Embed Size (px)
Citation preview

Implications of Molecular and
Chemosensitivity Testing:
What Drug for What Marker–Are We
There?
NO!
Harvey I. Pass, MD
NYU Langone Medical Center
NO!

Disclosures• Research Funding from NCI/NIH, DOD, CDC, Covidien,
Mensanna, Rosetta Genomics, SomaLogic, Celera, SourceMDx,
Fujirebio, Pfizer, Response Genetics, Meso Scale Diagnostics,
Integrated ,and Fox, Stephen Banner Lung Foundation,
Simmons Mesothelioma Foundation, and a whole bunch of
patients.
• Medical Advisory Boards for Quest Diagnostics, Rosetta • Medical Advisory Boards for Quest Diagnostics, Rosetta
Genomics, Champions, Precision Therapeutics, Pinpoint
Genomics, GSK, and GE Healthcare
• CDAs with Avantra, Caris Life Sciences, Transgenomics,
Foundation Medicine
• Patents for use of osteopontin and microRNA for
diagnosis/prognosis of mesothelioma; osteopontin isoforms for
NSCLC; EFEMP1 for diagnosis of mesothelioma

Predictive Biomarkers
• “Hot off the press” Surgically Resected Prognostic Stratification
– WHO should get adjuvant therapy (as opposed to WHICH adjuvant therapy should be used)
• The Paucity of Validated Predictive Biomarkers
• Adjuvant Therapy and Predictive “tissue” • Adjuvant Therapy and Predictive “tissue” Biomarkers
• Next Generation Sequencing for Biomarker Discovery
• Chemosensitivity Testing: The Data, Please!
• In vivo Tumorgraft Personalized Treatment

Pro
gn
ost
ica
tio
n 14 genes
Non-Squamous
qPCR
Lancet 2012 March 3:379(918): 823-832
Pro
gn
ost
ica
tio
n

Predictive Markers
• Companion Diagnostics that hopefully will be able to discriminate populations which are sensitive to a cytotoxic or targeted therapy
• Great potential for personalized adjuvant therapy• Great potential for personalized adjuvant therapy

Which Stage IV Lung Cancer Treatments Have Companion Predictive Biomarkers?
� EGFR H-score (IHC) NO NO
TARGETCLINICALLY
VALIDATED
COMPANION
DX
� EGFR mutation YES NO
� ALK-Fusion YES YES
� EGFR H-score (IHC) NO NO
� C-MET NO NO
� ERCC1 NO NO
� RRM1 NO NO
� BRCA NO NO
� TS NO NO

ALK FUSION AND LUNG CANCEROnly 7% But a Predictive Assay and Treatment Selectivity
CRIZOTINIB
MET/ALK TKI
Novel fusion identified in Novel fusion identified in 20072007 in NSCLC; in NSCLC; EML4EML4--ALKALK
Soda et al., Nature 2007
Anaplastic Lymphoma Kinase (ALK)Anaplastic Lymphoma Kinase (ALK)
Echinoderm microtubule-associated protein-
like 4 (EML)

~250 kb ~300 kb
t(2;5) ALK gene
breakpoint region
2p23 regionTelomere Centromere
3’ 5’
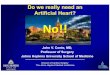
FISH Assay for ALK Rearrangement*
Break-apart FISH assay
ALK 29.3
EML4 42.3
q14.1
q12.3q12.1
p12
p13.2
p14
p16.1
p16.3
p22.1
p23.2
p22.3
p24.1
p24.3
p25.2
q14.1
q12.3q12.1
p12
p13.2
p14
p16.1
p16.3
p22.1
p23.2
p22.3
p24.1
p24.3
p25.2
Break-apart FISH assay
for ALK-fusion genes1
ALK break-apart FISH assay
q36.1
q36.3
q37.2
q34
q32.1
q32.3
q33.2
q31.3
q24.3
q24.1
q23.2q22.2
q22.1
q21.2
q14.3
q36.1
q36.3
q37.2
q34
q32.1
q32.3
q33.2
q31.3
q24.3
q24.1
q23.2q22.2
q22.1
q21.2
q14.3
Split
signal
Non-split
signal
*Assay is positive if rearrangements can be detected in ≥15% of cells
FISH = fluorescence in situ hybridization Solomon, B et al:JTO
4:1450-1454,2009.

