Embed Size (px)
Citation preview

H
IMPLEMENTING EVIDENCE-BASED GUIDELINES FOR
RADIOGRAPHY IN ACUTE LOW BACK PAIN:
A PILOT STUDY IN A CHIROPRACTIC COMMUNITY
Carlo Ammendolia, DC, MSc,a Sheilah Hogg-Johnson, PhD,b Victoria Pennick, RN, MHSc,c
Richard Glazier, MD, MPH,d and Claire Bombardier, MD, MScb
ABSTRACT
aCanadian MemWork & Health, T
b Institute for Woof Medicine, Toro
c Institute for WdUniversity of T
Canada.This research
Foundation for SpSubmit requests
Institute for WorkToronto, Ontarioiwh.on.ca).Paper submitted
2003.0161-4754/2004Copyright n 20doi:10.1016/j.jm
170
Objective: To evaluate the ability of a systematic educational intervention strategy to change the plain radiography
ordering behavior of chiropractors toward evidence-based practice for patients with acute low back pain (LBP).
Design: A quasi-experimental method was used comparing outcomes before and after the intervention with those of a
control community.
Setting: Two communities in southern Ontario.
Data Source: Mailed survey data on the management of acute LBP.
Outcome Measures: Plain radiography use rates for acute LBP based on responses to mailed surveys.
Results: Following the intervention, there was a 42% reduction in the self-report need for plain radiography for
uncomplicated acute LBP (P< .025) and a 50% reduction for patients with acute LBP < 1 month (P < .025) in the
intervention community. There was no significant change in the self-report need for plain radiography in the control
community (P > .05).
Conclusions: The educational intervention strategy used in this study appeared to have an effect in reducing the
perceived need for plain radiography in acute LBP. (J Manipulative Physiol Ther 2004;27:170-9)
Key Indexing Terms: Radiology; Chiropractic; Low Back Pain
INTRODUCTION
istorically, conventional radiography has been an
intregral part of chiropractic practice; yet, its
role remains controversial.1-3 This is particularly
true for the use of plain radiography for assessing patients
with back pain.4,5 National clinical guidelines on the
management of acute low back pain (LBP), including
orial Chiropractic College, and Institute fororonto, Ontario, Canada.rk & Health, and University of Toronto, Facultynto, Ontario, Canada.ork & Health, Toronto, Ontario, Canada.oronto, Faculty of Medicine, Toronto, Ontario,
was partially funded by the Chiropracticinal Research.for reprints to: Carlo Ammendolia DC, MSc,& Health 481 University Ave, Suite 800,M5G 2E9, Canada (e-mail: cammendol@
December 3, 2002; in revised form January 2,
/$30.0004 by National University of Health Sciences.pt.2003.12.021
the use of radiography, have been published in at least
11 countries since 1994.6 Recommendations on the use of
plain radiography are similar and suggest radiographs are
of limited value unless there are red flags present sugges-
tive of serious pathology, such as fracture, infection,
cancer, and inflammatory disease. Collectively, these con-
ditons are uncommon, representing less than 6% of all
causes of back pain.7,8
Despite the limited evidence for its use, studies of Ontario
and US chiropractors have demonstrated a high radiography
use rate for patients with acute low back pain, ranging from
58% to 92%.9-11
Unnecessary radiography use has implications for health
care costs and public safety. In 1991, an estimated $500
million was spent on low-back radiographs in the United
States,12 while in 1995, the Ontario Health Insurance Plan
spent over $16 million.13 Lumbar spine radiographs result in
one of the highest cumulative doses of radiation to the
reproductive organs of any radiological study.14 This expo-
sure increases the risk of cell mutation and cancer in this
highly susceptible tissue.15
In addition to their limited value, high cost, and potential
risks, a recent randomized control trial found lumbar spine

Fig 1. Questions pertaining to radiography use in survey.
Ammendolia et alJournal of Manipulative and Physiological TherapeuticsRadiography Guidelines and Acute LBPVolume 27, Number 3
171
radiographs were also associated with less favorable clin-
ical outcomes.16 Changing practice behavior is complex.
