Embed Size (px)
Citation preview

Impact of Magnetic Resonance Imaging on the Diagnosis of Abdominal Complications of Paroxysmal Nocturnal Hemoglobinuria
By Didier Mathieu, Alain Rahmouni, Patricia Villeneuve, Marie Christine Anglade, Henri Rochant, and Norbert Vasile
Magnetic resonance (MR) imaging is a method of choice for assessing vascular patency and parenchymal iron overload. During the course of paroxysmal nocturnal hemoglobinuria (PNH), it is clinically relevant to differentiate abdominal vein thrombosis from hemolytic attacks. Furthermore, the study of the parenchymal MR signal intensity adds informations about the iron storage in kidneys, liver, and spleen. Twelve PNH patients had 14 MR examinations of the abdomen with spin-echo T1- and T2-weighted images and flow-sensitive gradient echo images. Vessels patency and parenchymal sig- nal abnormalities-either focal or diffuse-were assessed. MR imaging showed acute complications including hepatic vein obstruction in five patients, portal vein thrombosis in
AROXYSMAL nocturnal hemoglobinuria (PNH) is a rare acquired disorder of a hematopoetic stem cell
caused by a mutation within the phosphatidyl inositol gly- can-class A (PIG-A) gene resulting in an abnormal glycosyl- phosphatidylinositol anchor that is unable to bind membrane functional proteins. Among these proteins, the inhibitors of complement play a key role in protecting the blood cells from complement cascade attack. The lack of these proteins in PNH explains the characteristic chronic hemolysis with occurrence of acute intravascular hemolytic exacerba- tions.”3 However, the most serious and life-threatening com- plication of PNH is thrombosis of intraabdominal veins. An increased sensitivity of PNH platelets to activation by the terminal complement proteins may explain in part these thrombotic complications? Distinguishing acute hemolytic attacks from abdominal venous thrombosis may be of critical importance for therapy. Abdominal venous thrombosis can involve the hepatic veins with subsequent Budd Chiari syn- drome (BCS), the portal vein, and the mesenteric and splenic veins.5,6 Multiple imaging modalities have been used for the evaluation of these vascular thromboses including ultraso- nography (US), angiography, and computed tomography (CT).’,’ During these acute complications, US examination is frequently limited by ascitis and bowel gas distension. In addition, iodinated contrast agents, used on angiography and CT, may induce acute hemolysis during PNH.q3’o Magnetic resonance (MR) imaging, on the contrary, is a safe and sensi- tive method for the diagnosis of abdominal venous thrombo- sis.”.” Previous occasional MR case reports have empha- sized the abnormal signal intensity of kidneys in PNH.’’-l6 The purposes of this study including 12 patients with PNH were twofold: to assess the value of MR imaging in the diagnosis of these acute abdominal complications and to clarify the appearances and, particularly, the significance of the abnormal signal intensities observed in the kidneys, liver, and spleen. In this study, we have not formally compared MR imaging with the other radiologic methods.
P
MATERIALS AND METHODS
From January 1991 to June 1994, 14 MR examinations were per- formed in 12 patients with PNH, 6 women and 6 men aged from 18 to M) years old (mean, 30 years). The diagnosis of PNH was confirmed
Blood, Vol 85, No 11 (June l), 1995: pp 3283-3288
two patients, splenic infarct in one patient. In one patient treated with androgens, hepatocellular adenomas were shown. Parenchymal iron overload was present in the renal cortex of eleven patients with previous hemolytic attacks. On the first MR study of the remaining patient with an acute abdominal pain showing PNH, no iron overload was present in the renal cortices. Follow-up MR imaging showed the on- set of renal cortex iron overload related to multiple hemo- lytic attacks. Despite the fact that all our patients were trans- fused, normal signal intensity of both liver and spleen was observed in three of them. MR imaging is particularly helpful for the diagnosis of abdominal complications of PNH. 0 1995 by The American Society of Hematology.
by a positive Ham test (acid hemolysis test) and a positive sucrose hemolysis test. According to the clinical presentation, three groups of patients underwent MR examination: (1) in the first group, MR imaging was performed during an acute abdominal pain occuning in previously diagnosed PNH patients (6 patients, Table 1); (2) in the second group, MR imaging was performed in the follow-up of previously diagnosed PNH patients without current acute clinical symptoms (5 patients, Table 2); and (3) MR imaging was performed in a patient presenting with an acute abdominal pain showing PNH dsease (Table 3).