ALK-Positive Non-Small Cell Lung Cancer
Study A8081001:Crizotinib Response, PFS & OSApproved by the US FDA on 26 August 2011
Best Percent Change in Tumor Size (N*=106)
Median OS not reached, with 79% pts still in
follow-up. Survival probability at 6 months:
90.0%, at 12 months: 80.5% Median PFS = 10.0 mo

We Would Love To Have The EML4-ALK Story For Adjuvant Therapy……
� But we don’t because
– The biomarkers are not fully validated
– The biomarkers have various platforms for their
measurement without consensus in some cases of measurement without consensus in some cases of
which to use
• IHC vs mutation analysis vs FISH for EGFr
• rtPCR vs AQUA for ERCC1/RRM1
� Sooooo….what DO we have in order to
discover adjuvant predictive biomarkers?

Trial n Stage Chemotherapy 5-yr OS (%) HR (95% CI) p value
CT C
IALT * 1867 I–IIIA Cisplatin-based 44.5 40.4
0.86
(0.76–0.98) <0.03
JBR.10* 482 IB–II
Cis/
vinorelbine 69 54
0.69
(0.52–0.91) 0.009
Adjuvant Studies for Predictive Marker
Development and Validation
JBR.10* 482 IB–II vinorelbine 69 54 (0.52–0.91) 0.009
CALGB 344 IB
Carbo/
paclitaxel 59 57
0.80
(0.60–1.07) 0.1
LACE*
meta-
analysis 4584 I–IIIA Cisplatin-based 48.8 43.5
0.89
(0.82–0.96) 0.004
FFPE blocks are available from studies for IHC

P53, BCL2,
BAXp27
KRas, EGFr
Weinberg, Cell: 2000
βTubulins
RRM1
TS
VEGF, EGFr
Repair of DNA DamageERCC1
MSH2BRCA1

Biomarker Clinical Relevance Studies
ERCC1 Low ERCC1 =improved outcome after treatment
with platinum-based chemotherapy
IALT-Bio;
LACE-Bio Pending
MSH2 Low MSH2 = longer survival after treatment with
platinum-based chemotherapy
IALT-Bio;
alone and combined
BaxAssociation between high Bax levels and sensitivity Both IALT-Bio,
Predictive Biomarkers Validated Retrospectively in
Adjuvant Trials
BaxAssociation between high Bax levels and sensitivity
to chemotherapy
Both IALT-Bio,
and LACE-Bio
Class III
βtubulin
High expression of class III -tubulin = longer OS and
DFS survival (taxanes) JBR.10
15-gene
signatureHigh-risk patients benefit from adjuvant
chemotherapyJBR.10

Other Predictive Markers Moving to Prospective
Validation
BRCA1 RRM1 Thymidylate Synthase
• DNA repair, mitosis and cell
division
• High levels associated with
platinum resistance in vitro
• Important for DNA synthesis
• Enhanced expression is
associated with resistance to
gemcitabine in cell lines
• High TS expression is
associated with reduced
efficacy of pemetrexed in
vitroplatinum resistance in vitro gemcitabine in cell lines vitro
• High TS expression is
associated with squamous
cell carcinoma

Biomarker Trial
EGFrErlotonib vs placebo + adjuvant ChT (up to 4 cycles), IHC +
FISH
BRCA1Randomized Study of Customized Adjuvant Chemotherapy Based
on BRCA1 mRNA Levels in Completely Resected Stages II–IIIA in
Non-Small Cell Lung Cancer (GECP-SCAT)
ERCC1/RRM1 Gemcitabine and Cisplatin in Treating Patients With Stage I Non-
Ongoing Prospective Biomarker Studies Used in An
Adjuvant Setting
ERCC1/RRM1 Gemcitabine and Cisplatin in Treating Patients With Stage I Non-
Small Cell Lung Cancer That Was Removed by Surgery (SWOG
0720)
ERCC1/EGFR mutation
status TAilored Post-Surgical Therapy in Early Stage NSCLC (TASTE)
ERCC1/thymidylate
synthase
International Tailored Chemotherapy Adjuvant (ITACA) trial
Therapy
MAGE-A3 GSK1572932A Antigen-Specific Cancer Immunotherapeutic as
Adjuvant n Patients With Non-Small Cell Lung Cancer (MAGRIT)
15 gene signature Precision Therapeutics

