Embed Size (px)
DESCRIPTION
Implications of new hepatitis C treatments for WHO activities related to people who inject drugs. Nicolas Clark, Medical Officer Management of Substance Use WHO, Geneva CREIDU Colloquium Melbourne 2014. Number of deaths/year from selected conditions, 2010. - PowerPoint PPT Presentation
Citation preview

Implications of new hepatitis C treatments for WHO activities
related to people who inject drugs
Implications of new hepatitis C treatments for WHO activities
related to people who inject drugsNicolas Clark, Medical Officer
Management of Substance Use
WHO, Geneva
CREIDU Colloquium
Melbourne 2014

2
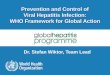
Number of deaths/year from selected conditions, 2010
Number of deaths/year from selected conditions, 2010
HIV/AIDS Viral hepatitis Tuberculosis Malaria0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
No
. o
f d
eath
s (m
illi
on
s)
Source: Global Burden of Disease Study 2010 Lozano et al, Lancet 2012
1.4 million people died in 2010 of viral hepatitis

3
Estimated annual deaths from selected causes by region, 2010Estimated annual deaths from
selected causes by region, 2010
Asia Pacific Americas Europe Africa & ME0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
Viral hepatitis HIV TB Malaria
Nu
mb
er
of d
ea
ths/
yea
r
Source: Courtesy of IHME – Global Burden of Disease Study

4
Number of hepatitis deaths by virus type and disease outcome, 2010
Number of hepatitis deaths by virus type and disease outcome, 2010
Acute Hepatitis
HBV - HCC
HBV - cirrhosis
HCV - HCC
HCV - cirrhosis
0.0
50.0
100.0
150.0
200.0
250.0
300.0
350.0
400.0
All
-ag
e d
eath
s (x
1,00
0)
A
B
C
E
Source: Global Burden of Disease Study 2010 Lozano et al, Lancet 2012
Most deaths are due to chronic hepatitis B and C

5
Global prevalence of hepatitis C infection, 2005 adults (19-49 years), by GBD region
Global prevalence of hepatitis C infection, 2005 adults (19-49 years), by GBD region
Source: Hannafiah et al. Hepatology 2013

6
Prevalence of HCV among persons who inject drugs
Prevalence of HCV among persons who inject drugs
HCV prevalence in PWID >50% in most countries; between 60-80% in 25 countriesand >80% in 12 countries
Nelson et al. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: results of systematic reviews. Lancet, 378 (9791), 2011.

7
Drug use GBD 2010 estimatesDrug use GBD 2010 estimates

8
Disease burden attributable to drug dependence by age in 2010 (Degenhardt et al, Lancet, 2013)
Disease burden attributable to drug dependence by age in 2010 (Degenhardt et al, Lancet, 2013)

9
Hep B immunizationBlood/injection safetyOutbreak controlWater and sanitation
WHO's Hepatitis area of work: evolution…
WHO's Hepatitis area of work: evolution…
2010 2011 2012 2013 2014
World Health Assembly
Resolution onViral Hepatitis
WHAresolution
STAC-Hep
Establishment of Global Hepatitis
Programme (GHP)
Reorganization of Global Hepatitis
Programme
2015(and beyond)
Implementation of Resolution
And Global Action
Plan
Global Framework

10
HIV/AIDS(HIV)
Pandemic and Epidemic Diseases
(PED)
Food Safety, Zoonoses and
Foodborne Diseases
(FOS)
Service Delivery and Safety (SDS)
Essential Medicines and
Health Products
(EMP)
Health Statistics and Information
Systems (HSI)
Management of Noncommunicable Diseases (MND)
Immunization, Vaccines and Biologicals
(IVB)
Mental Health and
Substance Abuse (MSD)
Country Offices
WHO's internal organization of the Global Hepatitis ProgrammeWHO's internal organization of the Global Hepatitis Programme
Country Offices
AFRO EURO SEARO
AMRO EMRO WPRO
RegionalOffices
GHP Secretariat
HQ

11
Global Hepatitis Framework: GoalsGlobal Hepatitis Framework: Goals
Within a health systems framework: Reduce transmission Reduce morbidity and mortality and improve treatment and
care of patients Reduce the socio-economic impact at individual, community
and population levels
Entry-point to link with and support other critical organizational priorities, including universal health coverage affordable access to commodities health inequities

