Embed Size (px)
Citation preview

COPYRIGHT © 2007 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
1832
Current Concepts Review
Impingement with Total Hip ReplacementBy Aamer Malik, MD, Aditya Maheshwari, MD, and Lawrence D. Dorr, MD
Investigation performed at The Arthritis Institute, Inglewood, California
➤ Impingement is a cause of poor outcomes of prosthetic hip arthroplasty; it can lead to instability, acceleratedwear, and unexplained pain.
➤ Impingement is influenced by prosthetic design, component position, biomechanical factors, and patient variables.
➤ Evidence linking impingement to dislocation and accelerated wear comes from implant retrieval studies.
➤ Operative principles that maximize an impingement-free range of motion include correct combined acetabularand femoral anteversion and an optimal head-neck ratio.
➤ Operative techniques for preventing impingement include medialization of the cup to avoid component im-pingement and restoration of hip offset and length to avoid osseous impingement.
he principles regarding impingement in the naturalosseous (anatomic) hip put forth by Ganz et al.1-5 aresimilar in concept to what can occur in the prosthetic
hip. To understand impingement, it is helpful to recognizethe common mechanisms that cause mechanical abutmentin both anatomic and prosthetic hips. In the anatomic hipjoint, impingement is a mechanical abutment conflict be-tween the bone of the femur and the pelvis; in a total hip re-placement, it is contact between the metal femoral neck andthe cup liner or bone-to-bone contact such as between thegreater trochanter and the pelvis3,6,7. The femoral head-neckratio, which is the relationship between the diameter of thefemoral head and the diameter of the femoral neck, influ-ences impingement. Cam impingement is caused by a re-duced femoral head-neck ratio. An example is the pistol-gripdeformity that is created by a decreased offset of the femoralhead-neck junction3 (Fig. 1). Cam impingement in a pros-thetic hip is caused by any implant feature that reduces thehead-neck ratio. A skirt on the metal femoral head or a largecircular femoral neck can cause mechanical abutment in aprosthetic hip through this mechanism8-10 (Fig. 1). Pincerimpingement in the anatomic hip is a mechanical abutment
caused by acetabular retroversion, protrusio, or coxa pro-funda. Pincer impingement in the prosthetic hip is caused byhooded and constrained liners or by placement of a smallfemoral head in a big acetabular cup11-13. Failure to removeacetabular osteophytes so that the metal neck or the femoralbone abuts on the osteophytes is another cause of pincer im-pingement (Fig. 1).
Because impingement is a dynamic process, it has beendifficult to identify it and to define its prevalence on the basisof clinical evaluations or plain radiographs. In the clinical set-ting, some causes of failure such as wear or dislocation areinferre to be related to impingement8-10,14,15, but a direct rela-tionship with impingement has been difficult to document.There are no radiographic techniques with which to validatethe occurrence of impingement. Retrieval studies are per-formed to examine implants that have failed16-20, but we are notaware of any autopsy retrieval studies of well-functioningprosthetic hips that have shown the true prevalence of im-pingement. The purpose of this review is to discuss the cur-rent understanding of the mechanisms of impingement intotal hip replacements, the clinical consequences of impinge-ment, and new developments.
T
Disclosure: In support of their research for or preparation of this work, one or more of the authors received, in any one year, outside funding or grantsin excess of $10,000 from Zimmer. In addition, one or more of the authors or a member of his or her immediate family received, in any one year, pay-ments or other benefits in excess of $10,000 or a commitment or agreement to provide such benefits from a commercial entity (ORTHOsoft). Nocommercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, division, center, clinical practice, or othercharitable or nonprofit organization with which the authors, or a member of their immediate families, are affiliated or associated.
J Bone Joint Surg Am. 2007;89:1832-42 • doi:10.2106/JBJS.F.01313
Dorr_CCR.fm Page 1832 Wednesday, July 11, 2007 2:05 PM

1833
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
Mechanisms of Impingement in Total Hip Replacements
mpingement in the prosthetic hip is both device andsurgeon-dependent21. The device-design factors are those
that influence the femoral head-neck ratio as well as featuresof acetabular design. The surgeon controls the position of thecup with regard to inclination and anteversion as well as to itsdepth in the osseous acetabulum. Following placement of thecup, the surgeon controls the level of the osseous femoral neckcut and the placement of the femoral component for the bio-mechanical reconstruction of the hip length and offset, whichreduces the occurrence of impingement22,23.
A common implant design feature that causes cam-typeimpingement is a reduced head-neck ratio15,19,21. The articula-tion of the prosthetic hip requires an acetabular component ofa certain thickness, thereby diminishing the size of the femoralhead compared with that of the osseous femoral head. A head-neck ratio of <2.0 in a prosthetic hip seems to greatly increasethe risk of impingement19. The head-neck ratio is influencedby the head size, the femoral neck geometry, and the use of askirt on the femoral head10,19,21 (Figs. 2-A and 2-B). Cam-typeimpingement can occur with use of a small head on a largecircular taper8,9,15 or use of a skirted femoral head8,10,12, both ofwhich can result in a head-neck ratio of <2.019. A trapezoidal-shaped neck designed to create a better head-neck ratio, par-ticularly with small heads, is preferable7,21.
Features that increase acetabular impingement includethe chamfer geometry of the rim of the polyethylene21,24,25 andthe presence of an extended-rim (hooded) liner, particularly ifthe hood is incorrectly positioned in the hip21,26,27. The surgeonincreases the risk of impingement by placing the cup in a lat-
eralized horizontal position28,29 or by failing to remove acetab-ular osteophytes that can impinge against the metal neck orthe femoral bone30,31. If a hood is used in an operation per-formed through a posterior approach, its apex should beplaced posteroinferiorly (in the 4 o’clock position in left hipsand in the 8 o’clock position in right hips), as the most fre-quent site of impingement is posterosuperior20,27.
Bone-on-bone impingement is surgeon-dependent, asthe surgeon controls implant position and the restoration oflimb length and offset6,22. A short hip length, or more com-monly a short offset, places the hip at risk for the femoralbone impinging against the pelvis at the extremes of motion.Most commonly, the offset of the hip in a standard total hipreplacement should even be increased a few millimeters toavoid impingement because the femoral head is smaller thanthe osseous head22,32,33. The neck-shaft angle of the femoralcomponent used by the surgeon can influence the reconstruc-tion of both limb length and offset7,23. The surgeon needs to beaware of the neck-shaft angle and the level of the correspond-ing osseous neck cut for that implant (Figs. 3-A and 3-B).