In the first group (Table l ) , the duration of PNH before the onset of the acute episode varied from 1 to 6 years. All six patients experi- enced previous multiple hemolytic attacks, infections, and thrombo- sis including episodes of hepatic vein obstructions (patients no. 1 and 2), or cerebral vein thrombosis (patients no. 4 and 6). All have been treated by blood transfusions and androgens.
In the second group (Table 2), the duration of PNH before the MR examination varied from 5 to 14 years. All five patients also experienced previous multiple hemolytic crisis, infections, and thrombosis including renal vein thrombosis (patient no. IO), cerebral vein thrombosis (patient no. 1 I ) , and episodes of hepatic vein ob- structions (patient no. 8). All five patients were treated by blood transfusions and androgens.
In an 18-year-old woman (patient no. 12, Table 3) with an acute abdominal pain, a portal thrombosis was diagnosed. The course of PNH was thereafter marked by multiple acute hemolytic attacks with gross hemoglobinuria. This patient was treated by blood transfusions (10 to 12 U/mo). For evaluation of abdominal pains, follow-up MR examina- tions were performed at 3 and 8 months after the initial MR study.
All 12 patients were examined by MR with a 1.5-T magnet (Mag- netom SP 63; Siemens, Erlangen, Germany). MR examinations were performed without intravenous injection of paramagnetic contrast agent. These successive axial transverse images were obtained: (1 )
From the Departments of Radiology and Hematology, Hripital Henri Mondor, 51, avenue du Mare‘chal de Luttre de Tassigny, 94010 Cre‘teil, France.
Submitted October I , 1994; accepted January 6, 1995. Address reprint requests to Didier Mathieu, MD, Department of
Radiology, Hapita1 Henri Mondor, 51, avenue du Marechal de Luttre de Tassigny, 94010 Cre‘teil, France.
The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8511-0009$3.00/0