12
Global Hepatitis Framework: Four AxesGlobal Hepatitis Framework: Four Axes
Axis 1: Partnerships, resource mobilization and communication
Axis 2: Data for policy and action
Axis 3: Prevention of virus transmission
Axis 4: Screening, care and treatment

13
Axis 1: Increasing engagement through awareness, partnerships and mobilizing resources
Axis 1: Increasing engagement through awareness, partnerships and mobilizing resources
• Status:– Low levels of awareness, engagement, political action, financial
commitment
• Actions and plans:– Promotion of World Hepatitis Day commemoration– Establish Global Hepatitis Network– Global Hepatitis Policy Report– Global Partners’ meeting on hepatitis– Formation of civil-society reference group

14
World Hepatitis Day 2013 sample postersWorld Hepatitis Day 2013 sample posters

15
WHO Global Policy Report 2013WHO Global Policy Report 2013
Aim: To assess WHO Member States' response to hepatitis – in the context of the WHO Resolution 63.18
Conducted in collaboration with World Hepatitis Alliance
Response rate: 125 of 194 (64%)Member States

16
Status: – Weak surveillance systems leading to poor quality of country-
level data on burden of infection and disease outcomes– Lack of reporting system to monitor implementation of
treatment scale-up
Actions:– Publish global prevalence and burden estimates for viral
hepatitis – Develop guidelines for hepatitis surveillance in low- and
middle-income countries
Axis 2: Evidence-based policy and data for action
Axis 2: Evidence-based policy and data for action

17
WHO sponsored systematic reviews of hepatitis prevalence data

18
Plans:– Establish modelling reference group– Conduct regional adaptation workshops of surveillance
guidance– Conduct country hepatitis burden-of-disease and national
planning workshops– Develop a monitoring and reporting framework for assessing
country and global hepatitis response
Axis 2: Evidence-based policy and data for action
Axis 2: Evidence-based policy and data for action

19
Axis 3: Prevention of virus transmission
Axis 3: Prevention of virus transmission
Status: Effective prevention measures exist but level of implementation is variable
Actions:– Blood safety:
• policy guidance and technical assistance to countries for– universal access to safe blood and blood products – self-sufficiency in safe blood and blood products based on
voluntary unpaid blood donation– Injection safety:
• SIGN Network• WHO-UNICEF-UNFPA for exclusive use of auto-disable syringes in
immunization services• Promotion of harm-reduction guidance and services

20
Axis 3: Prevention of virus transmission
Axis 3: Prevention of virus transmission
Plans:– Immunization:
• Promotion of birth dose administration• Hepatitis E vaccine SAGE working group
– Blood safety:• Continued emphasis on implementation of policies
– Injection Safety:• Launch of Global Injection Safety Campaign

21
Axis 4: TreatmentAxis 4: Treatment
Status:– Dramatic advances in treatment options– Very low levels of:
• Awareness among general public and health-care workers• Access to screening• High-quality, low-cost diagnostics• Laboratory infrastructure• Treatment uptake
– New WHO hepatitis treatment guidelines

22

23
WHO’s role in improving access to hepatitis therapy
WHO’s role in improving access to hepatitis therapy
Awareness Testing ReferralDisease-
stage assessment
Treatment Monitoring
World Hepatitis Day observanceImproved prevalence estimates
Prequalification of diagnosticsScreening/ testing guidelines
Treatment GuidelinesPrequalification of generic medicinesEssential Medicines ListAdvocacy, guidance and technical assistance for improved treatment accessMulti-stakeholder engagement
Screening Care Treatment

24
Topics for WHO hepatitis C screening, care and treatment guidelines
Topics for WHO hepatitis C screening, care and treatment guidelines
Awareness Testing ReferralDisease-
stage assessment
Treatment Monitoring
Who should be tested for hepatitis C (antibodies)?
When to confirm HCV infection (PCR)?
What interventions to slow progression of liver
disease?
How to assess degree of liver fibrosis/cirrhosis?
When to start treatment?
What medicines to use?
How to monitor for response to treatment and drug adverse
reactions?
Screening Care Treatment