Even in ideally reconstructed hips, two causes of im-pingement persist. Patients who are particularly flexible (usu-ally women) have a risk of osseous impingement at theextremes of motion3,30. The use of the largest femoral head sizepossible will be of benefit in flexible patients34,35. A secondcause of impingement is the degree of pelvic tilt that occurs insome patients as a result of the static pelvic position on theoperating table relative to the dynamic pelvic position duringactivities5,36. Even with correct combined anteversion of theimplants and biomechanical reconstruction of the hip, the ex-tremes of flexible pelvic positions change the component and
I
Fig. 1
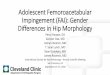
Biomechanics of impingement. Reduced clearance leads to repetitive abutment between the femur and the acetabular rim in
the anatomic hip or between the femoral component and the acetabulum in the prosthetic hip. A: A normal anatomic hip and
an ideal total hip replacement with a large femoral head and a high head-neck ratio. B: Cam-type impingement in the native
hip caused by a reduced femoral head-neck offset and similar impingement in a prosthetic hip with a small femoral head
and a skirted femoral neck. C: Pincer-type impingement can result from excessive overcoverage of the femoral head in the
native acetabulum or from inadequate removal of acetabular osteophytes in the prosthetic hip. D: A combination of the cam
and pincer types of impingement in the native hip as well as in a prosthetic hip with a small femoral head, a head-neck ratio
of <2.0, a large cup, and a polyethylene liner with no chamfers.
Dorr_CCR.fm Page 1833 Wednesday, July 11, 2007 2:05 PM

1834
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
bone relationships so that impingement can still occur5,36.The variables causing impingement are additive so that
it is incumbent on the surgeon to understand the device beingused, its influence on biomechanical reconstruction, and itslimitations in the context of patient variables. A good exampleof a patient who is at high risk for impingement would be aflexible woman with a small skirted femoral head and a poorlypositioned elevated acetabular liner.
Finite-Element Analysishe focus of finite-element studies has been to determinecomponent designs and positions that are least likely to
cause impingement throughout the range of motion24,25,37-44.Computer modeling is attractive because it makes it possibleto study specific variables under well-controlled conditions.
The limitation of these studies is the inability to evaluate therelationship of the three-element implant-soft tissue-bonestructure clinically6,45. Furthermore, the optimal componentposition for an impingement-free range of motion in a finite-element study may well have an adverse effect on wear andtherefore implant longevity. An example of this is the recom-mendation by D’Lima et al.24 that the ideal inclination of theacetabular component to avoid impingement is 45° to 55°.However, this same research group observed clinically that in-clination exceeding 45° led to a 40% increase in mean linearwear of the polyethylene41.
One weakness of finite-element studies is that the anglesof the cup are altered without any change in the center of ro-tation (depth) of the cup (Figs. 4-A, 4-B, and 4-C). When thecenter of rotation is not moved medially and/or superiorly, ade-quate coverage of the cup by acetabular bone can be achievedonly with higher inclination. Clinically, surgeons have learnedthat, by moving the cup medially and/or superiorly from theoriginal center of rotation, they can reduce the inclination to nomore than 45° and yet provide appropriate coverage of the cupso that the cup is not lateralized28,29,46,47 (Figs. 4-A, 4-B, and 4-C).Avoiding a lateralized cup decreases the likelihood of impinge-ment of the metal neck against the rim of the cup.
A second error in computer modeling of the position ofthe acetabular component has been the assumption that the an-teversion of the femoral component is 10° to 15°21,37. The sur-geon can control the amount of anteversion of a cemented stembut not of a noncemented stem40,48. Because of the necessity toobtain a press-fit of the implant into the bone, the anteversionpresented by the bone must be used for the implant40,48. In twostudies, computed tomography scans of implanted stemsshowed a range of femoral anteversion of 30° of retroversion to45° of anteversion, with a mean of 16.5° and 16.8°31,49.
Clinical Consequences of Impingementontact between a metal neck and a plastic liner can have anumber of potentially adverse consequences, including
limited motion and function; increased stress on the liner rim,resulting in dislodgment of the modular liner or acceleratedloosening of the implant; liberation of metal debris from thefemoral neck; generation of rim wear, potentially increasingthe risk of osteolysis; and subluxation and dislocation21.
Dislocation is a frequent cause of implant failure thatoccurs because of impingement8,9,15,21,36,50,51. When impinge-ment occurs in the prosthetic hip, there is a sliding contact ofthe femoral head within the polyethylene or a hard-on-hardarticular surface43. The polyethylene creates a resisted mo-ment to the femoral head, which helps prevent it from slidingout of the polyethylene bore43. If the external loading challengecreating the impingement is great enough, the resisting mo-ment cannot contain the femoral head and dislocation occurs.
Laboratory and clinical models have demonstrated thedirect relationship between impingement and dislocation.Computer-aided-design studies have shown a correlation be-tween specific implant variables and clinical outcomes withregard to dislocation8,15. Barrack et al.8 found that, when the
T
CFig. 2-B
A trapezoidal stem geometry favors an increase in the impingement-
free range of motion compared with that associated with a circular
neck design. The inset picture illustrates the decrease in neck diame-
ter with the trapezoidal design (darkly shaded area) compared with that
of a circular neck design (lightly shaded area).
Fig. 2-A
Figs. 2-A and 2-B Head size and neck geometry can influence the
head-neck ratio, which is the head diameter divided by the neck diame-
ter. These illustrations show the relationship between the cup and liner
with different head and neck designs. Fig. 2-A The effect of increasing
the femoral head size on impingement. A larger head increases the im-
pingement-free range of motion.
Dorr_CCR.fm Page 1834 Wednesday, July 11, 2007 2:05 PM

1835
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
femoral neck of an implant had a large circular cross-sectionaldiameter, the clinical dislocation rate (eight of fifty-two; 15%)was three times higher than the dislocation rate of implantswith a smaller trapezoidal neck (two of forty-six; 4%) (p =0.07). With use of earlier computer modeling, they had veri-fied an increase in impingement and a 46% decrease in the arcof motion in association with the large femoral tapers8. Simi-larly, Padgett et al.15, with a computer model study, found thatsmall-diameter heads with a larger taper demonstrated im-pingement at <90° of flexion. In a clinical review of 254 pri-mary hip prostheses with the same neck design, they found anoverall dislocation rate of 4.7% (twelve hips). As stratified byhead size, the dislocation rates were 3.6% for 28-mm bearings,4.8% for 26-mm bearings, and 18.8% for 22-mm bearings.Padgett et al. discontinued clinical use of the 22-mm headwith a large taper as a consequence of these results15.
Pain is a common consequence of impingement52,53.When impingement on capsular or tendon soft tissues occurs ina prosthetic hip, inflammation and swelling frequently result ingroin pain53,54. Three scenarios of pain resulting from soft-tissueimpingement are: (1) when a large acetabular component over-hangs medially or the lesser trochanter abuts against the is-chium, causing iliopsoas tendinitis; (2) when the capsule iscompressed between the metal neck and the cup; or (3) whenthe capsule is compressed between the greater trochanter andthe ilium53,54. Pain can be relieved by local anesthetic infiltrationor surgical release of the iliopsoas tendon without the need forrevision of the acetabular component54,55. Patients who experi-ence subluxation and pain may require computed tomographyscans to document osteophytes or component malposition thatcreates the impingement causing the subluxation31.
