Embed Size (px)
Citation preview

Pergamon
S0277-9536(96)0007-79
Soc. Sci. Med. Vol. 43, No. 12, pp. 1785-1794, 1996 Copyright © 1996 Elsevier Science Ltd
Printed in Great Britain. All fights reserved 0277-9536/96 $15,00 + 0.00
IMPACT OF WITNESSING DEATH ON HOSPICE PATIENTS
SHEILA PAYNE, ~ RICHARD HILLIER, 2 ALISON LANGLEY-EVANS ~ and TONY ROBERTS'
'Department of Psychology, University of Southampton, Murray Building, Salisbury Road, Southampton SO17 IBJ, U.K., zCountess Mountbatten House, Moorgreen Hospital, Botley Road, West End, Southampton
SO30 3JB, U.K.
Abstract--In the three decades since the concept of "awareness" was introduced to describe the nature of communication between dying people and their caters, there has been a radical change in hospital policies and medical practice. It is now common for the majority of cancer patients to be given full information about their disease and prognosis. Hospices provide a model of care in which death and dying are dealt with in an open manner. While this approach has been welcomed by the majority of people, a minority might still prefer a more limited awareness. An inevitable part of hospice care is the exposure to, and awareness of, people who are dying. There is little empirical data that considers the impact of death on fellow patients. This pilot investigation compared psychological morbidity, perceptions of comfort and/or distress, and descriptions of a "good death" in hospice cancer patients who reported witnessing a fellow patient's death (n = 34) with patients who did not have this experience (n = 33). Patients were assessed using the Hospital Anxiety and Depression scale, an Events Checklist and a semi-structnred interview. The results indicate that patients witnessing a death were significantly less depressed than those who did not. Awareness of dying was found to be both comforting and distressing, although overall patients reported more comforting than distres- sing events. A "good death" was defined by patients in terms of symptom conla'ol, including dying in their sleep, being pain free, quietness and dignity. Narratives were used to describe the meaning of a "good death". Quantitative and qualitative analyses have been undertaken to provide a complex interpretation of these issues. Copyright © 1996 Elsevier Science Ltd
Key words--palliative care, terminal care, communication, fellow patients, hospices
INTRODUCTION
The majority of people in Britain die in institutions, usually in hospitals. It is estimated that 54% of deaths occur in hospitals, 13% in nursing or residential homes and only 4% in hospices [1]. In 1993, approximately 28,000 deaths occurred in hospices, predominantly from cancer, and almost 100,000 patients received home care by palliative care nurses [2]. In January 1994, there were 203 in-patient palliative care units in Britain and Ireland.
There have been considerable developments in specialist palliative care services for the terminally ill, although there remain some concerns about unmet needs [3]. Previous research conducted in general hos- pitals indicates that dying patients were often both physically isolated by being cared for in side rooms and had only limited communication about their con- dition [4].
A number of studies have investigated death and dying as a social event in hospital [5], [6]. Sudnow suggested that dying is routinized and thereby becomes part of the day-to-day functioning of the hospital as an organization. Glaser and Strauss [5] described a range of awareness contexts in which patients, staff, families and friends may engage, in relation to the discussion of the terminal nature of the patient's condition. They proposed three major categories of awareness: " o p e n " - - i n which all participants acknowledged the
5514 43I I~'-I:
dying person's status; " m i x e d " - - i n which some mem- bers of the dying person's social network knew of the prognosis but others (which may include the patient) do not; and "c losed" - - in which an attempt was made, either by the medical staff or the patient's family, to keep the prognosis unknown. Thus the staff, families and patients may collude to avoid talking about dying, ostensibly to protect others. It has been argued that "closed" and "mixed" awareness con- texts are psychologically damaging to patients and their families [7] by preventing normal psychological processes associated with loss, such as anticipatory grief, from occurring.
However, these studies were conducted over 30 years ago and may not represent the experiences of dying people today. The hospice movement has devel- oped rapidly in the last two decades [8]. It seeks to provide an alternative model of care in which death and dying are dealt with in an open manner. This has occurred concurrently with wider changes in society that have removed some of the taboo surrounding death and produced a greater willingness by doctors to talk honestly with patients [9]. While this approach has been welcomed by the majority of people, a min- ority may still prefer a more limited awareness.
The concept of open "awareness" is central to hos- pice philosophy, but it remains problematic. Early hos- pice workers advocated that dying should be
1785
1786 Sheila Payne et al.
conducted "openly", in that dying patients should be cared for collectively in separate institutions or desig- nated areas [10]. Awareness contexts are not synon- ymous with cancer-related deaths but are associated with anticipated terminal disease trajectories. It has been proposed by Coleman [ 11 ] that ageing alone does not influence an individual's sense of self-integrity and attitudes to death, although he argues that physical and psychological frailty does.
An inevitable part of hospice care is the exposure to, and awareness of, people who are dying. Most research tends to be from the perspective of relatives or those caring for the dying rather than from patients and their perceptions [9]. Research on doctors and nurses indicates that interacting with and caring for dying patients is often perceived as a very stressful part of their role [12]. Likewise, relatives of the dying are often critical of their hospital experiences [13]. However, there is little empirical research that con- siders the impact of death on fellow patients. It is possible to speculate that such experiences may be dis- tressing, as they might remind the observing patients of their own imminent death. Alternatively, patients may be comforted by observing the care and attention afforded to the dying person. Such assumptions have been explored by Honeybun et al. [14] in a very small study of 20 hospice patients. They reported that the 11 patients who had witnessed a death were less de- pressed and more reassured by the experience than the nine patients who had not witnessed a death. However, an important aspect not considered was the nature of the observed death. In addition, patients develop re- lationships of varying intensity with their fellow patients, and this may be expected to influence the per- ception of these deaths. It is clear that patients have prior expectations of the dying process and the nature of a "good" death [15]. Moreover, Hunt's work indi- cates that nurses are instrumental in conveying their views about what constitutes a "good" death and what are appropriate "dying" behaviours.
With improvements in palliative medicine and nur- sing care it is possible that the dying phase of diseases such as cancer may be prolonged. Thus, health ser- vices should be mindful that in prolonging physical survival nothing is done to increase psychological dis- tress. Individuals should be given some freedom to shape the dying roles that they wish for, based on their social, spiritual and cultural expectations [16]. It is im- portant that we know to what extent health care pro- fessionals are aware of these individual differences. A recent British report [17] emphasized the need for good models of cultural and ethnically sensitive prac- tice in the care of the dying to be developed and com- municated to health professionals working with dying patients in the community and general hospitals. Thus, the purpose of this study was twofold:
• to assess the impact of death on fellow patients in terms of levels of anxiety and depression and perceived distress and/or reassurance; and
• to elicit patients' awareness of their own impending death.
