Embed Size (px)
Citation preview

Clinical Opinion www.AJOG.org
OBSTETRICS
Intrapartum management of category II fetal heart ratetracings: towards standardization of careSteven L. Clark, MD; Michael P. Nageotte, MD; Thomas J. Garite, MD; Roger K. Freeman, MD; David A. Miller, MD;Kathleen R. Simpson, RN, PhD; Michael A. Belfort, MD, PhD; Gary A. Dildy, MD; Julian T. Parer, MD;Richard L. Berkowitz, MD; Mary D’Alton, MD; Dwight J. Rouse, MD; Larry C. Gilstrap, MD; AnthonyM. Vintzileos, MD;J. Peter van Dorsten, MD; Frank H. Boehm, MD; Lisa A. Miller, CNM, JD; Gary D. V. Hankins, MD
nterpretation and management of
There is currently no standard national approach to the management of category II fetalheart rate (FHR) patterns, yet such patterns occur in the majority of fetuses in labor. Undersuch circumstances, it would be difficult to demonstrate the clinical efficacy of FHRmonitoring even if this technique had immense intrinsic value, since there has neverbeen a standard hypothesis to test dealing with interpretation and management of theseabnormal patterns. We present an algorithm for the management of category II FHRpatterns that reflects a synthesis of available evidence and current scientific thought. Useof this algorithm represents one way for the clinician to comply with the standard of care,and may enhance our overall ability to define the benefits of intrapartum FHR monitoring.Key words: fetal heart rate monitoring, neonatal encephalopathy, patient safety
I fetal heart rate (FHR) patterns duringlabor remains one of the most prob-lematic issues in obstetrics. Multiplebasic science investigations and clinicaltrials have been published since theintroduction of this technique in the late1950s.1-7 Unfortunately, this body ofwork has primarily served to raise morequestions than it has answeredeas amedical community, we seem to knowless than we thought we did 30 years agoregarding the utility of this ubiquitoustechnique.
In recent years, several specific issuesrelating to the interpretation and man-agement of FHR patterns have receivedconsiderable attention in the medicalliterature. These include the lack ofagreement in interpretation even amongrecognized experts, the role of FHRpatterns as a primary driver of a risingcesarean rate, and the explosion oflitigation involving FHR patterns, de-spite the consistent absence of scien-tific evidence to support the contentionthat intervention based on any singleFHR pattern or combination of FHR
From the Hospital Corporation of America (Dr ClarkTN; Long Beach Memorial Hospital, Long Beach (D(Drs Garite and Freeman), University of Southern CofCalifornia, San Francisco (Dr Parer), CA;MercyHoof Medicine and Texas Children’s Hospital (Drs BelfoHouston, TX, and University of Texas Medical BranPresbyterian/Columbia University, New York (Drs BHospital, Mineola (Dr Vintzileos), NY; Brown UniverIsland, Providence, RI (Dr Rouse); Medical UniversiDorsten); and Perinatal Risk Management and Con
Received Jan. 21, 2013; revised March 27, 2013;
Management recommendations discussed in this ddo not necessarily reflect endorsement by affiliated
The authors report no conflict of interest.
Reprints not available from the authors.
0002-9378/$36.00 � ª 2013 Mosby, Inc. All rights reser
patterns in fact prevents cerebralpalsy or other types of neurologicimpairment.8-12
Against this background, however,there remains in many of us suspicion(albeit based primarily upon anecdotalexperience and the original basic scienceinvestigations) that at least a portionof the conflicting evidence regardingthe clinical utility of intrapartum FHRmonitoring results from ad hoc inter-pretation of terminology, and the lack ofstandardized protocols for managementand intervention based onwhat are often
) and Vanderbilt University (Dr Boehm), Nashville,r Nageotte), University of California, Irvinealifornia, Los Angeles (Dr Miller), and Universityspital, St. Louis,MO (DrSimpson); BaylorCollegert and Dildy) and University of Texas (Dr Gilstrap),ch, Galveston (Dr Hankins), TX; New Yorkerkowitz and D’Alton) and Winthrop Universitysity and Women and Infant’s Hospital of Rhodety of South Carolina, Charleston, SC (Dr vansultation Services, Portland, OR (Ms Miller).
accepted April 24, 2013.
ocument reflect the opinions of the authors. Theyinstitutions or organizations.