Impingement between the metal neck of the femoralcomponent and the polyethylene rim of the cup can damage thepolyethylene both at the site where the neck contacts the rim
and the egress site where the femoral head escapes from thepolyethylene bore43. When the external load challenges are high,the resistive moment within the polyethylene can exceed theyield strength of the polyethylene and, with chronic impinge-ment, can lead to polyethylene damage through increasedwear and/or cracking of the liner with subsequent implantfailure10,19,56,57. Oxidized liners are at highest risk for damageand failure from impingement56,57. Birman et al.56 analyzed 120metal-backed conventional polyethylene liners and foundseventy-one (59%) to have impingement damage secondary tocontact between the metal neck and the polyethylene, seventy-eight (65%) to have oxidation damage, and forty-eight (40%)to have cracks in the polyethylene. Cracks were always associ-ated with some degree of impingement damage and oxidation.
Retrieval studies have shown impingement to be a con-tributing cause of increased wear. Yamaguchi et al.20 corre-lated impingement with linear wear, with the average wearrate being 0.33 ± 0.28 mm/yr for liners with impingementcompared with 0.19 ± 0.14 mm/yr for liners without impinge-ment (p = 0.009). Usrey et al.19, in a retrieval study of 113 cups,correlated volumetric wear of liners with the degree of impinge-ment; the average volumetric wear rate was 159 ± 42 mm3/yrfor liners with severe impingement compared with 70 ± 21mm3/yr for liners with no or mild impingement (p = 0.02).Kligman et al.58 found evidence of impingement in sixty-twoof eighty-six modular polyethylene liners and reported thatit was correlated with backside polyethylene wear and screw-metal shell corrosion and fretting. The superolateral (poster-osuperior) area of the liner is the most common site ofimpingement16,20,27. Yamaguchi et al. found that the most com-mon site was 78° ± 20° posterosuperiorly. Shon et al.18 con-firmed that posterior impingement is the most common butfound greater variation in impingement sites. It is possiblethat this variation was a combination of the impingement and
Fig. 3-A
Fig. 3-A An osteoarthritic right hip with a varus femoral neck-shaft angle of 124°. A standard implant with a neck-shaft angle of 131° does not re-
produce the correct offset. Fig. 3-B A high-offset implant with a neck-shaft angle of 121° allows correct reconstruction of offset.
Fig. 3-B
Dorr_CCR.fm Page 1835 Wednesday, July 11, 2007 2:05 PM

1836
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
the egress site in hips that had subluxated or dislocated. Bothposterosuperior and posteroinferior impingement can occurin the extension phase of the gait cycle20.
Impingement has been implicated as a cause of looseningof both femoral and acetabular components12,59,60. Bosco and
Benjamin59 and Kobayashi et al.61 reported a clinical correlationof impingement with wear and subsequent osteolysis. Bothgroups of authors reported loosening of a femoral componentresulting from wear debris generated almost exclusively by thepolyethylene damage at the neck-cup impingement site. Isaac etal.17, in their retrieval study, found that one of four possiblemechanisms of cup loosening was increased shear and tensileforces at the bone-cement interface resulting from increasedimpingement. Murray27 also correlated impingement with loos-ening of the Charnley cup. Dobzyniak et al.62 examined thecauses of revisions done in the first five years following total hipreplacements; they reported that loosening was the most com-mon cause for revisions performed from 1986 to 1991 and in-stability was a more common cause for those done from 1992 to2001. Loosening occurs early when it is caused by mechanicalabutment between poorly fixed implants. The prevalence of in-stability in the second half of the study by Dobzyniak et al. mayhave been caused by a change from cemented to noncementedstems and a failure to recognize a change in the femoral antever-sion of some stems from what had been anticipated. These au-thors desired a stem anteversion of 15° to 20°, which can becontrolled by the surgeon when a cemented stem is implantedbut is uncommonly achieved when a cementless stem is used.
Metal-on-metal and ceramic-on-ceramic impingementeach causes specific adverse outcomes leading to failure pecu-liar to the particular bearing surface. Recent reports seem toindicate an increased risk of fracture and squeaking due tosurface abrasion of the ceramic-on-ceramic couple related tocomponent malposition and impingement63,64. Metal-on-metal implants have been shown to generate metallosis sec-ondary to impingement52,65. Howie et al.66 found, in a retrievalstudy, that nine (38%) of twenty-four McKee-Farrar prosthe-
Fig. 4-A
An osseous anatomic osteoarthritic acetabulum that averages 55° of
inclination and 12° of anteversion is shown. Placing a cup in this posi-
tion provides adequate osseous coverage but is unfavorable for wear
and stability.
Fig. 4-B
Lateralizing the cup also is unfavorable with regard to impingement and consequent wear and in-
stability. If the cup is uncovered, there will be component-to-component impingement (arrows).
Dorr_CCR.fm Page 1836 Wednesday, July 11, 2007 2:05 PM

1837
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
ses had impingement caused by a poor head-neck ratio.Hip resurfacing provides large femoral head sizes that are
favorable in terms of the range of motion and stability, but anideal head-neck ratio can be difficult to achieve and there isstill a risk of implant failure caused by impingement67,68. Beauléet al.67 recognized the risk of impingement from malposition of
the implant or from a lack of correction of an underlying de-formity resulting in a reduced head-neck ratio (such as a pistol-grip deformity). Two considerations regarding offset must bekept in mind to avoid cam impingement postoperatively: first,in the coronal plane, it is critical to maintain the anterosupe-rior offset of the femoral head on the femoral neck and to
Fig. 5
Palpation to detect possible impingement by assessing the relationship of the tip of the lesser tro-
chanter to the tip of the ischium. At least one fingerbreadth of distance should be present. The same
test should be done to test for impingement of the greater trochanter against the ilium with the lower
limb in external rotation and abduction and to test for impingement of the greater trochanter against
the anterior inferior iliac spine with the lower limb in internal rotation, flexion, and adduction.
Fig. 4-C
Medializing the cup maintains the cup in 40° of inclination and 25° of anteversion while obtaining
correct cup coverage, but it increases the risk of bone-to-bone impingement (arrows). This can be
avoided by adjusting the level of the neck cut or using a longer femoral head or a high-offset stem.
Dorr_CCR.fm Page 1837 Wednesday, July 11, 2007 2:05 PM

1838
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
avoid notching, and second, in the sagittal plane, the anterioroffset should be reconstructed. Beaulé et al. found that preop-eratively 57% of sixty-three osteoarthritic hips had a femoralhead-neck offset ratio of ≤0.15, which requires correction atsurgery to decrease the risk of impingement.
Wiadrowski et al.69 found that the poor acetabular de-sign of the Wagner metal-on-polyethylene hip resurfacingprosthesis was a risk factor for impingement, with ninety-twoof 109 retrieved components showing peripheral damagecaused by impingement of the femoral neck on the polyethyl-ene cup. Wiadrowski et al. attributed this observation to thehemispherical (180°) sector of the cup and recommended thatfuture designs have less of a hemispherical shape. The newgeneration of hip resurfacing implants, such as the Birming-ham hip implant (Smith and Nephew, Memphis, Tennessee)and the Durom hip implant (Zimmer, Warsaw, Indiana) havesector angles of 159.2° and 165°, respectively. Impingementcan still be a problem with the new metal-on-metal design.Amstutz et al.70 reported the need for a revision of a surface re-placement in a dysplastic hip that had a poor femoral offsetthat had resulted in trochanteric-ischial impingement.