3283
3284 MATHIEU ET AL
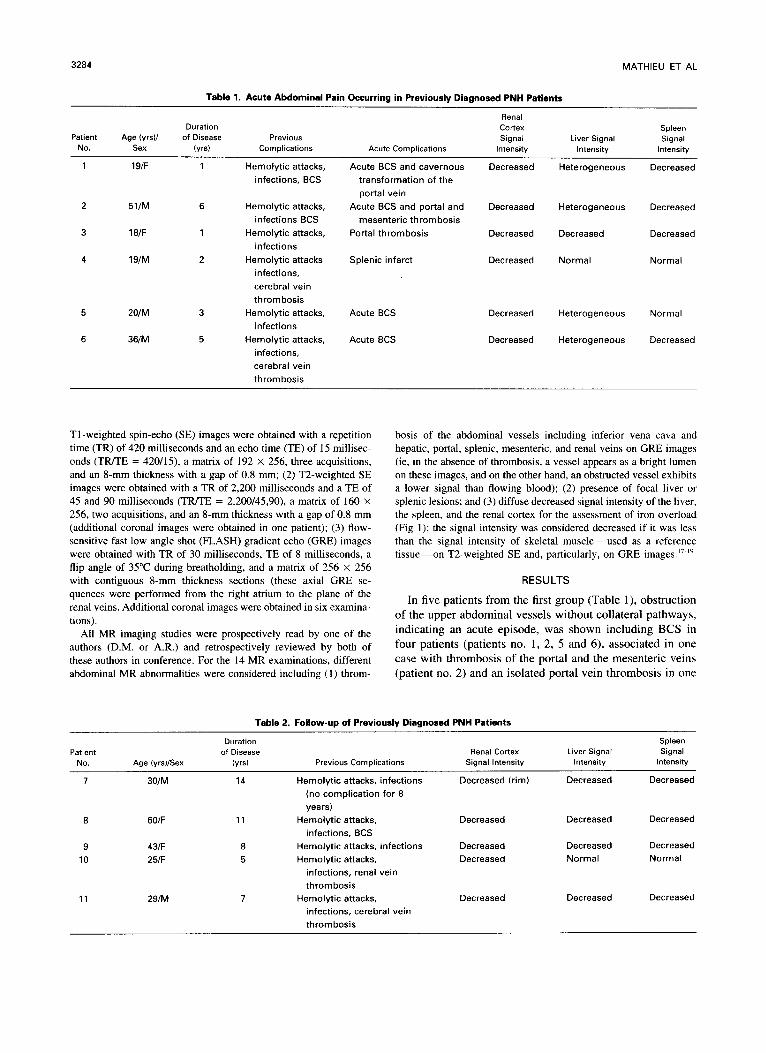
Table 1. Acute Abdominal Pain Occurring in Previously Diagnosed PNH Patients
Renal
Signal Patient Age (yrsl/ of Disease Duration Cortex Spleen
Liver Signal Signal Previous No. Sex (vrs) Acute Complications Intensity Intensity Intensity Complications
1 19/F 1 Hemolytic attacks, Acute BCS and cavernous Decreased Heterogeneous Decreased infections, BCS transformation of the
2 portal vein
51/M 6 Hemolytic attacks, Acute BCS and portal and Decreased Heterogeneous Decreased infections BCS
3 mesenteric thrombosis
18/F 1 Hemolytic attacks, Portal thrombosis Decreased Decreased Decreased infections
4 19/M 2 Hemolytic attacks Splenic infarct infections, cerebral vein thrombosis
5 20/M 3 Hemolytic attacks, Acute BCS infections
6 36/M 5 Hemolytic attacks, Acute BCS infections, cerebral vein thrombosis
Decreased Normal Normal
Decreased Heterogeneous Normal
Decreased Heterogeneous Decreased
TI-weighted spin-echo (SE) images were obtained with a repetition time (TR) of 420 milliseconds and an echo time (TE) of 15 millisec- onds (TRITE = 420/15), a matrix of 192 X 256, three acquisitions, and an 8-mm thickness with a gap of 0.8 mm; (2) T2-weighted SE images were obtained with a TR of 2,200 milliseconds and a TE of 45 and 90 milliseconds (TRITE = 2,200/45,90), a matrix of 160 X
256, two acquisitions, and an 8-mm thickness with a gap of 0.8 mm (additional coronal images were obtained in one patient); (3) flow- sensitive fast low angle shot (FLASH) gradient echo (GRE) images were obtained with TR of 30 milliseconds, TE of 8 milliseconds, a flip angle of 35°C during breatholding, and a matrix of 256 X 256 with contiguous 8-mm thickness sections (these axial GRE se- quences were performed from the right atrium to the plane of the renal veins. Additional coronal images were obtained in six examina- tions).