ved. � http://dx.doi.org/10.1016/j.ajog.2013.04.030
AUGUST 2013 A
challenging patterns. In a very real sense,the FHRmonitor is a medical device thatwas introduced into clinical practicewithout an instruction manual, withoutthe now common premarket testing tosupport the unrealistic expectationsof efficacy, and without clearly definedparameters for use. Under such cir-cumstances, it would be difficult todemonstrate clinical efficacy even of adevice with immense intrinsic value,since there has never been a standardhypothesis to test dealing with interpre-tation and management of abnormalpatterns. With respect to the assessmentof the clinical value of FHR monitoring,an evolving consensus exists in thematernal-fetal medicine community thatit is time to start over and establish somecommon language, standard interpreta-tion, and reasonable management prin-ciples and guidelines.13-19
A Eunice Kennedy Shriver NationalInstitute of Child Health and HumanDevelopment (NICHD) consensus panelin 2008 proposed a uniform system ofterminology inwhich any FHR pattern isclassified as category I, II, or III, based onthe presence or absence of well-definedaspects of the FHR.20 Once univer-sally adopted in clinical practice, these
merican Journal of Obstetrics & Gynecology 89

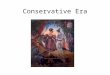
FIGURE 1Algorithm for management of category II fetal heart rate tracings
Yes
No
NoNo Yes No Yes
Yes Yes
No
No
Yes
Significant decelerations with ≥50% of contractions for 1 hour
Moderate variability or accelerations
Significant decelerations with ≥50% of contractions for 30 minutes
Latent Phase Active Phase Second Stage Observe for 1 hour
Normal labor progress Normal progress Persistent pattern
Manage per algorithmCesarean or OVDObserve ObserveCesarean Cesarean or OVD
OVD, operative vaginal delivery.
aThat have not resolved with appropriate conservative corrective measures, which may include supplemental oxygen, maternal position changes, intravenous fluid administration, correction of hypotension,reduction or discontinuation of uterine stimulation, administration of uterine relaxant, amnioinfusion, and/or changes in second stage breathing and pushing techniques.
Clark. Category II FHRT. Am J Obstet Gynecol 2013.
Clinical Opinion Obstetrics www.AJOG.org
definitions should serve as an importantfirst step in both the investigation of thesignificance of various FHR patterns,and the development of a uniformstandard of care in the interpretationand management of such patterns. Withthis in mind, subsequent recommenda-tions have been developed by theAmerican Congress of Obstetricians andGynecologists (ACOG) for the manage-ment of category I (normal) and cate-gory III (pathologically abnormal) FHRpatterns.20,21 Although useful, theserecommendations remain insufficientsince �80% of fetuses in labor demon-strate FHR patterns that fall into cate-gory II, patterns for which no specificACOG management recommendationsexist.21,22
The management of category II FHRpatterns remains the most importantand challenging issue in the field ofFHRmonitoring, and is arguably second
90 American Journal of Obstetrics & Gynecology
only to preterm birth as the mostpressing issue in clinical obstetrics. Inaddition, the overall cesarean deliveryrate exceeded 32% in the United States in2011, and exceeds 50% of all births insome US hospitals.23 While dystocia andprior cesarean delivery remain the lead-ing indicators for such surgical inter-vention, the presence of a category II orIII FHR in labor is a frequent indicationas well.11,24 For cesarean deliveries, thereis a wide variance in the reportedindications and their frequency, bothbetween hospitals and among membersof the medical staff practicing obstet-rics.24 Concern regarding FHR patternsis perhaps the indication that has thegreatest such variance; we believe thisobservation is directly related to theabsence of defined management pro-tocols for category II patterns.Accordingly, we present a suggested
algorithm for the management of
AUGUST 2013
category II FHR patterns (Figure 1)along with several important specificclarifications (Table). As outlined inFigure 1, it is reasonable to initiatemanagement of a category II FHRpattern with an assessment of variabilityand accelerations, thus allowing theclinician to immediately rule out thepresence of clinically significant meta-bolic acidemia. For nonacidemic fetuses,the focus then shifts to assessing thelikelihood of developing significantacidemia prior to delivery. While no al-gorithm can predict all cases of suddendeterioration due to sentinel events, evenwith category I FHR patterns, analysis ofthe frequency and nature of de-celerations and the progress in laborprovides the clinician with a reasonableapproach to such decision making(Figure 1).
With category II FHR tracings thatdo not exhibit moderate variability or

TABLEManagement of category II fetal heart rate patterns: clarifications for use in algorithm
1. Variability refers to predominant baseline FHR pattern (marked, moderate, minimal, absent) during a 30-minute evaluation period, as definedby NICHD.
2. Marked variability is considered same as moderate variability for purposes of this algorithm.3. Significant decelerations are defined as any of the following:
� Variable decelerations lasting longer than 60 seconds and reaching a nadir more than 60 bpm below baseline.� Variable decelerations lasting longer than 60 seconds and reaching a nadir less than 60 bpm regardless of the baseline.� Any late decelerations of any depth.� Any prolonged deceleration, as defined by the NICHD. Due to the broad heterogeneity inherent in this definition, identification of a prolonged
deceleration should prompt discontinuation of the algorithm until the deceleration is resolved.4. Application of algorithmmay be initially delayed for up to 30minutes while attempts are made to alleviate category II pattern with conservative
therapeutic interventions (eg, correction of hypotension, position change, amnioinfusion, tocolysis, reduction or discontinuation of oxytocin).5. Once a category II FHR pattern is identified, FHR is evaluated and algorithm applied every 30 minutes.6. Any significant change in FHR parameters should result in reapplication of algorithm.7. For category II FHR patterns in which algorithm suggests delivery is indicated, such delivery should ideally be initiated within 30 minutes of
decision for cesarean.8. If at any time tracing reverts to category I status, or deteriorates for even a short time to category III status, the algorithm no longer applies.
