Embed Size (px)
Citation preview

21
*Professor, University of Iowa Hospitals and Clinics, Hospital Dentistry Institute, Division of Maxillofacial Prosthodontics, 200 Hawkins Drive, Iowa City, IA 52242-1049
Implant Replacement of the Maxillary CentralIncisor Utilizing a Modified Ceramic Abutment(Thommen SPI ART) and Ceramic Restoration
ROBERT SCHNEIDER, DDS, MS*
ABSTRACTThe prosthetic restoration of a missing anterior tooth with a dental implant is a challenge. Treat-ment coordination with a multidisciplinary team is critical in the successful outcome of this typeof patient treatment. Newer surgical treatment modalities in the management of hard and softtissues are becoming common, with very good predictability and long-term stability. Addition-ally, the use of advanced dental technology and materials such as sintered zirconium allows therestorative practitioner the opportunity to fabricate an esthetic, precise-fitting, biocompatible,and strong definitive prosthesis for the patient, with good longevity.
CLINICAL SIGNIFICANCEThe use of an all-ceramic abutment and restoration is described, along with the “soft tissuesculpting” procedure through the use of a custom provisional restoration. The relative ease andconvenience of the procedure is also illustrated.
(J Esthet Restor Dent 20:21–28, 2008)
I N T R O D U C T I O N
The utilization of dentalimplants to replace single or
multiple missing teeth or entireedentulous arches has become com-mon in today’s prosthodontic andsurgical practices around theworld.1–4 Relatively recent advancesin implant dentistry allow practi-tioners the option to consider theextraction of a nonrestorable toothand the immediate placement of the implant, along with immediateprovisionalization. These
improvements in technique have ledto more predictable development ofacceptable emergence profiles,which is of obvious primary importance in the esthetic zone.5–7
Development of an appropriateemergence profile by the restorativedoctor, and also the laboratorytechnician, is paramount in themaintenance of long-term, peri-odontally sound oral health by supporting the soft tissues in anoptimal position and contour. Inaddition to optimal periodontal
health, a predictable long-termesthetic outcome is more easily achieved.
Today’s implant systems presentvery good long-term success levelsas well as several advantages overthe traditional fixed and removabletreatment alternatives in manycases. Additionally, single-implantrestorations are not without chal-lenge in the esthetic zone. Achieve-ment and maintenance of propergingival architecture caused by the
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N GDOI 10.1111/j.1708-8240.2008.00144.x V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8

22
I M P L A N T R E P L A C E M E N T U S I N G A N A L L - C E R A M I C A B U T M E N T A N D R E S T O R A T I O N
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
changes that take place in the alve-olar bone following tooth extrac-tion and the resultant apicalmigration of the patient’s gingivaltissues are a serious concern.
Recent development of new dentalmaterials have allowed the restora-tive doctor and dental technician tofacilitate the maintenance of theseconditions to improve the long-term esthetics for the patient. Mostrecently, the use of ceramic or zirco-nia abutments for implant systemshave helped improve their estheticcapabilities. The zirconia abutmenthas physical properties that, whenproperly utilized, can withstandroutine occlusal forces in the ante-rior portion of the mouth.8 The zirconia abutment can lead to amore natural-appearing implantrestoration, with no metal showingthrough or darkening of the soft tis-sue, and can adequately supportand retain an all-ceramic crown.
Although ceramic materials arevery strong in compressive strength,they have a tendency to becomeweak in tensile strength. In somepatients, these types of forces areexerted during chewing and para-function. Also, because of theextreme hardness of the ceramicmaterials utilized for these abut-ments, great care must be exercisedduring their preparation in the laboratory so as not to developGriffith’s flaws or stress cracks inthe material that could lead to catastrophic failure under minimalocclusal forces. The screw-retentionaccess hole in the ceramic abut-ments is a concern because if theexternal walls are prepared beyondthe manufacturer’s minimum speci-fications, catastrophic failure underfunction can be expected.
Another observed advantage of theall-ceramic abutments and restora-tions are that they seem to be very
kind to the periodontium and pro-mote good tissue health, even in thecase of suboptimal oral hygiene,compared with traditional ceramometal restorations.9
This article will review a techniquefor the utilization of a zirconiaceramic abutment, in addition toprovisionalization, to develop softtissue contours in an 18-year-oldmale patient.
P A T I E N T T R E A T M E N T
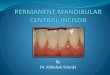
The maxillary left central incisorhad experienced trauma severalyears before, had been treatedendodontically, and has now exhib-ited nonrestorable internal rootresorption (Figure 1). The patientpresented with suboptimal oralhygiene, which was addressed withoral hygiene instructions and oraland written information on the needto improve hygiene and the poten-tially deleterious effects that this
A B
Figure 1. A, Patient’s condition at initial appointment. B, Initial periapical radiograph ofthe tooth with internal resorption.