Current Developments for Avoiding ImpingementComponent Positioning
nteversion of cemented stems can be controlled by the sur-geon because a stem with a diameter smaller than that of
the medullary canal of the femur can be used and can be ma-nipulated into 10° to 15° of anteversion while being fixed withthe cement. Research on the position of the acetabular compo-nent has focused on a so-called safe zone, which was consideredsafe for stability (and hopefully avoidance of impingement)when used in combination with a stem in 10° to 15° of antever-sion. For cemented total hip replacements, Charnley recom-mended that the cemented cup be positioned in little or noanteversion71, whereas Müller72 and Coventry et al.73 suggestedan anteversion angle of 10° and Harris74 recommended an ante-version angle of 20°. Lewinnek et al.75 recommended a targetrange of 5° to 25° of anteversion, and McCollum and Gray36
suggested 20° to 40° of anteversion with use of pelvic anatomiclandmarks for intraoperative cup placement. McCollum andGray discounted the importance of femoral stem positioningbecause they used cemented stems, and they considered thathead coverage by the acetabulum changes very little with simpleinternal and external rotation of the lower limb when femoralanteversion is 10° to 15°. The clinical data on impingement(discussed in the section on clinical consequences of impinge-ment) were all derived on the basis of operations in which thesurgeon assumed a femoral anteversion of 10° to 15° while posi-tioning the cup into a given target amount of anteversion.
It is now known that ≤45° of inclination is best forachieving stability and preventing wear41,42. Forty degrees iscommonly referenced as the best target number because it pro-vides a 5° margin of error21. Achieving 40° of inclination withcup coverage at the time of the operation requires medializa-tion or superior displacement of the acetabular center of rota-tion. The center can be medialized by as much as 7.5 mm or
displaced superiorly by as much as 13 mm without clinicalconsequences46,48. Moving the center of rotation in and/or upresults in cup coverage that prevents metal neck-on-cup im-pingement, but it can reduce the length and offset of the hip,causing bone-on-bone impingement. The solutions for theseproblems are a higher osseous femoral neck cut, a longer mod-ular head, a high-offset stem, or a combination of these21-23.
Recent research has increased our awareness of the sur-geon’s inability to control anteversion of a cementless femoralstem. The inflexibility of the position of the cementless stemwas suggested by D’Lima et al.40, in their finite-element study. Infact, this makes intuitive sense because a cementless stem musthave a tight fit in the bone. The femur has variable anteversionof the neck and variable anterior diaphyseal bowing, both ofwhich influence the anteversion of the prosthetic neck in rela-tion to the femoral axis76. The wide range of femoral stem ver-sion was confirmed by Wines and McNicol49 with use ofpostoperative computed tomography scans. They found a rangeof 15° of retroversion to 45° of anteversion with a mean of 16.8°of femoral anteversion. A similar mean of 16.5°, with a range of30° of retroversion to 37° of anteversion, was observed by Pier-chon et al.31, also with computed tomography scans, in theirstudy of cemented stems. These two studies emphasized that thesurgeon did not control the femoral stem, even when it wasfixed with cement, as well as had been thought. One of us(L.D.D.) and colleagues77 used imageless computer navigationand found a mean of 5° of anteversion of the femoral stem inmen, a mean of 9° in women, and a mean of 7° in the entiregroup. This anteversion was close to the mean of 9.8° found byMaruyama et al.76 when they measured intact cadaver femora.
A second factor that influences the anteversion of theprosthetic stem relative to the femur is the anterior bow of thefemoral diaphysis, which can be as much as 10°76. The morethe femur is bowed anteriorly, the less the relative anteversionof the prosthetic stem in relation to the femur. This has agreater effect on cementless straight stems than on cementlessanatomic stems, which compensate somewhat by fitting theanteversion of the metaphysis.
The concept of combined anteversion of the stem andcup has been emphasized by Ranawat. He has taught a manualcombined anteversion test for total hip replacement since theearly 1990s78. With the cup and stem in place, the lower limb ispositioned in neutral (or slight hip flexion) and is internally ro-tated until the femoral head is symmetrically seated (coplanar)in the cup. The amount of internal rotation in degrees neededto produce a coplanar head and cup is the combined ante-version78. Ranawat and Maynard recommended a combined an-teversion of approximately 45° in female patients and 20° to 30°in male patients79. McKibbin defined the stability index for ana-tomic hips to be 30° to 40°, with a range of 20° to 35° for menand 30° to 45° for women80. A combined anteversion of <20°was defined as severe retroversion. Barrack21 indirectly ad-dressed combined anteversion by recommending cup antever-sion of 15° when stem anteversion is 15°, but he recommendedan increase in cup anteversion if stem anteversion is <15°. Wid-mer and Zurfluh44 stated that combined anteversion could be
A
Dorr_CCR.fm Page 1838 Wednesday, July 11, 2007 2:05 PM

1839
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
determined by the formula: cup anteversion + (0.7 × stem an-teversion) = 37.3° (for example, femoral anteversion of 10° ×0.7 = 7°, so cup anteversion should be 30°). Finally, Komeno etal.81 used computed tomography scans to compare twenty dislo-cated hips with eighteen nondislocated hips in Japanese pa-tients. The mean combined anteversion was 47.8° in the hipswithout a dislocation, 27.4° in the hips with a posterior disloca-tion, and 72.2° in those with an anterior dislocation. Thesenumbers are higher than those reported for non-Japanese pa-tients because femoral anteversion is greater in Japanese pa-tients, in whom dysplasia is the most common reason for totalhip replacement. In both cases (posteriorly and anteriorly dislo-cated hips) the combined anteversion was significantly differentfrom that of the hips without dislocation (p = 0.0074 for theposteriorly dislocated group and p = 0.0056 for the anteriorlydislocated group). Komeno et al. concluded that the dislocationrate is not affected by the positioning of either the cup or thestem alone but is influenced by the combined anteversion.
Combined anteversion is also an important factor insurface replacement. McMinn82 stated that excessive antever-sion of the femoral neck, such as with developmental dysplasiaof the hip, can cause impingement on, and edge loading, in anoptimally positioned cup. His target was a combined antever-sion of 45°, so that if the femoral neck is in 40° of anteversionthe cup is placed in 5° of anteversion. McMinn recommendeda derotation femoral osteotomy if the osseous femoral ante-version is ≥60°.
Biomechanical Hip ReconstructionCorrect hip length and offset are both necessary to avoid im-pingement. Femoral reconstruction controls the biomechani-cal reconstruction because the level of the femoral neck cutand the head length that are used determine the hip lengthand offset (and the resting length of the muscles). Charles etal.22 studied the effect of soft-tissue balancing of the hip. If thecup position does not change the hip center of rotation by >5to 6 mm medially or superiorly, the templated femoral neckcut will reestablish the limb length and offset. If the cup is ex-cessively medialized or the angle between the osseous neckand the shaft is ≤125°, an offset femoral stem is needed to re-produce offset without lengthening of the limb22,23.