However, algorithm should be reinstituted if category I pattern again reverts to category II.9. In fetus with extreme prematurity, neither significance of certain FHR patterns of concern in more mature fetus (eg, minimal variability) or
ability of such fetuses to tolerate intrapartum events leading to certain types of category II patterns are well defined. This algorithm is notintended as guide to management of fetus with extreme prematurity.
10. Algorithm may be overridden at any time if, after evaluation of patient, physician believes it is in best interest of the fetus to intervene sooner.
FHR, fetal heart rate; NICHD, Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Clark. Category II FHRT. Am J Obstet Gynecol 2013.
www.AJOG.org Obstetrics Clinical Opinion
accelerations, but do exhibit patterns ofpersistent late or significant variabledecelerations, as defined in the Table,significant metabolic acidemia cannotbe excluded. Further, these decelerationpatterns signify the presence of physio-logic stresses that increase the riskof developing such acidemia. In suchcases, we recommend expeditious de-livery. Examples of the application ofthis algorithm are demonstrated inFigures 2-5. These examples assume thatthe 20-minute period shown in thefigures is representative of the 30-60minute observation period referred toin the algorithm. Should the patterneither improve or deteriorate during thistime frame, management should bechanged accordingly.
In assessing and implementing thisalgorithm, we wish to bring specificattention to a number of considerationswhich we consider to be particularlygermane.1. This algorithm follows the foun-
dational NICHD definitions andrecommendations.20,21
2. This algorithm should be un-derstood as a next step in the
development of management rec-ommendations for category II FHRpatterns. The effectiveness andassociated intervention rates of thisalgorithm may be further definedand refined in future studies.
3. Category II patterns identify fetusesthat may potentially be in somedegree of jeopardy but are either notacidemic, or have not yet developed adegree of hypoxia/acidemia thatwould result in neonatal encepha-lopathy.12,20,21 However, we believeone important goal of intrapartumcare is delivery of the fetus, whenpossible, prior to the development ofdamaging degrees of hypoxia/acid-emia. We offer this algorithm toassist the attending physician inaccomplishing this goal. We recog-nize that adherence to the algorithmcannot alter the course for an alreadyinjured fetus, or one that experiencesan unexpected catastrophic eventduring labor.
However, since any algorithmfor the management of category IIpatterns will apply to the majorityof fetuses during labor, the
AUGUST 2013 A
algorithm must also avoid unnec-essary intervention, and encouragevaginal delivery in women whoseFHR patterns suggest minimal riskof significant deterioration prior todelivery. We designed this algo-rithm with both goals in mind, butwith a primary focus on theavoidance of preventable injury.
4. The appropriateness of select con-servative attempts to relieve certaincategory II patterns is well estab-lished.25-29 However, valid scientificevidence affirming the effectivenessof such measures varies widely. Forexample, while amnioinfusion forrelief of oligohydramnios-associatedvariable decelerations is well sup-ported in the literature, no evidenceexists to support the efficacy ofmaternal oxygen administrationin commonly achievable concen-trations in increasing fetal tissueoxygenation, or in improving new-born outcomes regardless of oxygenconcentration.28,29 Nevertheless, anyof the commonly accepted ap-proaches to relief of abnormal FHRpatterns may be appropriately
merican Journal of Obstetrics & Gynecology 91

FIGURE 2Tracing exhibits minimal to absent variability without decelerations, despite regular contractions
Medication effect has been excluded clinically as part of the initial period of intrauterine resuscitation attempts. While the fetus may have experienced
prelabor central nervous system injury, absence of late decelerations excludes ongoing hypoxia in a neurologically intact fetus. However, since such
fetuses may not tolerate labor without sudden deterioration and demise, cesarean delivery would be appropriate, per algorithm, if pattern persists for
1 hour.
Clark. Category II FHRT. Am J Obstet Gynecol 2013.
Clinical Opinion Obstetrics www.AJOG.org
attempted in specific situations.Their effect should be apparentwithin 30 minutes of application(Figure 1). If theFHRtracing remainscategory II following these efforts, thealgorithm is applied to the patternobserved following these attempts attherapeutic intervention.
Attention should be given to theprompt elimination of excessiveuterine activity including tachysystoleor prolonged contractions, especiallywhen uterine stimulants (oxytocin orprostaglandin-containing agents) arebeing applied.30,31 Oxytocin infusionshould be reduced or discontinuedin the presence of excessive uterineactivity and a persistent category
FIGURE 3Tracing exhibits minimal to absent v
Per algorithm, expedited delivery is indicated rega
Clark. Category II FHRT. Am J Obstet Gynecol 2013.
92 American Journal of Obstetrics & Gynecology
II FHR pattern.21 Acceptable ap-proaches to monitoring of uterineactivity are well described in availableliterature.30,31
5. Recent data suggest that no singlequantitative value of fetal arterialpH serves to define a point ofhypoxia-induced damage applicableto all fetuses.32 However, the litera-ture is consistent in its demonstra-tion that for any individual fetus,baseline variability and accelera-tions will reliably be depressedbefore the pH has reached a level ofacidemia associated with neurologicinjury for that fetus, regardless ofits quantitative value.33,34 Hencethis algorithm relies strongly on the
ariability and late decelerations occurrin
rdless of labor progress.