All MR imaging studies were prospectively read by one of the authors (D.M. or A.R.) and retrospectively reviewed by both of these authors in conference. For the 14 MR examinations, different abdominal MR abnormalities were considered including (1 ) throm-
bosis of the abdominal vessels including inferior vena cava and hepatic, portal, splenic, mesenteric, and renal veins on GRE images (ie, in the absence of thrombosis, a vessel appears as a bright lumen on these images, and on the other hand, an obstructed vessel exhibits a lower signal than flowing blood); (2) presence of focal liver or splenic lesions; and (3) diffuse decreased signal intensity of the liver, the spleen, and the renal cortex for the assessment of iron overload (Fig 1); the signal intensity was considered decreased if it was less than the signal intensity of skeletal muscle-used as a reference tissue-on T2-weighted SE and, particularly, on GRE images.”~”
RESULTS
In five patients from the first group (Table l), obstruction of the upper abdominal vessels without collateral pathways, indicating an acute episode, was shown including BCS in four patients (patients no. 1, 2, 5 and 6), associated in one case with thrombosis of the portal and the mesenteric veins (patient no. 2) and an isolated portal vein thrombosis in one
Table 2. Follow-up of Previously Diagnosed PNH Patients
Duration Spleen Patlent of Disease Renal Cortex Liver Signal Signal
No. Age (yrs)/Sex (yrs) Previous Complications Signal Intensity Intensity Intensity
7 30/M 14 Hemolytic attacks, infections Decreased (rim) Decreased Decreased (no complication for 8 years)
infections, BCS 8 60/F 11 Hemolytic attacks, Decreased Decreased Decreased
9 43/F 8 Hemolytic attacks, infections Decreased Decreased Decreased 10 25/F 5 Hemolytic attacks, Decreased Normal Normal
infections, renal vein thrombosis
11 29/M 7 Hemolytic attacks, Decreased Decreased Decreased infections, cerebral vein thrombosis

IMPACT OF MRI IN PNH
Fig 1. Normal and abnormal appearance of kidneys in PNH dis- ease. (A) Normal appearance of the kidneys on axial GRE image. The signal intensity of the renal cortex was equal to the signal intensity of the skeletal muscles. The patency of the different abdominal ves- sels is marked by a bright signal (patient no. 12). (B) Iron overload of the renal cortex on axial GRE image. Diffuse low signal intensity of the renal cortex. This signal intensity is less than the signal inten- sity of the skeletal muscles (patient no. 9). (C) Localized low signal intensity of the corticomedullary junction on axial GRE image in a patient with PNH disease (patient no. 7). Notice the low signal inten- sity of both liver and spleen corresponding to iron overload.
3285
patient (patient no. 3. Fig 2). In the remaining patient. with a painful splenomegaly. MR study disclosed a splenic in- farct. as a hypointense lesion surrounded by a hyperintense rim on TI-SE images. becoming hyperintense on T?-SE im- ages. without abdominal vein thrombosis (patient no. 4. Fig 3). Splenectomy was performed and the diagnosis of hemor- rhagic infarct was confirmed.
In the four patients with BCS. liver enlargement and hy- pertrophic caudate lobe were associated with a heteroge- neous signal and the presence of hypointense peripheral areas on SE and GRE images (Figs 4, S. and 6B). Venous abnormalities included coma-shaped intrahepatic collateral veins (two patients). irregular hepatic veins (one patient). nonvisualization of the hepatic veins (one patient). Thrombo- sis o f the portal and mesenteric veins was also present in one patient with mesenteric infarction leading to a rapid fatal outcome (patient no. 2). In the four patients with acute BCS. the signal intensity of the liver was heterogeneous. as de- scribed above. In another patient. both liver and spleen had a low signal intensity on T2-SE and GRE images (patient no. 3). In the remaining patient. no iron overload could be detected in either liver or spleen (patient no. 4). In all the patients of this group (Table 1 ). the renal cortex had a low signal intensity on both T2-SE and GRE images (Fig IB).
In the five patients of the second group (Table 2). no vascular abnormalities were observed. In four patients. no liver or splenic focal lesions were observed. In one patient who had been treated by androgens for 4 years. three hepatic lesions (diameter, 2 to 4 cm) were present and consistent with the diagnosis of hepatocellular adenomas. ie. hypoin- tense on TI-SE images and slightly hyperintense on T2- SE images. Right hepatectomy and pathologic examination confirmed the presence of hepatocellular adenomas (patient no. IO). In four patients. both liver and spleen had a low signal intensity on T2-SE and GRE images (patients no. 7. 8, 9. and I 1 ). In another patient. no iron overload could be detected in the liver and the spleen (patient no. I O ) .
The renal cortex was abnormal in all five patients of this second group, on both T2-SE and GRE images. marked by a diffuse low signal intensity in four patients and a localized low signal intensity as a rim at the corticomedullary junction in one patient. For this latter patient. the diagnosis of PNH was made 14 years ago, and no recurrent hemolytic attacks had occurred for 8 years (patient no. 7. Fig IC).