The correctness of the reconstruction of the hip lengthand offset can be anatomically evaluated intraoperatively (Fig.5). The lesser trochanter should not touch the ischium with thelower limb in full extension; it should be proximal to the tip ofthe ischium by at least one fingerbreadth (the proper relation-ship can be determined from the preoperative radiograph if anearly normal contralateral hip is available for imaging). Thegreater trochanter should not touch the ilium in external rota-tion and abduction, or in flexion, adduction, and internal rota-tion. All anterior acetabular osteophytes must be removed. Themetal femoral neck should not touch the rim of the cup at theextremes of motion21,43. Impingement commonly occurs in hipswith low anteversion of a cementless femoral stem (≤5°) andhips with a low offset, and the anterosuperior aspect of the cap-sule and even the distal side of the anterior inferior iliac spine
may need to be removed from these hips30,48. In flexible womenand in hips with low femoral anteversion, impingement may beavoided only with the use of a large femoral head.
Femoral stems with a modular neck could allow optimi-zation of limb length and offset as well as control of femoralversion and varus or valgus angulation of the neck. However,to our knowledge, there are no published data to corroboratethese theoretical advantages. Furthermore, a new interfacemay be a source of wear and dissociation between the neckand the metaphyseal component, which was recently reportedafter the use of one modular neck design83.
In hip resurfacing, there is little flexibility to adjust limblength and offset if the cup is excessively medialized or placedsuperiorly. Therefore, the cup center of rotation must be re-produced and the proximal femoral reconstruction shouldmaintain the prosthetic center of rotation as near to the ana-tomic femoral center of rotation as possible67. Anterior femo-ral neck osteophytes must be carefully resected to reduce therisk of anterior cam impingement postoperatively. A trochan-teric osteotomy with trochanteric advancement is anothermethod of increasing clearance.
Large HeadsLarge femoral heads of ≥36 mm effectively solve the problem ofhow to achieve a correct head-neck ratio. This head size pro-vides a head-neck ratio of >2.0 even when a 14 to 16-mm taperneck with a 16-mm thickness at the base of the taper is used.However, the use of large heads has created a separate set oftechnical limitations and concerns. For example, the cup posi-tion with hard-on-hard surfaces is even more important thanthat with metal-on-polyethylene surfaces. With metal-on-metalarticulations, cup inclination of >50° can cause edge loading ofthe femoral head on the cup and result in so-called runawaywear; with ceramic-on-ceramic articulations, this cup positioncan cause fracture or squeaking84. The use of metal-on-metal ac-etabular components for surface replacement or for conven-tional total hip replacement with a large head has reducedacetabular sector angles to 159.2° (Birmingham implant; Smithand Nephew) and 165° (ASR; DePuy, Warsaw, Indiana, andDurom, Zimmer) and requires nearly complete coverage of thecup, which can promote inclination in excess of 50°. Prepara-tion of the acetabular bone must be adjusted for the 159° to165° cups to allow coverage with inclination of <45°. Techni-cally, this preparation is more difficult because the acetabularpreparation is done with reamers that have a 180° angle. Ream-ing medially must be adequate to achieve coverage and correctinclination, but it must be limited to ensure Zone-2 contact forthese 159° to 165° cups with a flattened dome85.
Highly cross-linked polyethylene has allowed routineimplantation of femoral heads of ≥36 mm in diameter. Labo-ratory studies have shown no increase in wear86. Our unpub-lished results of use of a 38-mm cobalt-chromium headarticulating with Durasul highly cross-linked polyethylene(Zimmer) showed a linear wear rate of 0.026 mm/yr at threeto four years postoperatively, which does not differ from ourpublished five-year linear wear rate of 0.029 mm/yr following
Dorr_CCR.fm Page 1839 Wednesday, July 11, 2007 2:05 PM

1840
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
the use of 28-mm cobalt-chromium heads articulating withDurasul polyethylene87. Volumetric wear with 38 and 44-mmheads (28.1 ± 19 mm3/yr) is greater than that with 32-mmheads (18.2 ± 9.7 mm3/yr, p = 0.021). This volumetric wear re-mains well below the 87 mm3/yr threshold for osteolysis88. Ifcups with highly crossed-linked polyethylene are abducted>55°, there is the threat of breakage89.
Techniques for Avoiding Impingementrthopaedic surgeons can agree about the benefits of theimplant design changes made in the last decade to avoid
impingement: elimination of skirts on femoral heads15, cham-fering of the polyethylene rim37, narrow femoral necks8, largefemoral heads35, and perhaps modular femoral necks83. Thereremains uncertainty about the best technical methods forminimizing neck-on-cup and/or bone-on-bone impingementin conventional total hip replacements.
The primary question for surgeons is what constitutesthe so-called safe zone for the cup. The most often used safezone is 5° to 25°, as described by Lewinnek et al.75. McCollumand Gray36 recommended 20° to 40°. Surgeons who use the an-terior approach for arthroplasty have always recommendedless cup anteversion. Charnley71 suggested little or no antever-sion, and Müller72 and Coventry et al.73 suggested 10°. Sur-geons who use the anterior approach, especially with thepatient in the supine position, may judge the position of thecup with use of Murray’s anatomic plane, whereas those whoapproach the hip posteriorly, with the patient in a lateral posi-tion, view the radiographic angle, which may explain some ofthe differences between target values90.
The concept of using combined anteversion, rather thantarget values, to determine the cup position when mating itwith the stem is becoming more prevalent 40,44,48,82,91. With a ce-mented stem in 10° to 15° of anteversion, the cup should beplaced within a “safe zone” of 25° ± 10° so that the combinedanteversion is 25° to 35° for men and 35° to 45° for women(on the basis of Murray’s radiographic plane values)44,79,80. Thecombined anteversion should be the same for both the ante-rior and the posterior approach, being that the same Murraydefinition is used, because wear and durability are related toavoidance of impingement18-20,52,56,58,90.
Total hip replacement with a cemented stem allows a safezone of targeted cup position because the position of the femo-ral stem is adjustable. However, the position of a cementlessfemoral stem in a total hip replacement is nearly fixed, so thecup position must be adjustable40,44,48,91. The surgeon must deter-mine the femoral anteversion with a trial stem before position-ing the cup, which means that the femoral preparation must becompleted prior to the acetabular preparation. The stem ante-version can be judged against the axis of the thigh by aligningthe thigh according to the epicondyles of the knee. This requiresthat the surgeon accept a change in the sequence in which he orshe performs the operation. The advantage of this technique isthe wide range of femoral version that is possible (15° of retro-version to 45° of anteversion)49. In our experience with cement-less femoral stems, the range has been 15° of retroversion to 30°
of anteversion and the surgeon, on the average, can correctly es-timate the femoral version to within 5°. However, this margin oferror for the surgeon’s estimation of the stem version still resultsin better precision for hip reconstruction than an assumption of10° to 15° of femoral anteversion for every case.