AUGUST 2013
presence of moderate baseline vari-ability or accelerations. In contrast,conflicting data exist regardingthe significance of variability withindeceleration nadirs.35,36 Variabilitywithin decelerations alone cannotbe reliably used to exclude fetalacidemia and accordingly is notaddressed in this algorithm.
6. FHR patterns cannot be inter-preted in isolation. Accordingly,we have incorporated labor prog-ress as described in traditionalterms (stage I latent phase, stage Iactive phase and second stage) intothis algorithm. This is of signifi-cance since the expected remaininglength of labor may influence
g with >50% of contractions

FIGURE 4Tracing exhibits moderate variability and accelerations, thus excluding clinically significant acidemia
Late decelerations represent protective cardiovascular response to contraction-induced reductions in fetal oxygenation. Per algorithm, if labor is
progressing normally in active phase or second stage, careful observation would be appropriate. If the fetus is remote from delivery, delivery would be
appropriate.
Clark. Category II FHRT. Am J Obstet Gynecol 2013.
www.AJOG.org Obstetrics Clinical Opinion
the likelihood of, and responseto, deterioration of category IIpatterns. A category II patternmay have a different indicatedmanagement when presenting inearly first-stage labor than anidentical pattern presenting in thelate second stage. We acknowledgerecent data suggesting that cesareandelivery based on classic definitionsof protracted active phase, arrest ofdilatation, or arrest of second-stagedescent alone may not be necessary,and that longer periods of obser-vation may yield lower interventionrates.10,37 However, data demon-strating the safety of these more
FIGURE 5Tracing exhibits moderate variability
Significant variable decelerations seen here sugges
Per algorithm, if labor is progressing normally in a
delivery, delivery would be appropriate.
Clark. Category II FHRT. Am J Obstet Gynecol 2013.
conservative approaches in thepresence of persistent category IIFHR patterns are lacking. Forexample, we hesitate to recommendnonintervention for an arrest ofactive phase dilatation of 4 hours inthe presence of recurrent late de-celerations, even in the presence ofmoderate variability. The superbreliability of accelerations andmoderate variability in excludingany degree of hypoxia-related cen-tral nervous system depression orrisk of ongoing hypoxic injurywould allow observation of patternswith these features and adequatelabor progress regardless of the
and acceleration, thus excluding clinic
t umbilical cord compression during contraction, wh
ctive phase or second stage, careful observation w
AUGUST 2013 A
deceleration pattern (Figure 1).However, intervention in patientswith certain category II patternsand slow, but technically adequatelabor progression may also be anappropriate option.
7. Some well-defined features ofcategory II patterns (eg, fetal tachy-cardia or marked variability) arenot included in the algorithm-based decision tree for interven-tion. This does not signify that suchpatterns are innocuouseindeed, itmay be exactly these features of atracing that mandate considerationas a category II pattern, and the useof this algorithm. However, in such
ally significant acidemia
ich could, over time, lead to significant acidemia.
ould be appropriate. If the fetus is remote from
merican Journal of Obstetrics & Gynecology 93

Clinical Opinion Obstetrics www.AJOG.org
cases, it is our expectation thatother concerning patterns includedin the algorithmwill appear prior tothe need for intervention.
8. This algorithm is intended toaddress the challenge of progressiveintrapartum hypoxia/acidemia dueto the effects of labor contractionson a susceptible fetus. Neither this,nor any other management ap-proach to labor, will ever predict,or prevent, unexpected sentinelevents that may occur withoutwarning and rapidly change a FHRpattern from category II to categoryIII. In such situations, even themost expeditious response may beinsufficient to avoid neonatal en-cephalopathy and its sequelae.38,39
However, 2 clinical situations existin which category II patterns, whileexcluding ongoing hypoxia/acid-emia, may be harbingers of sentinelevents that may rapidly lead toprofound hypoxia. These condi-tions are vaginal bleeding sufficientto suggest possible placental ab-ruption, and any woman undergo-ing a trial of labor after a previouscesarean.40-42 In both cases, thisalgorithm does not apply, as expe-ditious cesarean delivery is oftenindicated based on the suddenappearance of decelerations in acontext (moderate variability andaccelerations) that would be other-wise reassuring.
9. This algorithm does not address theissue of prolonged deceleration,as defined by the NICHD. Thisdefinition is too broad to be clini-cally useful in isolation.20,21 A 121-second deceleration to 90 beats/minand a 9-minute and 59-seconddeceleration to 50 beats/min are,from a clinical standpoint, verydifferent, yet both are, by definition,prolonged decelerations. The situa-tions associated with prolongeddecelerations also greatly impactthe decision makingea prolongeddeceleration following an epiduralshould give rise to a completelydifferent set of management con-siderations than an identical patternin a woman laboring with a scarred
94 American Journal of Obstetrics & Gynecology
uterus.40,42,43 Such variations arelegion and cannot be adequatelyaddressed with a single algorithmeindeed, their rarity and physiologicheterogeneity probably precludemeaningful study as a group.We canonly comment that tolerance forsuch recurrent patterns remotefrom delivery ought to be smallunless the etiology is apparent andcan be promptly ameliorated.
