Embed Size (px)
Citation preview

14-‐02-‐13
1
GENETICS
Keys to success in Gene9cs #1 – #2 – #3 – #4 – #5 -‐
Important terminology in Gene9cs Heteroplasmy: Variable expression: Incomplete penetrance: Loss of heterozygosity: Imprin9ng: Pleiotropy: An9cipa9on: Mosaicism:
PEDIGREE INTRODUCTION

14-‐02-‐13
2
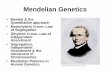
Autosomal Dominant Disorders
• Defect of a single gene leads to the disease • 50% chance of inheritance of AD disorder
Autosomal Dominant Inheritance
Tuberous Sclerosis
• Mul9 organ disorder • Non-‐malignant tumors grow abundantly Hamar9a à Malformed 9ssues Hamartomas à Benign growths Muta9on of 2 genes: ________ & ________ Codes for proteins called: ___________ &______________

14-‐02-‐13
3
Tuberous Sclerosis
• Follows the 2-‐hit hypothesis Brain tumor associated with TS = ____________ Dermatological findings include: -‐ Ash-‐leaf spots [fair skinned pt use Wood’s lamp] à Renal angiomyolipoma
Marfan Syndrome Muta9on of _________ gene on Chrom ____. Encodes for the Fibrillin-‐1 protein. à Fibrillin-‐1 is a component of the ECM These situa9ons look like Marfan’s syndrome: -‐ Homocys9nuria -‐ Congenital contractural arachnodactyly -‐ Ehlers-‐Danlos syndrome -‐ S9ckler syndrome -‐ MEN 2B
Marfan Syndrome
Findings: à Above average height à Arachnodactyly à Spinal abnormali9es à Lens disloca9on (upper por9on: pa9ent has trouble seeing above eye level)
à Aor9c aneurysm OR dilated aorta à Dural ectasia
Neurofibromatosis
Type 1 à Von Recklinghausen disease -‐ Muta9on of _______________ 1 gene, which is found on Chrom _______. -‐ Tumor suppressor gene ________________ works to inhibit the p21 ras oncoprotein.
Type 2 à Central neurofibromatosis -‐ Muta9on of the ___________ protein found on Chrom ______.

14-‐02-‐13
4
Neurofibromatosis Type 1
Diagnosed by finding: à Café-‐au-‐lait spots
à Neurofibromas
à Lisch nodules
Neurofibromatosis Type 2
Diagnosed by finding: à Bilateral acous9c neuromas (CN 8 aka Schwannoma)
Tumors can cause: -‐ HA -‐ Balance problems -‐ Facial weakness/paralysis (CN7 compression)
Hun9ngton’s Disease
• Trinucleo9de repeat disorder (CAG) • Demonstrates gene9c an9cipa9on • CAG encodes for the AA _______________
Affected gene = _______________, and is located on Chrom _____. Affected gene encodes for the __________ protein.
Hun9ngton’s Disease
• Hypermethyla9on of AA residues leads to the respression of transcrip9on
Gene9c muta9on leads to atrophy of the ______________ nucleus, which causes loss of GABAergic neurons. Diagnosis made by:

14-‐02-‐13
5
Hun9ngton’s Disease 2 forms of the disease: 1. Adult onset 2. Early onset
Findings: -‐ Personality changes -‐ Chorea -‐ Muscle rigidity -‐ Writhing -‐ Psychomotor func9on worsens -‐ Impaired execu9ve planning -‐ Short & long-‐term deficits
Hun9ngton’s Disease Neuropsychiatric Manifesta9ons include: -‐ Anxiety -‐ Depression -‐ Blunted affect -‐ Aggression -‐ Compulsive behaviors
Management: No cure à Can regulate with CNS depressants
Re9noblastoma
Re9nal cancer caused by muta9on of the _______ gene on Chrom _____. à Re9noblastoma protein a regulator of the G1àS phase transi9on
Hyperphosphorylated protein = ____________ Hypophosphorylated protein = _____________
Re9noblastoma
• Screening part of ‘well baby’ screening
Looking for the: 1. Red reflex (red/orange re9nal reflec9on) 2. Corneal light reflex (symmetrical reflec9on)