25
New Opportunities for treatment scale-upNew Opportunities for treatment scale-up
Current treatment regimens are complex, costly (drugs and monitoring) and have significant toxicities
Dramatic new treatment results, high SVR rates, oral regimens, pan-genotype and high safety profile
WHO published it’s first ever hepatitis C treatment guidelines in April 2014
Successful price reductions, – Egypt $900 for a 12 week course of
sofosbuvir – USA $84,000 in comparison

26
WHO recommendations on diagnosis and treatment of hepatitis C in PWID
WHO recommendations on diagnosis and treatment of hepatitis C in PWID
Screen PWID– anti-HCV antibodies
• rapid testing vs serology
Diagnosis– HCV RNA
Reduce alcohol intake
Staging– liver biopsy– non – invasive test
Treatment – genotype 1,2,3,4
• sofosbuvir• pegylated interferon and
ribavirin
– genotype 1• telaprovrevir or bocepravir
– genotype 1b & 1a (without Q80K polymorphism)• simepravir

27
SVR in PWUDSVR in PWUD
Aspinall et al. (2013)

28
Re-infection rates in PWUDRe-infection rates in PWUD
Aspinall et al. (2013)

29
What can we learn from HIV about increasing services for PWID?
What can we learn from HIV about increasing services for PWID?

30

31
Inequitable access to ART
Wolfe et al, The Lancet 2010; 376:355-66 .

32
Integration and colocation of services

33
Policy guidelines for TB and HIV services for drug users
Policy guidelines for TB and HIV services for drug users
Joint Planning Service providers
National & local coordination body Plans with roles, responsibilities & M&E Human resources and training available Support to operational research
Package of Care
TB infection control plans in care settings
Case finding protocols at services drug users present
Treatment services for TB and HIV available
Isoniazid prevention available
HIV prevention (Harm Reduction Package)
Overcoming Barriers
Integrated services (Link TB/HIV treatment and harm reduction
Equivalence of care in prisons
Adherence support measures
Comorbidity not to be used to withhold treatment

34
Overlapping EpidemicsOverlapping Epidemics
Hepatitis
HIV
IDU

35
HIV ProgramAntiretroviral TreatmentDrug InteractionsVCTToxicity MonitoringProphylaxis of OIsAdherence SupportSecondary PreventionSyringe Exchange
Hepatitis ProgrammeDOTDiagnosisStagingAlcohol counsellingTreatment monitoringAdherence SupportDrug Interactions
Drug TreatmentOpioid Substitution TherapyEffective CounselingDOTUrine MonitoringDrug InteractionsSyringe Exchange
CommunicationCollaboration
Communication
Collabora
tion
Comm
unication
Collaboration

36
models of caremodels of care
• non-integrated– referral– linkage
• integrated care– integrated in general health care
• primary care– multi-skilled team– specialist outreach
• integrated in district hospital– integrated specialist services
• hepatitis treatment provided in drug treatment– multiskilling or specialist outreach
• drug treatment provided in hepatitis clinic• combined addiction and hepatitis specializations

37
Can any part of the health system treat hepatitis?
Can any part of the health system treat hepatitis?

38
requirements for hepatitis treatmentrequirements for hepatitis treatment
• laboratory capacity– serology– NAT/genotype/viral load– testing throughout treatment
• reliable supply of medication
• dispensing capacity
• clinical skills– somewhat complicated treatment algorithms– potentially life threatening adverse events common

39
models of caremodels of care
• non-integrated– referral– linkage
• integrated care– integrated in general health care
• primary care– multi-skilled team– specialist outreach
• integrated in district hospital– integrated specialist services
• hepatitis treatment provided in drug treatment– multiskilling or specialist outreach
• drug treatment provided in hepatitis clinic• combined addiction and hepatitis specializations

40
HIV ProgramAntiretroviral TreatmentDrug InteractionsVCTToxicity MonitoringProphylaxis of OIsAdherence SupportSecondary PreventionSyringe Exchange
Hepatitis ProgrammeDOTDiagnosisStagingAlcohol counsellingTreatment monitoringAdherence SupportDrug Interactions
Drug TreatmentOpioid Substitution TherapyEffective CounselingDOTUrine MonitoringDrug InteractionsSyringe Exchange
CommunicationCollaboration
Communication
Collabora
tion
Comm
unication
Collaboration

