Embed Size (px)
Citation preview

A Professional Courtesy of: James E. Metz, D.D.S.General Dentist
Diplomate, American Board of Dental Sleep Medicine
1271 E. Broad StreetColumbus, Ohio 43205
(614) 252-4444 • Fax: (614) 252-6474www. ColumbusDentistry. com
Memberships:American Dental Association • Ohio Dental Association • Columbus Dental Society
American Academy of Restorative Dentistry International Academy of Gnathology • American College of DentistsEuropean Academy of Dental Sleep Medicine • American Academy of Dental Sleep Medicine • American Academy of Sleep Medicine
Implants in the Growing Patient
1. Children congenitally missing a single toothand having adjacent permanent teeth
Group 2. Children missing more than a few teethbut having permanent teeth present adjacent to theedentulous sites
Today, the available treatment options for an edentulous space almost always include a dental implant, the placement of which has
been restricted to patients with complete craniofadal growth. Recently, there have been reports of exceptions to this rule. Tliis issue of
Report on Prosthodontics discusses the appropriate timing of implant placement as it relates to the growth of the patient.
Timing forImplants in an Adolescent•BUI he success of dental implants has allowed dentists to
rehabilitate edentulous and partially edentulouspatients' oral function and social lifestyle. But place-
ment of an implant too early in a growing child's devel-opment may lead to implant dentition height discrepan-cies, a poor implant—crown ratio, occlusal disharmony anddiscrepancies of free gingival margin height, leading toesthetic compromise.
Sharma andVargervik from the University of California,San Francisco, outlined the indications and timing forthe use of dental implants in adolescents. Based on pub-lished data and their clinical experience, the authorsdivided adolescents with partial and complete anodontiainto 3 groups:
3. Children completely edentulous in I arch orhaving 1 or 2 teeth in poor positions in the arch
For patients in group 1,skeletal development ismore important thanchronologic age. If animplant is placed beforedentoalveolar growth iscomplete, the implantwill become submergedrelative to the adjacentteeth. If the implantcrown is remade to theappropriate length, the
Inside this issue:
:- V ; •.;> '.-:•
Winter 201Q
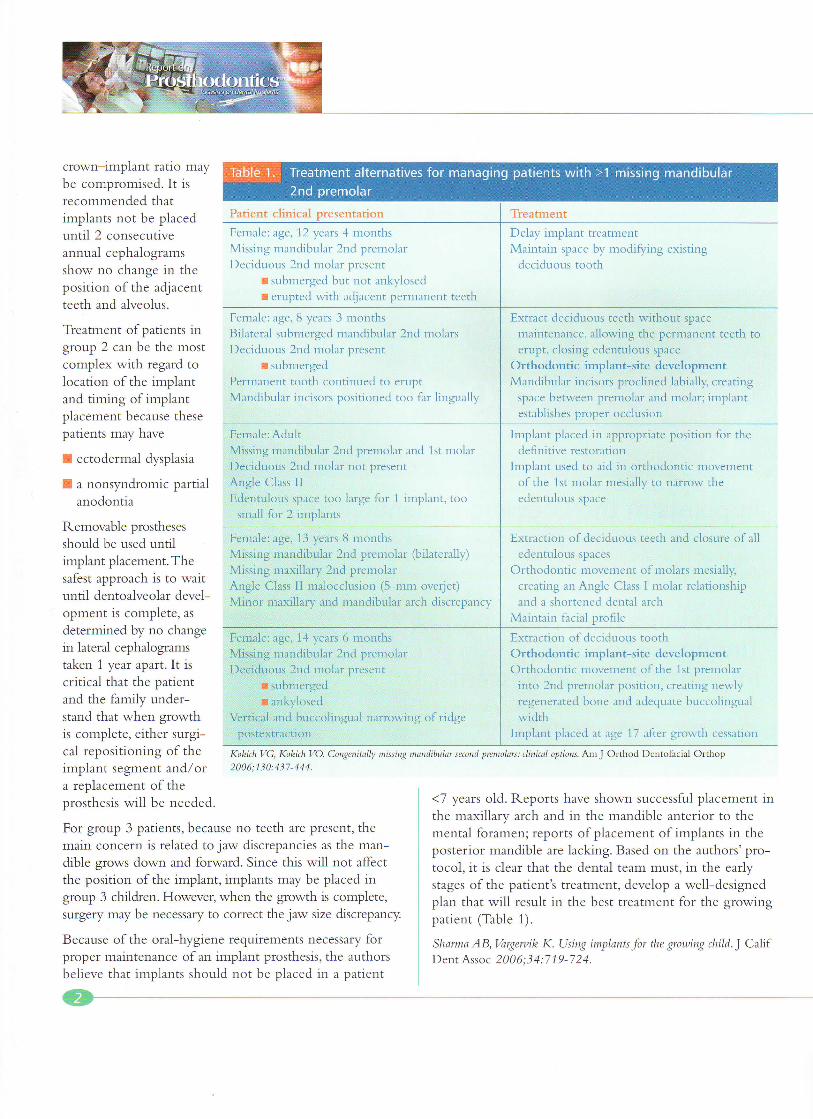
Table 1.