The acetabular cup, when used with a cementless femo-ral stem, should be positioned in relation to the stem positionrather than on the basis of a target value. This is necessary be-cause, if femoral anteversion is low (5° of anteversion to 5° ofretroversion), positioning a cup in 20° will increase the risk ofposterior dislocation; if the femoral anteversion is high (25° to30° of anteversion), a cup positioned in 20° will be at risk foranterior dislocation, especially if a posterior hood is used. Cupanteversion needs to be correctly mated to the stem antever-sion, and in our experience such cup anteversion ranges from10° to 15° in women with hip dysplasia to 30° to 35° in menwith a pistol-grip deformity. A safe zone for a cup used with acementless stem is not a realistic concept because the stem an-teversion cannot be controlled.
The safe zone for inclination is <45°. We consider the opti-mum cup inclination to be 40° as this allows a margin of error ofup to 5° for surgical placement, which would maximize cup in-clination at 45°. The lower limit of inclination is commonly set at30° because of the limitation of coverage of the superior metalwithout excessive medialization or superior displacement, whichwould decrease the offset of the hip and substantially increasethe risk of bone-on-bone impingement. If medialization or su-perior displacement does decrease the offset of the hip, the solu-tion is to use a higher femoral neck cut, a longer modular head,an offset stem, or a combination of these21-23.
The use of a large femoral head ensures an acceptablehead-neck ratio, even with a circular femoral neck. The largehead provides a margin of error of combined anteversion forstability, but it may not reduce the margin of error for wear,which requires inclination of ≤45° and is related to the com-bined anteversion (the higher the acetabular anteversion, theless the wear)42.
The improvement in articulation surfaces has raisedconfidence about increasing the durability of total hip replace-ment87. Impingement must still be avoided to fulfill theseexpectations, so research has continued with increased in-terest3,15,18,19,21,35,37,39,44,56,63,64,67,68,81,92-96. Computer navigation has im-proved the accuracy of component positioning97,98. Navigationprovides a scientific method for total hip reconstruction withnumerical confirmation of the combined anteversion and cupinclination of ≤45°. Studies involving computer navigationhave suggested the benefits of using a combined anteversiontechnique, rather than target values, for determining cup posi-tion, since femoral stem anteversion is known48,77.
Aamer Malik, MDAditya Maheshwari, MDLawrence D. Dorr, MDThe Arthritis Institute, 501 East Hardy Street, 3rd Floor, Inglewood, CA 90301. E-mail address for L.D. Dorr: [email protected]
O
Dorr_CCR.fm Page 1840 Wednesday, July 11, 2007 2:05 PM

1841
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
References
1. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012-8.
2. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip: a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83:1119-24.
3. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroaceta-bular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112-20.
4. Leunig M, Beck M, Dora C, Ganz R. [Femoroacetabular impingement: trigger for the development of coxarthrosis]. Orthopade. 2006;35:77-84. German.
5. Siebenrock KA, Kalbermatten DF, Ganz R. Effect of pelvic tilt on acetabular ret-roversion: a study of pelves from cadavers. Clin Orthop Relat Res. 2003;407:241-8.
6. Bartz RL, Nobel PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82:1300-7.
7. Krushell RJ, Burke DW, Harris WH. Range of motion in contemporary total hip arthroplasty. The impact of modular head-neck components. J Arthroplasty. 1991;6:97-101.
8. Barrack RL, Butler RA, Laster DR, Andrews P. Stem design and dislocation after revision total hip arthroplasty: clinical results and computer modeling. J Arthro-plasty. 2001;16(8 Suppl 1):8-12.
9. Hedlundh U, Carlsson AS. Increased risk of dislocation with collar reinforced modular heads of the Lubinus SP-2 hip prosthesis. Acta Orthop Scand. 1996;67:204-5.
10. Urquhart AG, D’Lima DD, Venn-Watson E, Colwell CW Jr, Walker RH. Polyethyl-ene wear after total hip arthroplasty: the effect of a modular femoral head with an extended flange-reinforced neck. J Bone Joint Surg Am. 1998;80:1641-7.
11. Berend KR, Lombardi AV Jr, Mallory TH, Adams JB, Russell JH, Groseth KL. The long-term outcome of 755 consecutive constrained acetabular components in total hip arthroplasty examining the successes and failures. J Arthroplasty. 2005;20(7 Suppl 3):93-102.
12. Earll M, Fehring T, Griffin WL, Mason JB, McCoy TH. Early osteolysis associ-ated with trunion-liner impingement. Clin Orthop Relat Res. 2004;418:153-6.
13. Kelley SS, Lachiewicz PF, Hickman JM, Paterno SM. Relationship of femoral head and acetabular size to the prevalence of dislocation. Clin Orthop Relat Res. 1998;355:163-70.
14. Dorr LD, Wan Z. Causes of and treatment protocol for instability of total hip replacement. Clin Orthop Relat Res. 1998;355:144-51.
15. Padgett DE, Lipman J, Robie B, Nestor BJ. Influence of total hip design on dislocation: a computer model and clinical analysis. Clin Orthop Relat Res. 2006;447:48-52.
16. Hall RM, Siney P, Unsworth A, Wroblewski BM. Prevalence of impingement in explanted Charnley acetabular components. J Orthop Sci. 1998;3:204-8.
17. Isaac GH, Wroblewski BM, Atkinson JR, Dowson D. A tribological study of re-trieved hip prostheses. Clin Orthop Relat Res. 1992;276:115-25.
18. Shon WY, Baldini T, Peterson MG, Wright TM, Salvati EA. Impingement in to-tal hip arthroplasty: a study of retrieved acetabular components. J Arthroplasty. 2005;20:427-35.
19. Usrey MM, Noble PC, Rudner LJ, Conditt MA, Birman MV, Santore RF, Mathis KB. Does neck/liner impingement increase wear of ultrahigh-molecular-weight polyethylene liners? J Arthroplasty. 2006;21(6 Suppl 2):65-71.
20. Yamaguchi M, Akisue T, Bauer TW, Hashimoto Y. The spatial location of impingement in total hip arthroplasty. J Arthroplasty. 2000;15:305-13.
21. Barrack RL. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg. 2003;11:89-99.
22. Charles MN, Bourne RB, Davey JR, Greenwald AS, Morrey BF, Rorabeck CH. Soft-tissue balancing of the hip: the role of femoral offset restoration. Instr Course Lect. 2005;54:131-41.
23. Danesh-Clough T, Bourne RB, Rorabeck CH, McCalden R. The mid-term re-sults of a dual offset uncemented stem for total hip arthroplasty. J Arthroplasty. 2007;22:195-203.
24. D’Lima DD, Chen PC, Colwell CW Jr. Optimizing acetabular component posi-tion to minimize impingement and reduce contact stress. J Bone Joint Surg Am. 2001;83 Suppl 2:87-91.
25. Maxian TA, Brown TD, Pederson DR, Callaghan JJ. Finite element modeling of dislocation propensity in total hip arthroplasty. Orthop Trans. 1996;20:647-8.
26. Cobb TK, Morrey BF, Ilstrup DM. Effect of the elevated-rim acetabular liner on loosening after total hip arthroplasty. J Bone Joint Surg Am. 1997;79:1361-4.
