Embed Size (px)
Citation preview
Implementation of an EmergencyDepartment–based Transient Ischemic AttackClinical Pathway: A Pilot Study in KnowledgeTranslationMichael D. Brown, MD, MSc, Mathew J. Reeves, PhD, Ted Glynn, MD, Arshad Majid, MD, Rashmi U. Kothari, MD
AbstractObjectives: To assess the feasibility of implementing an emergency department (ED)–based transientischemic attack (TIA) clinical pathway that uses computer-based clinical support, and to evaluate measuresof quality, safety, and efficiency.
Methods: This was a prospective cohort study of adult patients presenting to a community ED withsymptoms consistent with acute TIA. Adherence to the clinical pathway served as a test of feasibility.Compliance with guideline recommendations for antithrombotic therapy and vascular imaging wereused as process measures of quality. The 90-day risk of recurrent TIA, stroke, or death provided estimatesof safety. Efficiency was assessed by measuring the rate of uneventful hospitalization, defined as a hospitaladmission that did not result in any major medical event or vascular intervention such as endarterectomyor stent placement.
Results: Of the 75 subjects enrolled, physician adherence to the clinical pathway was 85.3%, and 35 patients(46.7%) were discharged home from the ED. Antithrombotic agents were prescribed to 68 (90.7%), andvascular imaging was performed in 70 (93.3%). The 90-day risk of recurrent TIA was seven out of 75(9.3%; 95% confidence interval [CI] = 4.6% to 18.0%), one patient experienced stroke (1.3%; 95% CI =0.2% to 7.2%), and three patients died (4.0%; 95% CI = 1.4% to 11.1%). Uneventful hospitalization occurredin 38 of 40 patients (95.0%).
Conclusions: Implementation of a clinical pathway for the evaluation and management of TIA usingcomputer-based clinical support is feasible in a community ED setting. This pilot study in knowledgetranslation provides a design framework for further studies to assess the safety and efficiency of astructured ED-based TIA clinical pathway.
ACADEMIC EMERGENCY MEDICINE 2007; 14:1114–1119 ª 2007 by the Society for Academic EmergencyMedicine
Keywords: TIA, transient ischemic attack, emergency department, clinical pathway
From the Grand Rapids MERC/Michigan State University
Program in Emergency Medicine (MDB), Grand Rapids, MI;
Departments of Epidemiology (MDB, MJR) and Neurology and
Ophthalmology (AM), Michigan State University, East Lansing,
MI; Michigan State University Emergency Medicine Residency
Program (TG), Lansing, MI; and Borgess Research Institute,
Michigan State University/Kalamazoo Center for Medical Stud-
ies (RUK), Kalamazoo, MI.
Received March 29, 2007; revision received April 25, 2007;
accepted April 25, 2007.
Supported by a grant from the Michigan State University Foun-
dation.
Contact for correspondence: Michael D. Brown, MD, MSc;
e-mail: [email protected].
ISSN 1069-6563
PII ISSN 1069-65635831114
Emergency physicians are frequently faced with anevaluation and disposition dilemma for patientspresenting with transient ischemic attack (TIA).
In the United States, the population rate of emergencydepartment (ED) visits for TIA is 1.1 per 1,000, and TIAis diagnosed in 0.3% of all ED visits.1 Although a numberof clinical practice guidelines for TIA have been pub-lished,2 there is considerable variability in adherenceto these recommendations with respect to diagnosticimaging, treatment with antiplatelet medications, andED disposition.1,3,4 Clinical decision rules for risk stratifi-cation have also been developed5; however, controversyregarding the appropriate interpretation of these rules inmaking disposition decisions persists.6 The purpose of
ª 2007 by the Society for Academic Emergency Medicine
doi: 10.1197/j.aem.2007.04.019

ACAD EMERG MED � November 2007, Vol. 14, No. 11 � www.aemj.org 1115
clinical practice guideline development is to improve theprocess and outcomes of health care and to optimize re-source utilization.7 If based on current and valid re-search, guidelines can provide a tool for the translationof research evidence into practice.7 However, knowledgetranslation does not occur by simply disseminatingguidelines or prediction rules in the form of publicationsor continuing medical education courses.8 Effectiveimplementation strategies at the local level are requiredif guidelines are to impact patient care.9 Developmentof a clinical pathway, taking into account local resourcesand attitudes, can provide clinicians with an organizedand sequenced clinical approach for complex entitiessuch as TIA.7 A beneficial effect of clinical pathways ismore likely when decision aids provide specific recom-mendations and are incorporated into clinicians’ work-flow using computer-based clinical support.10,11
We hypothesized that a structured clinical pathway uti-lizing computer-based clinical support to encourage im-mediate carotid vascular imaging would reduce hospitaladmissions without increasing the risk of recurrentTIA, stroke, or death following discharge. This pilotstudy was part of a demonstration project to determinethe feasibility of performing a large, multicenter, ran-domized trial designed to assess the safety and efficiencyof an ED-based TIA clinical pathway.