The publication and distribution of clinical practice guide-
lines do not appear to be sufficient to change practice
behavior.17-21 Strategies aimed at changing the use of
radiography for LBP in primary care toward an evidence-
based approach have had mixed results.22-26 Strategies that
appear to have some success are those that use multiple
interventions, such as audit and feedback and academic
detailing, and use opinion leaders and/or peers deemed to
be educationally influential to assist in the delivery of the
interventions.27,28
The purpose of this pilot study was to test the effec-
tiveness of a multifaceted educational intervention strategy
in reducing the perceived need for radiography use for
acute LBP among chiropractors in a select community
in Ontario.
METHODS
Research Design, Setting, and ParticipantsThe study design was quasi-experimental, comparing
outcomes before and after an educational intervention with
those of a concurrent control group. Data were collected
from chiropractors using surveys. Information from non-
responders was obtained via personal communication. Two
southern Ontario communities were involved in the study; 1
received the intervention and the other acted as a control
group. The communities were preselected by researchers at
the Institute for Work & Health (IWH) based on feasibility
factors surrounding implementation of an intervention for a
larger study.29 Each community had a population of ap-
proximately 100,000 with similar total labor force, unem-
ployment rate, and average income. All chiropractors in
each community were sent a survey. The chiropractors were
identified from the directory of the College of Chiropractors
of Ontario,30 the licensing body for Ontario chiropractors
which assigns all practicing chiropractors to a particular
community based on postal codes. There were 25 eligible
chiropractors in the intervention community and 21 in the
control community.
Preintervention Phase (July 1997 to January 1998)Description of surveys. Surveys were mailed to all chiroprac-
tors in each community. A modified Dillman mailing strat-
egy was used: 2 mailings (second mailing to nonresponders),

Table 1. Summary of survey respondents and participants in intervention community
Total no. of
Survey respondents
No. of chiropractors No. of chiropractors
No. of one to one chiropractor
chiropractors Pre Post Both in focus group at workshop Visits Phone
Intervention 25 19 14 14 7 9 17 1
Control 21 13 13 13 N/A N/A N/A N/A
Table 2. Comparison of personal and practice characteristics of responders and nonresponders to preintervention surveys inboth communities
Intervention Control
Characteristics Responders (n = 19) Nonresponders (n = 6) Responders (n = 13) Nonresponders (n = 8)
Age, mean years 41.3* 43.7 37.3 46.1z
Duration in practice, mean years 14.4* 16.5 11.2 17.3z
Year of graduation, % z 1983 42 50 69 43z
Male, % 79 67 77 88
Solo practice, % 68 33 31 50
Postgraduate training, % 50* 50 38 25
Teach chiropractic trainees, % 11* 0 15 0
Canadian Chiropractic College
graduate, %
95 100 77 100z
In-office radiography use, % 74 67 50y 63
*n = 18, y n = 12, and z n = 7 due to missing data.
Table 3. Personal and practice characteristics and the proportionof respondents who indicated they would use radiography forclinical vignette 1 using pooled data from both communities
Characteristics
Proportion of
respondents (n)
Year of graduation z 1983 0.59 (10)
Male 0.61 (14)
Solo practice 0.65 (11)
Postgraduate training 0.67 (10)
Inoffice radiography use 0.67 (14)
172 Journal of Manipulative and Physiological TherapeuticsAmmendolia et alMarch/April 2004Radiography Guidelines and Acute LBP
1 postcard reminder, and 2 telephone calls.31 The survey
instrument had been used in a previous study and pretested
for reliability (kappa 0.81) and content validity.9 For this
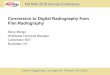
study, the questions of interest from the survey are described
in Figure 1.
Identification and training of educationally influential chiropractors.The preintervention survey also included a question used
to assist in the identification of local chiropractors that
were considered by their peers to be educationally
influential in the community. These individuals were to
be trained to assist in the delivery of the educational
intervention.
Focus group session. A focus group was conducted in the
intervention community to gather information on the views
and beliefs of the use of radiography. This information
was used to tailor a workshop and other components of
the intervention. Seven local chiropractors in the interven-
tion community participated in the focus group session.
Methods used for the focus group have been published
elsewhere.32
Intervention Phase (January 1998 to June 1998)Workshop. Since educationally influential chiropractors
were not identified, the workshop was conducted by the
principal investigator (PI ) (the first author). Nine (36%)
of the chiropractors in the intervention community
attended the workshop (Table 1). The 2-hour workshop
consisted of an interactive discussion led by the PI.