METHOD
The research context
The research was conducted in a 25-bedded palliative care unit located in the South of England. This hospice provides in-patient care for cancer patients who are usually accommodated in four-bedded bays. Statistics for the last 14 years indicate a large increase in the referrals to the hospice from 616 in 1981, to 1261 in 1994. While the death rate shows annual fluctuations, overall it remains fairly constant with a mean of 315 in-patient deaths (ranging from 287 in 1991 to 365 in 1987). It appears that the major increase in workload can be accounted for in the rise in discharges. This probably results from improvements in symptom control and better community care facilities. It also means that potentially more patients may witness the death of fellow patients whilst they are in- patients.
Patient recruitment
One hundred patients were invited to take part in the study. Between 16 May and 22 September 1994 there were 237 in-patient admissions. Eighty of the patients were deemed "fit" to participate. The exclu- sion criteria were:
• the mentally confused; • those unable to express themselves; and • those too unwell to complete data collection.
Patients admitted on more than one occasion were only invited to participate on the first occasion. Thus, during these four months only 35% of all patients admitted were deemed able to participate. These patients were approached by the research as- sistant six to seven days after their admission to the hospice. A delay in recruitment was desirable to both stabilize their medical condition and increase the likelihood that they would have witnessed a death.
Patients were informed (verbally and in writing) of their rights to refuse participation, which it was explained would be without detriment to their medi- cal and nursing care. They were usually given 24 hours or longer to make their decision. During October 1994, a further 20 patients were invited to participate by the same research assistant, using the same criteria.
Sixty-nine of the 100 patients approached agreed to take part in the study. This represents a refusal rate of 31%. Although this is a higher rate than we would have wished, we consider that it can be accounted for by the advanced state of their disease. Moreover, we were careful not to place the patients under any press- ure to participate. We noted a trend for refusal rates to increase during times of higher mortality. A further
Impact of witnessing death on hospice patients 1787
two patients became unwell during data collection, and their responses were excluded from the subsequent analyses. The results are based on the 67 patients who completed the three elements of the data collection phase.
Careful records of the timing and location of all deaths were kept, This information allowed verification between patients' reports of perceived and actual wit- nessing of deaths. Three patients had not actually wit- nessed a death in their bay but were aware of those deaths occurring nearby, and two patients chose to be "unaware" of the deaths that occurred in the next bed. Patients were allocated into two groups depending upon whether they reported witnessing or not witnes- sing the death of a fellow patient: 34 witnessed a death and 33 did not.
Ethical issues
Research conducted with dying patients must be mindful of the ethical issues [18]. It has been argued that any research conducted with dying patients is morally unjustifiable [19], although such an extreme stance has been vigorously attacked on the grounds that it is "paternalistic, devaluing and disrespectful" not to provide an opportunity for patients to share their experiences if they wished to [20]. In our study, we were concerned not to increase the burden or distress of patients. In addition to obtaining Hospital Ethical Committee permission, the study design and conduct were carefully monitored with ethical issues in mind. We recruited a research assistant who was both a qua- lified nurse and a psychology graduate (A. L.-E.), and she had recent clinical experience in interacting with elderly patients. She spent a week becoming familiar with the routine organization of the hospice. Once the data collection started, she introduced herself to all patients fairly soon after their admission so that they were aware of who she was and that a research study was being conducted in the hospice. The relatively high refusal rate indicates that patients were not press- ured to take part. Finally, we believe that most of those patients who chose to participate gained from the experience. Patients appeared pleased to have someone to share their perspective with. None asked to termi- nate the interview. While the expression of sadness or distress was not uncommon during the interview, none were left distressed at the end, and many shared feel- ings of happiness or humour as well. Thus, we con- clude that while it is generally ethically defensible to conduct research with dying patients, as it is important to gain an understanding of their needs and views, there remain specific circumstances where it is not ethically defensible, for example, during episodes of acute physical illness or emotional distress.
distress and/or reassurance were assessed by the fol- lowing measures.
First, the Hospital Anxiety and Depression scale (HAD) was used [21]. This scale is a 14-item ques- tionnaire divided into two subscales for anxiety and depression. Patients rate each item on a 4-point descriptive scale. Standard cut-off criteria were used: scores of 0-7 were taken to be indicative of no pathology, 8-10 a borderline case, and 11-21 a probable case. The HAD scale is acceptable to patients, and by excluding somatic items it mini- mizes the likelihood of confounding disease-related symptoms and psychological aspects. This measure has been widely used with cancer patients and has proved to be valid and reliable [22], [23], although Silverstone [24] has found that the scale has poor predictive ability in the diagnosis of major de- pressive disorders in general medical and psychiatric patients. It has been suggested that the HAD scale is only used as a clinical indicator of depressive dis- order rather than as a diagnostic tool [24]. The HAD scale has been successfully used with dying patients [25], although there are concerns that social withdrawal and anhedonia might be representative of normal processes of dying rather than features of the "pathological" condition of depression. We were aware that one item in the depression subscale--"I feel as if I am slowed down"mwas potentially con- founded by physical status in advanced disease.
Next, an Events Checklist was adapted with the authors' permission from that used with hospice patients by Honeybun et al. [14]. It described 11 po- tentially distressing and nine potentially comforting events, which patients rated on a 5-point scale, ranging from 0 = not at all comforting/distressing to 4=extremely comforting/distressing. The order of presentation was randomized to reduce response bias.
Third, a short interview based on that previously used by Honeybun et al. [14] was developed. It con- rained two open questions about distressing and com- forting events that had occurred since admission. Patients were also asked an open-ended question to eli- cit their perceptions of a "good" death.
Finally, socio-demographic and clinical data were obtained from medical records.
The procedure for collecting data were as follows: the study was explained, informed consent was obtained, the interview was started, the HAD scale was administered either verbally or in writing and was completed by the patients themselves, the interview continued, the Checklists were given, the interview was concluded and the patient thanked. Responses during the interviews were audio tape recorded with the patients' permission. All interviews were tran- scribed.
Method of patient assessment
All patients were interviewed once by the same research assistant who came to their bedside or other private area. Psychological morbidity and perceived
RESULTS
Both quantitative and qualitative data analyses were undertaken. The former are presented first.
1788 Sheila Payne er al.
Patient characteristics
The patient sample consisted of 34 males and 33 females, with significantly more men (26) than women (8) reporting witnessing a death (~2=9.60, df= 1, P<0.001).
The mean age of the total sample was 66.5 years (SD= 12.8, range 18-84 years). Men were signifi- cantly older (mean age = 70.48 years, SD = 7.99) than women (mean age ffi 63.55 years, SD = 15.02) (unpaired t = 2.25, df= 65, P<0.02). The mean age of the "witnessed death" group was 68.2 years (SD= 11.7, range 18-84) and the "not witnessed death" group 64.7 years (SD= 13.9, range 30-84), which was not significantly different (t -- 1.10, df= 65, P=0.27) . Thirty-three patients were married, 21 widowed, eight divorced and five single. The majority (43) were admitted from home to the hospice. They had a range of common cancers, including lung (11), breast (11), prostate (9), colo-rectal (7), upper gastro- intestinal (7) and others (22). Comparison of diagnoses between the groups revealed no marked differences, other than in prostate cancer where all except one patient was in the "witnessed" group. Overall, length of illness was very variable, although the largest num- ber of patients had been ill for less than one year.