METHODS
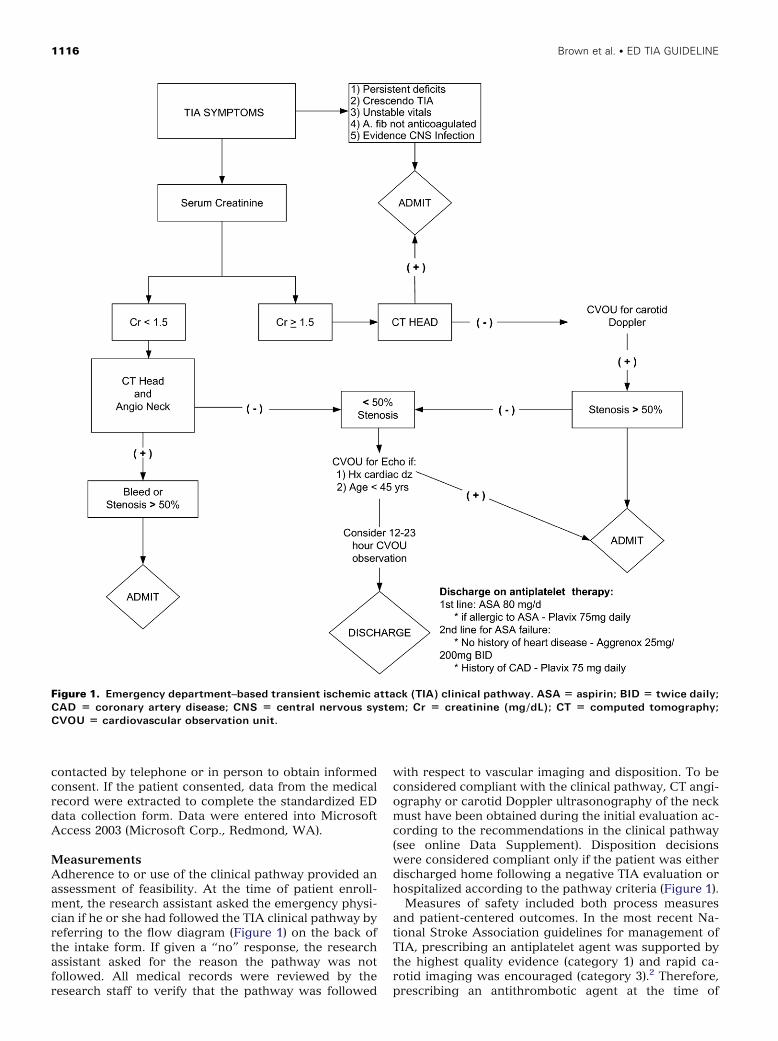
A multifaceted approach to knowledge translation wasutilized in the development and implementation of theED-based TIA clinical pathway.8 We made use of infor-mation published in TIA clinical guidelines and relevantsystematic reviews.12–15 Local emergency physicians,neurologists, and radiologists were involved in the devel-opment of the TIA clinical pathway, which was intro-duced and approved by the Department of EmergencyMedicine. Physician outreach methods used for localdissemination of the clinical pathway (Figure 1)included meetings, group e-mails, and posting the path-way on a point-of-care ED Intranet site (the completeTIA clinical pathway is available as an online DataSupplement at http://www.aemj.org/cgi/content/full/j.aem.2007.04.019/DC1).