Important elements included feedback to the participants
on their community’s radiography use rate based on the
results of the preintervention surveys; a comparison of the
radiography use rates of other communities and that
suggested by the current literature; an introduction to a
decision aid tool to assist in determining the need for
radiography based on the presence of ‘‘red flags’’; and an
overview on the evidence for radiography use and the
associated potential risks. All participants were given a
take-home educational package containing information
presented at the workshop, including a summary of
radiography guidelines for acute LBP, letters from prom-
inant chiropractors endorsing the guidelines, a copy of the
decision aid tool, and key peer-reviewed articles and
reviews on radiography use for acute LBP.
Academic detailing. Following the workshop, the PI con-
tacted all chiropractors in the intervention community. A
total of 17 (68%) chiropractors agreed to meet individu-
ally with the PI to review and discuss the information

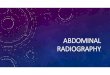
Fig 2. Focus group session; reasons given for taking radiographs for acute LBP.
Ammendolia et alJournal of Manipulative and Physiological TherapeuticsRadiography Guidelines and Acute LBPVolume 27, Number 3
173
presented at the workshop. Those who did not attend
the workshop were given a copy of the take-home
educational package. Eight chiropractors who could not
or were unwilling to meet with the PI or attend the
workshop were also sent a copy of the take-home educa-
tional package.
Media campaign. A news release was produced and later
published (June 1998) by a local newspaper in the
intervention community (Appendix 1). The news release
highlighted issues surrounding the overutilization of radi-
ography, with special emphasis on the potential risks
associated with unnecessary back radiographs. The goal
of the media campaign was to educate the public. Public
media campaigns have been demonstrated to be helpful
in improving general practitioner beliefs about back
pain.33
Postintervention Phase (June 1998 to October 1998)Postintervention surveys. Following the completion of the
intervention, postintervention surveys were mailed to both
communities (June and July 1998). The surveys and
mailing strategy were similar to that used in the pre-
intervention phase. A questionnaire evaluating the com-
ponents of the intervention was also mailed (October
1998) to all chiropractors in the intervention community
(Appendix 2). A total of 11 chiropractors responded to
the questionnaire.
AnalysisSurvey data. The proportion of survey respondents who
requested a radiograph for Clinical Vignette 1 (Fig 1)
before and after the intervention was compared with that
of the control community, using McNemar’s Exact Test
for correlated proportions.34 Only data from chiropractors
who responded to both preintervention and postinterven-
tion surveys were analyzed. The same test was used to
compare a change in the proportion of survey respondents
who agreed that a radiograph was useful in the diagnostic
workup of patients with acute LBP of less than 1-month
duration. Descriptive analyses were performed on personal
and practice characteristics of both communities using
preintervention and postintervention survey data. Similar
analyses were used to compare respondents and nonres-
pondents. A bivariate comparison was performed using
pooled preintervention data from both communities for
radiography use in uncomplicated acute LBP (Clinical
Vignette 1) and characteristics thought to influence radi-
ography use using the Fisher Exact Test.34
RESULTS
Baseline CharacteristicsA total of 19 (76%) eligible chiropractors in the
intervention community and 13 (62%) in the control
community responded to the preintervention surveys.
One survey returned from an inactive chiropractor was
excluded. A comparison of personal and practice charac-
teristics and answers to questions on x-ray use by the
respondents are summarized in Table 2. The mean age of
respondent chiropractors in the control community was
37.3 years compared with 41.3 in the intervention com-
munity. There was a proportionately higher number of
solo practitioners (68% versus 31%) and in-office radiog-
raphy facilities (74% versus 50%) in the intervention

Table 4. Change in the proportion of respondents to questions onradiography use in acute LBP in preintervention surveys comparedwith postintervention in both communities
Preintervention Postintervention P value
Intervention
Total respondents* 14 14
Radiography in
clinical vignette 1
Yes 9 (64.3) 3 (21.4) < .025
Radiography useful in
ALBP < 1 month
Agree 10 (71.4) 3 (21.4) < .025
Control
Total respondents* 13 13
Radiography in
clinical vignette 1
Yes 6 (46.2) 5 (38.5) > .05
Radiography useful in
ALBP < 1 month
Agree 6 (46.2) 8 (61.5) > .05
LBP, Low back pain, ALBP, acute low back pain.