Of the 31 patients who refused to partici~ate, there were 15 males and 16 females whose mean age was a little older, 69.41 years (range 36-92 years), than those who took part, but this was not statistically different ( t= 1.07, d f=95, P=0.28) . The majority were married (16), with 10 widowed, four divorced and one single person. The majority had been admitted from home (20), and they had a similar pattern of diagnoses. There appeared to be no major differences in socio-demographic variables in those patients who agreed to participate and those who did not.
Psychological morbidity
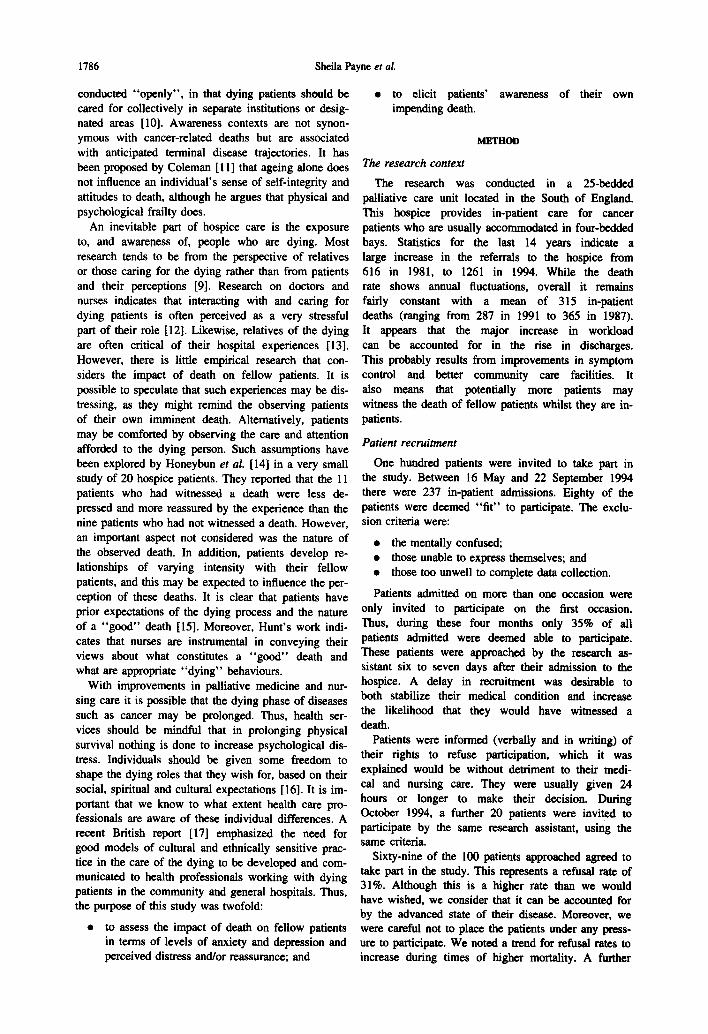
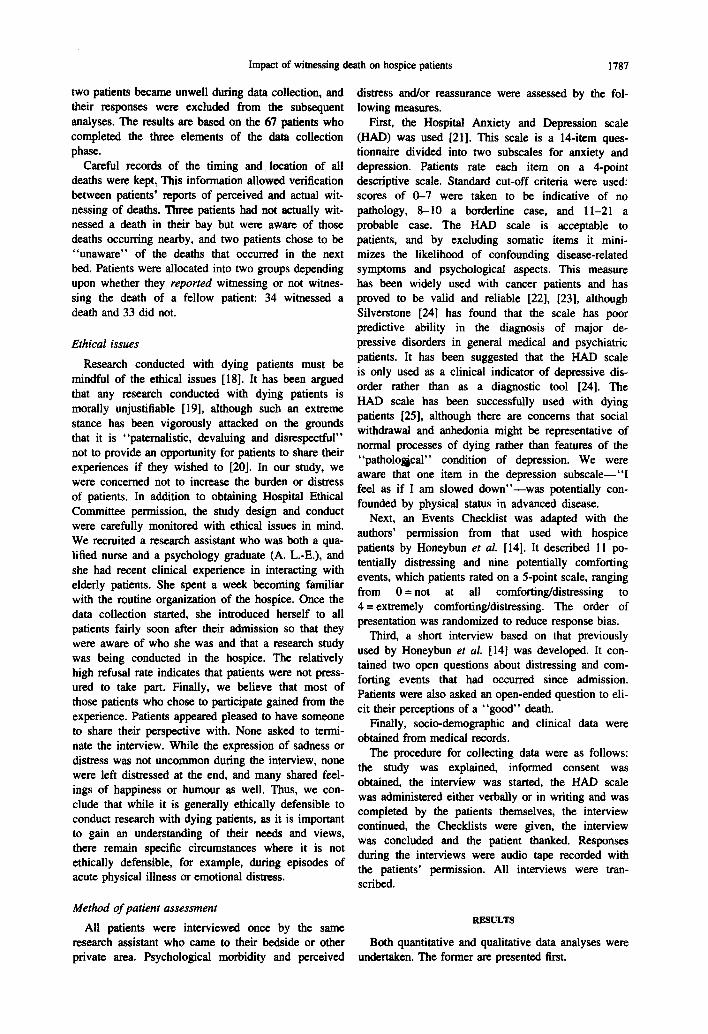
We hypothesized from the findings of Honeybun et al. [14] that patients who had witnessed a death would be less depressed than those who had not witnessed a death. This was supported by the data which indicated that the mean depression score for the witness group (n = 34) was 6.70 (SD = 3.9), and for the non-witness group (n = 33) the mean depression score was 9.36 (SD = 4.12). This was a statistically significant differ- ence (unpaired t = - 2 . 6 8 , df=65, P<0.01) . No pre- diction about the relationship of anxiety to awareness of death in others was made. There was no significant difference in mean levels of anxiety between the groups; the witness group mean was 5.35 (SD = 4.0) and the non-witness group mean was 6.27 (SD = 4.47) (unpaired t = - 0.88, df= 65, P = 0.37).
Overall mean levels of psychological morbidity were in the normal range (0-7), except for the non- witness group mean depression score, which was in the "borderline" category (8-10). However, it is im- portant to recognize that certain individuals were scor-
25
20
15
10
5
0 Witness Non-Witness
Fig. 1. Depression scores from the HAD scale.
ing in the probable psychiatric "case" range (11-21) in both groups as shown in Fig. 1 and Fig. 2.