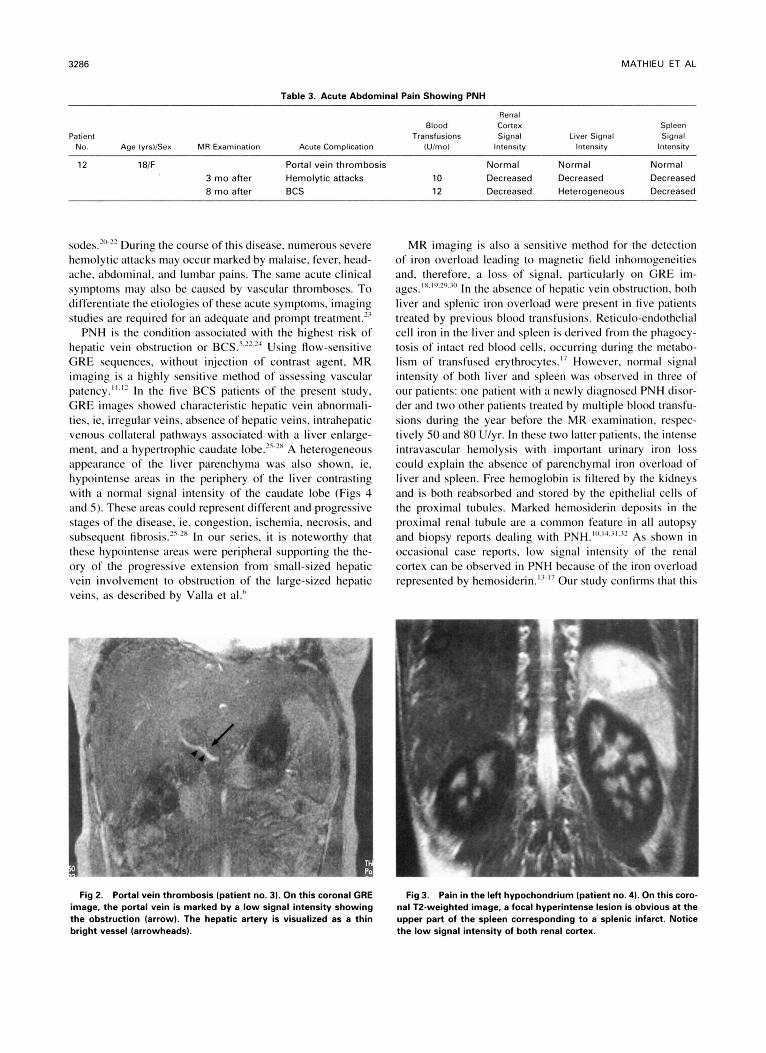
Finally, in patient no. 12, MR imaging showed an obstruc- tion of the main portal vein (Table 3). On this MR examina- tion. no parenchymal iron overload, particularly of the renal cortex. could be detected (Fig 6A). On the 3-month follow- up MR examination. decreased signal intensity of the renal cortex was obvious. associated with decreased signal intensity of both liver and spleen. This low signal intensity of the renal cortex was still present at the 8-month follow-up MR examination. which also showed a hepatic venous obstruction and a cavernous transformation of the portal vein (Fig 6B).
DISCUSSION
The PNH syndrome encompasses pancytopenia. chronic intravascular hemolysis. and recurrent thrombotic epi-
3286 MATHIEU ET AL
Table 3. Acute Abdominal Pain Showing PNH
Renal Blood Cortex Spleen
No. Age (yrs)/Sex MR Examination Transfusions Signal Liver Signal Signal
Acute Complication (Ulmo) Intensity Intensity Intensity Patient
12 18IF Portal vein thrombosis Normal Normal Normal 3 mo after Hemolytic attacks 10 Decreased Decreased Decreased 8 mo after BCS 12 Decreased Heterogeneous Decreased
sodes.?"'~~ During the course of this disease. numerous severe hemolytic attacks may occur marked by malaise, fever, head- ache, abdominal, and lumbar pains. The same acute clinical symptoms may also be caused by vascular thromboses. To differentiate the etiologies of these acute symptoms, imaging studies are required for an adequate and prompt treatment.'>
PNH is the condition associated with the highest risk of hepatic vein obstruction or BCS.""-?' Using flow-sensitive GRE sequences, without injection of contrast agent, MR imaging is a highly sensitive method of assessing vascular patency."." In the five BCS patients of the present study, GRE images showed characteristic hepatic vein abnormali- ties, ie, irregular veins, absence of hepatic veins, intrahepatic venous collateral pathways associated with a liver enlarge- ment, and a hypertrophic caudate A heterogeneous appearance of the liver parenchyma was also shown, ie, hypointense areas in the periphery of the liver contrasting with a normal signal intensity of the caudate lobe (Figs 4 and S). These areas could represent different and progressive stages of the disease, ie, congestion, ischemia, necrosis, and subsequent fibrosis.'"'x In our series, it is noteworthy that these hypointense areas were peripheral supporting the the- ory of the progressive extension from small-sized hepatic vein involvement to obstruction of the large-sized hepatic veins, as described by Valla et al."
