Embed Size (px)
Citation preview
April 1 9 9 5 SSAT A 1 2 4 9
• INTERMEDIATE FOLLOW UP OF LAPAROSCOPIC ANTIREFLUX SURGERY. TL Trus. S Mauren. WS Laycock, JG Hunter. JP Wadng, G BRANUM~ EMERY UNIVERSITY, ATLANTA GEORGIA Open antiraflux surgery is an established long term treatment for
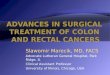
chronic gastroesophageal reflux disease (GERD).Short term results of [aparoseopic antireflux surgery are excellent, however long term follow up data is not yet available. We report our intermediate results of ambulatory esophageal pH monitoring following laparoscopic antiraflux surgery. 59 patients have had 24 hour pH monitoring 6 weeks after operation and 51 of these patients (87%) had normal pH studies. 23 patients (15 male, 8 female) have had pre- and postoperative ambulatory pH monitoring at least I year following laparoscopic antireflux surgery. 17 patients had a Nissen fundoplication and 6 had partial fundoplication. The duration of follow up ranged from 12 to 33 months (median,18). 22 patients (96%) demonstrated a significant reduction of the total time of pH < 4.0 which correlated with improvements in symptom scores. Only one patient developed recurrent symptoms of reflux after a normal 6 week follow up pH study. Subsequently, she developed abnormal pH results and was found to have trans-diaphragmatic migration of the fundoplication on barium swallow. There was no difference between partial and total fundoplication.
40- m \ 24 hour ambulatory pH results in ~ \ laparoscepic fundoplication patients
30- ~ 1 to 3 years postoperatively
20- Total T i m e . ~ ~ . . 2 3 pH < 4.0
I0- ~ ~ ~ abnormal
0 ~re- 6 18 op wks mos
Conclu$iQn: Long term efficacy of laparoscopie fundoplication remains to be seen, but intermediate results suggest that long term efficacy will be equivalent to open fundoplication.
IMPACT OF SOCIOECONOMIC STATUS ON SURVIVAL IN AFRICAN-AMERICANS WITH COLON AND RECTAL CANCER. *W.B. Tuckson, F. Dawkins, M. Johnson, D. Sm_oo_.QL and V. Lee Departments of Surgery, *University of Louisville, Louisville, KY and Howard University, Washington, D.C.
In the United States, between 1981 and 1987, the 5-year relative survival rate for African-Americans with colon and rectal cancer was 47%, while for whites it was 57%. The poorer survival rate in African-Americans may reflect socioeconomic status. This study evaluated the influence of race and socioeconomic status (SES) on stage and survival in an African-American population with colon and rectal cancer. The stage, SES, and 5-year relative survival rate of 233 consecutive African-Americans diagnosed with colon and rectal cancer between 1986 and 1992 were reviewed. SES was determined by the type of insurance: lower SES=self pay and Medicaid, higher SES=conunercial insurance, BC/BS, or HMO. Medicare patients were classified separately. Five-year relative survival rates were determined by the actuarial method. The results were compared with SEER data. Twenty percent of the patients were Dukes' stage A, 29% B, 25% C, and 26% D. There was no significant difference in the stage at presentation by SES. The overall 5-year relative survival rate was 46%, but for Dukes' A it was 86%, B 57%, C 40%, and D 11%. The 5-year relative survival rate in the lower SES group was 34%, 57% in the higher SES group, and 43% in the Medicare group. Five year survivals for stages A, B, and C disease were better in the higher SES group than in either the lower SES group or Medicare group. Our overall 5-year survival rate was lower than that reported for whites. Though SES was not a factor in the stage at presentation, higher SES was associated w.ith bet~r survival. The poorer survival of African-Americans with colon and rectal cancer compared to whites, reflects in part, factors related to socioeconomic status.
O ENDOSCOPIC MANAGEMENT OF BENIGN AND MALIGNANT BILIARY STRICTURES. G_. C. Vitale e M. Geor@e e K. McIntyre, G. Larson and T. J. Wieman. Department of Surgery, University of Louisville, Louisville, KY.