To guide physicians through the clinical pathway, com-puter-based clinical support was implemented as a TIAorder set that included critical elements of the pathway.The TIA diagnostic tests were preset in the ED com-puter-based physician order entry system and includedbasic laboratory studies, electrocardiography, computedtomography (CT) of the head, and CT angiography of theneck. If any of the tests recommended in the clinical path-way were not indicated or desired, the physician had todeselect that option. Orders that were not preset butwere made available for selection within the TIA orderset included carotid Doppler ultrasonography, echocar-diography, aspirin, aspirin-dipyridamole combination,and clopidogrel.
Given the known increased risk of stroke over the first48 hours following a TIA,4,5,16 and the knowledge thatmedicolegal concerns are a barrier to guideline imple-mentation,8 the clinical pathway allowed for a 12- to 23-hour period of observation in the ED’s observation unit
if further studies such as echocardiography wereindicated or if the physician was uncomfortable withimmediate discharge home following a negative TIAevaluation.
Study DesignFollowing implementation of the TIA clinical pathway, aprospective cohort study was conducted to assess qualityof care and clinical outcomes of patients presenting tothe ED with suspected TIA. Similar to an impact analysisof a clinical decision rule in the real-world setting,10 wesought to assess the impact of the TIA clinical pathwayon patient safety and efficiency. This pilot study waspart of a demonstration project to assess the feasibilityof designing a multicenter study to validate a clinicalprediction rule and test the impact of a structured TIAclinical guideline. The study was approved by the institu-tional review boards of Spectrum Health and MichiganState University. Informed consent was obtained fromall participants before study enrollment.
Study Setting and PopulationThe study was conducted at a university-affiliated com-munity hospital with an ED census of approximately130,000 patient visits in 2006. Spectrum Health-Butter-worth is an urban teaching hospital with 30 emergencymedicine residents and 35 full-time attending physicians.Patients were enrolled for 14 months from July 2005 toAugust 2006.
The operational case definition of TIA included the fol-lowing three criteria: 1) an ED discharge diagnosis of TIAor an acceptable equivalent label of rule-out TIA, TIA/stroke, or unilateral weakness; 2) duration of symptomsless than 24 hours; and 3) no alternative final diagnosisprovided. Inclusion criteria therefore included the pre-sentation or recent history of focal acute stroke symp-toms (e.g., unilateral weakness or numbness, speechabnormality, or transient vision problems) that lastedless than 24 hours. Patients were excluded if they had sig-nificant cognitive impairments or other comorbidities(such as hearing loss) that would have prevented themfrom participating in a 90-day follow-up call.
Study ProtocolThe goal of the study was to enroll consecutive patientspresenting to the ED with signs and symptoms consistentwith TIA. The study made use of an existing stroke teamstructure that included 24-hour coverage by an ED phar-macist. The protocol for contacting the stroke team wasexpanded during the study period so that clinicianswere to contact the ED pharmacist for all patients withsuspected TIA. The ED pharmacist was responsible forscreening ED patients for eligibility and obtaining patientinformed consent.
Given that the goal was to obtain a consecutive sample,we anticipated that clinicians would fail to contact thestroke team for some patients with TIA, so the computer-ized medical record was screened by research staff forchief complaints consistent with possible TIA (i.e., TIA,rule-out TIA, TIA/stroke, unilateral weakness, speech im-pairment) every one to three days. The chart of any pa-tient identified as having a possible TIA was reviewed,and those meeting the inclusion criteria for TIA were
1116 Brown et al. � ED TIA GUIDELINE
Figure 1. Emergency department–based transient ischemic attack (TIA) clinical pathway. ASA = aspirin; BID = twice daily;
CAD = coronary artery disease; CNS = central nervous system; Cr = creatinine (mg/dL); CT = computed tomography;
CVOU = cardiovascular observation unit.
contacted by telephone or in person to obtain informedconsent. If the patient consented, data from the medicalrecord were extracted to complete the standardized EDdata collection form. Data were entered into MicrosoftAccess 2003 (Microsoft Corp., Redmond, WA).