Patient clinical presentation
Female: age, 12 years 4 monthsMissing mandibular 2nd premolarDeciduous 2nd molar present
• submerged but not ankylosed• erupted with adjacent permanent teeth
Female: age, 8 years 3 monthsBilateral submerged mandibular 2nd molarsDeciduous 2nd molar present
• submergedPermanent tooth continued to eruptMandibular incisors positioned too far lingually
Female: AdultMissing mandibular 2nd premolar and 1st molarDeciduous 2nd molar not presentAngle Class IIEdentulous space too large for 1 implant, too
small for 2 implants
crown—implant ratio maybe compromised. It isrecommended thatimplants not be placeduntil 2 consecutiveannual cephalogramsshow no change in theposition of the adjacentteeth and alveolus.
Treatment of patients ingroup 2 can be the mostcomplex with regard tolocation of the implantand timing of implantplacement because thesepatients may have
• ecto dermal dysplasia
III a nonsyndromic partialanodontia
Removable prosthesesshould be used untilimplant placement. Thesafest approach is to waituntil dentoalveolar devel-opment is complete, asdetermined by no changein lateral cephalogramstaken 1 year apart. It iscritical that the patientand the family under-stand that when growthis complete, either surgi-cal repositioning of theimplant segment and/ora replacement of theprosthesis will be needed.
For group 3 patients, because no teeth are present, themain concern is related to jaw discrepancies as the man-dible grows down and forward. Since this will not affectthe position of the implant, implants may be placed ingroup 3 children. However, when the growth is complete,surgery may be necessary to correct the jaw size discrepancy.
Because of the oral-hygiene requirements necessary forproper maintenance of an implant prosthesis, the authorsbelieve that implants should not be placed in a patient
Treatment alternatives for managing patients with >1 missing mandibular
2nd premolar
:•. ntnient
Delay implant treatmentMaintain space by modifying existing
deciduous tooth
Extract deciduous teeth without spacemaintenance, allowing the permanent teeth toerupt, closing edentulous space
Orthodontic implant-site developmentMandibular incisors proclined labially, creating
space between premolar and molar; implantestablishes proper occlusion
Implant placed in appropriate position for thedefinitive restoration
Implant used to aid in orthodontic movementof the 1st molar mesially to narrow theedentulous space
Female: age, 13 years 8 monthsMissing mandibular 2nd premolar (bilaterally)Missing maxillary 2nd premolarAngle Class II malocclusion (5-nim overjet)Minor maxillary and mandibular arch discrepancy
Female: age, 14 years 6 monthsMissing aim d aa ar 2nd premolarI /eciduous 2nd molar present
: ,ei emerged• ankyiosed
Vertical and buccolniguai narrowitpostextnic don
nitulty missing
Extraction of deciduous teeth and closure of alledentulous spaces
Orthodontic movement of molars mesially,creating an Angle Class I molar relationshipand a shortened dental arch
Maintain facial profile
I Extraction of deciduous toothOrthodontic implant-site developmentOrthodontic movement of the 1st premolar
into 2nd premolar position, creating newlyregenerated bone and adequate buccolingualwidth
Implant placed at age 1.7 after growth cessation
irs: clinical options. Am J Orthod Dentofacial Orthop
<7 years old. Reports have shown successful placement inthe maxillary arch and in the mandible anterior to themental foramen; reports of placement of implants in theposterior mandible are lacking. Based on the authors' pro-tocol, it is clear that the dental team must, in the earlystages of the patient's treatment, develop a well-designedplan that will result in the best treatment for the growingpatient (Table 1).