* Includes respondents who completed both preintervention and post-intervention surveys.
174 Journal of Manipulative and Physiological TherapeuticsAmmendolia et alMarch/April 2004Radiography Guidelines and Acute LBP
community compared with the control community. With
respect to radiography use, 63% of the chiropractors in
the intervention community and 54% in the control
community requested a radiograph for the patient in
Clinical Vignette 1 (uncomplicated acute LBP of 1-week
duration). Radiography was considered useful in acute
LBP of less than 1-month duration (strongly agree or
agree) by 68% of the chiropractors in the intervention
community and 64% of the chiropractors in the control
community.
Less than 10% of chiropractors in the control community
and none in the intervention community stated they were
likely to use radiography for LBP because patients expected
them to do so.
In the bivariate analysis, none of the personal and practice
characteristics tested were found to be associated with
radiography use for uncomplicated acute LBP (Clinical
Vignette 1) when using pooled data from both communities
(Table 3).
When comparing preintervention survey respondents (n =
19) with nonrespondents (n = 6) in the intervention com-
munity, they appeared comparable in most characteristics,
except there were a proportionately higher number of solo
practitioners among respondents (68%) compared with
nonrespondents (33%). In the control community, survey
nonrespondents appeared to be older (by almost 10 years)
and have 20% more solo practitioners compared with
respondents (Table 2).
Educationally influential chiropractors could not be iden-
tified using the surveys. Very few responded to the question
regarding whom they seek for advice on the management of
low back pain. Of those who responded, no chiropractor
was mentioned more than once.
Focus Group SessionDetailed results and discussion of the focus group session
were recently published.32 Most of the chiropractors in the
focus group used plain radiography for reasons besides
ruling out pathology (Fig 2).
Change in Postintervention OutcomesPrimary outcome. There was a 64% response rate for the
postintervention surveys from the intervention community
and 62% from the control community. A total of 14 (56%)
and 13 (62%) respondents completed and returned both
preintervention and postintervention surveys from the
intervention and the control communities, respectively
(Table 4). In the intervention community, there was a
42.9% decrease in the proportion of respondents who
requested radiographs in Clinical Vignette 1 in the post-
intervention surveys compared with that in the prein-
tervention surveys. This difference was statistically
significant (P < .025). There was a 7.7% decrease in the
control community, which was not a statistically significant
change (P > .05).
Secondary outcome. There was a 50% decrease in the
proportion of respondents from the intervention commu-
nity who agreed that radiographs were useful in acute LBP
of less than 1-month duration, when compared with the
preintervention surveys. This was a statistically significant
decrease (P < .025). In the control community, there was a
15.3% increase, which was not statistically significant
(P > .05).
When comparing personal and practice characteristics of
respondents who completed and returned both preinterven-
tion and postintervention surveys in each community, the
differences noted were similar to those found in the
preintervention surveys (Table 5). When comparing
respondents with nonrespondents, the intervention com-
munity had similar characteristics. In the control commu-
nity, the same differences found in the preintervention
surveys were noted (Table 5). Characteristics among
respondents who reported high radiography use for Clin-
ical Vignette 1 at baseline and those who had a positive
response to the intervention for Clinical Vignette 1
appeared similar (Table 6).
There were 5 respondents in the intervention community
who completed the preintervention but not the postinterven-
tion surveys. Of these 5, 4 indicated they would request a
radiograph for Clinical Vignette 1 and also agreed that a
radiograph was useful in the diagnostic workup of patients
with acute LBP of less than 1-month duration. The remain-
ing respondent responded ‘‘no’’ to both questions. In the

Table 5. Comparison of personal and practice characteristics of responders and nonresponders to both preintervention andpostintervention surveys in both communities
Intervention Control
Characteristics Responders (n = 14) Non responders (n = 11) Responders (n = 13) Non responders (n = 8)
Age, mean years 44.9 41.8 37.3 46.1z
Duration in practice, mean years 17.3 15.7 11.2 17.3z
Year of graduation, % z 1983 43 45 69 43z
Male, % 86 73 77 88
Solo practice, % 57 55 31 50
Postgraduate training, % 43 64* 38 25
Teach chiropractic trainees, % 0 18* 15 0
Canadian Chiropractic College
graduate, %
100 91 77 100z
In-office radiography use, % 71 73 50y 63
*n = 10, y n = 12, z n = 7 due to missing data.