27. Murray DW. Impingement and loosening of the long posterior wall acetabular implant. J Bone Joint Surg Br. 1992;74:377-9.
28. Johnston RC, Brand RA, Crowninshield RD. Reconstruction of the hip. A math-ematical approach to determine optimum geometric relationships. J Bone Joint Surg Am. 1979;61:639-52.
29. Yoder SA, Brand RA, Pedersen DR, O’Gorman TW. Total hip acetabular compo-nent position affects component loosening rates. Clin Orthop Relat Res. 1988;228:79-87.
30. Padgett DE, Warashina H. The unstable total hip replacement. Clin Orthop Relat Res. 2004;420:72-9.
31. Pierchon F, Pasquier G, Cotten A, Fontaine C, Clarisse J, Duquennoy A. Causes of dislocation of total hip arthroplasty. CT study of component alignment. J Bone Joint Surg Br. 1994;76:45-8.
32. Bourne RB, Rorabeck CH. Soft tissue balancing: the hip. J Arthroplasty. 2002;17(4 Suppl 1):17-22.
33. Davey JR, O’Connor DO, Burke DW, Harris WH. Femoral component offset. Its effect on strain in bone-cement. J Arthroplasty. 1993;8:23-6.
34. Beaulé PE, Schmalzried TP, Udomkiat P, Amstutz HC. Jumbo femoral head for the treatment of recurrent dislocation following total hip replacement. J Bone Joint Surg Am. 2002;84:256-63.
35. Geller JA, Malchau H, Bragdon C, Greene M, Harris WH, Freiberg AA. Large di-ameter femoral heads on highly cross-linked polyethylene: minimum 3-year re-sults. Clin Orthop Relat Res. 2006;447:53-9.
36. McCollum DE, Gray WJ. Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop Relat Res. 1990;261:159-70.
37. Barrack RL, Lavernia C, Ries M, Thornberry R, Tozakoglou E. Virtual reality computer animation of the effect of component position and design on stability after total hip arthroplasty. Orthop Clin North Am. 2001;32:569-77, vii.
38. Callaghan JJ, Brown TD, Pedersen DR, Johnston RC. Choices and compro-mises in the use of small head sizes in total hip arthroplasty. Clin Orthop Relat Res. 2002;405:144-9.
39. Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR. Bio-mechanics of large femoral heads: what they do and don’t do. Clin Orthop Relat Res. 2004;429:102-7.
40. D’Lima DD, Urquhart AG, Buehler KO, Walker RH, Colwell CW Jr. The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. J Bone Joint Surg Am. 2000;82:315-21.
41. Patil S, Bergula A, Chen PC, Colwell CW Jr, D’Lima DD. Polyethylene wear and acetabular component orientation. J Bone Joint Surg Am. 2003;85 Suppl 4:56-63.
42. Robinson RP, Simonian PT, Gradisar IM, Ching RP. Joint motion and surface contact area related to component position in total hip arthroplasty. J Bone Joint Surg Br. 1997;79:140-6.
43. Scifert CF, Brown TD, Pedersen DR, Callaghan JJ. A finite element analysis of factors influencing total hip dislocation. Clin Orthop Relat Res. 1998;355:152-62.
44. Widmer KH, Zurfluh B. Compliant positioning of total hip components for opti-mal range of motion. J Orthop Res. 2004;22:815-21.
45. Kummer FJ, Shah S, Iyer S, DiCesare PE. The effect of acetabular cup orien-tations on limiting hip rotation. J Arthroplasty. 1999;14:509-13.
46. Karachalios T, Hartofilakidis G, Zacharakis N, Tsekoura M. A 12- to 18-year radiographic follow-up study of Charnley low-friction arthroplasty. The role of the center of rotation. Clin Orthop Relat Res. 1993;296:140-7.
47. Sarmiento A, Ebramzadeh E, Gogan WJ, McKellop HA. Cup containment and orientation in cemented total hip arthroplasties. J Bone Joint Surg Br. 1990;72:996-1002.
48. Dorr LD. Hip arthroplasty: minimally invasive techniques and computer navi-gation. Philadelphia: Saunders; 2005.
49. Wines AP, McNicol D. Computed tomography measurement of the accuracy of component version in total hip arthroplasty. J Arthroplasty. 2006;21:696-701.
50. Brien WW, Salvati EA, Wright TM, Burstein AH. Dislocation following THA: com-parison of two acetabular component designs. Orthopedics. 1993;16:869-72.
Dorr_CCR.fm Page 1841 Wednesday, July 11, 2007 2:05 PM

1842
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B E R 8 · AUG U S T 2007IM PI N GE M E N T W I TH TOT A L HIP RE P LA CE M E N T
51. Cobb TK, Morrey BF, Ilstrup DM. The elevated-rim acetabular liner in total hip arthroplasty: relationship to postoperative dislocation. J Bone Joint Surg Am. 1996;78:80-6.
52. Dorr LD, Hilton KR, Wan Z, Markovich GD, Bloebaum R. Modern metal on metal articulation for total hip replacements. Clin Orthop Relat Res. 1996;333:108-17.
53. Trousdale RT, Cabanela ME, Berry DJ. Anterior iliopsoas impingement after total hip arthroplasty. J Arthroplasty. 1995;10:546-9.
54. Heaton K, Dorr LD. Surgical release of iliopsoas tendon for groin pain after total hip arthroplasty. J Arthroplasty. 2002;17:779-81.
55. Ala Eddine T, Remy F, Chantelot C, Giraud F, Migaud H, Duquennoy A. [Anterior iliopsoas impingement after total hip arthroplasty: diagnosis and conservative treatment in 9 cases]. Rev Chir Orthop Reparatrice Appar Mot. 2001;87:815-9. French.
56. Birman MV, Noble PC, Conditt MA, Li S, Mathis KB. Cracking and impinge-ment in ultra-high-molecular-weight polyethylene acetabular liners. J Arthroplasty. 2005;20(7 Suppl 3):87-92.
57. Kurtz SM, Hozack WJ, Purtill JJ, Marcolongo M, Kraay MJ, Goldberg VM, Sharkey PF, Parvizi J, Rimnac CM, Edidin AA. Significance of in vivo degrada-tion for polyethylene in total hip arthroplasty. Clin Orthop Relat Res. 2006;453:47-57.
58. Kligman M, Furman BD, Padgett DE, Wright TM. Impingement contributes to backside wear and screw-metallic shell fretting in modular acetabular cups. J Ar-throplasty. 2007;22:258-64.
59. Bosco JA, Benjamin JB. Loosening of a femoral stem associated with the use of an extended-lip acetabular cup liner. A case report. J Arthroplasty. 1993;8:91-3.
60. Messieh M, Mattingly DA, Turner RH, Scott R, Fox J, Slater J. Wear debris from bipolar femoral neck-cup impingement. A cause of femoral stem loosening. J Arthroplasty. 1994;9:89-93.
61. Kobayashi S, Takaoka K, Tsukada A, Ueno M. Polyethylene wear from femoral bipolar neck-cup impingement as a cause of femoral prosthetic loosening. Arch Orthop Trauma Surg. 1998;117:390-1.