MR imaging is also a sensitive method for the detection of iron overload leading to magnetic field inhomogeneities and, therefore. a loss of signal, particularly on GRE im-
liver and splenic iron overload were present in five patients treated by previous blood transfusions. Reticulo-endothelial cell iron in the liver and spleen is derived from the phagocy- tosis of intact red blood cells, occurring during the metabo- lism of transfused erythrocytes." However, normal signal intensity of both liver and spleen was observed in three of our patients: one patient with a newly diagnosed PNH disor- der and two other patients treated by multiple blood transfu- sions during the year before the MR examination, respec- tively SO and 80 U/yr. In these two latter patients, the intense intravascular hemolysis with important urinary iron loss could explain the absence of parenchymal iron overload of liver and spleen. Free hemoglobin is filtered by the kidneys and is both reabsorbed and stored by the epithelial cells of the proximal tubules. Marked hemosiderin deposits in the proximal renal tubule are a common feature in all autopsy and biopsy reports dealing with PNH.".'J~''.z2 As shown in occasional case reports, low signal intensity of the renal cortex can be observed in PNH because of the iron overload represented by hemosiderin.'"' Our study confirms that this
ages~lx,l",?",z" In the absence of hepatic vein obstruction, both
P 1
Fig 2. Portal vein thrombosis (patient no. 31. On this coronal GRE image, the portal vein is marked by a low signal intensity showing the obstruction (arrow). The hepatic artery is visualized as a thin bright vessel (arrowheads).
Fig 3. Pain in the left hypochondrium (patient no. 4). On this coro- nal T2-weighted image, a focal hyperintense lesion is obvious at the upper part of the spleen corresponding to a splenic infarct. Notice the low signal intensity of both renal cortex.

IMPACT OF MRI IN PNH 3287
I ' .
Fig 4. Budd-Chiari syndrome. Hypointense peripheral areas (*l in comparison to the normal signal intensity of the hypertrophic cau- date lobe. Presence of multiple intrahepatic and periperal collateral veins with a patent WC. Notice the diffuse low signal of the renal cortex of the left kidney on this axial GRE image.
tinding is always present when previous hemolytic attacks have occurred during the course of PNH. This low signal intensity was diffuse within the cortex in IO patients with previous hemolytic attacks (Fig IB). In one patient of our series, this low signal intensity was localized at the corti- comedullary junction (Fig IC). It is tempting to speculate that this peculiar feature was a residual hemosiderin deposi- tion in a patient who did not experienced hemolytic attacks for many years. Finally, in one patient, MR appearance of the kidneys was normal (Fig IA). This patient had no previous hemolytic attacks before the MR examination. The course of this patient was rapidly marked by multiple acute episodes of hemolysis, and then a decreased signal intensity of the renal cortex appeared on follow-up MR examinations (Fig
Fig 5. Budd-Chiari syndrome. On this coronal GRE image, hypoin- tense peripheral areas ( W ) are present within an enlarged liver. The portal vein and the mesenteric vein are patent.
l . I
3
Fig 6. Patient with acute portal thrombosis showing a PNH dis- ease (patient no. 12). (AI On this initial MR examination, the signal intensity of both kidneys appears normal in comparison with the signal intensity of the skeletal muscles on this coronal GRE image. (B) 8-month follow-up MR examination. On an identical coronal GRE image, the signal intensity of renal cortex is now low. Notice the presence of hypointense areas of the inferior part of the right hepatic lobe corresponding t o hepatic venous obstruction.