Table 6. Comparison of personal and practice characteristicsof respondents reporting high radiography use for clinical
Ammendolia et alJournal of Manipulative and Physiological TherapeuticsRadiography Guidelines and Acute LBPVolume 27, Number 3
175
control community, there were no preintervention respond-
ents lost to follow-up.
vignette 1 at baseline with those who had a positive response tothe interventionCharacteristics
High radiography
use clinical vignette
1 (n = 12)
Positive response
to intervention
(n = 6)
Age, mean years 41.7* 43
Duration in practice,
mean years
15.9* 16.7
Year of graduation,
% z 1983
42 67
Male, % 38 83
Solo practice, % 75 67
Postgraduate training, % 58* 50
Teach chiropractic
trainees, %
11* 15
Canadian Memorial
Chiropractic College
graduate, %
92 83
In-office radiography
use, %
75 67
*n = 11 due to missing data.
DISCUSSION
The results of this study suggest a high rate of use of
plain radiography for uncomplicated acute LBP in the 2
study communities. This finding is consistent with other
studies evaluating radiography use among chiroprac-
tors.9,10,35-38 This rate is also high compared with the
radiography use rates found among primary care physicians
for acute LBP9,10,39-41 and the rate expected when using
evidence-based guidelines.39-41 Although the rate of use is
lower, there are also concerns about inappropriate and
excessive use of radiography for LBP among primary care
physicians.10,41-44
The focus group session provided some insight into the
reasons for the high rate of radiography use (Fig 2).
Qualitative methods, such as the use of focus groups, can
often be used to complement quantitative research and are
well suited to helping understand beliefs and behaviors and
how and why decisions are made.45-47 Although all partic-
ipants in the focus group agreed that radiography use was
important to rule out pathology in acute LBP, the majority
felt there were other reasons to take radiographs, many
being unique to chiropractors using spinal manipulation.
However, there is no evidence to support the majority of
these other reasons.2,32,48-51
The positive results in this pilot study, a 43% (P < .025)
and 50% (P < .025) reduction in both primary and secondary
outcomes, respectively, suggest the educational intervention
in this study was successful in changing the self-reported
need for radiography use in acute LBP.
Other studies evaluating interventions to reduce radiog-
raphy ordering behavior among primary care practitioners
have had mixed results.22-26 There are no other known
community-based studies evaluating interventions to reduce
radiography among chiropractors.
Systematic reviews on implementation of clinical guide-
lines17-19,27,28,52 suggest that moderately effective interven-
tions include audit and feedback targeted to specific
providers and delivered by peers considered to be educa-
tionally influential. The most successful strategies appear to
use reminder systems, academic detailing, and/or consist of
multiple practice and community-based interventions.
In this study, it is not possible to determine which
component(s) of the intervention had the most influence
on the positive change seen in responses. The majority of
those who responded to the evaluation of the intervention
(Appendix 2) felt that each component (in which they
took part) was either useful or very useful. The only
exception was the news release, which most respondents
felt was either not very useful or they could not tell.

176 Journal of Manipulative and Physiological TherapeuticsAmmendolia et alMarch/April 2004Radiography Guidelines and Acute LBP
However, the apparent success of intervention was likely
due to the implementation of all the components together
as a complete strategy, as opposed to incorporating them
individually.
There are several methodological limitations in this pilot
study that may impact the validity of the results. Important
limitations include the lack of randomization and the small
number of study communities and participants. The 2
communities in this pilot study were preselected and
matched, which may affect the generalizability of the
results. In addition, since the intervention was communi-
ty-based, the effectiveness of the intervention would best be
tested using the community as the unit of analysis rather
than the individual chiropractors. However, a properly
matched comparison (matching communities on key attri-
butes) would require 48 matched pairs of communities to
achieve 80% power to detect a change in radiography use
from 0.70 to 0.40 with a type 1 error rate of 5%.53
Although this would provide sufficient statistical power
and a means for appropriate randomization, a project this
size may not be feasible.
An attempt was made to compare the 2 communities
for characteristics that independently might influence
radiography use. However, qualitative comparisons rather
than statistical significance were used due to a lack of
power.
