Embed Size (px)
Citation preview

Implementing Potentially Better Practices for Improving Family-CenteredCare in Neonatal Intensive Care Units: Successes and Challenges
Kimberly A. Cisneros Moore, RNC, BSN*; Kara Coker, RN, MSN‡; Allison B. DuBuisson, MS§;Betsy Swett, RNC�; and William H. Edwards, MD¶
ABSTRACT. Objective. Multidisciplinary teams from11 medical center neonatal intensive care units collabo-rated in a quality improvement project with a focus onfamily-centered care.
Methods. Through a process of self-analysis, litera-ture review, benchmarking site visits, and expert consul-tation, 10 potentially better practice (PBP) areas weredefined. Improvement activities in 4 of the 10 areas aregiven as examples of successes and challenges that indi-vidual centers encountered. The 4 areas are vision andphilosophy, unit culture, family participation in care, andfamilies as advisors.
Results. Centers were at different places for all of thePBPs at the beginning and throughout the collaboration.Seven centers developed or revised their vision or phi-losophy of care statements about family-centered care.Incorporating the vision and philosophy of care intoperformance appraisals, hiring of new personnel, andchanging unit culture to a more family-centered practicewere more challenging than developing the statements.Full parent participation in care requires unrestrictedaccess to the neonatal intensive care unit. The shift fromconsidering parents to be “visitors” to being partners incaring for their child was more difficult for centers withrestricted visitation policies. All centers developed, ex-panded, or started plans for establishing family advisorycouncils. The experience of 2 centers is described.
Conclusions. Family-centered care is more of a jour-ney than a destination. Collaborating centers in thisproject found themselves at different places in that jour-ney. Through perseverance in implementing the PBPs,all have moved further along the path. Pediatrics2003;111:e450–e460. URL: http://www.pediatrics.org/cgi/content/full/111/4/e450; family-centered care, parental in-volvement, parent advisory council, collaborative qualityimprovement, multidisciplinary, neonatal intensive care,NIC/Q 2000.
ABBREVIATIONS. NICU, neonatal intensive care unit; NIC/Q2000, Neonatal Intensive Care Unit Quality Improvement Collab-orative Year 2000; PBPs, potentially better practices.
KEY POINTS OF ARTICLE• Family-centered care is less a destination than a
journey.• Neonatal intensive care units (NICUs) that are
seeking to provide family-centered care may beginat very different places and proceed along differ-ent paths.
APPLYING LESSONS LEARNED TO PRACTICE• Family-centered care vision and philosophy of
care statements are meaningful only when theyare incorporated into the culture and daily prac-tice of the NICU.
• Families can be effective partners both in caringfor their own child and in providing advice toimprove care in NICUs.
Eleven centers that participated in the VermontOxford Network Neonatal Intensive Care UnitQuality Improvement Collaborative Year 2000
(NIC/Q 2000) chose to focus on family-centered careas a strategy to improve the care of infants in NICUsand their families. The project was supported bycollaboration with the Institute for Family-CenteredCare. Through a process of self-analysis, literaturereview, benchmarking site visits, and expert consul-tation, potentially better practices (PBPs) were de-fined.1 In this article, some of the successes and chal-lenges encountered by the centers as theyimplemented these practices are described. Exam-ples are taken from 4 of the 10 PBP content areas:vision and philosophy, unit culture, family partici-pation in care, and families as advisors.
VISION AND PHILOSOPHY• Vision and philosophy of care statements articu-
late the unit’s commitment to family-centeredcare.
• Family-centered vision and philosophy is consis-tently applied to unit policies, practices, and pro-grams.
A vision and/or a philosophy of care statementthat incorporates the principles of family-centeredcare provides a foundation for a NICU’s policies,decisions, goals, and new directions. Without a vi-sion and core belief system, the culture has no cleardirection. This can result in inconsistent family-cen-tered care practices and decision making. The impor-tance of an expressed vision or philosophy of carewas evident at all benchmark site visits as well as in
From the *Children’s Hospital at Providence Alaska Medical Center, An-chorage, Alaska; ‡DeVos Children’s Hospital, Grand Rapids, Michigan;§Women’s Hospital of Greensboro, Greensboro, North Carolina; �Woman’sHospital, Baton Rouge, Louisiana; and ¶Children’s Hospital at Dartmouth,Lebanon, New Hampshire.Received for publication Aug 13, 2002; accepted Oct 24, 2002.Address correspondence to William H. Edwards, MD, Children’s Hospitalat Dartmouth, One Medical Center Dr, Lebanon, NH 03756-0001. E-mail:[email protected] (ISSN 0031 4005). Copyright © 2003 by the American Acad-emy of Pediatrics.
e450 PEDIATRICS Vol. 111 No. 4 April 2003 http://www.pediatrics.org/cgi/content/full/111/4/e450 by guest on July 8, 2018www.aappublications.org/newsDownloaded from

published reports.1,2 The 11 centers in the family-centered care focus group started the project at dif-ferent places for this practice. Some had already de-veloped statements, others developed or revisedthem during the project, and some were still workingon them at project end. The individual vision andphilosophy statements from 7 centers are included inAppendix A.