GECP-SCAT

What is coming?
Search for Actionable Mutations with Next
Generation Sequencing
• Lung Cancer Mutation Consortium
• The Cancer Genome Atlas (TCGA)
– Squamous Cell Carcinoma
– Adenocarcinoma– Adenocarcinoma
• Industry-Based Mutation Analyses
– Foundation Medicine
• 200 most common mutations: $5000

Lung Cancer Mutation Consortium
Simultaneous Testing
for 8 mutations
by Snapshot Or Sequenome
and
MET amplification or
ALK Fusion by FISH
Panel testing is feasible but
many alterations are rare

Tyrosine Kinase Domains of Dominant “Driver” Mutations are
Established Therapeutic Targets
• EGFR
• HER2
• BRAF
• EML4/ALK
• MET Amplification
• EGFR Amplification
Mutation Testing
FISH Testing for Fusion
and/or Copy Number Testing
• BRAF
• PI3KCA
• AKT1
• MAP2K1
• KRAS
• NRAS
• EGFR Amplification
• HER2 Amplification
Drugs approved for NSCLC
Drugs approved for other cancers
Drugs targeting these genes in
clinical development
The majority of tested patients receive targeted drug

Chemoresponse Testing
Chemoresponse Assay Measure of Drug Effect
ATP tumor chemosensitivity assay(ATP-TCA)
Luciferase assay measures ATP content of tumor cells
Microculture kinetic (MiCK) assayContinuous measure of apoptosis induced by cytotoxic drugs
DISC , MTT, ATP, Caspase 3/7 assayCorrelative assays of cell death and
• Encouraging data in GYN malignancies (the only Medicare approval)
DISC , MTT, ATP, Caspase 3/7 assayCorrelative assays of cell death and apoptosis
ChemoFx® assayMeasures primary tumor cell survival in response to cytotoxic drugs

Relation to Lung Cancer Adjuvant Therapy?• Plate Prep: Automated, Robotic
• Cell Plating: Automated, Robotic
(384 wells, 24 hr incubation)
• Drug Solution Prep
• Serial Drug dilution Prep
(10 Concentrations)
• Add Drug to cells/wells
(72 hour incubation)
• Fix Cells
• Stain Cells to count cell nuclei
Schuchert, M.J., Cerfolio, R.J., et al. Ann Surg Onc. 2011; 18 (suppl 1; abstr 292)

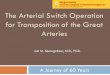
Potential TumorGraft Attributes and Advantages
Maintain growth factor-
tumor interactions
Maintain cancer cell
heterogeneity
Maintain supporting
stroma
Maintain tumor-vascular
interactions
� Maintains fundamental genotype
� Maintains heterogeneity of original cancer
� Maintain supporting stroma & cancer stem cells as in the human tumor.
• At least through 9 generations (F9)
� Can be molecular categorized for targeted drug development
� Exploring means to shorten cycle times
Courtesy of Champions Oncology

SURGERY FIRST ROUND
PA
TIE
NT
RECOVERY
EXPANSION
4-6 months
TREATMENT
2-3 weeks
TU
MO
RG
RA
FT
RESECTIONENGRAFTMENT
24 hours
Courtesy of Champions Oncology

In Vitro vs In Vivo
Number Of
NSLC
Patients
Tested
Data
Turnover
Time
Cost Includes
Mutational
Analyses
Medicare
Approved
Published
Results For
Time To
Progression
ChemoFx Hundreds 1-2 weeks $5000 Soon Selectively YesChemoFx Hundreds 1-2 weeks $5000 Soon Selectively
in Ovarian
Yes
(ovarian)
Tumorgrafts < 20 6 months $5000-
25,000
Yes No Yes
(pancreatic)

Conclusions
• There are no validated companion tissue biomarkers at present which predict efficacy of adjuvant chemotherapy.
• However, prospective trials are ongoing which test the ability of biomarkers to predict the utility of companion biomarkers.companion biomarkers.
• Future targets for therapy may be defined by whole genome sequencing for targetable novel mutations in lung cancer.
• In vitro/in vivo testing for personalization of adjuvant therapy, although promising, awaits validation in well designed prospective trials.