A series of further analyses was undertaken to deter- mine whether anxiety and depression were associated with other variables. There were no gender differences in mean scores of depression ( t = - 0 . 3 1 , df=65, P = 0.75) or of anxiety (t = 0.32, df= 65, P = 0.74). Neither depression ( r=0.03) nor anxiety ( r = - 0 . 1 9 ) were correlated to any extent with age. In fact, anxiety scores showed a very slight negative correlation with increasing age. Likewise, duration of illness since pri- mary diagnosis was not correlated with any of the vari- ables measured.
Comforting and distressing events checklists
All patients were presented with the Events Checklists. It was possible that the order in which patients were presented with lists of comforting or dis- tressing events might bias their subsequent responses. However, since no order effects were found during preliminary analyses, the reported analyses are based on the total sample divided into groups on their reports of witnessing a death or not.
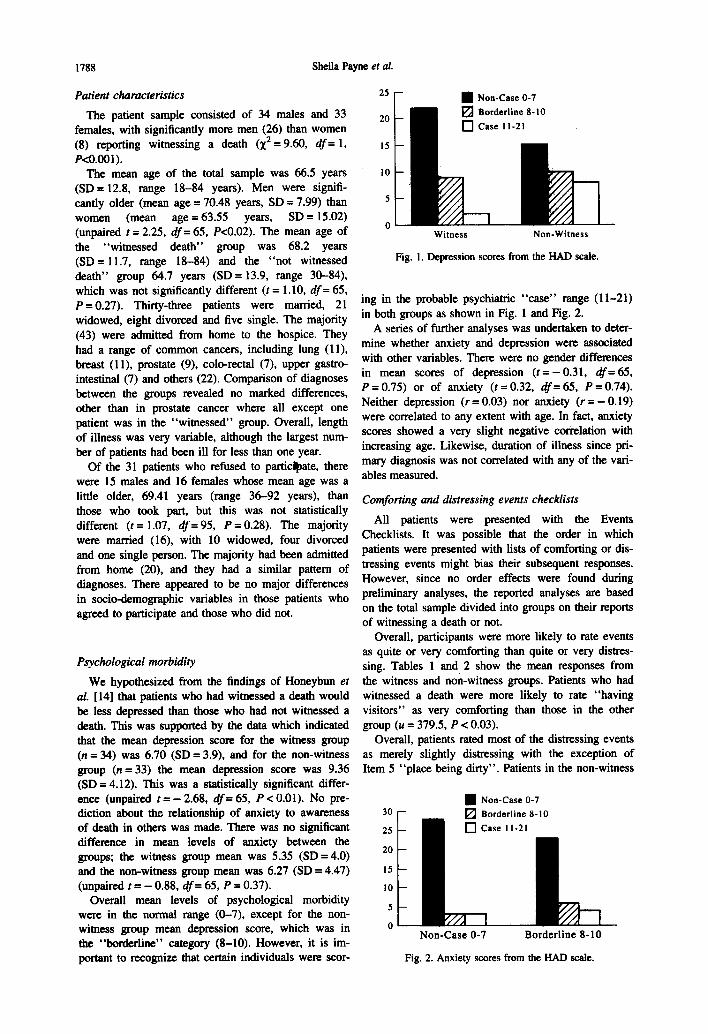
Overall, participants were more likely to rate events as quite or very comforting than quite or very distres- sing. Tables 1 and 2 show the mean responses from the witness and non-witness groups. Patients who had witnessed a death were more likely to rate "having visitors" as very comforting than those in the other group (u -- 379.5, P < 0.03).
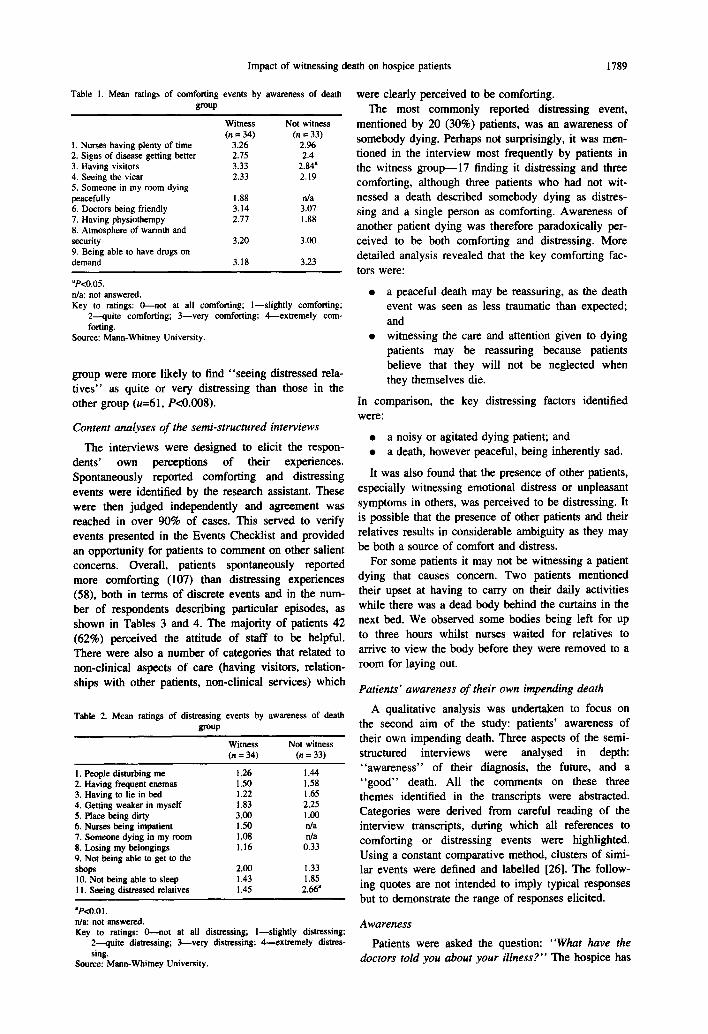
Overall, patients rated most of the distressing events as merely slightly distressing with the exception of Item 5 "place being dirty". Patients in the non-witness
30
25
20
15
I0
5
0
• Non-Case 0-7 [ ] Borderline 8-10
Non-Case 0-7 Borderline 8-10
Fig. 2. Anxiety scores from the HAD scale.
Impact of witnessing death on hospice patients 1789
Table 1. Mean ratings of comforting events by awareness of death group
Witness Not witness (n = 34) (n = 33)
I. Nurses having plenty of time 3.26 2.96 2. Signs of disease getting better 2.75 2.4 3. Having visitors 3.33 2.84 a 4. Seeing the vicar 2.33 2.19 5. Someone in my room dying peacefully 1.88 n/a 6. Doctors being friendly 3.14 3.07 7. Having physiotherapy 2.77 1.88 8. Atmosphere of warmth and security 3.20 3.00 9. Being able to have drugs on demand 3.18 3.23
ap<o.05. n/a: not answered. Key to ratings: 0--not at all comforting; l--slightly comforting;
2---quite comforting; 3--very comforting; 4--extremely com- forting.