Yakima Valley Memorial Hospital developed itsvision statement as part of this quality improvementproject. After discussion and brainstorming, a mul-tidisciplinary committee that included families pro-posed several potential statements. Keeping the vi-sion statement short and concise was a priority. Thestatements were widely presented for input and dis-cussion by nursery staff, physicians, and families,and a single choice was made by consensus. Theproposed statement was then communicated to nurs-ery personnel for input by a variety of mechanisms.A banner of the proposed statement was displayedin the NICU and conference room. Newsletters andbulletin boards were dedicated to development ofthe statement. Over 2 weeks, written and verbalfeedback was sought and comments were tran-scribed onto a board for communications about cur-rent issues. All feedback was reviewed, and the state-ment was revised into its current version: “Memorialand families: Partners in care.” It is especially appro-priate that the idea for this vision statement origi-nated with a comment from a mother who describedthe neonatal care team as being “partners in caringfor her infant.”
After creating the vision statement, the YakimaValley Memorial improvement team took steps tomake it a part of their culture. They incorporated thevision statement on paperwork used for the unit,including meeting agendas and minutes and statio-nery letterheads. They mailed information about thevision to all nursery staff and placed signs with thevision statement in various places throughout theunit. When a planned survey was conducted of allnursery personnel, 80% both knew the unit had avision statement and were able to state it.
The philosophy of care statement devised by theNICU at Fairview University Medical Center reflectsthe key principles of family-centered care: “We rec-ognize the family is the most important and constantfactor in each infant’s life. Our goal is to establish acollaborative partnership between parents and thehealth care team to promote communication, respectdiversity, and empower families.”
The Fairview team used the process of developingtheir philosophy of care statement and incorporatingit into the NICU’s policies and parent information tostimulate ideas for promoting family-centered care.One outcome measure for this improvement projectwas that 86% of nursery staff were able to giveexamples of ways they could promote family-cen-tered care.
The Children’s Hospital at Providence AlaskaMedical Center had created a vision statement beforethis project. Although it existed on paper, it was nota living document in the NICU. The DevelopmentalCare Council, the Family Advisory Board, and the
Parent and Community Coordinator (a paid parentposition) together analyzed and rewrote the visionstatement, drawing from insights gained during thebenchmarking visits and the development of the 10PBPs. A professionally designed poster of the newvision and mission statements was prominentlyplaced at the main entrance to the NICU. The family-centered vision and mission statements are now im-portant components for hiring new personnel. Poten-tial employees are asked to “define family-centeredcare” during the interview process. Including family-centered care as a key competence in staff perfor-mance appraisals led to counseling some staff torelocate to other positions within the hospital. Thecommitment to a family-centered care philosophyhas not been easy.
UNIT CULTURE• Vision and philosophy of care statements are de-
veloped collaboratively by representatives of alldisciplines working on the unit and by familyrepresentatives.
• Committees that develop programs and practiceshave members who represent all disciplines work-ing on the unit, and family representatives.
• Accountability for patient and family outcomes isshared by all unit staff.
The process of developing a vision or philosophyof care statement can be a positive affirmation of thecore beliefs of a NICU. Once developed, the chal-lenge is to compare systematically current realitywith the ideal and make improvements until thevision and philosophy accurately reflect the NICU’sculture. This PBP concept naturally follows and over-laps with vision and philosophy.
Presbyterian St. Luke’s Medical Center in Denver,Colorado, confronted a substantial barrier to imple-menting family-centered care. Two different unitsproviding neonatal care within the center each hadseparate staffing and different goals. Communica-tion between the 2 units was poor, and project lead-ers sensed a general apathy about implementingfamily-centered care in both. They formed a multi-disciplinary committee called INFO (ImplementingNeonatal and Family Outcomes) drawn from thestanding committees of both units. The purpose ofINFO was to find ways to bring family-centered careprinciples back to the standing committees. Collab-oration between the 2 units was further enhanced byestablishing daily meetings between the 2 units andsetting up e-mail accounts for every staff member.Signs of a positive effect have been an increase instaff involvement in committees and projects and arenewed enthusiasm for providing primary carenursing.