10. The current NICHD classificationsystem uses the classic descriptionsof deceleration patterns initiallydeveloped by Kulbi and colleagues.1
However, because different types ofdecelerations have unique etiol-ogies, a given fetus may have >1pathologic process ongoing duringlabor. One example would be agrowth-restricted fetus with oligo-hydramnios demonstrating bothvariable decelerations secondary tocord compression and late de-celerations due to hypoxia duringcontractions based on uteropla-cental insufficiency. This may giverise to a less well-defined, hybridpattern of decelerationsefor exam-ple, late decelerations superim-posed upon variable decelerations.Because relatively benign variabledecelerations are visually moredramatic than the subtle, yet moreconcerning, late decelerations, thelatter may be easily overlooked.In such cases, the patient shouldbe managed with a focus on thelate, rather than the variable de-celerations. Such hybrid decelera-tion patterns differ from the morecommonly seen “atypical” variabledecelerations that have no correla-tion with fetal acidemia.35 It isimportant for clinicians to carefullyevaluate any atypical-appearingvariable decelerations in this light.
11. The algorithm presented authorizesjudgment in some situations be-tween cesarean delivery and opera-tive vaginal delivery. We wish toemphasize that operative vaginaldelivery is not universally appli-cable, but rather depends on thepatient meeting appropriate criteriafor vacuum or forceps, as well as
AUGUST 2013
operator expertise in use of thesetechniques.44,45 Because deliverybased on this algorithm will beprincipally driven by concern forfetal well-being, and because vari-able levels of expertise in operativevaginal delivery exist among prac-titioners, we anticipate that cesareandelivery will be the most commonprocedure elected in many situa-tions. In contrast to some types ofcategory III tracings in which theurgency of intervention may occa-sionally justify acceptance of somedegree of risk for trauma, the vastmajority of category II tracings inwhich delivery is indicated onlywarrant initiation of delivery within30 minutes of the decision fordelivery. A limited attempt at oper-ative vaginal delivery by an ex-perienced clinician may representoptimal care in some circumstances.However, the physician with limitedexperience in operative vaginal de-livery should not delay preparationsfor cesarean, nor persist in attemptsat operative vaginal delivery withoutprogressive descent with each con-traction. Without real expertise inoperative vaginal delivery, a deteri-orating category II FHRT will oftenbe best managed by prompt cesar-ean delivery.
12. The most vexing issue in the devel-opment of this algorithm was theissue of decreased vs absent vari-ability. We accept the accuracy ofdata concluding that FHR vari-ability must be absent to reliablyreflect a high degree of correla-tion with severe fetal acidemia.20,21
However, we caution against delay-ing delivery of a deteriorating FHRpattern because criteria indicatingprobable severe metabolic acidemiahave not yet been met. We havechosen to treat persistent minimaland absent variability as one for thefollowing reasons.
a. Variability cannot be consideredto be a strictly binary feature ofa FHR pattern. It is evident thata fetus with moderate vari-ability (thus excluding concur-rent fetal metabolic acidemia)

www.AJOG.org Obstetrics Clinical Opinion
that devolves to a state of frankasphyxia and severe metabolicacademia with absent variabilityas a result of episodes of intra-partum hypoxia must first passthrough a stage of minimalvariability, unless the deteriora-tion is abrupt and catastrophic asseen in a sentinel event.
b. While it is possible for apparentvariability to be exaggeratedwith the use of a first-genera-tion external, ultrasound-basedheart rate monitoring device,autocorrelation techniques em-ployed with most currentmonitoring systems have mini-mized this tendency.46 Unfortu-nately erratic signal detection ortransient artifact may give rise toperiods of apparent “minimalvariability” that could be falselyreassuring to some cliniciansand lead to delay in delivery. Iftechnically feasible, the fetuswith a category II pattern andpoor FHR signal quality shouldbe monitored with a fetal scalpelectrode.
c. An external FHR monitor thatyields a consistent high-qualitytracing, or a continuous fetalscalp lead tracing, will generallyallow the qualified clinician todistinguish different degrees ofvariability, even in the presenceof classic late or variable de-celerations. Unfortunately, sucha determination may be ren-dered more difficult by many ofthe category II patterns actuallyencountered in clinical practice.Such difficulties are especiallycommon in the presence ofatypical variable decelerations,in which determination of re-turn to baseline may be difficult.In such cases, a “baseline”apparently exhibiting some de-gree of variability may in factstill be a part of a recoveringdeceleration.