MeasurementsAdherence to or use of the clinical pathway provided anassessment of feasibility. At the time of patient enroll-ment, the research assistant asked the emergency physi-cian if he or she had followed the TIA clinical pathway byreferring to the flow diagram (Figure 1) on the back ofthe intake form. If given a ‘‘no’’ response, the researchassistant asked for the reason the pathway was notfollowed. All medical records were reviewed by theresearch staff to verify that the pathway was followed
with respect to vascular imaging and disposition. To beconsidered compliant with the clinical pathway, CT angi-ography or carotid Doppler ultrasonography of the neckmust have been obtained during the initial evaluation ac-cording to the recommendations in the clinical pathway(see online Data Supplement). Disposition decisionswere considered compliant only if the patient was eitherdischarged home following a negative TIA evaluation orhospitalized according to the pathway criteria (Figure 1).
Measures of safety included both process measuresand patient-centered outcomes. In the most recent Na-tional Stroke Association guidelines for management ofTIA, prescribing an antiplatelet agent was supported bythe highest quality evidence (category 1) and rapid ca-rotid imaging was encouraged (category 3).2 Therefore,prescribing an antithrombotic agent at the time of
ACAD EMERG MED � November 2007, Vol. 14, No. 11 � www.aemj.org 1117
discharge from the ED or hospital was used as a processmeasure of quality. Although aspirin was recommendedas the first-line agent in the clinical pathway, acceptablealternatives included clopidogrel or aspirin-dipyridamolecombination for patients with aspirin failure and warfa-rin for those with atrial fibrillation.17 Our local TIA clini-cal pathway recommended CT angiography of the neckin patients with a creatinine level <1.5 mg/dL and no his-tory of contrast allergy or renal insufficiency; otherwise,carotid Doppler ultrasonography was suggested. Al-though the clinical pathway did not recommend vascularimaging if the patient recently had carotid imaging per-formed (within one year) or the patient was not a surgicalcandidate, we chose to use compliance with obtainingcarotid vascular imaging as a second process measureof quality. The patient-centered safety outcome was therisk of experiencing a recurrent TIA, stroke, or deathwithin 90 days of the initial ED visit. Follow-up was ob-tained by telephone interview or short mail question-naire; if both were unsuccessful, hospital medicalrecords and the social security death index weresearched for outcome events. All reported events wereconfirmed by review of the subject’s medical record.
Uneventful hospitalization was the primary measure ofefficiency and was defined as the proportion of admittedpatients who did not have any major medical event (i.e.,TIA, stroke, or death) or vascular intervention (i.e., end-arterectomy or cerebrovascular stenting) during theirhospitalization.
Data AnalysisStatistical analysis was performed based on simple pro-portions with 95% confidence intervals (CIs) calculatedusing the Wilson method in CI analysis (version 2.0;University of Southampton, Southampton, England).Descriptive statistics were performed using the SAS sta-tistical application program (version 9.1; SAS Institute,Inc., Cary, NC).
RESULTS
Characteristics of Study SubjectsThe study cohort included 75 patients presenting with amean age of 67.1 years (range, 19–100 years) and aneven distribution of men and women (Table 1). Follow-up at 90 days by telephone interview or mail was ob-tained on 64 of 75 patients (85.3%); for the 11 subjectswho did not respond to telephone or mail inquiries, fol-low-up was performed by medical record review and asearch of the social security death index.