At the Children’s Hospital at Dartmouth, it wasrecognized that ongoing family input into all aspectsof unit operations, policies, and practices was a nat-ural evolution of the concept of considering familiesas true collaborators in care. The way in which theparent advisory council was included in the admin-istrative structure of the unit is a strong statement ofthe belief in partnership. The parent council has been
http://www.pediatrics.org/cgi/content/full/111/4/e450 e451 by guest on July 8, 2018www.aappublications.org/newsDownloaded from
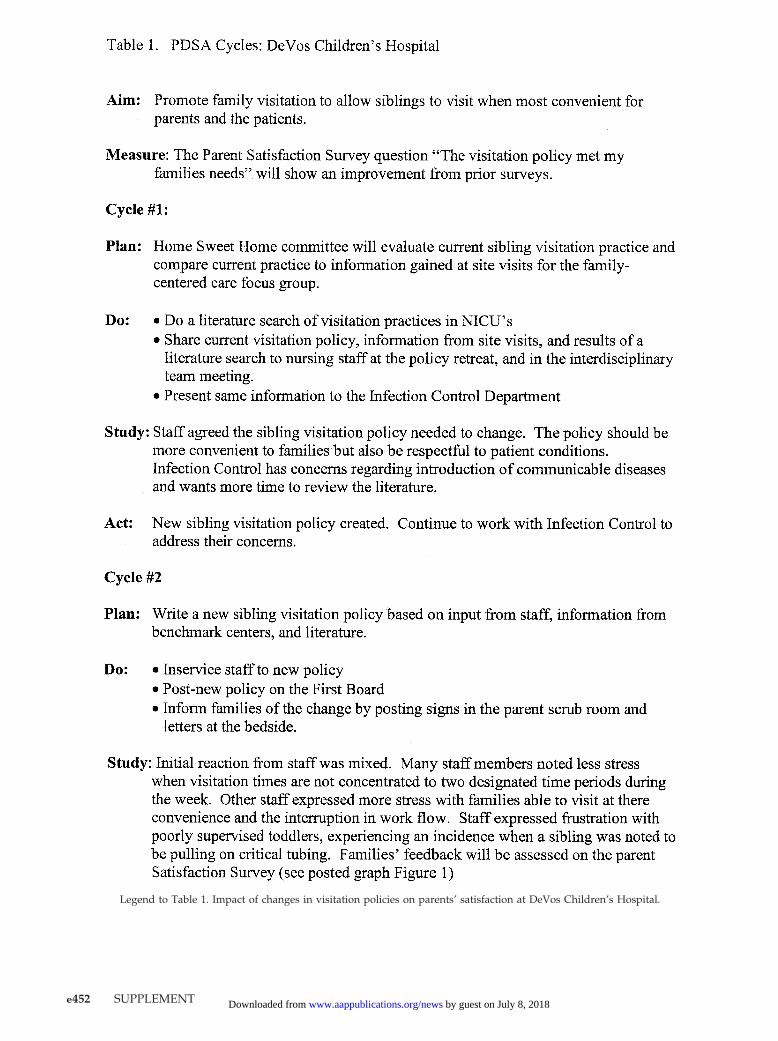
Legend to Table 1. Impact of changes in visitation policies on parents’ satisfaction at DeVos Children’s Hospital.
e452 SUPPLEMENT by guest on July 8, 2018www.aappublications.org/newsDownloaded from
incorporated and voted into the by-laws as an equalpartner in the intensive care nursery shared gover-nance model. The chair of the parent council is avoting member of the coordinating council, com-posed of the chairs of each of the shared governancecouncils and the unit nursing and medical directors.
FAMILIES’ PARTICIPATION IN CARE• Families are viewed as integral members of the
care team and as primary caregivers to their in-fants (not as visitors).
• Families are seen as the primary decision makersfor their infants.
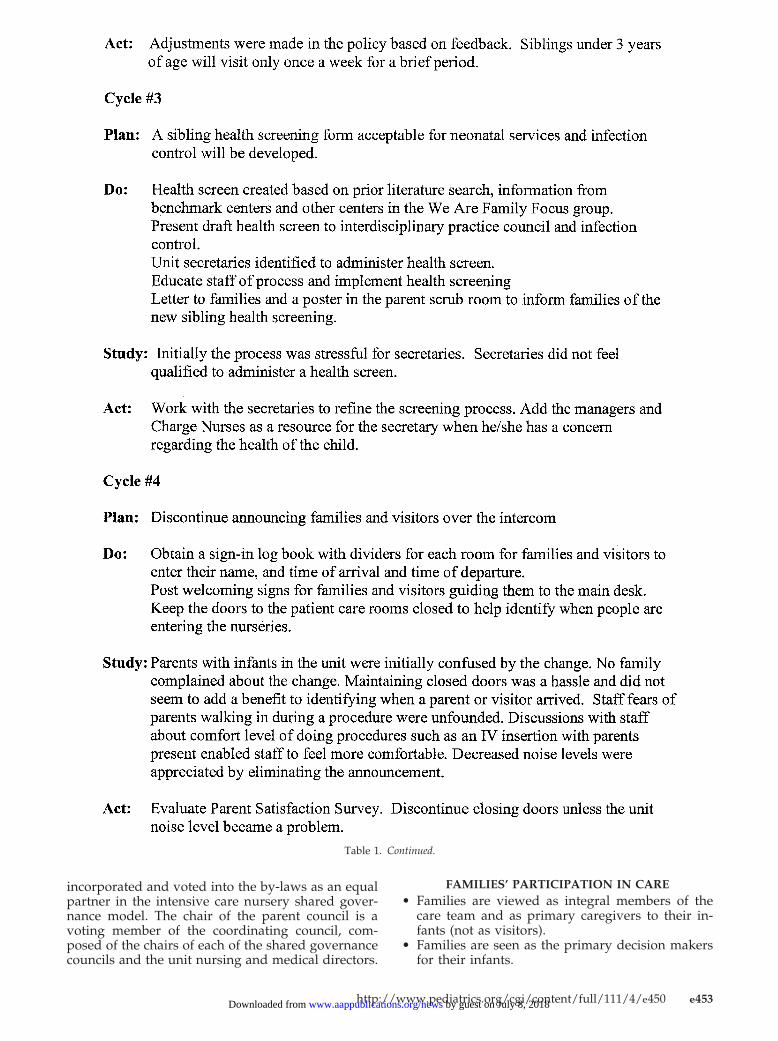
Table 1. Continued.