Source: Mann-Whitney University.
group were more likely to find "seeing distressed rela- tives" as quite or very distressing than those in the other group (u=61, P<0.008).
Content analyses of the semi-structured interviews
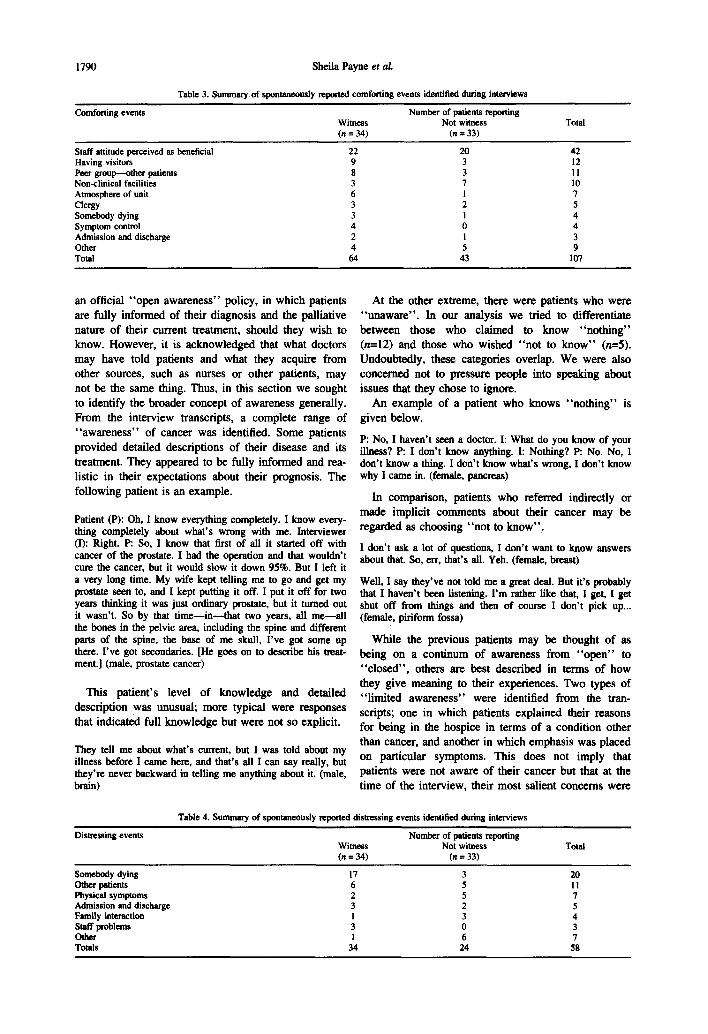
The interviews were designed to elicit the respon- dents' own perceptions of their experiences. Spontaneously reported comforting and distressing events were identified by the research assistant. These were then judged independently and agreement was reached in over 90% of cases. This served to verify events presented in the Events Checklist and provided an opportunity for patients to comment on other salient concerns. Overall, patients spontaneously reported more comforting (107) than distressing experiences (58), both in terms of discrete events and in the num- ber of respondents describing particular episodes, as shown in Tables 3 and 4. The majority of patients 42 (62%) perceived the attitude of staff to be helpful, There were also a number of categories that related to non-clinical aspects of care (having visitors, relation- ships with other patients, non-clinical services) which
Table 2. Mean ratings of distressing events by awareness of death group
Witness Not witness (n - 34) (n --- 33)
I. People disturbing me 1.26 1.44 2. Having frequent enemas 1.50 1.58 3. Having to lie in bed 1.22 1.65 4. Getting weaker in myself 1.83 2,25 5. Place being dirty 3.00 1.00 6. Nurses being impatient 1.50 n/a 7. Someone dying in my room 1.08 n/a 8. Losing my belongings 1.16 0.33 9. Not being able to get to the shops 2.00 1.33 10. Not being able to sleep 1.43 1.85 11. Seeing distressed relatives 1.45 2.66 a
aP<0.01. n/a: not answered. Key to ratings: 0--not at all distressing; l--slightly distressing;
2--quite distressing; 3--very distressing; 4---extremely distres- sing.
Source: Mann-Whitney University.
were clearly perceived to be comforting. The most commonly reported distressing event,
mentioned by 20 (30%) patients, was an awareness of somebody dying. Perhaps not surprisingly, it was men- tioned in the interview most frequently by patients in the witness group--17 finding it distressing and three comforting, although three patients who had not wit- nessed a death described somebody dying as distres- sing and a single person as comforting. Awareness of another patient dying was therefore paradoxically per- ceived to be both comforting and distressing. More detailed analysis revealed that the key comforting fac- tors were:
• a peaceful death may be reassuring, as the death event was seen as less traumatic than expected; and
• witnessing the care and attention given to dying patients may be reassuring because patients believe that they will not be neglected when they themselves die.
In comparison, the key distressing factors identified were:
• a noisy or agitated dying patient; and • a death, however peaceful, being inherently sad.
It was also found that the presence of other patients, especially witnessing emotional distress or unpleasant symptoms in others, was perceived to be distressing. It is possible that the presence of other patients and their relatives results in considerable ambiguity as they may be both a source of comfort and distress.
For some patients it may not be witnessing a patient dying that causes concern. Two patients mentioned their upset at having to carry on their daily activities while there was a dead body behind the curtains in the next bed. We observed some bodies being left for up to three hours whilst nurses waited for relatives to arrive to view the body before they were removed to a room for laying out.
Patients' awareness of their own impending death
A qualitative analysis was undertaken to focus on the second aim of the study: patients' awareness of their own impending death. Three aspects of the semi- structured interviews were analysed in depth: "awareness" of their diagnosis, the future, and a "good" death. All the comments on these three themes identified in the transcripts were abstracted. Categories were derived from careful reading of the interview transcripts, during which all references to comforting or distressing events were highlighted. Using a constant comparative method, clusters of simi- lar events were defined and labelled [26]. The follow- ing quotes are not intended to imply typical responses but to demonstrate the range of responses elicited.
Awareness
Patients were asked the question: "What have the doctors told you about your illness?" The hospice has
1790 Sheila Payne et al.
Table 3. Summary of spontaneously reported comforting events identified during intecviews
Comforting events Number of patients reporting Witness Not witness Total (n = 34) (n = 33)
Staff attitude perceived as beneficial 22 20 42 Having visitors 9 3 12 Peer group---other patients 8 3 l 1 Non-clinical facilities 3 7 10 Atmosphere of unit 6 1 7 Clergy 3 2 5 Somebody dying 3 1 4 Symptom control 4 0 4 Admission and discharge 2 1 3 Other 4 5 9 Total 64 43 107
an official "open awareness" policy, in which patients are fully informed of their diagnosis and the palliative nature of their current treatment, should they wish to know. However, it is acknowledged that what doctors may have told patients and what they acquire from other sources, such as nurses or other patients, may not be the same thing. Thus, in this section we sought to identify the broader concept of awareness generally. From the interview transcripts, a complete range of "awareness" of cancer was identified. Some patients provided detailed descriptions of their disease and its treatment. They appeared to be fully informed and rea- listic in their expectations about their prognosis. The following patient is an example.