62. Dobzyniak M, Fehring TK, Odum S. Early failure in total hip arthroplasty. Clin Orthop Relat Res. 2006;447:76-8.
63. Ha YC, Kim SY, Kim HJ, Yoo JJ, Koo KH. Ceramic liner fracture after cement-less alumina-on-alumina total hip arthroplasty. Clin Orthop Relat Res. 2007;458:106-10.
64. Toran MM, Cuenca J, Martinez AA, Herrera A, Thomas JV. Fracture of a ce-ramic femoral head after ceramic-on-ceramic total hip arthroplasty. J Arthroplasty. 2006;21:1072-3.
65. Iida H, Kaneda E, Takada H, Uchida K, Kawanabe K, Nakamura T. Metallosis due to impingement between the socket and the femoral neck in a metal-on-metal bearing total hip prosthesis. A case report. J Bone Joint Surg Am. 1999;81:400-3.
66. Howie DW, McGee MA, Costi K, Graves SE. Metal-on-metal resurfacing versus total hip replacement—the value of a randomized clinical trial. Orthop Clin North Am. 2005;36:195-201, ix.
67. Beaulé PE, Harvey N, Zaragoza E, Le Duff MJ, Dorey FJ. The femoral head/neck offset and hip resurfacing. J Bone Joint Surg Br. 2007;89:9-15.
68. Howie DW, McCalden RW, Nawana NS, Costi K, Pearcy MJ, Subramanian C. The long-term wear of retrieved McKee-Farrar metal-on-metal total hip prostheses. J Arthroplasty. 2005;20:350-7.
69. Wiadrowski TP, McGee M, Cornish BL, Howie DW. Peripheral wear of Wagner resurfacing hip arthroplasty acetabular components. J Arthroplasty. 1991;6:103-7.
70. Amstutz HC, Antoniades JT, Le Duff MJ. Results of metal-on-metal hybrid hip resurfacing for Crowe type-I and II developmental dysplasia. J Bone Joint Surg Am. 2007;89:339-46.
71. Charnley J. Total hip replacement by low-friction arthroplasty. Clin Orthop Relat Res. 1970;72:7-21.
72. Müller ME. Total hip prostheses. Clin Orthop Relat Res. 1970;72:46-68.
73. Coventry MB, Beckenbaugh RD, Nolan DR, Ilstrup DM. 2,012 total hip arthro-plasties. A study of postoperative course and early complications. J Bone Joint Surg Am. 1974;56:273-84.
74. Harris WH. Advances in surgical technique for total hip replacement: with-out and with osteotomy of the greater trochanter. Clin Orthop Relat Res. 1980;146:188-204.
75. Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60:217-20.
76. Maruyama M, Feinberg JR, Capello WN, D’Antonio JA. Morphologic features of the acetabulum and femur: anteversion angle and implant positioning. Clin Orthop Relat Res. 2001;393:52-65.
77. Dorr LD. Long WT, Inaba Y, Sirianni LE, Boutary M. MIS total hip replacement with a single posterior approach. Semin Arthroplasty. 2005;16:179-85.
78. Lucas DH, Scott RD. The Ranawat sign. A specific maneuver to assess com-ponent positioning in total hip arthroplasty. J Orthop Tech. 1994;2:59-61.
79. Ranawat CS, Maynard MJ. Modern techniques of cemented total hip arthro-plasty. Tech Orthop. 1991;6:17-25.
80. McKibbin B. Anatomical factors in the stability of the hip joint in the newborn. J Bone Joint Surg Br. 1970;52:148-59.
81. Komeno M, Hasegawa M, Sudo A, Uchida A. Computed tomographic evalua-tion of component position on dislocation after total hip arthroplasty. Orthope-dics. 2006;29:1104-8.
82. McMinn D. Hip resurfacing video techniques: BMHR Dysplasia 2006. http://www.mcminncentre.co.uk
83. Sporer SM, DellaValle C, Jacobs J, Wimmer M. A case of disassociation of a modular femoral neck trunion after total hip arthroplasty. J Arthroplasty. 2006;21:918-21.
84. Restrepo C, Parvizi J, Purtill JJ, Sharkey P, Hozack W, Rothman R. Noisy ceramic hip: is component malpositioning the problem? Read at the Annual Meeting of the American Association of Hip and Knee Surgeons, 2006 Nov 3-5; Dallas, TX.
85. DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976;121:20-32.
86. Muratoglu OK, Wannomae K, Christensen S, Rubash HE, Harris WH. Ex vivo wear of conventional and cross-linked polyethylene acetabular liners. Clin Orthop Relat Res. 2005;438:158-64.
87. Dorr LD, Wan Z, Shahrdar C, Sirianni L, Boutary M, Yun A. Clinical perfor-mance of a Durasul highly cross-linked polyethylene acetabular liner for total hip arthroplasty at five years. J Bone Joint Surg Am. 2005;87:1816-21.
88. Wan Z, Dorr LD. Natural history of femoral focal osteolysis with proximal in-growth smooth stem implant. J Arthroplasty. 1996;11:718-25.
89. Halley D, Glassman A, Crowninshield RD. Recurrent dislocation after revision total hip replacement with a large prosthetic femoral head. A case report. J Bone Joint Surg Am. 2004;86:827-30.
90. Murray DW. The definition and measurement of acetabular orientation. J Bone Joint Surg Br. 1993;75:228-32.
91. Dorr LD. Computer navigation for total hip replacement. Op Tech Orthop. 2006;16:112-9.
92. Clohisy JC, McClure JT. Treatment of anterior femoroacetabular impingement with combined hip arthroscopy and limited anterior decompression. Iowa Orthop J. 2005;25:164-71.
93. Mardones RM, Gonzalez C, Chen Q, Zobitz M, Kaufman KR, Trousdale RT. Surgical treatment of femoroacetabular impingement: evaluation of the effect of the size of the resection. Surgical technique. J Bone Joint Surg Am. 2006;88 Suppl 1 (Pt1):84-91.
94. Murphy S, Tannast M, Kim YJ, Buly R, Millis MB. Debridement of the adult hip for femoroacetabular impingement: indications and preliminary clinical results. Clin Orthop Relat Res. 2004;429:178-81.
95. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoro-acetabular impinge-ment due to acetabular retroversion. Treatment with periacetabular osteotomy. J Bone Joint Surg Am. 2003;85:278-86.
96. Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res. 2004;429:170-7.
97. DiGioia AM, Jaramaz B, Blackwell M, Simon DA, Morgan F, Moody JE, Nikou C, Colgan BD, Aston CA, Labarca RS, Kischell E, Kanade T. Image guided navigation system to measure intraoperatively acetabular implant alignment. Clin Orthop Relat Res. 1998;355:8-22.
98. Kalteis T, Handel M, Bathis H, Perlick L, Tingart M, Grifka J. Imageless navigation for insertion of the acetabular component in total hip arthro-plasty: is it as accurate as CT-based navigation? J Bone Joint Surg Br. 2006;88:163-7.
Dorr_CCR.fm Page 1842 Wednesday, July 11, 2007 2:05 PM