http://www.pediatrics.org/cgi/content/full/111/4/e450 e453 by guest on July 8, 2018www.aappublications.org/newsDownloaded from

• Families are asked how they would like to partic-ipate in their infants’ care and are given the edu-cation, resources, and support to participate to thelevel they desire.
• Families have the opportunity to discuss andrecord observations of their infant.
• The unit welcomes families 24 hours a day, includ-ing during rounds and change of shift.
The differences among the centers collaborating onimproving family-centered care were nowhere moreevident than in policies and practices about familyparticipation in care. Some centers encouraged par-ents’ participation in rounds and nursing shiftchanges, whereas others had rules excluding parents.This PBP required each center to reevaluate its visi-tation policies. When family-centered care is prac-ticed, parents and family are collaborators, or part-ners, in care and not “visitors.” Many centers rewroteguidelines to distinguish parent and family partici-pation in care from visitation guidelines for extendedfamily and friends. Making changes in visitationguidelines was difficult for some centers. DeVosChildren’s Hospital’s experience illustrates the bar-riers and challenges in changing visitation policies.
At DeVos Children’s Hospital, an interdisciplinarycommittee called the “Home Sweet Home” commit-tee was created to improve the nursery environmentso that families were better supported to participatein care. The committee was presented with informa-tion from several sources: preliminary work by theNIC/Q 2000 collaborative focus group on family-centered care, including benchmarking site visit re-sults, information from the Institute for Family-Cen-tered Care, and information from the DeVos parentsatisfaction survey. The committee identified andprioritized several ideas for improvement. Reevalu-ation of the current visitation policy with emphasison sibling visitation was selected as the first priority.Changes to the visitation policy were made in stagesover 1 year to receive staff input and address theirconcerns. These stages were conducted as improve-ment cycles using the improvement method of plan-do-study-act (Table 1). The overall aim was to pro-mote family visitation by allowing siblings to visitwhen most convenient for parents.
The existing visitation policy allowed parents to“visit” any time except change of shift. Grandparentscould also visit at any time with a parent. Siblingsand other family members could visit only whenaccompanied by a parent on Thursday night from7:30 to 9:30 or Sunday afternoon from 2:00 to 4:00.The neonatal unit was closed to all visitors exceptparents during respiratory syncytial virus season,which typically began in the fall and ended in latespring. The committee believed that these rules weretoo restrictive and set a goal of creating an environ-ment where families would always feel welcome.Initial reactions to liberalization of visitation guide-lines were mixed. Concerns were expressed that in-fection rates would increase, infants would becomeoverstimulated from increased noise, and the in-creased number of people visiting would interruptworkflow.
The first improvement cycle included gatheringinformation on the rationale and safety of the pro-posed change and presenting it to nursery staff andto the infection control department. The infectioncontrol department was particularly skeptical be-cause of concern for potentially introducing into theunit communicable diseases such as chicken pox andrespiratory syncytial virus.
The second improvement cycle involved draftingnew visitation guidelines, training personnel, andinitiating a pilot trial. Some staff initially believedthat having families with children on the unit morefrequently would adversely affect their workflow.After initial issues were addressed, most staff ex-pressed feeling less stress with more open siblingvisitation. Expanded sibling visitation reducedcrowding that had been a problem during the previ-ous sibling visitation hours. Problems encounteredwith lack of supervision of toddler-age siblings andan incident involving a toddler pulling on criticaltubing led to a decision to continue to restrict visita-tion by siblings below age 3 to 1 brief visit per week.