S C H N E I D E R
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 23
may have on the long-term outcomeof the restoration/implant complex.The tooth was atraumaticallyextracted, and a 5.0-mm-diameterSwiss Precision Implant (SPI), Element type implant was placed(Thommen Medical, Cleveland,OH, USA), utilizing a surgicalguide. A healing cap was placed andthe soft tissue allowed to mature for6 weeks. During the healing period,
the patient wore a provisionalremovable partial denture.
At the 6-week healing period, thefinal impression was made at theimplant level. Following the finalimpression at the implant level, anEASY abutment (Thommen Med-ical) was placed to facilitate thefabrication of the provisional forfurther soft tissue contouring
(Figure 2). A PMMA provisionalcomponent made for the EASYabutment (Thommen Medical) wasutilized as the substructure to maintain marginal integrity andadaptation to the abutment. A thermoplastic matrix made fromthe patient’s diagnostic casts preex-traction was utilized to form theprovisional restoration utilizing aPMMA material (Figures 3–7). The
Figure 2. Healing at 6 weeks, and the EASY abutment inplace to retain provisional restoration.
Figure 3. Thermoplastic matrix made from the diagnosticcast before the tooth was extracted.
Figure 4. Provisional components made from PEEK plastic(tan), primarily for use in the posterior area, and PMMA(white) for the fabrication of custom acrylic resin provisionals.
Figure 5. Initial appearance of the provisional followingremoval from the mouth.

24
I M P L A N T R E P L A C E M E N T U S I N G A N A L L - C E R A M I C A B U T M E N T A N D R E S T O R A T I O N
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
optimal emergence profile wasachieved by the further addition ofPMMA following the removal ofthe provisional from the patient’smouth, smoothed, polished, andcemented with a provisional cement(Figure 8).
The laboratory analog was attachedto the impression coping and the
master cast poured in high-strength,low-expansion die stone. It wasdetermined, utilizing the thermo-plastic matrix on the master cast,that the zirconia ART EASY abut-ment (Thommen Medical) wouldrequire some modification/reduction to obtain optimal room for the final all-ceramiccemented restoration.
Marking the ART abutment on themaster cast, the areas of reductionwere identified and very carefullyreduced using abrasive rotaryinstruments in the laboratory, withvery light pressure and copiousamounts of irrigation so as to notbuild up heat and create microfrac-tures in the ceramic material (Figures 9–12). Also, very close
Figure 6. Optimal emergence profile of the provisionalrestoration developed by the addition of PMMA, finishing,and polishing before cementation.
Figure 7. Lateral view of the completed provisional restoration.
Figure 8. Appearance of the provisional restoration atcementation.
Figure 9. ART ceramic abutment marked for modificationto place the restoration margin slightly below the patient’smarginal gingival.

S C H N E I D E R
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 25
attention was given to the manufac-turer’s directions on minimal wallthickness to ensure optimal abut-ment strength properties by notoverpreparing the abutment.
The laboratory can now fabricatethe definitive restoration of the cho-sen materials and return the finalrestoration and abutment to theprosthodontist/restorative doctor
for delivery (Figures 13 and 14).The definitive zirconia abutmentand all-ceramic restoration are triedin, adjusted if necessary, and repol-ished. The author places a smallamount of PVS material in theabutment access following tighten-ing to the recommended torquebefore cementation to allow futureaccess to the retaining screw if nec-essary. The restoration can then be
cemented with the practitioner’scement of choice (Figures 15–17).Note the better periodontal healtharound the ceramic abutment andrestoration compared with theother areas of the patient’s mouth.Even though the patient’s oralhygiene was less than optimal, therewas less bleeding, plaque, andinflammation around the restora-tion than his natural teeth. This
Figure 10. Reduction of the ART abutment with abrasiverotary instruments in the laboratory.
Figure 11. Facial view of the finished preparation of theART abutment.
Figure 12. Diagram of the minimum reduction specifications for the ART abutment.
Figure 13. Completed all-ceramic crown.

