals; no significant reduction in HCV RNA levels
in chronically infected
individuals
I -41 (pepti e- ase vaccine containing eight ifferent epitopes
erive from NS3,
core an NS4)-Cellular immune responses in both healthy and
chronically infected
individuals; small but significant reduction in viral load in
chronically infected
individuals
hron ac- ( N vaccine enco ing NS3; electroporation elivery)-
Cellular immune responses induced in one chronically infected
individual
66
-
8/7/2019 Immunotherapy for Infection (2)
67/75
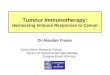
BloodMonocytes
IL-4 + GM-CSF
ImmatureDendritic cells
Peptide +
MatureDendritic cells
Inject i.v.
Freeze forboosts
LPS
Poly I:C
CpG oligoTNFE
CD40L
TLR
ligands
Making dendritic cell vaccines
67
-
8/7/2019 Immunotherapy for Infection (2)
68/75
INFECTIOUS AGENTS & OTHERS AS
IMMUNOTHERAPEUTICS
68
-
8/7/2019 Immunotherapy for Infection (2)
69/75
USE OF LISTERIA MONOCYTOGENES
an irreversibly attenuated and highly
immunogenic L. monocytogenes platform,the
L. monocytogenes dal-,dat-,andactA-deleted
strainthatexpresses the human prostate-specific antigen (PSA)
using an antibiotic
resistance marker-free plasmid1.
Oral Immunotherapy With H. InfluenzaeReduces Severity of COPD
Flares2 .
69
-
8/7/2019 Immunotherapy for Infection (2)
70/75
MACROLIDES AS IMMUNOMODULATORY
MEDICATIONS1-
their long-term use in treating neutrophil-dominated
inflammation in diffusepanbronchiolitis, bronchiectasis,
rhinosinusitis, and cystic fibrosis. due to inhibition of
extracellular signal-
regulated kinase 1/2 (ERK1/2)phosphorylation and nuclear factor
kappa B
(NF- B) activation. A concern is that long-termuse of macrolides
increases the emergence ofantimicrobial resistance.
70
-
8/7/2019 Immunotherapy for Infection (2)
71/75
TO SEARCH
9. Doherty, T. M., and A. Sher. 1998. IL-12 promotes
drug-inducedclearance ofMycobacteriumavium infectioninmice. J.
Immunol.160:54285435.
Onyeji, C. O., K. Q. Bui, D. P. Nicolau, C. H. Nightingale, L.
Bow, and R.Quintiliani. 1999. Influence of adjunctive
interferon-gamma on
treatment of gentamicin- and vancomycin-resistantE
nterococcusfaecalis infectioninmice. Int. J. Antimicrob. Agents
12:301309.
Pammit, M. A., V. N. Budhavarapu, E. K. Raulie, K. E. Klose, J.
M.Teale, and B. P. Arulanandam. 2004. Intranasal
interleukin-12treatment promotes antimicrobial clearance and
survival inpulmonary Francisella tularensis subsp. novicida
infection.A
ntimicrob.Agents Chemother.
48:4513
4519
.
71
-
8/7/2019 Immunotherapy for Infection (2)
72/75
OTHERS
72
S l bl MHC tid t t i l b d t d t t ifi T ll
-
8/7/2019 Immunotherapy for Infection (2)
73/75
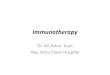
Soluble MHC-peptide tetrameric complexes can be used to detect
specific T cells
E1E2
E3 F2M
E1E2
E3 F2M
Membrane
DomainBiotin
Natural Class I1HC Soluble Class I1HCPeptide
Avidin
PE
Fluorescent MHC-peptide
Tetrameric complex
73
-
8/7/2019 Immunotherapy for Infection (2)
74/75
Human normal immunoglobulin (HNIG) is derivedfrom the pooled
plasma of donors and containsantibodies to infectious agents that
are currentlyprevalent in the general population. HNIG is usedfor
the protection of immunocompromised childrenexposed to measles and
of individuals afterexposure to hepatitis A.
Specific immunoglobulins are available fortetanus, hepatitis B,
rabies and varicella zoster
74
-
8/7/2019 Immunotherapy for Infection (2)
75/75
successful use ofIFN- in the treatment of thephagocytic cell
defect in chronic granulomatousdisease.
Intermittent infusions ofIL-2 in HIV-infectedindividuals in the
early or intermediate stages ofdisease have resulted in substantial
and sustainedincreases in CD4+ T cells.
CTLA-4 protein into clinical trials- block T cellactivation via
TCR/CD28 ligation during organ orbone marrow transplantation .