The third improvement cycle was designed to ad-dress concerns about the potential infection risk witha more open visiting policy. The committee reviewedliterature and asked other NICUs with more liberalpolicies how they managed infection risks.3 A simplequestionnaire was developed to screen for recentfever, runny nose, flu- and cold-like symptoms, andexposure to chickenpox. The unit secretary was as-signed to help families answer the questionnaire andmaintain documentation of the screening. When achild was cleared for entering the unit, he or shereceived a fun sticker of his or her choice, whichserved to identify that the sibling had been screened.The secretary documented the initial screening in anotebook. At each subsequent visit, the secretary andfamily would repeat the questions and the datewould be recorded. The process was stressful for thesecretaries initially. They did not feel qualified toscreen families about health. Assigning the clinicalmanagers and charge nurses to serve as resources forthe secretaries solved their concerns. Since changingto a more liberal sibling visitation policy, acquiredinfection as a result of transmission by siblings hasnot yet been suspected.
The fourth improvement cycle was designed todecrease noise and distraction in the patient careareas by discontinuing the practice of announcingthe arrival of parents over an intercom. Staff wereconcerned that a family member might walk into thepatient care area during a procedure or resuscitation.A system of calling out to the desk to inform thesecretaries when such an event was happening wasinitially developed but over time became unneces-sary. In the rare instance when a family member maywalk in during a procedure or resuscitation, a staffmember will assume the responsibility of explainingwhat is happening and supporting the parent if nec-essary. Not only has the elimination of added noisefrom the intercom been an improvement, nurses nolonger have to stop what they are doing to answerthe telephone when a parent arrives.
Reponses by parents to the question on the parent
e454 SUPPLEMENT by guest on July 8, 2018www.aappublications.org/newsDownloaded from
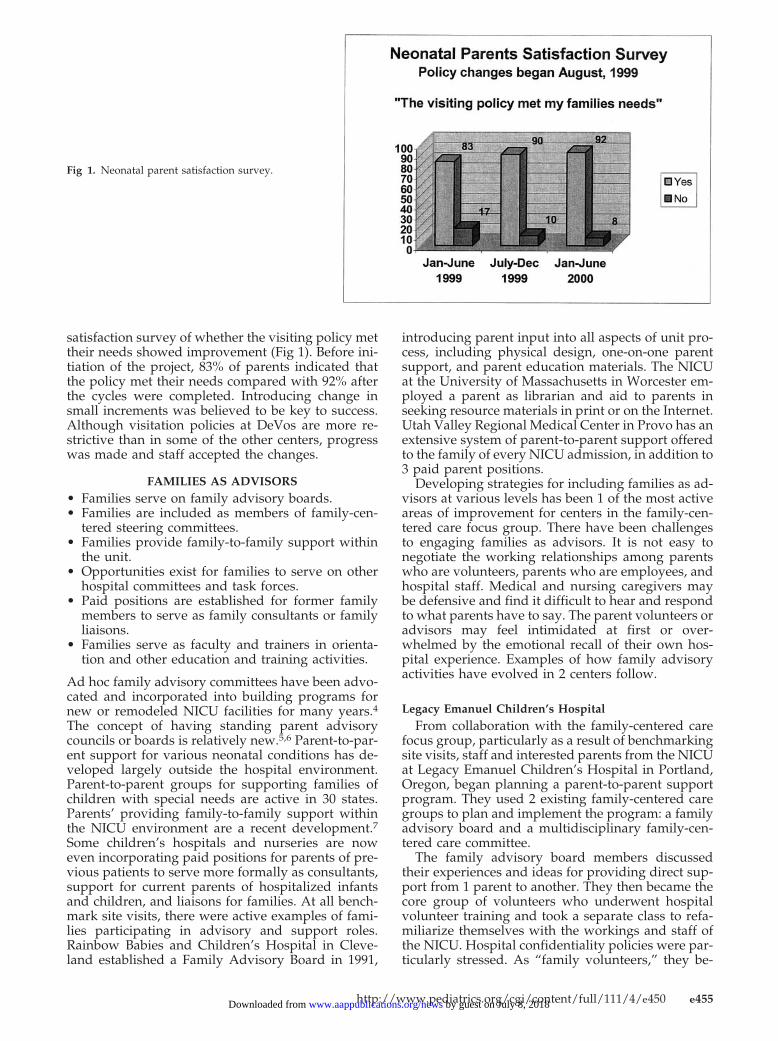
satisfaction survey of whether the visiting policy mettheir needs showed improvement (Fig 1). Before ini-tiation of the project, 83% of parents indicated thatthe policy met their needs compared with 92% afterthe cycles were completed. Introducing change insmall increments was believed to be key to success.Although visitation policies at DeVos are more re-strictive than in some of the other centers, progresswas made and staff accepted the changes.
FAMILIES AS ADVISORS• Families serve on family advisory boards.• Families are included as members of family-cen-
tered steering committees.• Families provide family-to-family support within
the unit.• Opportunities exist for families to serve on other
hospital committees and task forces.• Paid positions are established for former family
members to serve as family consultants or familyliaisons.