6, A and B). However, low signal intensity of the renal cortex is not pathognomonic of PNH because this appearance has otherwise been shown in the kidneys of patients with long-standing sickle cell anemia. treated by multiple blood transfusions, with hemosiderin deposition in glomerular epi- thelium.3'." This MR tinding may also be obtained in any patient with chronic hemoglobinuria.
ACKNOWLEDGMENT
We thank Dr Anne Lavaud for her referrals and Dr Fr6d6ric GalnctCros for his help with the discussion.

3288 MATHIEU ET AL
REFERENCES 1. Takeda J, Miyata T, Kawagoe K, Iida Y, Endo Y, Fujita T,
Takahashi M, Kitani T, Kinoshita T: Deficiency of the GP1 anchor caused by a somatic mutation of the PIG-A gene in paroxysmal nocturnal hemoglobinuria. Cell 73:703, 1993
2. Miyata T, Takeda J, Iida Y, Yamada N, Inoue N. Takahashi M, Maeda K, Kitani T, Kinoshita T The cloning of PIG-A, a compo- nent in the early step of GPI-anchor biosynthesis. Science 259: I3 18, 1993
3. Bessler M, Mason PJ, Hillmen P, Myata T, Yamada N, Takeda J, Luzzatto L, Kinoshita T: Paroxysmal nocturnal haemoglobinuria (PNH) is caused by somatic mutations in the PIG-A gene. EMBO J 13:110, 1994
4. Dixon R H , Rosse WF: Mechanism of complement-mediated activation of human platelets in vitro. Comparison of normal and PNH platelets. J Clin Invest 59:360, 1977
5 . Leibovitz AI, Hartmann RC: The Budd-Chiari syndrome and paroxysmal nocturnal haemoglobinuria. Br J Haematol 48:1, 1981
6. Valla D, Dhumeaux D, Babany G, Hillon P, Rueff B, Rochant H, Benhamou J P Hepatic vein thrombosis in paroxysmal nocturnal hemoglobinria: A spectrum from asymptomatic occlusion of hepatic venules to fatal Budd-Chian syndrome. Gastroenterology 93569, 1987
7. Staab EV, Hartmann RC, Parrot JA: Liver imaging in the diagnosis of hepatic venous thrombosis in paroxysmal nocturnal hemoglobinuria. Radiology 117:341, 1975
8. Birgen HS, Hancke S, Rosenklint A, Hansen NE: Ultrasonic demonstration of clinical and subclinical hepatic venous thrombosis in PNH. Br J Haematol 64:737, 1986
9. Kolb WP, Long JH, Lasser EC: Nonimmunologic complement activation in normal human serum induced by radiographic contrast media. J Immunol 121:1232, 1978
10. Clark DA, Butler SA, Braren V, Hartmann RC, Jenkins DE: The kidneys in paroxysmal nocturnal hemoglobinuria. Blood 57:83, 1981
11. Anglade MC, Derhy S, Delvalle A, Cauquil P, Roche A, Mathieu D: Abdominal venous thrombosis: Application of gradient echo magnetic resonance imaging. Diagn Interv Radiol l:6l, 1989
12. Anivi L, Menu Y, Dessarts I, Dubray B, Vullierme M-P, Vilgrain V, Najmark D, Nahum H: Diagnosis of abdominal venous thrombosis by means of spin-echo and gradient echo MR imaging: Analysis with receiver operating characteristic curves. Radiology 181:661, 1991
13. Lupetin AR: Magnetic resonance appearance of the kidneys in paroxysmal nocturnal hemoglobinuria. Urol Radiol 8:101, 1986
14. Munopulos GP, Turner DA, Schwartz MM, Murakami ME, Clark JW: MRI of the kidneys in paroxysmal nocturnal hemoglobin- uria. AJR 14651, 1986
