Embed Size (px)
Citation preview

System Technology
IMPLANTED SYSTEM COMPONENTS
RECEIVER ELECTRODE
T R A N S M I T T E R
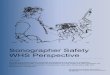
Phased array ultrasound transmitter is implanted sub-muscular over a cardiac echo window. Synchronizes with an RV pacing pulse to transmit ultrasound energy to the receiver electrode to provide Bi-V endocardial pacing.
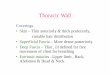
Secure AttachmentEndothelializes for a low risk of thromboembolic events
Anchors onto endocardial wall with 5 nitinol tines
Passive device with no need for replacement
Full endothelialization in animal testing at 30 to 45 days*
B A T T E R Y Implanted subcutaneously on the left mid axillary line, powers the transmitter.
R E C E I V E R E L E C T R O D E Implanted onto the endocardium, the receiver electrode converts ultrasound energy into electrical energy to pace the left ventricle.
C O - I M P L A N T D E V I C E Co-implanted pacemaker, ICD or CRT paces the right ventricle.
SITE
EVA
LUAT
ION
ANCH
ORI
NG
ANCH
ORE
D
Small SizeExpected to diminish the need for chronic anticoagulation
LENGTH OF BODY: 9.1mmDIAMETER: 2.7mm
WEIGHT: 0.12 gramsVOLUME: 0.05 cc
* Echt DS, Moore D, Cowan M, Valli VE, Whitehair, JG, Willis NP. Chronic implantation of leadless pacing electrodes in the left ventricle of a goat model. Heart Rhythm 2010;7:S451-2.
Caution: Not commercially available in the United States
LV ENDOCARDIUM WALL
Image taken from In-vivo study (caprine) at
45 days post implant
ENDO
THEL
IALI
ZED
ACTUAL SIZE

DELIVERY SYSTEM
WiSE CRT IMPLANTATION PROCESS
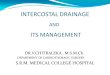
Designed for Safe Receiver Electrode Placement^
Innovative inflatable polyester balloon, creates an atraumatic tip for safety during anchoring of the receiver electrode
Radiopaque materials enhance visualization of sheath tip position during implant
Direct connection of the cathode tip of the Receiver Electrode to EP systems for analysis of local EGM signals, pacing and threshold testing^ Results from the SELECT-LV trial confirm all Receiver Electrode devices were
safely placed without pericardial effusion events (N=34)
Stage 2: Receiver Electrode Implantation
➊ Introduce the 12F Delivery System into the LV via a retrograde aortic approach
➋ Navigate the Delivery System to a target site using fluoroscopy
➌ Evaluate conventional pacing capture thresholds, local electrograms, and/or hemodynamics of pacing the site prior to anchoring the receiver electrode
➍ Once a suitable site has been selected, anchor the receiver electrode into the LV wall, detach and release it from the Delivery System
Sheath’s ballooon on LV wall (with Transmitter and the RV lead in view)
Contrast injection is used to confirm receiver electrode is anchored into LV wall
Stage 1: Transmitter and Battery Implantation
➊ Make incisions above the identified Transmitter implantation site and on the mid-axillary line
➋ Create pockets for the transmitter and the battery➌ Create a tunnel between pockets for the transmitter cable➍ Secure the transmitter to the intercostal muscle ➎ Connect the transmitter cable to the battery and secure
the battery in the subcutaneous pocket Submuscular transmitter implantation with pocket formed
through dissection down to the intercostal muscle
RIB INTERCOSTAL MUSCLE RIB
MUSCLE MUSCLE
FAT FATSKIN SKIN
Stage 0: Pre-implant Assessment
Performed by a cardiac sonographer in an outpatient setting using standard TTE
Intercostal spaces are assessed for transmitter implantation to identify acoustic transmission paths that are free of lung and rib
Select a location for the Transmitter implant over ICS 4 through 7
ICS 4
ICS 5
ICS 6
ICS 7
EBR Systems, Inc. 686 W. Maude Ave., Suite 102, Sunnyvale, CA 94085 USA www.ebrsystemsinc.com© 2016 EBR Systems, Inc. All Rights Reserved. WiSE is a trademark of EBR Systems, Inc.Caution: Not commercially available in the United States
RETRACTABLE 8F CATHETER WITH MOUNTED RECEIVER ELECTRODE
ATRAUMATIC BALLOON INFLATABLE WITH CONTRAST
12F STEERABLE DELIVERY SHEATH
MC-03242 Rev. A