• Families serve as faculty and trainers in orienta-tion and other education and training activities.
Ad hoc family advisory committees have been advo-cated and incorporated into building programs fornew or remodeled NICU facilities for many years.4The concept of having standing parent advisorycouncils or boards is relatively new.5,6 Parent-to-par-ent support for various neonatal conditions has de-veloped largely outside the hospital environment.Parent-to-parent groups for supporting families ofchildren with special needs are active in 30 states.Parents’ providing family-to-family support withinthe NICU environment are a recent development.7Some children’s hospitals and nurseries are noweven incorporating paid positions for parents of pre-vious patients to serve more formally as consultants,support for current parents of hospitalized infantsand children, and liaisons for families. At all bench-mark site visits, there were active examples of fami-lies participating in advisory and support roles.Rainbow Babies and Children’s Hospital in Cleve-land established a Family Advisory Board in 1991,
introducing parent input into all aspects of unit pro-cess, including physical design, one-on-one parentsupport, and parent education materials. The NICUat the University of Massachusetts in Worcester em-ployed a parent as librarian and aid to parents inseeking resource materials in print or on the Internet.Utah Valley Regional Medical Center in Provo has anextensive system of parent-to-parent support offeredto the family of every NICU admission, in addition to3 paid parent positions.
Developing strategies for including families as ad-visors at various levels has been 1 of the most activeareas of improvement for centers in the family-cen-tered care focus group. There have been challengesto engaging families as advisors. It is not easy tonegotiate the working relationships among parentswho are volunteers, parents who are employees, andhospital staff. Medical and nursing caregivers maybe defensive and find it difficult to hear and respondto what parents have to say. The parent volunteers oradvisors may feel intimidated at first or over-whelmed by the emotional recall of their own hos-pital experience. Examples of how family advisoryactivities have evolved in 2 centers follow.
Legacy Emanuel Children’s HospitalFrom collaboration with the family-centered care
focus group, particularly as a result of benchmarkingsite visits, staff and interested parents from the NICUat Legacy Emanuel Children’s Hospital in Portland,Oregon, began planning a parent-to-parent supportprogram. They used 2 existing family-centered caregroups to plan and implement the program: a familyadvisory board and a multidisciplinary family-cen-tered care committee.
The family advisory board members discussedtheir experiences and ideas for providing direct sup-port from 1 parent to another. They then became thecore group of volunteers who underwent hospitalvolunteer training and took a separate class to refa-miliarize themselves with the workings and staff ofthe NICU. Hospital confidentiality policies were par-ticularly stressed. As “family volunteers,” they be-
Fig 1. Neonatal parent satisfaction survey.
http://www.pediatrics.org/cgi/content/full/111/4/e450 e455 by guest on July 8, 2018www.aappublications.org/newsDownloaded from

gan spending blocks of time in the unit, reconnectingwith staff and meeting current NICU families. Theirschedules appear alongside unit staffing schedules toboost visibility and integration. They wear specialbuttons to distinguish them from “regular” hospitalvolunteers. The parents of a newly admitted infantwill find a “calling card” at the infant’s bedside,giving information about the program. If the parentsexpress interest, then a family volunteer will beasked (usually by the bedside nurse) to meet withthem. The interaction and support are tailored toeach family’s interests and needs during their child’sinpatient stay. A family volunteer is on call aroundthe clock to talk with parents by telephone.
The new program, called Precious Beginnings, hasa mission “to touch the life of each family in theNICU in a positive and lasting way.” Precious Be-ginnings has incorporated as a nonprofit organiza-tion in the state of Oregon. This has been an impor-tant step that allows them to engage in tax-exemptfundraising. In addition to parent-to-parent supportactivities, participating volunteers publish a familynewsletter monthly and hold pizza night twice amonth to broaden their network of support to par-ents.
Benefits from the Legacy Family Advisory Boardand Precious Beginnings are
• Increased support presence on the NICU• Education of families• A growing network of committed volunteers• Promoting Legacy Emanuel Children’s Hospital as
a champion of family-centered care
Establishing a collaborative and even collegial rela-tionship between parent volunteers and NICU staffhas been a goal and will be a key to success. Accep-tance of the parent-to-parent program has dependedon the enthusiasm and energy of the family volun-teers, the grateful responses of NICU parents, andthe emerging visibility of the program. The volun-teers have found that their strong commitment tomaking the NICU experience less stressful for par-ents makes a lasting and favorable impression onstaff.
Children’s Hospital at DartmouthFounding and establishing a parent advisory
council has been one of the most important changesthat has resulted from Children’s Hospital at Dart-mouth’s participation in the family-centered care fo-cus group. Founded officially in October 1999, theidea originated with the Parent Care Initiative, an adhoc multidisciplinary task force that preceded theNIC/Q 2000 project. That task force developed theintensive care unit philosophy statement: “We be-lieve the parent-child relationship is essential. Webelieve in providing a nurturing environment wherethe child is part of a family, and the family is part ofthe care team.”