14-‐02-‐13
6
Re9noblastoma
Findings: -‐ Leukocoria -‐ Deteriora9ng vision -‐ Irrita9on of the eye -‐ Concurrent glaucoma -‐ Enlargement of the eye
Myotonic Dystrophy
• Chronic, slowly progressing mul9systemic disease characterized by:
à Was9ng of the muscles à Cardio disturbances à Endocrine disorders à Visual disturbances
2 types: Type 1 (Steinert diz) Type 2 (PROMM)
Myotonic Dystrophy
Type 1: DMPK gene à On long arm of chromosome _____ à Encodes _________________ protein kinase à Is a trinucleo9de repeat disorder (CTG)
Type 2: ZNF9 gene à Found on chromosome _____ à Tetranucleo9de repeat disorder (CCTG)
Familial Hypercholesterolemia
• Muta9on of _____ gene that encodes the LDL receptor protein
• Gene located on chromosome _____ located on the short arm of the chromosome.
Main findings: Xanthelasma, tendon xanthomas High risk of __________________, which may lead to CAD

14-‐02-‐13
7
Adult Polycys9c Kidney Disease
• Both AR and AD versions
AD version: 3 muta9ons in PKD-‐1, PKD-‐2, PKD-‐3 PKD-‐1 gene located on Chrom _____ and codes for a protein that regulates the cell cycle & intracellular transport of _______________ in epithelial cells.
Adult Polycys9c Kidney Disease Findings in the kidney: -‐ Mul9ple cysts on both kidneys
Extrarenal findings: -‐ Cerebral aneurysms -‐ Pancrea9c & hepa9c cysts -‐ Mitral valve prolapse -‐ Aor9c root dilata9on -‐ Colonic diver9cula
Von Hippel Lindau
• Caused by muta9on of the ______ tumor suppressor gene located on Chrom ____.
Pa9ents develop: -‐ Benign & malignant tumors (MC In CNS) -‐ Capillary hemangioblastomas in re9na -‐ Clear cell renal carcinoma -‐ Pheocromocytoma -‐ Pancrea9c neuroendocrine tumors
Von Hippel Lindau
Diagnosis: Family hx + sx men9oned above Management: No cure à Rou9ne screenings important à Early recogni9on + symptoma9c tx can improve quality of life

14-‐02-‐13
8
Achondroplasia
• MCC of dwarfism
à Fibroblast growth factor receptor 3 (FGFR3) muta9on (at the epiphyseal growth plate)
à Results in abnormal car9lage forma9on
* No effect on intelligence
Achondroplasia
Findings: -‐ Short stature -‐ Large head-‐to-‐body size difference -‐ Prominent forehead -‐ Decreased muscle tone -‐ Bowed legs -‐ Spinal stenosis -‐ Kyphosis and lordosis
Acute Intermitent Porphyria • Heme produc9on disturbed • Porphobilinogen deaminase deficiency • 2nd MC porphyria (auer Cutanea Tarda)
Findings: -‐ Severe abdominal pain -‐ Peripheral neuropathy -‐ CNS signs ** NO RASH
Von Willebrand Disease
Type 1 & 2 = AD Type 3 = AR • vWF deficiency • vWF required for platelet adhesion • vWF gene located on Chrom ____

14-‐02-‐13
9
Von Willebrand Disease Presenta9on: -‐ Easy bruising -‐ Nosebleeds -‐ Bleeding gums -‐ Heavy menstrual periods (females)
Type 1: Quan9ta9ve defect in vWF (Majority of cases) Type 2a: Qualita9ve defect (normal quan9ty) Type 2b: Hyperbinding of vWF to glycoprotein 1 Type 3: Complete absence of vWF (most severe)
Von Willebrand Disease
Diagnosis: à Measure vWF quan9ty in a vWF an9gen assay à Measure vWF func9onality with any of (glycoprotein 1b binding assay’, collagen binding assay’, ristoce9n cofactor ac9vity’)
Mgmt: Desmopressin MOA: S9mulates release of vWF from Weibel Palade bodies of endothelial cells + increases vWF levels
Osteogenesis Imperfecta
• Qualita9ve or quan9ta9ve deficiency of type 1 collagen (decreased structural quality of collagen)
• Glycine is replaced with bulky amino acids
Osteogenesis Imperfecta
Type 1 – MILD… COL1A1 gene Type 2: LETHAL.. COL1A1 & COL1A2 gene Type 3: Progressive/deforming Type 4: Deforming, normal sclera Type 5: Similar to type 4 (histology = mesh-‐like) Type 6: Similar to type 4 (histology = Fish scale) Type 7: CRTAP gene, car9lage associated protein Type 8: Severe/lethal, Leprecan protein (LEPRE1 gene)