With exceptional expertise, most ofthese situations can be appropriatelydelineated. However, that level of
expertise is not universal among prac-ticing obstetricians. Indeed, even amongrecognized experts there is significantinterobserver variation in the differen-tiation of FHR patterns with minimal vsabsent variability.9 A basic principle ofany safety protocol is the direction ofsuch guidelines to the least, not thegreatest expected level of user compe-tence. Thus, we have used moderaterather than moderate or minimal vari-ability as a defining reassuring feature ofour algorithm. While we acknowledgethat such a decision will lead to inter-vention in cases that, in hindsight, mightbe proven to be unnecessary, we believethat following the algorithm as writtenwill avoid preventable neurologic injurydue to lack of intervention for a categoryII FHR pattern, and will be associatedwith an appropriate intervention rate.Cases of fetal hypoxia/acidemia duringlabor due to unexpected sentinel eventsremain largely unpreventable.38,39
13. A fetus presenting with persistentminimal to absent FHR variabilityand absent accelerations butwithout significant decelerationsposes a significant diagnostic andmanagement dilemma. In many ofthese cases, such a pattern repre-sents preexisting central nervoussystem injury with marked meta-bolic acidemia. In other cases, in-trauterine events leading to theinjury may have resolved (eg, um-bilical cord compression) and thefetus will have recovered metaboli-cally, but not neurologically. Devel-opmental anomalies unrelated tohypoxia/acidemia may give riseto a similar picture. Although thebenefit of cesarean delivery inimproving neurologic outcome insuch fetuses has never beendemonstrated, these fetuses may beless likely to tolerate the additionalhypoxia and acidemia that accom-panies even normal labor withoutintrapartum demise. In the absenceof significant decelerations however,the clinician may be assured thatwhile the fetus may be damaged, it isnot being damaged. Under thesecircumstances, a limited period of
AUGUST 2013 A
observation is appropriate, and isembraced in the algorithm.
14. The algorithm presented here rep-resents a consensus of the bestthoughts of 18 authors regard-ing one reasonable approach tocategory II FHR patterns given ourpresent scientific understanding.All authors are highly experiencedclinicians with significant peer-reviewed research experience andpublications in the area of fetalevaluation. They also represent abroad geographic spectrum andexperience in both the academicand private practice worlds andrepresent the disciplines of medi-cine, nursing, and midwifery. Assuch, it is reasonable for cliniciansto utilize this algorithm in themanagement of category II FHRpatterns; compliance with this pro-tocol is one way to meet thestandard of care in the UnitedStates. Importantly, as with mostother areas of medicine, the estab-lishment of this algorithm as oneway to comply with the standardof care does not exclude the exis-tence of other equally acceptableapproaches. While the authors uni-formly agree on the appropriatenessof this model for any laboringpatient, each of us can think ofnumerous situations in which al-ternative approaches to any branchof the algorithm would be equallyacceptable.
15. This algorithm is supported byavailable clinical experience, a sub-stantial body of basic science evi-dence, and indirect clinical data.Given the current state of obstetricknowledge, we do not believe it ispossible to simultaneously eliminatepreventable fetal neurologic injuryand significantly reduce the cesar-ean delivery rate for abnormal FHRpatternseseveral decades of suchattempts have resulted in the cur-rent state of Brownian motionin which neither goal has beenmeasurably achieved. Our goal indeveloping this algorithm has beento fix one variable in this equationby presenting an algorithm, which if
merican Journal of Obstetrics & Gynecology 95

Clinical Opinion Obstetrics www.AJOG.org
implemented as one component ofgood obstetrical care, will assist theclinician in avoiding preventableintrapartum fetal hypoxia, meta-bolic acidemia, and hypoxic injurybased on failure to deliver in the faceof certain persistent category II FHRpatterns. Of course, as with anyset of recommendations, clinicalstudies directly applying this algo-rithm both retrospectively to largeseries of category II patterns, andprospectively to large populations,are needed to potentially improvethe efficacy of the algorithm, and tobetter ascertain the actual inter-vention rate associated with itsapplication. It is anticipated thatsuch studies may facilitate refine-ment of this basic algorithm toreduce the intervention rate withoutincurring preventable morbidity ormortality.