Several factors contributed to the successful initi-ation of the parent advisory council. Multidisci-plinary teams including staff nurses and parents par-ticipated in the benchmarking site visits. The
enthusiasm generated on return from the visits was amajor factor in developing and promoting improve-ment ideas for family-centered care. A second factorwas the commitment to a bidirectional free flow ofideas. Nursery staff members are encouraged to par-ticipate in monthly parent advisory council meetingsand to present new ideas and initiatives for familyinput. Conversely, representatives from the parentcouncil frequently serve on ad hoc nursery commit-tees for specific improvement projects. A third factorhas been support for the parent council in the form ofspace to meet at the medical center, food for meet-ings, and on-site child care. Incorporating the parentadvisory council into the shared governance of theunit was described in the section “Unit Culture.”
There have been several challenges to starting theparent advisory council. Some nurses were con-cerned that parents would be overly critical andmake demands for changes without understandingall of the issues that nurses encounter. Open commu-nication and collaboration have largely dispelled thisconcern. Because the intensive care nursery is a re-gional referral center, most parents reside a distanceaway from the medical center. This creates obviouslogistic problems in recruitment of council membersand participation. Some strategies have been to usespeakerphones to connect to the meetings and devel-oping tasks that can be done by communication overelectronic mail rather than attendance at meetings. Aproblem shared by most parent councils is gettingrepresentation from parents across the cultural, age,and economic spectrum. Finally, strategies for fund-ing activities have not been fully resolved. Fundrais-ing efforts done by the parent council may conflictwith similar activities by Children’s Hospital at Dart-mouth. Clearly defining the goals and needs has ledto success in designating the proceeds of certainfundraising activities for the parent advisory council.
A brief list of accomplishments by the parent ad-visory council include
• Creating a combination parent information guideand journal called “Special Beginnings” to begiven along with a gift bag to the parents of everyadmission to the intensive care nursery
• Successfully advocating with nursery staff for atoll-free call-in line for parents
• Supporting and explaining why eliminating exclu-sion of parents from nursing “change of shift” wasimportant
• Teaching nursery staff about parents’ perspectivesduring mandatory “Skills Days” and during ori-entation of new staff
• Participating in interviewing and recruitingnurses and physicians
• Participating in fundraising and promoting Chil-dren’s Hospital at Dartmouth
• Expressing parents’ perspective on the issue ofparents presence during teaching and patient carerounds and collaborating to address issues of con-fidentiality
• Sponsoring parent support activities, such aspizza nights and Sunday coffee hour, for intensivecare nursery parents
e456 SUPPLEMENT by guest on July 8, 2018www.aappublications.org/newsDownloaded from

• Contributing articles to the unit’s monthly news-letter
Future goals of the parent advisory council includedeveloping a parent-to-parent support program andhelping to establish a salaried permanent parent sup-port liaison.
Parent volunteer programs have special chal-lenges, and each hospital has had to answer crucialquestions during their evolution. When is a parent“ready” to serve in an advisory role? How can parentcouncils address issues of diversity and languagebarriers? What is the best way to “support” a familyin the NICU? Welcoming families to serve as advi-sors requires commitment from the organization andfrom departmental leaders. Like most new pro-grams, it requires time, money, and enthusiasm, aswell as sensitivity to the resistance that may arisefrom introducing a new “culture” to the workplace.
DISCUSSIONIn 1992, a group of parents met with neonatal
professionals to discuss how care providers couldcollaborate more effectively with parents of sicknewborn infants. Subsequent to that meeting, an ar-ticle summarizing “The Principles for Family-Cen-tered Neonatal Care” was published.8 These princi-ples have since been reflected in statements from theAmerican Academy of Pediatrics as well as otherorganizations, supporting the role of families in de-cision making.9–11 Although progress has been madeto include families in major decisions, intensive careunits remain environments where nurses and physi-cians maintain most of the control.
Families dealing with the stress of sick infants whorequire critical care often feel lost, out of control, andin unfamiliar surroundings.12–14 Parents have repeat-edly expressed their need to be an integral part of thecare of their children. Unfortunately, examples ofbreakdowns in the relationships between neonatalcare providers and parents abound.15–17 The prob-lems in neonatal intensive care are not unique but arerepresentative of a broader problem. The currenthealth care system often falls short of meeting theneeds of the population. Improving the care pro-vided will require a change in the fundamental be-liefs and philosophy of care.
The Institute of Medicine proposed changesneeded to improve the quality of health care in theUnited States for the 21st century.18 The proposedrules address patient and provider relationships.
Recommendations include customizing care accord-ing to patient needs and values, recognizing the pa-tient as the source of control, and placing the patientand family in the center of choices about care—allprinciples consistent with family-centered care.