It is now possible to endoecopically dilate and stent most common bile duct strictures. The issue remains whether this is an acceptable alternative to an operative approach given the fact that repeat dilatations and stent changes are needed. With this in mind, we have reviewed the experience in our surgical endoscopy unit with endoscopic treatment of biliary strictures. Over a two year period, we have treated 43 patients with benign stricture and 61 patients with a malignant stricture. Many of these patients had extensive tumor burden or high lying porta-hepatis strictures and were not approachable surgically for biliary enteric bypass. Sphincterotomy and dilatation and/or stenting with polyethylene (PE) or metallic, self-expanding stents were performed. In benign cases, stants are left out after one year. In malignant cases, they remain for life. Results were as follows:
Sphine. + Stricture n Dilatation Benign 43 9 Malignant 61 0
PE Metal Radiol. Surgical Stent Stent Stent Draina@e 30 0 4 0 35 12 8 6
Complications included hemorrhage (2) and pancreatitis (8). There were no ERCP related deaths; one patient died with bleeding from transhepatic stenting. Six patients with malignant stricture underwent biliary enteric bypass after failed ERCP and/or tranehepatie approach, and four patients underwent gastrojejunostomy. Eleven patients, all with malignant strictures, required early stent change : for cholangitis. In benign cases, no patients have required reoperation or re-stenting for recurrent stricture with mean follow up of two years. In summary, endoscopic stenting is possible with minimal morbidity and mortality and should be considered an acceptable option to surgical management in both benign and malignant cases.
O POSITRON EMISSION TOMOGRAPHY (PET) TO STAGE COLORECTAL CARCINOMA METASTATIC TO THE LIVER. J.V .... Vitola, D. Delbeke, M.P° Sandier, M. CamDhello T.A. Powers. J.K. Wrlqht, W.C. Chapman, C.W. Pinson. Vanderbilt University School of Medicine, Nashville, TN.
PET is an imaging technique based on metabolic function that may be complimentary to anatomical- ly based techniques. In this study we examine the results of F-18-fluorodeoxyglucose (FDG)-PET in staging recurrent colorectal carcinoma metastasis in the liver and compare it to CT and CT portogram. Methodsz Twenty consecutive patients previously treated surgically for colorectal Ca were suspected of recurrence based on CEA level or CT. All patients underwent an entire body PET scan looking for intra- and extrahepatic malignant lesions and had a CT scan, a CT portogram or both. Results were compared with operative findings including intraoperative ultrasound and histopathology. Results: Of 48 suspicious lesions, 35 were malignant including 3 extrahepatic foci. Results are expressed as number of lesions true positive (T+), false negative (F-), true negative (T-), false positive (F+), sensitivity (SEN) and specificity (SPE).
T+ F- T- F+ SEN SPE CT SCAN (n=14) 17 4 4 4 81% 50% CT PORTOGRAM (n=15) 29 1 i 7 97% 13% PET SCAN (n=20) 31 4 12 1 89% 92% The findings of PET scan altered su: . plans in 6 of 20 (30%) patients. Conclusions: (i) PET and CT portogram had the highest sensitivity to diagnose hepatic metastasis. (ii) The improved sensitivity of CT portogram in comparison to CT scan markedly sacrifices specificity. (iii) PET scan had the highest specificity of all tests for intra and extrahepatic recurrences. (iiii) PET, due to its high specificity, is a complementary diagnostic modality and alters surgical treatment in many patients.








![Retrospective Study Critical appraisal of laparoscopic vs ... · with colon and rectal cancer[1214]. This is suboptimal as the prognosis and recurrence pattern of colon and rectal](https://img.pdfslide.net/doc/110x75/5edc7da5ad6a402d66672bbb/retrospective-study-critical-appraisal-of-laparoscopic-vs-with-colon-and-rectal.jpg)














![Chassin's Operative Strategy in Colon and Rectal Surgery,(2006) [UnitedVRG]](https://img.pdfslide.net/doc/110x75/56d6c06f1a28ab30169a63d7/chassins-operative-strategy-in-colon-and-rectal-surgery2006-unitedvrg.jpg)