16. Wemake no claim of the superiorityof this algorithm over other ap-proaches that might have beendeveloped. We began with thepremise that standardization andsimplification of critical care pro-cesses are fundamental principlesof patient safety. In virtually anyhuman endeavor, particularly onethat relies on the performance ofmultiple team members in an effortto achieve an optimal result, stan-dardization will yield improved re-sults.47-50 As such, unless one idealapproach to care has been demon-strated to be superior to all others byvirtue of well-performed clinicaltrials, it is not necessary to demon-strate the superiority of one specificapproach over others that are, whenconsidered individually, likely tobe equivalent. Rather, the adoptionby the clinical care team of oneappropriate specific managementplan will, by virtue of standardiza-tion alone, yield results superiorto those achieved by randomapplication of several individuallyequivalent approaches. This is par-ticularly true at the facility level.47-50
For example, protocols used toguide the provision of cardiopul-monary resuscitation have not been
96 American Journal of Obstetrics & Gynecology
demonstrated to be superior to allothers in randomized clinical tri-als.51 Yet the near universal adop-tion of these standard approacheshas resulted in improved outcomesfor cardiac arrest patients. Such al-gorithms have, over time, also un-dergone modification due toadvances in clinical understandingbased on new data. It is alsoimportant to note that in thisinstance, our algorithm does notseek to replace any establishedmethodical approach to the man-agement of category II patterns.Rather, we suggest that this algo-rithm will be helpful in the currentclinical setting in the United Statesin which a lack of clear direction hasled to divergent decision makingregarding cesarean section for FHRabnormalities.24
Adoption of this algorithm for themanagement of category II FHR patternsby the clinician is one approach toachieving compliance with the currentstandard of care. Application of thealgorithm, along with the integrationof future evidence-based modificationsdriven by additional research, willprovide clinicians with a standardized,simple, rational, evidence-based, andnationally accepted approach to themanagement of category II FHRpatterns. -
REFERENCES
1. Kubli FW, Hon EH, Khazin AF, Takemura H.Observations on heart rate and pH in the humanfetus during labor. Am J Obstet Gynecol 1969;104:1190-4.2. Meyers RE. Two patterns of brain damageand their conditions of occurrence. Am J ObstetGynecol 1972;112:246-51.3. Martin CB Jr, De Haan J, van der Wildt B,et al. Mechanisms of late decelerations in thefetal heart rate: a study with autonomic blockingagents in fetal lambs. Eur J Obstet GynecolReprod Biol 1979;9:361-73.4. Lee ST, Hon EH. Fetal hemodynamicresponse to umbilical cord compression. ObstetGynecol 1963;22:553-62.5. Haverkamp AD, OrleansM, Langendoerfer S,et al. A controlled trial of differential effects ofintrapartum fetal monitoring. Am J ObstetGynecol 1979;134:399-412.6. Banta HD, Thacker SB. Costs and benefitsof electronic fetal monitoring: a review of theliterature. April DHEW publication no. (PHS)
AUGUST 2013
79-3245. Hyattsville, MD: National Center forHealth Services Research, US Department ofHealth, Education, and Welfare; 1979.7. Freeman R. Intrapartum fetal monitoringeadisappointing story. N Engl J Med 1990;322:624-6.8. Chauhan SP, Klauser CK,Woodring TC, et al.Intrapartum nonreassuring fetal heart ratetracing and prediction of adverse outcome:interobserver variation. Am J Obstet Gynecol2008;198:623.9. Blackwell SC, Grobman WA, Antoniewitz L,et al. Interobserver and intraobserver reliabilityof the NICHD 3-tier fetal heart rate inter-pretation system. Am J Obstet Gynecol 2011;205:375.10. Spong KY, Berghella V, Wenstrom KD,Mercer BM, Saade GR. Preventing the first ce-sarean delivery. Obstet Gynecol 2012;120:1181-93.11. Clark SL, Hankins GDV. Temporal anddemographic trends in cerebral palsy: factand fiction. Am J Obstet Gynecol 2003;188:628-33.12. American College of Obstetricians andGynecologists and American Academy ofPediatrics. Neonatal encephalopathy and cere-bral palsy: defining the pathogenesis andpathophysiology. Washington, DC: AmericanCollege of Obstetricians and Gynecologists;2003.13. Avres-de-Campos D, Bernardes J. Twenty-five years after the FIGO guidelines for the use offetal monitoring: time for a simplified approach?Int J Gynaecol Obstet 2010;110:1-6.14. The National Institute of Child Healthand Human Development Research PlanningWorkshop. Electronic fetal heart rate moni-toring: research guidelines for interpretation.J Obstet Gynecol Neonatal Nurs 1997;26:635-40. (and in Am J Obstet Gynecol1997;177:1385-90.)15. The Royal Australian and New ZealandCollege of Obstetricians and Gynecologists.Intrapartum fetal surveillance: clinical guidelines,2nd ed. Victoria, Australia: RANZCOG; 2006.16. The Royal College of Obstetricians andGynecologists. Clinical guidelines on intra-partum fetal surveillance. London: RCOG Press;2001.17. Liston R, Sawchuck D, Young D. Fetalhealth surveillance: antepartum and intrapartumconsensus guideline. J Obstet Gynaecol Can2007;29(Suppl):S3-56.18. Parer JT, Ikeda T. A framework for stan-dardized management of intrapartum fetal heartrate patterns. Am J Obstet Gynecol 2007;197:26.e1-6.19. Elliot C,Warrick PA,GrahamE,Hamilton EF.Graded classification of fetal heart rate tracings:association with neonatal metabolic acidosisand neurologic morbidity. Am J Obstet Gynecol2010;202:258.e1-8.20. Macones GA, Hankins GD, Spong CY, et al.The 2008 National Institute of Child Health andHuman Development workshop report on elec-tronic fetal monitoring; update on definitions,

www.AJOG.org Obstetrics Clinical Opinion
interpretation and research guidelines. ObstetGynecol 2008;112:661-6.21. American College of Obstetricians andGynecologists. Management of intrapartumfetal heart rate tracings: ACOG practicebulletin no. 116. Obstet Gynecol 2010;116:1232-40.22. Jackson M, Holmgren CM, Esplin MS, et al.Frequency of fetal heart rate categories andshort-term neonatal outcome. Obstet Gynecol2011;118:803-8.23. Hamilton BE, Martin JA, Ventura SJ. Births:preliminary data for 2011. Natl Vital Stat Rep61;5:1-20.24. Clark SL, Belfort MA, Hankins GDV, et al.Variation in the rates of operative delivery in theUnited States. Am J Obstet Gynecol 2007;196:526-7.25. Simpson KR, James DC. Efficacy of intra-uterine resuscitation techniques in improvingfetal oxygen status during labor. Obstet Gynecol2005;105:1362-8.26. Hofmeyr GJ. Amnioinfusion for potentialor suspected umbilical cord compression inlabor. Cochrane Database Syst Rev 2005;2:CD001182.27. Garite TJ, Simpson KR. Intrauterine resus-citation during labor. Clin Obstet Gynecol 2011;54:28-39.28. Haydon M, Gorenberg D, Nageotte M, et al.The effect of maternal oxygen administration onfetal pulse oximetry during labor in fetuses withnon-reassuring fetal heart rate patterns. Am JObstet Gynecol 2006;195:735-8.29. Dildy GA III, Clark SL. Effects of maternaloxygen administration on fetal pulse oximetry.Am J Obstet Gynecol 2007;196:13-6.30. Clark SL, Belfort MA, Saade GA, et al.Implementation of a conservative, checklistbased protocol for oxytocin administration:maternal and fetal outcomes. Am J ObstetGynecol 2007;197:480.e1-5.