14-‐02-‐13
10
Osteogenesis Imperfecta
Findings: -‐ Bone fragility -‐ Spinal curvature -‐ Loose joints -‐ Poor muscle tone -‐ Blue sclera (see underlying choroidal veins) -‐ Hearing loss
Hypokalemic Periodic Paralysis
• Defect in CNA4A gene • Defect in voltage-‐gated calcium channels (blood K+ levels fall rapidly)
Main findings: -‐ Muscle weakness/paralysis -‐ Lasts hours to days
Hypokalemic Periodic Paralysis
Management: -‐ Focuses on preven9ng future atacks -‐ Avoid high-‐carb meals, strenuous exercise, other triggers
à K+ sparing diure9c like ________________ can keep K+ levels elevated
Hereditary Spherocytosis
• Defect in RBC’s cytoskeleton (due to Spectrin & Ankyrin abnormali9es)
Classic Manifesta9ons: -‐ Jaundice -‐ Hemoly9c anemia -‐ Splenomegaly

14-‐02-‐13
11
Hereditary Spherocytosis
Findings: -‐ Oval-‐shaped RBCs (Elliptocytosis) -‐ RBC small/red, no central pallor -‐ Re9culocytosis / incr RDW / incr MCHC
Confirm with _____________ fragility test
Li-‐Fraumeni Syndrome
• Early cancer development due to p53 gene muta9on
• Requires inherited muta9on of p53 + soma9c muta9on of 2nd allele
à Look for mul9ple cancers in someone < 45yr of age
à MC tumors in breast, adrenal cortex, brain, blood, & sarcomas
Osler-‐Weber-‐Rendu Syndrome
• Hereditary hemorrhagic telangiectasia
Findings: Telangiectasias in skin + mucus membranes of the lips/oronasopharynx/respiratory tract/GI tract/urinary tract à Rupture leads to epistaxis, GI bleeding, hematuria
Essen9al Tremor • Worsens with ac9vity • MC in upper extremity Classic finding: Improves with ___________ consump9on Management: _________________ MOA: Non-‐selec9ve beta blocker Why it works à Suppresses tremor through beta-‐2 blockade

14-‐02-‐13
12
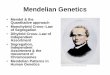
Autosomal Recessive Disorders
• MC enzyme deficiencies • There is a 25% chance of inheri9ng an AR disorder
Autosomal Recessive Disorders
Autosomal Recessive Inheritance

14-‐02-‐13
13
CYSTIC FIBROSIS
• Muta9on of _______________ gene • Dele9on of 3 nucleo9des that code for ______ results in the loss of Phenylalanine
CFTR is an ______-‐binding transmembrane ion transporter.. Pumps __________ ions out of the epithelial cells.
Cys9c Fibrosis (Sweat Gland)
Cys9c Fibrosis (Lungs) Phenylketonuria (PKU) • Deficiency of ______________ hydroxylase • Cannot convert Phe à Tyr
If we can’t make Tyr, we wont get: -‐ DA -‐ NE -‐ EPI
If we can’t make Melanin, we see: -‐ Light skin -‐ Blonde hair -‐ Blue eyes

14-‐02-‐13
14
PKU
Accumula9on of the following: à à à ** These account for the musty odor Mgmt: Eliminate _____ from the diet, add _____
Cys9nuria • Get forma9on of cys9ne stones in the kidney, ureter, & bladder.
Muta9ons in _________ & _________ genes, which encodes for transporter protein in kidney. Findings: -‐ Flank pain -‐ Radia9ng pain to the groin
Mgmt: Fluids to dilate urine / lithotrypsy for big stones
Alkaptonuria
• Deficiency of Homogen9sic acid oxidase • Muta9on of ______ gene
Body cannot breakdown _______ & _______. Findings: Urine darkens upon standing (Dx factor) Infant à darkened urine in diaper Adults à Arthri9s, darkening of ear, dark spots on sclera
Galactosuria • Benign spilling of galactose into the urine • Deficiency of _______________ enzyme • Due to muta9on of the _______ gene, located on Chrom _____.
Worrisome complica9on is CATARACTS, caused by accumula9on of ____________ in the lens. Mgmt: If cataracts we remove them… à Eliminate ____________ & ____________ from the diet.