Previous studies have suggested that solo practice,
radiography machine ownership, and less experienced
providers were associated with higher radiography
use.10,54 At baseline, chiropractors in the intervention
community were more experienced, had a higher number
of solo practitioners and ownership of radiography
machines, and took more radiographs compared with the
control community (Table 2). Similar differences were
noted among chiropractors who responded to both prein-
tervention and postintervention surveys (Table 5). These
trends suggested a bias in favor of higher radiography use
in the intervention community and appear to add support to
the results in this study.
Another potential study limitation was the use of self-
reported surveys as the sole data source. Data from the
surveys were not verified by objective means and may
not have reflected actual practice patterns. Recall bias,
misinterpretation of questions, wanting to please the PI,
or the nonspecific effect of being involved in the study
(the Hawthorne effect)55 may all have influenced the
responses, which may not have been a reflection of their
actual practice patterns. However, the use of clinical
vignettes have been demonstrated to be an effective and
useful tool for evaluating practice behavior and elicit-
ing practitioner attitudes and beliefs.56,57 Moreover, the
rate of radiography use estimated from the survey re-
sponses appeared consistent with those of other studies,
which further adds confidence to the validity of the pre-
intervention survey results.
Since the results of the primary and secondary outcomes
in this study were based on data from survey respondents, it
is not certain if there was a change in the perceived need for
radiographs among nonrespondents following the interven-
tion. However, in the intervention community, respondent
and nonrespondent characteristics appear comparable in
both preintervention and postintervention surveys. This
may help support the generalizibility of the results to the
intervention community as a whole.
CONCLUSION
The results of this pilot study suggest the multifaceted
intervention strategy used was successful in reducing the
self-reported need for radiology use in uncomplicated acute
LBP by chiropractors in a select community in Ontario.
Notwithstanding the limitations in this study, the positive
results suggest the need for further study. A large-scale,
randomized controlled trial, although desirable, would re-
quire an enormous effort and would likely not be feasible.
Well-conducted, small trials measuring actual practice out-
comes may be the more realistic alternative.
REFERENCES
1. Phillips RB. Plain film radiology in chiropractic. J Manipula-tive Physiol Ther 1992;15:47-50.
2. Mootz RD, Hoffman LE, Hansen DT. Optimizing clinical useof radiography and minimizing radiation exposure in chiro-practic practice. Top Clin Chiropr 1997;4:34-44.
3. Ernst E. Chiropractor’s use of x-rays. BMJ 1998;71:248-51.4. Phillips RB, Frymoyer JW, MacPherson BV, Newburg AH.
Low back pain: a radiographic enigma. J Manipulative PhysiolTher 1986;9:183-7.
5. Phillips RB, Howe JW, Bustin G, Mick TJ, Rosenfeld I, MillsT. Stress x-rays and the low back pain patient. J ManipulativePhysiol Ther 1986;9:1127-33.
6. Koes B, van Tulder M, Ostelo R, Burton K, Waddell G. Clin-ical guidelines for the management of low back pain in pri-mary care. Spine 2001;26:2504-14.
7. Deyo RA, Weinstein JN. Low back pain. N Engl J Med2001;344:363-70.
8. Liang M, Komaroff AL. Roentgograms in primary care in lowback pain: a cost effectiveness analysis. Arch Intern Med1982;142:1100-12.
9. Aker P, Bombardier C, Jansz G, Bressler H. Chiropractic man-agement of low back pain: a survey of Ontario chiropractors.Presented at the Second International Forum for Primary CareResearch on Low Back Pain; May 30-31, 1997; The Hague,The Netherlands.
10. Carey TS, Garrett J. North Carolina back pain project. Patternsof ordering diagnostic tests for patients with acute low backpain. Am Coll Physicians 1996;125:807-13.
11. Cherkin CD, MacCornack FA, Berg AO. Managing lowback pain–a comparison of the beliefs and behaviours offamily physicians and chiropractors. West J Med 1988;149:475-80.
12. Russo R, Cook P. Diagnosis of low back pain: role of imagingstudies. Occup Med 1998;13:83-96.

Ammendolia et alJournal of Manipulative and Physiological TherapeuticsRadiography Guidelines and Acute LBPVolume 27, Number 3
177
13. Anderson G. Presentation of OHIP data on lumbar spineimaging. Institute for Work & Health; March 19, 1996;Toronto, Canada.