15. Kim SH, Han MC, Lee JS, Kim S: Paroxysmal nocturnal hemoglobinuria. Case report of MR imaging and CT findings. Acta Radiol 32:315, 1991
16. Tanaka YO, Anno I, Itai Y, Abe T: Paroxysmal nocturnal
hemoglobinuria: MR findings. J Comput Assist Tomogr 17:749, 1993
17. Siegelman ES, Mitchell DG, Rubin R, Hann H-WL, Kaplan KR, Steiner RM, Rao VM, Schuster SJ, Burk DL, Rifkin MD: Parenchymal versus reticuloendothelial iron overload in the liver: Distinction with MR imaging. Radiology 179:361, 1991
18. Chezmar JL, Nelson RC, Mako JA, Bernardino ME: Hepatic iron overload: Diagnosis and quantification by noninvasive imaging. Gastrointest Radiol 15:27, 1990
19. Stark DD, Moseley ME, Bacon BR, Moss AA, Goldberg HI, Bass NM, James TL: Magnetic resonance imaging and spectroscopy of hepaatic iron overload. Radiology 154:137, 1985
20. Rosse W: Paroxysmal nocturnal haemoglobinuria in aplastic anemia. Clin Haematol 7541, 1978
21. Rotoli B, Luzzatto L: Paroxysmal nocturnal hemoglobinuria. Semin Hematol 26:201, 1989
22. De Gramont A, Debray J: Himoglobinurie paroxystique noc- turne: synthkse et riflexions h partir d’une sCrie francophone de 15 I patients. Rev Med Interne 6:477, 1985
23. Rosse WF: Treatment of paroxysmal nocturnal hemoglobin- uria. Blood 60:20, 1982
24. Peytremann R, Rhodes RS, Hartmann RC: Thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) with particular refer- ence to progressive, diffuse hepatic venous thrombosis. Ser Haema- to1 S : 1 15, 1972
25. Mathieu D, Kracht M, Zafrani ES, Dhumeaux D, Vasile N: Budd-Chiari syndrome, in Ferrucci JT, Mathieu DG (eds): Advances in Hepatobiliary Radiology. St Louis, MO, Mosby, 1990
26. Stark DD, Hahn PF, Trey C, Clouse ME, Ferrucci JT: MRI of the Budd-Chiari syndrome. AJR 146: 1 141, 1986
27. Friedman AC, Ramchandani P, Black M, Caroline DF, Ra- decki PD, Heeger P Magnetic resonance imaging diagnosis of Budd- Chiari syndrome. Gastroenterology 9 1 : 1289, 1986
28. Miller WJ, Federle MP, Straub WH, Davis PL: Budd-Chiari syndrome: Imaging with pathologic correlation. Abdom lmaging 18:329, 1993
29. Stark DD, Moseley ME, Bacon BR, Moss AA, Goldberg HI, Bass NM, James TL: Magnetic resonance imaging and spectroscopy of hepatic iron overload. Radiology 154: 137, 1985
30. Gomori JM, Horev G, Tamary H, Zandback J, Kornreich L, Zaizov R, Freud E, Krief 0, Ben-Meir J, Rotem H, Kuspet M, Rosen P, Rachmilewitz EA, Loewenthal E, Gorodetsky R: Hepatic iron overload: Quantitative MR imaging. Radiology 179:367, 1991
31. Rubin H: Paroxysmal nocturnal hemoglobinuria with renal failure. JAMA 215:433, 1971
32. Heitzman EJ, Campbell JS, Stefanini M: Paroxysmal noctur- nal hemoglobinuria with hemosiderin nephrosis. Am J Clin Pathol 273:975, 1953
33. Lande IM, Glazer GM, Samaik S, Aisen A, Rucknagel D, Martel W: Sickle-cell nephropathy: MR imaging. Radiology 158:379, 1986
34. Bernstein J, Whitten CF: A histologic appraisal of the kidney in sickle cell anemia. Arch Pathol 70:407, 1960