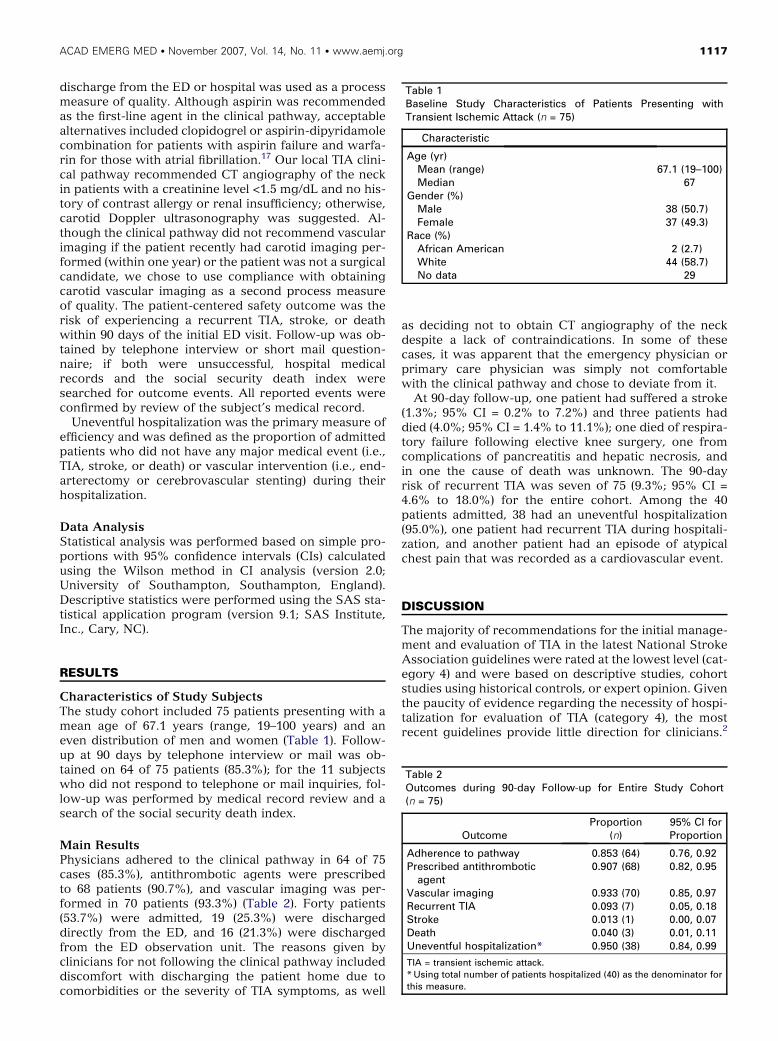
Main ResultsPhysicians adhered to the clinical pathway in 64 of 75cases (85.3%), antithrombotic agents were prescribedto 68 patients (90.7%), and vascular imaging was per-formed in 70 patients (93.3%) (Table 2). Forty patients(53.7%) were admitted, 19 (25.3%) were dischargeddirectly from the ED, and 16 (21.3%) were dischargedfrom the ED observation unit. The reasons given byclinicians for not following the clinical pathway includeddiscomfort with discharging the patient home due tocomorbidities or the severity of TIA symptoms, as well
as deciding not to obtain CT angiography of the neckdespite a lack of contraindications. In some of thesecases, it was apparent that the emergency physician orprimary care physician was simply not comfortablewith the clinical pathway and chose to deviate from it.
At 90-day follow-up, one patient had suffered a stroke(1.3%; 95% CI = 0.2% to 7.2%) and three patients haddied (4.0%; 95% CI = 1.4% to 11.1%); one died of respira-tory failure following elective knee surgery, one fromcomplications of pancreatitis and hepatic necrosis, andin one the cause of death was unknown. The 90-dayrisk of recurrent TIA was seven of 75 (9.3%; 95% CI =4.6% to 18.0%) for the entire cohort. Among the 40patients admitted, 38 had an uneventful hospitalization(95.0%), one patient had recurrent TIA during hospitali-zation, and another patient had an episode of atypicalchest pain that was recorded as a cardiovascular event.