Patient (P): Oh, I know everything completely. I know every- thing completely about what's wrong with me. Interviewer (I): Right. P: So, I know that first of all it started off with cancer of the prostate. I had the operation and that wouldn't cure the cancer, but it would slow it down 95%. But I left it a very long time. My wife kept telling me to go and get my prostate seen to, and I kept putting it off. I put it off for t w o years thinking it was just ordinary prostate, but it turned out it wasn't. So by that time--in--that two years, all me--all the bones in the pelvic area, including the spine and different parts of the spine, the base of me skull, I've got some up there. I've got secondaries. [He goes on to describe his treat- ment.] (male, prostate cancer)
This patient 's level of knowledge and detailed description was unusual; more typical were responses that indicated full knowledge but were not so explicit.
They tell me about what's current, but I was told about my illness before I came here, and that's all I can say really, but they're never backward in telling me anything about it. (male, brain)
At the other extreme, there were patients who were "unaware" . In our analysis we tried to differentiate between those who claimed to know "no th ing" (n=12) and those who wished "no t to know" (n=5). Undoubtedly, these categories overlap. We were also concerned not to pressure people into speaking about issues that they chose to ignore.
An example of a patient who knows "no th ing" is given below.
P: No, I haven't seen a doctor. I: What do you know of your i l lness? P: I don't know anything. I: Nothing? P: No. No, I don't know a thing. I don't know what's wrong, I don't know why I came in. (female, pancreas)
In comparison, patients who referred indirectly or made implicit comments about their cancer may be regarded as choosing "no t to know" .
I don't ask a lot of questions, I don't want to know answers about that. So, err, that's all. Yeh. (female, breast)
Well, I say they've not told me a great deal. But it's probably that I haven't been listening. I'm rather like that, I get, I g e t shut off from things and then of course I don't pick up... (female, piriform fossa)
While the previous patients may be thought of as being on a continum of awareness from " o p e n " to "c losed" , others are best described in terms of how they give meaning to their experiences. Two types of "l imited awareness" were identified from the tran- scripts; one in which patients explained their reasons for being in the hospice in terms of a condition other than cancer, and another in which emphasis was placed on particular symptoms. This does not imply that patients were not aware of their cancer but that at the time of the interview, their most salient concerns were
Table 4. Summary of spontaneously reported distressing events identified during interviews
Distressing events Number of patients reporting Witness Not witness Total (n = 34) (n = 33)
Somebody dying 17 3 20 Other patients 6 5 I I Physical symptoms 2 5 7 Admission and discharge 3 2 5 Family interaction 1 3 4 Staff problems 3 0 3 Other 1 6 7 Totals 34 24 58
Impact of witnessing death on hospice patients 1791
related to concurrent pathology or processes such as ageing. Hospice workers have long acknowledged the concept of "total pain" that results from more than just the cancer.
Well, they said that, not these doctors, that apparently I had a gast/'ie ulcer or something and that had got cancer cells in and all. I had a big stomach operation and I don't think they removed it all, sort of thing, so where we go from here I don't know. And my chief complaint is asthmatical. (male, stomach)
That I've got diabetes. (male, lung)
Err, well I don't know, it's just old age I should think. You know, I am getting past doing things for myself. (female, ovary)
Other patients, while acknowledging their cancer, tended to focus attention on immediate concerns.
Nothing much about my illness because I'm only here for a rest really. Nothing has developed in my illness recently. My only problem I've had since I've been here is my upset stomach. (male, myeloma)
Patients appeared to be able to control their levels of awareness in ways that were tolerable for them, In the course of an interview, some patients indicated different levels of awareness at different stages. Thus, we would propose the "awareness" should not be viewed as a stable attribute.
Future
Patients were asked the question: "How do you see your future?" There appeared to be two major dimen- sions along which responses were distributed. One dimension was the perceived length of future that they had and their feelings about that, and the other con- cerned goals or anticipated activities and events. The first dimension (the perceived length of their future) produced a cluster of responses (n = 7) at one extreme that indicated that the person perceived themselves to have no future.
Well basically, what they've told me is that I haven't got one!
Other patients reported not thinking about the future (n = 4), not looking at the future (n = 2), or not know- ing about the future (n = 2).
I don't think about the future any more because it's so uncer- tain. Don't know if I have got one. I don't know how long it is...and until I do I don't plan, I just get on with it and I do what I do while I can do it, and when I can't, I rest. That's all I can do.
Another group of responses may be thought of as being further along the continuum. These patients acknowledged that they might not have long to live (n = 2) and emphasized the importance of living "day- to-day" (n = 4).
Well, take it steady, day by day. That's all I've got to do really, and try to do little things what I want to do.
At the furthest extreme of this dimension, three patients spoke about "getting better" and two of enjoying life.
P: Well, sometimes I think I'm going to get better and I'll be okay. I: What about other times? P: I don't even think of that.
The alternative dimension (goals or anticipated ac- tivities) ranged from explicit references to death (n = 5) as a frequently anticipate event, to other, not necessarily incompatible goals such as returning home (n = 6) and other activities (n = 4). Only one patient explicitly mentioned being in favour of euthanasia.
I should like them to bring in euthanasia. If you gets pain then you can do away with yourself.
Most references to their own death indicated resig- nation and a lack of fear. The following is an example:
Oh, I think my future is that, quite definitely, probably within the next six months I will die. That's my future but it doesn't bother me. I can, I know it, I'm not mad, and I'm not stupid, but I really feel that within a year without any doubt, but it doesn't bother me in the least, you see. Don't know why I feel like this but I do. I didn't know I'd have the strength to go on like this but it doesn't bother me at all.
Other patients concentrated on achieving specific goals. The most commonly mentioned one was "going home". Four other goals were identified: driving the car, gardening, playing bridge and going shopping.
Well, I'm doing something about it at the moment by..Tm going to go home shortly, I'm working towards it with the physio, I did this, I went home before and there were...at- tempts to get me mobile to a certain level...I enjoy going home. That's why I'm keen to go again, even if it means being mobile in a chair, slightly different, but not impossible.
The most distressing aspect of the future for three people was their perception of the consequences of their death for relations. Some patients reflected on how their death might sadden their spouse or family.
"Good death"
In those patients who explicitly mentioned the word "death" , or made explicit reference to dying, we asked the question: "Have you an idea of what wouM make a good death?" To comply with Hospital Ethical Committee guidelines, it was decided not to ask this question of all patients as we wished to respect their right not to dwell on the topic of death if they did not wish to be "aware" . The most commonly (n = 6) identified characteristic of a good death was to die in one's sleep.