Changing the culture of care in NICUs is not easy.The experiences of centers in the family-centeredcare focus group illustrate challenges as well as suc-cesses. Family-centered care is more of a journeythan a destination. Collaborating centers in thisproject found themselves at different places in thatjourney. Through perseverance in implementing thePBPs, all have moved further along the path.
REFERENCES1. Saunders RP, Abraham MR, Crosby MJ, Thomas K, Edwards WH.
Evaluation and development of potentially better practices for improv-ing family-centered care in neonatal intensive care units. Pediatrics.2003;111(suppl):e437–e449
2. Nyqvist KH, Karlsson KH. A philosophy of care for a neonatal intensivecare unit. Scand J Caring Sci. 1997;11:91–96
3. Montgomery LA, Kleiber C, Nicholson A, Craft-Rosenberg M. A re-search-based sibling visitation program for the neonatal ICU. Crit CareNurse. 1997;17:29–39
4. White R, Martin GI, Graven SN. Newborn intensive care unit design:scientific and practical considerations. In: Avery GB, Fletcher MF, Mac-Donald MG, eds. Neonatology: Pathophysiology and Management of theNewborn. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:49–59
5. Jeppson E, Thomas J. Essential Allies: Families as Advisors. Bethesda, MD:Institute For Family-Centered Care; 1995
6. Jeppson E, Thomas J. Families as Advisors: A Training Guide for Collabo-ration. Bethesda, MD: Institute For Family-Centered Care; 1995
7. Roman LA, Lindsay JK, Boger RP, et al. Parent-to-parent support initi-ated in the neonatal intensive care unit. Res Nurs Health. 1995;18:385–394
8. Harrison H. The principles for family-centered neonatal care. Pediatrics.1993;92:643–650
9. AAP Committee on Bioethics Policy Statement. Ethics and the Care ofCritically Ill Infants and Children. Pediatrics. 1996;98:149–152
10. AAP Committee Fetus and Newborn Policy Statement. The initiation orwithdrawal of treatment for high-risk newborns. Pediatrics. 1995;96:362–363
11. AAP Committee on Fetus and Newborn and ACOG Committee onObstetric Practice Policy Statement. Perinatal care at the threshold ofviability. Pediatrics. 1995;96:974–976
12. Gordin P, Johnson BH. Technology and family-centered perinatal care:conflict or synergy. J Obstet Gynecol Neonatal Nurs. 1999;28:401–408
13. Meck NE, Fowler SA, Claflin K, Rasmussen LB. Mother’s perceptions oftheir NICU experience 1 and 7 months after discharge. J Early Interv.1995;19:288–301
14. Wereszczak J, Miles MS, Holditch-Davis D. Maternal recall of the neo-natal intensive care unit. Arch Psychiatr Nurs. 1997;11:118–125
15. Stinson R, Stinson P. The Long Dying of Baby Andrew. Boston, MA: Little,Brown; 1983
16. Mehren E. Born Too Soon: The Story of Emily, Our Premature Baby. NewYork, NY: Doubleday; 1991
17. Woodwell WH Jr. Coming to Term: A Father’s Story of Birth, Loss, andSurvival. Jackson, MI: University Press of Mississippi; 2001
18. Institute of Medicine. Crossing the Quality Chasm: A New Health Systemfor the 21st Century. Washington, DC: National Academy Press; 2001
http://www.pediatrics.org/cgi/content/full/111/4/e450 e457 by guest on July 8, 2018www.aappublications.org/newsDownloaded from
e458 SUPPLEMENT by guest on July 8, 2018www.aappublications.org/newsDownloaded from
http://www.pediatrics.org/cgi/content/full/111/4/e450 e459 by guest on July 8, 2018www.aappublications.org/newsDownloaded from
e460 SUPPLEMENT by guest on July 8, 2018www.aappublications.org/newsDownloaded from

2003;111;e450Pediatrics William H. Edwards
Kimberly A. Cisneros Moore, Kara Coker, Allison B. DuBuisson, Betsy Swett andin Neonatal Intensive Care Units: Successes and Challenges
Implementing Potentially Better Practices for Improving Family-Centered Care
ServicesUpdated Information &
0http://pediatrics.aappublications.org/content/111/Supplement_E1/e45including high resolution figures, can be found at:
References
0#BIBLhttp://pediatrics.aappublications.org/content/111/Supplement_E1/e45This article cites 11 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/hospital_medicine_subHospital Medicinesubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 8, 2018www.aappublications.org/newsDownloaded from
2003;111;e450Pediatrics William H. Edwards
Kimberly A. Cisneros Moore, Kara Coker, Allison B. DuBuisson, Betsy Swett andin Neonatal Intensive Care Units: Successes and Challenges
Implementing Potentially Better Practices for Improving Family-Centered Care
http://pediatrics.aappublications.org/content/111/Supplement_E1/e450located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2003 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 8, 2018www.aappublications.org/newsDownloaded from