31. Clark SL, Rice-Simpson K, Knox E,Garite TJ. Oxytocin: new perspectives on anold drug. Am J Obstet Gynecol 2009;200:35.e1-6.32. Shankaran S, Laptook AR, Ehrenkrantz RA,et al.Whole-body hypothermia for neonateswithhypoxic-ischemic encephalopathy. N Engl JMed 2005;353:1574-84.33. Clark SL, GimovskyML, Miller FC. The scalpstimulation test: a clinical alternative to fetalscalp blood sampling. Am J Obstet Gynecol1984;148:274-7.34. Nageotte MP, Gilstrap LC. Intrapartum fetalsurveillance. In: Creasy RK, Resnik R, Iams JD,et al., eds. Maternal-fetal medicine, principlesand practice, 6th ed. Philadelphia: Saunders;2009.35. Cahill AG, Roehl KA, Odibo AO,Macones GA. Association of atypical deceler-ationswith acidemia. Obstet Gynecol 2012;120:1387-94.36. Hamilton E, Warrick P, O’Keefe D. Vari-able decelerations: do size and shape matter?J Matern Fetal Neonatal Med 2012;25:648-53.37. Zhang J, Landy HJ, Branch W, et al.Contemporary patterns of spontaneous laborwith normal neonatal outcomes. Obstet Gynecol2010;116:1281-7.38. Martinez-Biarge M, Madero R, Gonzalez A,Quero J, Garcia-Alix A. Perinatal morbidity andrisk of hypoxic-ischemic encephalopathy asso-ciated with intrapartum sentinel events. Am JObstet Gynecol 2012;206:148.e1-7.39. Nageotte MP, vander Waal B. Achievementof the 30 minute standard in obstetrics. Can itbe done? Am J Obstet Gynecol 2012;206:104-7.40. Leung AS, Leung EK, Paul RH. Uterinerupture after previous cesarean delivery:maternal and fetal consequences. Am J ObstetGynecol 1993;169:945-50.
AUGUST 2013 A
41. Oyelse Y, Ananth CV. Placental abruption.Obstet Gynecol 2006;108:1005-16.42. American College of Obstetricians andGynecologists. Practice bulletin no. 115: vaginalbirth after previous cesarean delivery. ObstetGynecol 2010;116:450-63.43. Cheng SL, Bautista D, Leo S, Sia TH.Factors affecting fetal bradycardia followingcombined spinal epidural for labor analgesia.J Anesth 2013;27:169-74.44. Hankins GD, Uckan E, Rowe TF, Collier S.Forceps and vacuum delivery: expectationsof residency and fellowship training programdirectors. Am J Perinatol 1999;16:23-8.45. Yeomans ER. Operative vaginal delivery.Obstet Gynecol 2010;115:645-53.46. Boehm FH, Fields LM, Hutchison JM,Bowen AW, VaughnWK. The indirectly obtainedfetal heart rate: comparison of first- and second-generation electronic fetal monitors. Am JObstet Gynecol 1986;155:10-4.47. Clark SL, Belfort MA, Meyers JA, et al.Improved outcomes, fewer cesarean deliveriesand reduced litigation: results of a new paradigmin patient safety. Am J Obstet Gynecol 2008;199:105.e1-7.48. Clark SL, Meyers JA, Frye DK, Perlin JA.Patient safety in obstetrics: the HospitalCorporation of America experience. Am JObstet Gynecol 2011;204:283-7.49. Institute of Medicine. To err is human:building a safer health care system.Washington,DC: National Academy Press; 2000.50. Institute of Medici Medicine. Crossing thequality chasm: a new health system for the 21stcentury. Washington, DC: National AcademyPress; 2001.51. Field JM, Hazinski MF, Sayre MR, et al. Part1: executive summary; 2010 American HeartAssociation guidelines for cardiopulmonaryresuscitation and emergency cardiovascularcare. Circulation 2010;122(Suppl):S640-56.
merican Journal of Obstetrics & Gynecology 97