14-‐02-‐13
15
Galactosemia
• Deficiency of _________________________ leads to accumula9on of Gal-‐1-‐Phosphate.
Lactase breaks down Lactose into these 2 sugars: 1. 2.
Galactosemia Findings: -‐ Feeding problems -‐ Failure to thrive -‐ Liver damage/failure -‐ Bleeding -‐ Infec9ons
Without treatment, what happens to levels of ammonia? Mgmt: Restrict ______________ in the diet.
Gaucher’s Disease
• MC lysosomal storage disease • Dysfunc9onal metabolism of sphingolipids Deficiency of ____________________ enzyme. Defec?ve gene is the _____________________, which is on Chrom 1q21. à See accumula9on of _________________ in the lysosomes.
Gaucher’s Disease Three MC types: Type 1: MC form à Non-‐neuropathic à Hepatosplenomegaly
Type 2: Acute infan9le neuropathic à Within 6 months of birth à H/S megaly à Neuro findings
Type 3: Chronic neuropathic form à From childhood into adulthood à Slowly progressing neuro sx
Mgmt: Type 1 & 3 = Replace enzyme

14-‐02-‐13
16
Gangliosidoses
• Lipid storage disorder whereby lipids are accumulated • TWO types (GM1 & GM2)
GM1: Deficiency of Beta-‐Galactosidase Early infan?le: Neurodegenera9on, seizure, H/S megaly, coarsening of facial feat., skel abn. Late infan?le: Between 1-‐3 yr, (ataxia, seizure, demen9a, speech difficulty) Adult onset: Muscle atrophy, less severe/slower-‐developing neuro findings
Gangliosidoses
GM 2: Deficiency of Beta-‐Hexosaminidase à Enzyme found in lysosomes à Lipids accumulate in nervous 9ssue (leads to neuro findings)
Hartnup’s Disease Muta9on of _______________ gene on Chrom ____.
Affects absorp9on of non-‐polar AA’s (most importantly: __________) TRP needed because it converts to the following: -‐ Serotonin -‐ Melatonin -‐ Niacin
Hartnup’s Disease Findings: -‐ FTT -‐ Photosensi9vity -‐ Nystagmus -‐ Ataxis (intermitent) -‐ Increased AA in the urine -‐ Pellagra (4 D’s)
Mgmt: High ___________ diet (helps overcome deficiency of neutral AA’s) à Avoid sunlight & drugs that cause photosensi9vity Which drugs cause photosensi9vity?

14-‐02-‐13
17
Hurler’s Syndrome
• Lysosomal storage disease • Defect in the ________ gene which is on Chrom _____.
Buildup of: -‐ GAGs (due to deficiency of _____________) -‐ ____________ & _____________ sulfate.
Hurler’s Syndrome
Findings: -‐ Progressive deteriora9on -‐ H/S megaly -‐ Dwarfism -‐ Progressive mental retarda9on -‐ Death by end of __st decade of life
Mgmt: Enzyme replacement
Krabbe’s Syndrome
• Defect in sphingolipid metabolism • Causes degenera9on of _________ sheath in the CNS
Muta?on of ________ gene located on chrom__ Deficiency of _________________ enzyme.
Krabbe’s Syndrome Findings: Start 3-‐6 months auer birth -‐ Irritability -‐ Fever -‐ Seizure -‐ Feeding difficulty -‐ Vomi9ng -‐ Mental/motor regression -‐ Muscle weakness -‐ Spas9city -‐ Deafness -‐ Op9c nerve atrophy
Mgmt: BM transplant

14-‐02-‐13
18
Maple Syrup Urine Disease • Deficiency of _________________________ Muta?on in 4 genes: 1. BCKDHA 2. BCKDHB 3. DBT 4. DLD This enzyme required to breakdown BCAA’s: à à à
Maple Syrup Urine Disease Findings: à Sweet-‐smelling urine -‐ Poor feeding -‐ N/V -‐ Dehydra9on -‐ Lethargy -‐ Hypoglycemia -‐ Ketoacidosis -‐ Neuro findings
Mgmt: Avoid BCAA’s & foods rich in them à Avoid nutrasweet
Metachroma9c Leukodystrophy
• Lysosomal storage disease • Deficiency of _______________ enzyme.
à Altered G&D of myelin à Build-‐up of Sulfa9des in 9ssue (destroys myelin sheath in CNS & PNS)
Several forms… focus on: Late infan9le, Juvenile form, Adult form
Metachroma9c Leukodystrophy Late Infan9le: MC form seen -‐ Difficulty walking around 2nd year
Juvenile Form: Between 3-‐10yr of age -‐ Progressive symptoms
Adult Form: Auer 16yr of age -‐ Psych disturbances -‐ Progress to demen9a
Mgmt: NO CURE (terminal illnesses)