DISCUSSION
The majority of recommendations for the initial manage-ment and evaluation of TIA in the latest National StrokeAssociation guidelines were rated at the lowest level (cat-egory 4) and were based on descriptive studies, cohortstudies using historical controls, or expert opinion. Giventhe paucity of evidence regarding the necessity of hospi-talization for evaluation of TIA (category 4), the mostrecent guidelines provide little direction for clinicians.2
Table 1Baseline Study Characteristics of Patients Presenting withTransient Ischemic Attack (n = 75)
Characteristic
Age (yr)Mean (range) 67.1 (19–100)Median 67
Gender (%)Male 38 (50.7)Female 37 (49.3)
Race (%)African American 2 (2.7)White 44 (58.7)No data 29
Table 2Outcomes during 90-day Follow-up for Entire Study Cohort(n = 75)
OutcomeProportion
(n)95% CI forProportion
Adherence to pathway 0.853 (64) 0.76, 0.92Prescribed antithrombotic
agent0.907 (68) 0.82, 0.95
Vascular imaging 0.933 (70) 0.85, 0.97Recurrent TIA 0.093 (7) 0.05, 0.18Stroke 0.013 (1) 0.00, 0.07Death 0.040 (3) 0.01, 0.11Uneventful hospitalization* 0.950 (38) 0.84, 0.99
TIA = transient ischemic attack.
* Using total number of patients hospitalized (40) as the denominator for
this measure.

1118 Brown et al. � ED TIA GUIDELINE
Therefore, we chose to use compliance with prescribingan antithrombotic agent as one process measure forquality, because this was one of the few recommen-dations supported by strong evidence (category 1).2
The 90.7% compliance with this recommendation com-pares favorably with historical data. In the United Statesduring the 1990s, only 25% of patients with TIA weregiven antiplatelet agents in the ED.1 According to a Ca-nadian registry database from 2000, 50% of the patientswith TIA discharged from the ED were prescribed antith-rombotic medication.4 The results of this single processmeasure imply that the quality of care delivered by fol-lowing a structured clinical pathway is high; however,given our observational study design, the high rate ofcompliance cannot be solely attributed to implementa-tion of the clinical pathway.
Urgent carotid imaging was integrated into the clinicalpathway because the information gained assists the clini-cian in making disposition decisions, and it has beenshown that patients undergoing endarterectomy farebetter if the procedure is performed early rather thanlater.5,18,19 Before implementation of the TIA clinicalpathway, vascular imaging by CT angiography of theneck was not routinely performed in our ED. Therefore,the 93% adherence to the vascular imaging processmeasure may be largely attributed to implementation ofthe clinical pathway but, was slightly less than the 97%rate of carotid imaging reported in a recent clinical trialusing an ED observation unit accelerated diagnosticprotocol.20
Based on multiple cohort studies in the United Statesand the United Kingdom, and registry data from Canada,the 90-day stroke risk among patients with TIA is consis-tently in the 9%–10% range.5,21 Although only one strokeevent was confirmed over the 90-day follow-up period,our estimates are imprecise due to the small samplesize and the upper limit of the 95% CI extending to 7%.The mortality of 4% during the 90-day follow-up wasslightly higher than the 2.6% death rate reported in thelarge prognosis study by Johnston et al.16 The sameprognosis study reported a 12.7% TIA recurrencerate,16 which is similar to our rate of recurrent TIA(9.3%).
In the United States, the rate of hospitalization overthe ten-year period from 1991 to 2001 was 54%, andalthough there were regional differences (68% in theNortheast), there was no evidence of a significant in-crease or decrease in admission rates over time.1 Theappropriateness of hospital admission for the evaluationof TIA continues to be debated, but there is littledisagreement that hospitalization is expensive.22,23 OurTIA clinical pathway recommended discharge homefollowing a negative TIA workup in the ED; however,the rate of hospitalization (53%) was not lower than thenational average over the past decade. However, basedon anecdotal reports, the hospitalization rate for TIA atlarger centers is much higher since the publication ofED-based studies that have raised awareness of the risksof stroke following TIA.16 Our rate of uneventful hospi-talization (95%) is difficult to interpret because thismeasure of efficiency has not been reported previously.Although the pathway allowed for a period of ED obser-vation if the physician was uncomfortable discharging
the patient home, this option was used in only 21% ofcases, and some clinicians still chose admission to thehospital despite a negative TIA evaluation. When theclinical pathway was disseminated, the importance ofusing good clinical judgment with application to the indi-vidual patient was stressed. It is possible that appropriatedeviation from the structured clinical pathway may haveactually improved patient safety.10 Another approach todecrease the rate of uneventful hospitalizations wouldbe to further risk stratify patients by integrating a clinicalprediction rule into the clinical pathway.5 However,given that no standardized approach can account for allof the nuances inherent in clinical practice, physiciansmust be allowed flexibility when applying an algorithmor rule to the individual patient.