Sharma AB, Vargervik K. Using implants for the growing child.] CalifDent Assoc 2006;34:719-724.

Winter 2010
Implants in Children withEctodermal Dysplasia
Ithough there are >170 forms of ectodermal dyspla-sia (ED), the disease is characterized by a primary
*Hlidefect in >1 of the tissues: nails, hair, teeth or sweatglands. Children and adolescents with mild forms of ED arecommonly concerned about dental anomalies and facialappearance, the results of irregular distribution and abnor-mal shape of the teeth that often restrict the use of crownsand fixed prostheses. Because the underdeveloped hypo-dontic mandible may provide inadequate retention and sup-port for a conventional prosthesis, conventional prosthodontictreatment may be insufficient. Placement of dental implantsto replace missing teeth is usually delayed until craniofacialgrowth is complete. Kramer et al from Georg-August-Uni-versity of Goettingen, Germany, presented a case report toillustrate the current literature regarding implants in chil-dren with ED.
Clinical and radiographic analysis of a 3-year-old male pa-tient revealed severe hypodontia of the maxilla and man-dible. The deciduous dentition consisted of the maxillarycentral incisors, and the permanent dentition consisted ofcentral incisors and a tooth germ of a right mandibular firstmolar. A diagnosis of hypohydratic ED was made based onclinical findings and a skin biopsy.
At age 5 years, maxillary and mandibular dentures were fab-ricated for the patient. By age 8 years, the mandibular pros-thesis became increasingly difficult for the patient to man-age because of mandibular growth and the deficient alveolarridge. As a result of loss of function and pyschosocial issuesrelated to the lack of teeth, two 3.75-mm x 13-mm im-plants were placed in the anterior mandible. After a sub-merged healing period, a bar connecting the implants, amandibular implant overdenture and a maxillary completedenture were fabricated. The dentures had been function-ing well for 2 years at the time of the report.
The insertion of dental implants in children and adoles-cents before the completion of craniofacial growth can re-sult in infraocclusion and multidimensional dislocation ofthe implant when compared with the developing teeth. Ina pediatric patient with ED and near anodontia, this issue ismoot. However, because the maxillary growth process ofdrift and displacement can result in unpredictable disloca-
tions of the implants in both vertical and anteroposteriordirections, fixed implant prostheses crossing the midpalatalsuture will result in a transverse growth restriction of themaxilla. In the posterior mandible, growth occurs with an-teroposterior, transverse and vertical changes in late child-hood. The mandibular rotational growth results in additionalvertical changes. Currently, there are no reports in the litera-ture of the use of implants in the posterior mandibles ofchildren.
The majority of anterior mandible alveolar growth occurs inearly childhood. Although implants placed in the anteriormandible of severely anodontic children may be a viablesolution, the use of implants to replace a single missing toothin the anterior mandible is ill-advised.
When placing implants in children with ED, the pediatricdentist, orthodontist, surgeon, periodontist and prostho-dontist must work together. Regardless of the timing of theimplant placement, definitive prosthodontic rehabilitationmust address the patient's functional, esthetic and psycho-logical needs. Preservation of the existing dentition mayextend the timing for implant placement. In patients whomay have some remaining teeth, orthodontic treatmentmay optimize tooth position. With the prosthodontist'sknowledge of craniofacial growth and development and ofthe prosthetic issues for the care of these patients, an early in-terdisciplinary approach will result in greater success for thepatient.