26
I M P L A N T R E P L A C E M E N T U S I N G A N A L L - C E R A M I C A B U T M E N T A N D R E S T O R A T I O N
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
Figure 14. Delivery of the ART abutment, with the appropriate torque applied to the retaining screw (25 Ncm).
Figure 15. Delivery of the abutment and restoration.
Figure 16. Patient’s smile following the delivery of the restoration and minorreshaping on the natural central incisal edge to improve esthetic contours.
Figure 17. Radiograph of the completedrestoration.
clinical observation has been made by other authors withoutdefinitive explanation.9
C O N C L U S I O N
More predictable esthetics and stable periodontal health are now
achievable with newer techniquesand materials utilized in traditionaland implant dentistry. The responseof the soft tissue to a particulardental material is an important factor in selecting the material to beused for fabrication of a prosthesis.
Microorganisms that tend to adhereto dental materials can impact thesoft tissue response to that material.It appears that some of the all-ceramic materials may have a tendency to collect fewer microorganisms than

S C H N E I D E R
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 27
some of the traditionally utilized materials.8
As we treat more and youngerpatients with dental implants, as aprofession, we must ensure that therestorations will have long life andcause minimal problems whenreplacement is required. The ulti-mate clinical longevity of single-tooth implants is thought to bemany years; however, the clinicallife span of some of the newerrestorative materials, especiallywhen utilized with dental implants,has yet to be definitively deter-mined. The current results arepromising for helping our patientsparticipate in the decision of materials utilized in the delivery of their dental care with great confidence.
The use of dental implants and zir-conia restorative components isbecoming more commonplace andpredictable with increased research,and numbers of patients success-fully treated with this type of
restoration may become routine intoday’s practice.
D I S C L O S U R E A N D
A C K N O W L E D G M E N T S
Dr. Schneider occasionally lecturesfor Thommen Medical, for whichhe receives honoraria.
The author thanks Todd Fridrich,CDT, FNBC, for his expertise in thepreparation of the abutment, andMidwest Aesthetics (Cedar Rapids,IA, USA) for their assistance in the fabrication of the definitive restoration.
R E F E R E N C E S
1. Kois JC, Kan JY. Predictable peri-implantgingival aesthetics: surgical and prostho-dontic rationales. Pract Proced AesthetDent 2001;13(9):691–8.
2. Schropp L, Kostopoulos L, Wenzel A.Bone healing following immediate versusdelayed placement of titanium implantsinto extraction sockets: a prospective clin-ical study. Int J Oral Maxillofac Implants2003;18(2):189–99.
3. Kois JC. Altering gingival levels: therestorative connections. Part 1: biological variables. J Esthet Dent1994;6:3–9.
4. Spear FM. Maintenance of the interdentalpapilla following anterior tooth removal.Pract Periodontics Aesthet Dent1999;11(1):21–8.
5. Petrungaro PS. Immediate restoration ofimplants utilizing a flapless approach topreserve interdental tissue contours. Pract Proced Aesthet Dent2005;17(2):1151–8.
6. Saadoun AP, Le Gall MG. Periodontalimplications in implant treatment plan-ning for esthetic results. Pract Periodon-tics Aesthet Dent 1998;10(5):655–64.
7. Kan JY, Rungcharassaeng K. Immediateplacement and provisionalization of max-illary anterior single implants: a surgicaland prosthetic rationale. Pract Periodon-tics Aesthet Dent 2000;12(9):817–24.
8. Chang PP, Henegbarth EA, Lang LA.Maxillary zirconia implant fixed partialdentures opposing an acrylic resin implant fixed complete denture: a twoyear clinical report. J Prosthet Dent2007;97:321–30.
9. Bindl A, Mohrmann WM. Survival rate ofmono-ceramic and ceramic-coreCAD/CAM generated anterior crownsover 2–5 years. Eur J Oral Sci2004;112(2):197–204.
Reprint requests: Robert Schneider, DDS,MS, University of Iowa Hospitals and Clin-ics, Hospital Dentistry Institute, Division ofProsthodontics, 200 Hawkins Drive, IowaCity, IA 52242-1049. Tel.: 319-384-8655;Fax: 319-353-6923; e-mail: [email protected]