LIMITATIONS
We had intended to perform a true inception cohortstudy and capture consecutive patients suspected ofTIA. Unfortunately, this was much more difficult than ex-pected. Based on retrospective review of ICD-9 codes, itwas apparent that a number of patients diagnosed withTIA over the study period were never approached for en-rollment. Not only did clinicians fail to contact the stroketeam for all suspected TIA cases, but our method ofscreening chief complaints for suspected TIA was inade-quate. The end result was a convenience sample ratherthan a consecutive sample; the effect of this bias on ourresults is uncertain. Future studies will need to better ad-dress this problem so that the study population repre-sents a true inception cohort.
The design of this observational study could not com-pensate for the Hawthorne effect with respect to themeasurement of adherence to the clinical pathway.24
The research staff was instructed to ask physicianswhether or not they followed the clinical pathway, whichmay have resulted in a bias toward a ‘‘yes’’ response.Although medical records were reviewed to verifyresponses and complete any missing information, thisverification process was also prone to error, because itwas done retrospectively. The 85% adherence to the clin-ical pathway is most likely inflated, and it is expected thatadherence may be less when implemented in othersettings.
Although making comparisons with historical datamay provide insight into the potential risk and benefitof implementing a TIA clinical pathway, any attempt toestimate measures of effect based on comparisons withhistorical controls would be inappropriate secondary toconfounding. Similarly, a before-after study designwould have allowed for a comparison in outcomes beforeimplementation of the clinical pathway with thosefollowing implementation, but this type of study designis also prone to bias, because many factors other thanthe intervention could account for changes in practicepatterns and patient outcomes. Therefore, a multi-institu-tional cluster-randomized study is the preferred trialdesign for testing the impact of a clinical pathway. Thelogistic and economic challenges for this type of studyare considerable, so planning the study design is para-mount.10,25
ACAD EMERG MED � November 2007, Vol. 14, No. 11 � www.aemj.org 1119
CONCLUSIONS
The results of this study should be interpreted within thescope of a pilot or fact-finding study paving way for alarger multicenter study. Implementation of an ED-basedTIA clinical pathway is feasible in a community ED set-ting, and it is possible to measure adherence to acceptedprocesses of care and assess the impact on efficiency andpatient safety.
The authors thank Jacque Perrin, BA, and the Spectrum HealthED pharmacists for their invaluable work in performing patientenrollment and data collection activities; Arya Khatiwoda andJulia Gargano for assistance with data analyses; and CatherinePuetz, MD, and Eugene Wiley, MD, for review and revision ofthe TIA Clinical Pathway at Spectrum Health.
References
1. Edlow JA, Kim S, Pelletier AJ, Camargo CA Jr.National study on emergency department visits fortransient ischemic attack, 1992-2001. Acad EmergMed. 2006; 13:666–72.
2. Johnston SC, Nguyen-Huynh MN, Schwarz ME, et al.National Stroke Association guidelines for the man-agement of transient ischemic attacks. Ann Neurol.2006; 60:301–13.
3. Chang E, Holroyd BR, Kochanski P, Kelly KD, ShuaibA, Rowe BH. Adherence to practice guidelines fortransient ischemic attacks in an emergency depart-ment. Can J Neurol Sci. 2002; 29:358–63.
4. Gladstone DJ, Kapral MK, Fang J, Laupacis A, Tu JV.Management and outcomes of transient ischemicattacks in Ontario. CMAJ. 2004; 170:1099–104.
5. Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al.Validation and refinement of scores to predict veryearly stroke risk after transient ischaemic attack.Lancet. 2007; 369:283–92.
6. Kernan WN. Stroke after transient ischaemic attack:dealing in futures. Lancet. 2007; 369:251–2.
7. Cook DJ, Greengold NL, Ellrodt AG, Weingarten SR.The relation between systematic reviews and practiceguidelines. Ann Intern Med. 1997; 127:210–6.