14. Maravilla KR, Cohen WA, Wessbecher FW. Imaging studiesin the assessment of low back pain. Neurosurg Clin N Am1991;2:817-22.
15. Owens JP, Rutt G, Keir MJ, Spencer H, Richardson D,Richardson A, et al. Survey of general practitioners’ opinionson the role of radiology in patients with low back pain. Br JGen Pract 1990;40:98-101.
16. Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R,Pringle M. The role of radiography in primary care patientswith low back pain of at least 6 weeks duration: a rando-mised (unblinded) controlled trial. Health Technol Assess2001;5:1-69.
17. Davis D, Taylor-Vaisey A. Translating guidelines into practice.Can Med Assoc J 1997;157:408-16.
18. Lomas J. Teaching old (and not so old) docs new tricks: ef-fective ways to implement research findings. CHEPAworkingpaper series no. 93-4. Hamilton, Ontario, Canada: McMasterUniversity; 1993.
19. Lomas J, Haynes RB. A taxonomy and critical review oftested strategies for the application of clinical practice recom-mendations: from ‘‘official’’ to ‘‘individual’’ clinical policy.Am J Prev Med 1988;4(Suppl 4):72-94.
20. Haynes RB. Some problems in applying evidence in clinicalpractice. Ann N Y Acad Sci 1993;703:210-25.
21. The Lancet editorial. Lancet 1998;351:997.22. Oakeshott P, Kerry SM, Williams JE. Randomized controlled
trial of the effect of the Royal College of Radiologists’ guide-lines on general practitioners’ referrals for radiographic exam-ination. Br J Gen Pract 1994;44:197-200.
23. Freeborn DK, Shye D, Mullooly JP, Eraker S, Romeo J.Primary care physicians’ use of lumbar spine imaging tests.J Gen Intern Med 1997;12:619-25.
24. Cherkin D, Deyo RA, Berg AO, Bergman JJ, Lishner DM.Evaluation of a physician education intervention to improveprimary care for low-back pain I: impact on physicians. Spine1991;16:1168-72.
25. Kerry S, Oakeshott P, Dundas D, Williams J. Influnce of postaldistribution of The Royal College of Radiologists’ guidelines,together with feedback n radiological referral rates, on x-rayreferrals from general practice: a randomised controlled trial.Fam Pract 2000;17:46-52.
26. Eccles M, Steen N, Grimshaw J, Thomas L, McNamee P,Soutter J, et al. Effect of audit and feedback, and remindermessages on primary care radiology referrals: a randomizedtrial. Lancet 2001;357:1406-9.
27. Jamtvedt G, Young JM, Kristoffersen DT, Thomson O’BrienMA, Oxman AD. Audit and feedback: effects on the profe-ssional practice and health care outcomes (Cochrane Re-view). In: The Cochrane Library, issue 1. Chichester, UK:John Wiley & Sons; 2004.
28. Thomson O’Brien MA, Oxman AD, Davis DA, Haynes RB,Freemantle N, Harvey EL. Educational outreach visits: effectson professional practice or patient outcomes (Cochrane Re-view). In: The Cochrane Library, issue 1. Chichester, UK: JohnWiley & Sons; 2004.
29. Guzman J. Development and initial evaluation of an evidence-based in-office decision aid to improve the assessment andtreatment of patients with acute low back pain in primary carepractice: the Peterborough back rules template [master of sci-ence thesis]. Toronto: University of Toronto; 1999.
30. College of Chiropractors of Ontario. Directory 1996. Ontario,Toronto, Ontario: College of Chiropractors of Ontario; 1996.
31. Dillman A, Christenson J, Carpenter E, Brooks R. Increasingmail questionnaires response: a four state comparison. AmSociol Rev 1974;39:744-56.
32. Ammendolia C, Bombardier C, Hogg-Johnson S, Glazier R.Views on x-ray use in patients with acute low back painamong chiropractors in an Ontario community. J ManipulativePhysiol Ther 2002;25:511-20.
33. Buchbinder R, Jolley D, Wyatt M. Population based interven-tion to change back pain beliefs and disability: three partevaluation. BMJ 2001;322:516-20.
34. Rosner B. Fundamentals of biostatistics. 4th ed: Belmont(CA): Wadsworth Publishing Company; 1995. p. 379.
35. Plamindon RL. Summary of 1994 ACA statistical study. LatAm Chiropr Assoc 1995;32:57-63.
36. Hurwitz EL, Coulter ID, Adams AH, Genovese BJ, ShekellePG. Use of chiropractic services from 1985 through 1991 inthe United States and Canada. Am J Public Health 1998;88:771-6.