41
Case example - UkraineCase example - Ukraine
• Before– example of OST / HIV / TB in Ukraine many years ago
• OST on one side of town, HIV medication on another• no OST in TB hospital…
• Now– multiple models of care
• ARVs in narcology dispensaries• OST in HIV services• both ARV and OST in primary care and public hospitals

42
• Collaboration of 150 NGOs, organised HCV treatment for co-infected individuals
• Negotiated price reduction of interferon and ribavirin from $20,000 to $5,000 dollars per course
• Decentralised approach– “Aids Clinic”– OST clinics– Community Clinics
• Integrated into harm reduction/ART delivery.
• Doctors providing the majority of care
• Estimated to have treated 100 people,
• Issues now with the political instability and clinics in Crimea and Eastern Ukraine have closed

43
Case example - TanzaniaCase example - Tanzania
• Muhimbili medical centre• integrated treatment in an outbuilding of a district hospital• developed by infectious disease unit • integrated treatment:
– drug dependence– HIV– TB– other conditions
• daily dispensing:– methadone– ARV– TB treatment

44
‘One-stop-shop’‘One-stop-shop’
Family support
Overdose, HIV, Hepatitis
prevention
Antiretroviral therapy
General health care
Social assistance &
protection
Mental health care
Drug dependence
treatment
Drug user

45
Current data on treating hepatitis in PWUDCurrent data on treating hepatitis in PWUD

46

47
USA14
CANADA4
AUS8
N.Z.1
SUISSE1
SCOTLAND 2
ENGLAND3
UKRAINE1
ITALY3
NETHERLANDS1
Geographic distribution of models of care

48
Addiction Centres
GP Practices Prison Patient's home
"Public Health Cetres"
Sexual Health Clinic
Specialist HCV clinic
0
2
4
6
8
10
12
14
16
18
2018
13
6
1 1 1 1
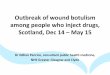
Characteristics of Health Care Setting providing HCV care in 38 models of care
Location of HCV treatment
Number of models

49
How to increase rates of adherence in treating PWUD
How to increase rates of adherence in treating PWUD
• accessible
• affordable
• non judgemental
• train staff in how to manage other issues faced by PWUD– psychosocial skills– encourage and provide OST for people who are opioid dependent
• employ people with a history of drug use
• work with the local drug using community
• offer case management and outreach services

50
Other drug and alcohol activities at WHOOther drug and alcohol activities at WHO
• UNODC/WHO programme on drug dependence treatment and care
• mhGAP programme on management of mental health, substance use and neurological conditions in non specialist settings

51

52

53
mhGAP-IG standard course - pilot test version – Oct 2012
53

54

55

56
SummarySummary
• Safe and effective treatment is now available and will be affordable in many low income settings
• PWID have excellent rates of SVR in published trials
• Need to avoid PWID being left behind in the hepatitis treatment scale up
• Need to support the development of the right treatment models

57
SummarySummary
• Support country level hepatitis epidemiology that includes drug use as a risk factor and comorbidity
• Support the development of hepatitis national plans that include appropriate level of concern to PWID
– Support screening in IDU• drug treatment and outreach
– rapid testing and prequalification of diagnostics– reliable supply of medication– alcohol reduction advice– effective models of care for PWID
• OST
• Support the implementation of national plans
• Monitor progress

58
HIV/AIDS(HIV)
Pandemic and Epidemic Diseases
(PED)
Food Safety, Zoonoses and
Foodborne Diseases
(FOS)
Service Delivery and Safety (SDS)
Essential Medicines and
Health Products
(EMP)
Health Statistics and Information
Systems (HSI)
Management of Noncommunicable Diseases (MND)
Immunization, Vaccines and Biologicals
(IVB)
Mental Health and
Substance Abuse (MSD)
Country Offices
WHO's internal organization of the Global Hepatitis ProgrammeWHO's internal organization of the Global Hepatitis Programme
Country Offices
AFRO EURO SEARO
AMRO EMRO WPRO
RegionalOffices
GHP Secretariat
HQ

59
Thank youThank you