8. Lang ES, Wyer PC, Haynes RB. Knowledge transla-tion: closing the evidence-to-practice gap. AnnEmerg Med. 2007; 49:355–63.
9. Grol R, Grimshaw J. From best evidence to best prac-tice: effective implementation of change in patients’care. Lancet. 2003; 362:1225–30.
10. Reilly BM, Evans AT. Translating clinical researchinto clinical practice: impact of using prediction rulesto make decisions. Ann Intern Med. 2006; 144:201–9.
11. Kawamoto K, Houlihan CA, Balas EA, Lobach DF.Improving clinical practice using clinical decisionsupport systems: a systematic review of trials to iden-tify features critical to success. BMJ. 2005; 330:765.
12. Culebras A, Kase CS, Masdeu JC, et al. Practiceguidelines for the use of imaging in transient ische-mic attacks and acute stroke: a report of the StrokeCouncil, American Heart Association. Stroke. 1997;28:1480–97.
13. Agency for Healthcare Research and Quality. Effec-tiveness and Cost-Effectiveness of Echocardiographyand Carotid Imaging in the Management of Stroke,File Inventory, Evidence Report/Technology Assess-ment Number 49. AHRQ Publication No. 02-E022,Jul 2002. Rockville, MD: Agency for HealthcareResearch and Quality, 2002.
14. Tran H, Anand SS. Oral antiplatelet therapy in cere-brovascular disease, coronary artery disease, andperipheral arterial disease. JAMA. 2004; 292:1867–74.
15. Leonardi-Bee J, Bath PMW, Bousser M-G, et al. Dipy-ridamole for preventing recurrent ischemic strokeand other vascular events: a meta-analysis of individ-ual patient data from randomized controlled trials.Stroke. 2005; 36:162–8.
16. Johnston SC, Gress DR, Browner WS, Sidney S.Short-term prognosis after emergency departmentdiagnosis of TIA. JAMA. 2000; 284:2901–6.
17. Sacco RL, Adams R, Albers G, et al. Guidelines forprevention of stroke in patients with ischemic strokeor transient ischemic attack: a statement for health-care professionals. From the American Heart Associ-ation/American Stroke Association Council onStroke: co-sponsored by the Council on Cardiovascu-lar Radiology and Intervention: The American Acad-emy of Neurology affirms the value of this guideline.Stroke. 2006; 37:577–617.
18. Johnston SC. Clinical practice. Transient ischemicattack. N Engl J Med. 2002; 347:1687–92.
19. Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP,Barnett HJM. Endarterectomy for symptomatic ca-rotid stenosis in relation to clinical subgroups andtiming of surgery. Lancet. 2004; 363:915–24.
20. Ross MA, Compton S, Kilanowski P, Medado P,O’Neil B. An emergency department diagnostic pro-tocol for patients with transient ischemic attack: arandomized controlled trial [abstract]. Acad EmergMed. 2006; 13(Suppl 1):S8.
21. Hill MD, Yiannakoulias N, Jeerakathil T, Tu JV,Svenson LW, Schopflocher DP. The high risk ofstroke immediately after transient ischemic attack:a population-based study. Neurology. 2004; 62:2015–20.
22. Rothwell PM, Buchan A, Johnston SC. Recent ad-vances in management of transient ischaemic attacksand minor ischaemic strokes. Lancet Neurol. 2006; 5:323–31.
23. Gubitz G, Phillips S, Dwyer V. What is the cost ofadmitting patients with transient ischaemic attacksto hospital? Cerebrovasc Dis. 1999; 9:210–4.
24. Verstappen WH, van der Weijden T, ter Riet G,Grimshaw J, Winkens R, Grol RP. Block designallowed for control of the Hawthorne effect in a ran-domized controlled trial of test ordering. J Clin Epi-demiol. 2004; 57:1119–23.
25. Wright J, Bibby J, Eastham J, et al. Multifaceted im-plementation of stroke prevention guidelines in pri-mary care: cluster-randomised evaluation of clinicaland cost effectiveness. Qual Saf Health Care. 2007;16:51–9.