Just go to sleep and not wake up any more.
Patients also defined "good deaths" as being quiet, peaceful, dignified and pain-free.
Quietly in my sleep. I do pray sometimes that I would go, when I'm in pain, you know, and then I think how awful it's going to be for my family, you know, 'cause we are very close.
Opinions were divided on whether it was better to have warning of impending death or whether a sudden death was preferable. A small group of patients found the subject inappropriate to talk or think about.
1792 Sbeila Payne et al.
I don't know, I haven't thought about it. I've never wanted to talk about it.
Relatively few people made explicit references to religion or spiritual beliefs in response to our question, although those that did clearly found their belief sys- tems to be helpful. It was more common for people to mention their acceptance of death and their lack of fear, and one person spoke of being reunited with his spouse.
I have to be with the Lord. I've always believed in God. You just go peaceful.
Interestingly, a "good death" was rarely described as an abstract phenomenon. Patients generally provided us with descriptions of actual "good" deaths and less frequently "bad" deaths which they had witnessed. These were often the deaths of family members whom they had cared for. These were often detailed narra- tives, during which our respondents highlighted aspects of a "good" death.
Well, I always said I'd like to die like my second husband. He just simply dropped dead one day. He'd been on the sick list, but he simply just dropped dead. He'd been mowing the lawn out in the garden. Now my first husband, I watched die slowly of cancer, so I know which I would chose. I always prayed that when I die it would be...I think most people would. Nobody would wish to linger on. But having said that, I don't think I'd go so far as to try and assist, assist in any way. Your time is your time.
Patients also engaged in social comparisons between themselves and other patients, which indicates the im- portance of their perceptions of other patients, such as the following example.
Without pain. Yes, what more can I say, I don't know. Like the guy opposite and went to sleep one night and forgot to wake up.
In summary, a "good death" was defined not only as a list of features that included sleep, freedom from pain, quietness and dignity, but as narratives of actual deaths that were contextualized within their life.
DISCUSSION
The results of this study have provided evidence that patients are aware of their fellow patients in a pal- liative care unit but that "awareness" of their own and others' deaths may best be thought of as a process rather than as a stable attribute. Our findings support the hypothesis that patients who report witnessing the death of fellow patients are significantly less depressed than those who do not. Thus, this study replicates the findings of Honeybun e t al. [14] in a larger sample and in a different institution. It is important to recog- nize that admitting patients to an in-patient palliative care unit, where they may be exposed to other dying patients, does not increase psychological morbidity. In fact, it may be construed as being helpful for patients to witness the care and attention afforded to others.
This study is limited in several respects. In sampfing only one palliative care unit, we are cautious in gener-
alizing these findings. As the study design was cross- sectional, we are unable to draw conclusions about the direction of causality. Moreover, although we have argued that "awareness" may be a dynamic rather than static attribute, this is based on changes occurring during the course of a single interview. A series of interviews would provide more convincing evidence such as the methodology employed by Hinton [27]. The sample size, although larger than that reported by Honeybun et al. [14], must be regarded as relatively small. The refusal rate of 31% means that there may be an important subgroup that we know little about.
The use of standardized measures and checHists can go only so far in providing an understanding of the ex- perience of patients. We wished to provide patients with an opportunity to express their salient concerns in the context of a semi-structured interview. Thus, we would argue that the qualitative analysis goes some way to enable patients to voice their experiences, although we acknowledge the power relationships that are inherent during interviews and the process of selec- tion and reconstruction that are required during analy- sis [28].
Psychological morbidity in our sample was largely accounted for by depression, rather than anxiety, unlike data collected from breast cancer patients in the early stages of treatment where anxiety is more com- mon. A point prevalence of psychiatric disorder of 48% at six weeks and 17% at 20 weeks post-diagnosis of breast cancer has been reported [29]. This indicates much higher initial levels than in the terminally ill where we found 10.4% (7/67) had probable case levels of anxiety and 16.4% (I 1/67) had probable case levels of depression. There is some discussion as to whether the social withdrawal, reduced engagement with others, and lack of enjoyment of usual activities, which are characteristic of people dying of cancer, are indicative of clinical depression [30]. It could be argued that these are normal aspects of the process of dying. We found that two items on the HAD scale were probably confounded with physical deterioration. They were: "I feel slowed down" and "I still enjoy the activities that I use to enjoy". We suggest that other investigators may wish to remove these items or investigate an alternative measure of depression for these types of patients.
More male patients than female patients reported witnessing a death. It is known that men are less likely to report psychological and physical symptoms [31], [32]. However, this systematic bias is unlikely to account for our results because we found no statisti- cally significant gender differences in depression scores. In addition, increasing age or the duration of the illness were not correlated with the levels of de- pression recorded.
In offering an explanation for these findings, we wish to propose that patients may systematically vary in their social orientation to, and engagement with, other people. The evidence for this proposal is in the differences in responses to the Events Checklist, where
Impact of witnessing death on hospice patients 1793
patients in the witness group were significantly more comforted by having visitors while the non-witness group were significantly more distressed by seeing dis- tressed relatives. It could be argued that patients who did not witness a death were less socially orientated to events in the hospice and that they found it more diffi- cult to cope with other patients and their relatives. Overall, patients in the witness group reported both more comforting and distressing events. This suggests that they were more aware of, or more willing to talk about, what was happening around them, both "good" and "bad" events. An alternative explanation is that they were less ill or less heavily sedated. The focus of research has been on death as an event, rather than the social processes that occur in the period preceding and immediately following a death that are likely to involve a number of interactants, namely, the patients, their relatives and friends, and staff. It is possible that vicarious suffering is endured by some patients who witness the distress of others' loved ones. Future in- vestigators may wish to explore these possibilities.
Awareness of others dying was found to be both comforting and distressing. Interaction with other patients may be ambiguous. Patients may choose to maintain a social distance from their fellow patients because they need to protect themselves [33]. According to Festinger's social comparison theory [34], people use other people rather than objective criteria as a basis for comparison. From the inter- views, we found many instances of social comparison which on the whole appeared to be helpful to patients, as they perceived others to be worse off than themselves. There is evidence that cancer patients use fellow patients as a reference group [35], [33] and that there is a tendency to denigrate others in the process. For example, patients may emphasize the more negative attributes of others, especially in relation to symptoms. Social identity theory would predict that people have both a personal identity and a group identity [36]. It is possible that patients who are not socially engaged with others in the hospice fail to acquire a group identity.