Kramer F-J, Baethge C, Tschernitschek H. Implants in children with ec-
todermal dysplasia: a case report and literature review. Clin Oral Imp!
Res 2007;18:140-146.
Timing ofIn the Growing
I n a growing child, replacing a permanent tooth lostfrom trauma with an implant poses a challengingdilemma because the implant's lack of eruption poten-
tial can lead to discrepancies in the occlusal plane, estheticproblems and possible disruption of the normal develop-ment of the jaw. Op Heij et al from Catholic University ofLeuven, Belgium, summarized the growth patterns of eachjaw, noting their implications and giving treatment recom-mendations (Table 2).

i
Winter 2010
Table 2. Implications of early implant placement by location and type of growth
Maxilla
Implication
Mandible
Implication
Transverse growth
Anterior regioncompleted prior toadolescent growthspurt
Sutural wideninggreater in posterior
• Can lead todiastema andshifting of midlineto the implant side
Anterior growthceases early; limitedremodeling causesleast problems
Posterior growthcontinues longerthrough remodelingand bone apposition
• Premolar or molarimplant could beshifted into alingual position
Sagittal growth
Closely associated withskeletal growth; when itfollows the mandibulargrowth, loss of suturalgrowth via resorptionresults
• Anterior resorptioncould result in loss ofbone on labial side ofimplant
Endochondral growth atcondyle and remodelingof ramus
• No impact on implantplacement
• Rotation in sagittalplane must beconsidered
Vertical growth
Maxilla displaced downwardvia sutural growth, remodelingand eruption; adult levels ofvertical growth usually reachedat age 17—18 in girls and laterin boys
• Leads to infraocclusal;unfavorable
• Endosseous-supraosseousratio
Height increase bv condylargrowth and bone apposition
Facial types develop indifferent ways
• Normal: minor rotation
• Short: horizontal growth.forward rotation, deep bite
• Long: vertical growth,posterior rotation, skeletalopen bite
• Affects antereoposterior andvertical eruption patterns
• Affects relationship betweenimplant and adjacent toothin vertical and labiolingualdirection
Recommendation
Delay implant placementuntil skeletal growthcomplete
*In anodontic child,implant placement inthe posterior could beconsidered under well-planned conditions
Delay implant placementuntil skeletal growthcomplete
*In a severe anodonticor oligodontic child.implants may be placed
mandible
*Lack of reports withreffi:rd tu mrpi-iiU1- - \r mandible
The key to implant placement in these patients appears tobe the determination of cessation of growth. Because theage at which growth is complete varies widely, chronologicage is not a true indicator of growth cessation. The averageage of growth spurts in girls is 12 years, while the averageage in boys is 14 years. However, growth changes occurbeyond the time of the growth spurt and may vary by asmuch as 6 years. Additionally, individuals with short andlong face types have shown changes up to the age of25 years.
Treatment of these patients begins with a reliable evalua-tion of growth based on cephalometric radiographic exam-ination. Management of the edentulous space should beincreased through an interim prosthesis until the appropri-ate time for implant placement. These patients require thecoordinated treatment of a dental team consisting of pedi-atric dentist, orthodontist, surgeon and prosthodontist.
Op Heij DG, Opdebeeck H, van Steenberghe D, et al. Facial development,
continuous tooth eruption, and mesial drift as compromising factors for im-
plant placement, hit J Oral Maxillofac Implants 2006;21:867-878.
the Next Issue









![Small-Diameter Implants - dentalCEtoday.com · Small-Diameter Implants: ... impressions, shade (A2 VITA Shade Guide [Vident]), and ... epithelial growth factors.7-9 The patient was](https://img.pdfslide.net/doc/110x75/5ad50f0c7f8b9aff228ca0f1/small-diameter-implants-implants-impressions-shade-a2-vita-shade-guide.jpg)



