37. Petersen P. A survey of chiropractic practice in Europe. Eur JChiropr 1994;42:3-28.
38. Assendelft WJJ, Pfeifle ChE, Bouter LM. Chiropractic in theNetherlands: a survey of Dutch chiropractors. J ManipulativePhysiol Ther 1995;18:129-39.
39. Frazier LM, Carey TS, Lyles MF, Khayrallah MA, McGaghieWC. Selective criteria may increase lumbosacral spine roent-genogram use in acute low-back pain. Arch Intern Med1989;149:47-50.
40. Schroth WS, Schectman JM, Elinsky EG, Panagides JC. Uti-lization of medical services for the treatment of acute low backpain. Conformance with clinical guidelines. J Intern Med1992;17:486-91.
41. Suarez-Almazor ME, Belseck E, Russell AS, Mackel JV. Useof lumbar radiographs for the early diagnosis of low backpain. Proposed guidelines would increase utilization. JAMA1997;227:1782-6.
42. Deyo RA. Early diagnostic evaluation of low back pain. J GenIntern Med 1986;1:328-38.
43. Ferriman A. Early x-rays for low back pain confers little ben-efit. BMJ 2000;321:1489.
44. Espeland A, Baerheim A, Albrektsen G, Korsbrekke K, LarsenJ. Patients’ views on the importance and usefulness of plainradiography for low back pain. Spine 2001;26:1356-63.
45. Kingry MJ, Tiedje LB, Friedman LL. Focus groups: a researchtechnique for nursing. Nurs Res 1990;39:124-5.
46. Quandt SA, Arcury TA. Qualitative methods in arthritis re-search: overview and data collection. Am J Rheumatol 1997;10:273-81.
47. Pope C, Mays N. Reaching the parts other methods cannotreach: an introduction to qualitative methods in health andhealth services research. Br Med J 1995;311:42-45.
48. Taylor JAM, Resnick D. Imaging decisions in the manage-ment of low back pain. In: Advances in chiropractic. Vol. 1St. Louis: Mosby; 1994. p. 1-20.
49. van Tulder MW, Assendelft WJJ, Koes BW, Bouter LM. Spinalradiographic findings and non-specific low back pain: a sys-tematic review of observational studies. Spine 1997;22: 427-34.
50. Gatterman M. Standards of practice relative to complicationsof and contraindications to spinal manipulative therapy. J CanChiropr Assoc 1991;35:232-6.
51. Bigos SJ, Bowyer OR, Braen GR, Brown K, Deyo R,Haldeman S, et al. Acute low back problems in adults. Rock-ville (MD): Agency for Health Care Policy and Research,Public Health Service, US Department of Health and HumanServices; 1994. Clinical practice guideline no. 14.
52. Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD,

178 Journal of Manipulative and Physiological TherapeuticsAmmendolia et alMarch/April 2004Radiography Guidelines and Acute LBP
Thomson MA. Closing the gap between research and practice:an overview of systematic reviews of interventions to promotethe implementation of research findings. BMJ 1998;317:465-8.
53. Green SB, Corle DK, Gail MH, Mark SC, Pee D. Interplaybetween design and analysis for behavioral intervention trialswith community as the unit of randomization. Am J Epidemiol1995;142:587-93.
54. Childs AW, Hunter ED. Non-medical factors influencing useof diagnostic x-ray by physicians. Med Care 1972;X:323-35.
APPENDIX 1.News release sent to local newspapers
55. Parson HM. What happened at Hawthorne? Science 1974;193:922-932.
56. Jones TV, Gerrity MS, Earp J. Written case simulations: dothey predict physicians’ behaviour? J Epidemiol 1990;43:805-15.
57. Langley GR, Trichler DL, Llewellyn-Thomas HA, Till JE.Use of written cases to study factors associated with re-gional variations in referral rates. J Clin Epidemiol 1991;44:391-402.

APPENDIX 2.
Evaluation of the components of the intervention
Ammendolia et alJournal of Manipulative and Physiological TherapeuticsRadiography Guidelines and Acute LBPVolume 27, Number 3
179