This study aimed to understand to what extent patients were aware of their own impending death. We wished to know how they understood the construct "good death". It has been suggested that the "good death" has become an ideal institutionalized by the hospice movement [37]. Patients were more likely to mention that a "good death" occurred in one's sleep, although quietness, pain control and dignity were also important issues. Some patients provided narratives of the deaths they had known. In these narratives, they were able to highlight features of the deaths that rep- resented to them good and bad aspects. Thus, in these interviews, death was not usually constructed as an abstract phenomenon that could be analysed in its con- stitnent parts but was presented to us as actual stories embedded in their social context. This corresponds with Taylor's [38] findings and conclusions in a study of hospice nurses' concepts of death, that narratives
are a good methodological tool for investigating these issues.
Bearing in mind the caveats about the methodologi- cal limitations of this study, the results seem largely to support the view that while, paradoxically, awareness of dying is reported by patients as both comforting and distressing, patients who report witnessing the deaths of fellow patients were less depressed than those who do not. "Awareness" is a central tenet of hospice phil- osophy, yet remains problematic. There is an assump- tion that "open awareness" is a good thing and that the attainment of this goal should guide the provision of care and style of communication in palliative care. It is unknown to what extent patients may have a pri- vate awareness that is not manifest in public state- ments or discussions with staff and/or family. The accounts provided by patients during this investigation suggest that further research would be timely and worthwhile.
Acknowledgements--We would like to thank the patients and staff at the hospice, who generously gave their time to partici- pate in this study. This study was funded by the Wessex Regional Health Authority.
REFERENCES
1. Field D. and James N. Where and how people die. In The Future of Palliative Care (Edited by Clark D.), pp. 6-29. Open University Press, Buckingham, 1993.
2. Directory of Hospice and Palliative Care Services. Hospice Information Service, Sydenham, London, 1994.
3. Sykes N. P., Pearson S. E. and Chell S. Quality of care of the terminally ill: the carer's perspective. Palliative Medicine 6, 227-236, 1992.
4. Field D. Nursing the Dying. Routledge, London, 1989.
5. Glaser B. G. and Strauss A. L. Awareness of Dying. Aldine, Chicago, 1965.
6. Sudnow D. Passing On: The Social Organisation of Dying. Prentice-Hall, Englewood Cliffs, NJ, 1967.
7. Kubler-Ross E. On Death and Dying. New York, Macmillan, 1969.
8. James N. and Field D. The routinization of hospice: charisma and bureaucratization. Social Science & Medicine 34 (12), 1363-1375, 1992.
9. Seale C. Communication and awareness about death: a study of a random sample of dying people. Social Science & Medicine 32 (8). 943-952, 1991.
10. Saunders C. The philosophy of terminal care. In The Management of Terminal Disease (Edited by Saunders C.), pp. 193-202. Edward Arnold, London, 1978.
11. Coleman P. G. Identity management in later life. In Handbook of the Clinical Psychology of Ageing (Edited by Woods R.), pp. 93-113. Wiley, Chichester, 1995.
12. Mackay L. Conflicts in Care. Chapman and Hall, London, 1993.
13. Manning M. The Hospice Alternative: Living with Dying. Condor Books, Souvenir Press, London, 1984.
14. Honeybun J., Johnston M. and Tookman A. The impact of death on fellow hospice patients. British Journal of Medical Psychology 65, 67-72, 1992.
1794 Sheila Payne et al.
15. Hunt M. "Scripts" for dying at home---displayed in nurses', patients' and relatives' talk. Journal of Advanced Nursing 17, 1297-1302, 1992.
16. Littlewood J. Aspects of Grief. London, Routiedge, 1992.
17. Standing Medical Advisory Committee and Standing Nursing and Midwifery Advisory Committee. The Principles and Provision of Palliative Care, Joint Report. HMSO, London, 1992.
18. Bryant A. and Payne S. Difficulties inherent in research with cancer patients. Journal of Cancer Care 2, 143-146, 1993.
19. de Raeve L. Ethical issues in palliative care research. Palliative Medicine 8, 298-305, 1994.
20. Mount B. M. et al. Ethical issues in palliative care research revisited. Palliative Medicine 9, 165-170, 1995.
21. Zigmond A. S. and Snaith R. P. The Hospital Anxiety and Depression scale. Acta Psychiatria Scandinavia 67, 361-370, 1983.
22. Moorey S. et al. The factor su'ucture and factor stab- ility of the Hospital Anxiety and Depression scale in patients with cancer. British Journal of Psychiatry 158, 255-259, 1991.
23. Carroll B. T. et al. Screening for depression and anxiety using the Hospital Anxiety and Depression scale. General Hospital Psychiatry 15, 69-74, 1993.
24. Silverstone P. H. Poor efficacy of the Hospital Anxiety and Depression scale in the diagnosis of major depressive disorder in both medical and psy- chiatric patients. Journal of Psychosomatic Research 38 (5), 441--450, 1994.
25. Lloyd Williams M. Assessing depression in the hos- pice population using the Hospital Anxiety and Depression scale---a pilot study. Journal of Cancer Care 3, 164-165, 1994.
26. Strauss A. L. and Corbin J. Basics of Qualitative Research: Grotolded Theory Procedare$ and Techniques. Sage, Newbury Park, CA, 1990.
27. Hinton J. Can home care maintain an acceptable quality of life for patients with terminal cancer and their relatives? Palliative Medicine 8, 183-196, 1994.
28. Reissman C. K. Narrative Analysis. Sage, London, 1993.
29. Pinder K. L., Ramirez A. J., Richards M. A. and Gregory W. M. Cognitive responses and psychiatric disorder in women with operable breast cancer. Psycho-Oncology 3, 129-137, 1994.
30. Mermeistein H. T. and Lesk L. Depression in patients with cancer. Psycho-Oncology I, 199-215, 1992.
31. Popay J., Bartiey M. end Owen C. Gender inequal- ities in health: social position, alfective disorders and minor physical morbidity. Social Science & Medicine 36 (1), 21-32, 1993.
32. Macintyre S. Gender differences in the perception of common cold symptoms. Social Science & Medicine 36 (1), 15-20, 1993.
33. Isaksen A. S. The sicnlflcance of fellow patients to hospitalized cancer patients. Paper presented at the 8th International Conference on Cancer Nursing, Vancouver, Canada, 1994.
34. Festinger L. A theory of social comparison processes. Human Relations 7, 117-140, 1954.
35. Payne S. Quality of life in women with advanced cancer. Unpublished PhD thesis. University of Exeter, Exeter, 1989.
36. Brewer M. B. The social self: on being the same and different at the same time. Personality and Social Psychology Bulletin 17, 475--482, 1991.
37. McNamara B., Waddell C. and Colvin M. The insti- tutionalization of the good death. Social Science & Medicine 39 (11), 1501-1508, 1994.
38. Taylor B. Hospice nurses tell their stories about a good death: the value of storytelling as a qualitative health research method. Annual Rei, iew of Health and Social Science 3, 97-108, 1993.





