14-‐02-‐13
19
Ataxia Telangiectasia • Defect in DNA repair genes • The ______ gene is affected à This gene manages the cell’s response to stress induced _________ breaks.
Findings: -‐ Cerebellar atrophy -‐ Oculocutaneous telangiectasia -‐ Telangiectasia -‐ Immune deficiency -‐ Increased cancer risk
Chediak-‐Higashi Syndrome
à Diagnosed in childhood Nuero defects include: Immunodeficiencies include: Skin findings include:
Leukocyte Adhesion Deficiency
• Gene9c absence of CD___ • Disturbs forma9on of Integrins
What are Integrins needed for?
Leukocyte Adhesion Deficiency
Findings: -‐ Late separa9on of _________________ (which is the major sign)
-‐ Poor wound healing -‐ Recurring skin infec9ons -‐ Gingival inflamma9on

14-‐02-‐13
20
Kartagener’s Syndrome
AKA “primary ciliary dyskinesia” Dynein protein defect leads to dynein arm defect. Findings: Any structure depending on mo9lity is nega9vely affected… -‐ Sperm -‐ Cilia à Situs invertus
Hemochromatosis
• Muta9on to _____ gene on Chrom ____. • Abnormally high absorp9on of _____ in the GI
Where is the most important site for HFE gene expression?
Hemochromatosis
Iron overload in the following: -‐ Heart -‐ Pancreas -‐ Liver
TWO most worrisome complica?ons: à Liver cirrhosis à Hepatocellular carcinoma
Wilson’s Disease
• Toxic accumula9on of Copper • Muta9on of the _______ gene on Chrom ____
Neuropsych sx: -‐ Parkinsonism -‐ Seizure/migraine -‐ Demen9a

14-‐02-‐13
21
Wilson’s Disease
Organ-‐specific findings: Eyes: Kayser-‐Fleischer rings (Copper deposi9on in Descemet’s membrane) Heart: Cardiomyopathy Kidneys: Renal tubular acidosis Endocrine: Parathyroid dysfunc9on
Wilson’s Disease Overview of pathophysiology…. Normal physiology: à Copper membrane transporter (CMT1) allows for absorp9on in
stomach & duodenum à Once in the liver is incorporated into an alpha-‐2 globulin (forms
ceruloplasmin).. Via ATP7B protein à Released into plasma as circula9ng Copper
Pathophysiology: à Defect in ATP7B protein à Copper not incorporated into Ceruloplasmin à Copper accumulates in liver (leads to oxida9ve damage)
Wilson’s Disease Making a diagnosis: -‐ Abnormal ______ -‐ Bilirubin is _______ -‐ AST is _______ -‐ Albumin is ____________ -‐ PT is ________________ -‐ Ceruloplasmin levels are _______________ -‐ Serum copper is _____, urine copper is ______ à Confirm diagnosis when liver sample contains at least _____ug of copper
per gram of dried liver 9ssue.
Mgmt: Diet low in copper-‐containing foods à Copper chelator ___________________ binds to copper and is excreted through the urine.
Sickle Cell Disease
MC AR disease in African Americans Main findings: 1. Hemolysis 2. Vaso-‐occlusive sx 3. Infec9ons

14-‐02-‐13
22
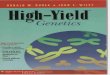
X-‐linked dominant diseases
• X-‐linked dominant diseases and transmited through both parents
• All female offspring of an affected father will be affected
• Both male and female offspring of an affected female may be affected
X-‐linked dominant inheritance
X-‐linked dominant diseases
• Alport’s syndrome • Ret’s syndrome • Vitamin D resistant rickets/Hypophosphatemic rickets
Alport’s Syndrome
Muta9on of _______, ________, & _________ genes, located on Chrom ____. Muta9ons lead to improper produc9on of type ____ collagen, which is required for basement membrane forma9on. Ini9al presenta9on is ouen ______________.

14-‐02-‐13
23
Alport’s Syndrome Diagnosis: Based on finding 4/10 criteria… 1. Bilateral sensorineural hearing loss 2. Muta9on in COL4An (n=3,4,5) 3. Family hx of nephri9s 4. Persistent hematuria 5. Immunohistochemical evidence 6. Ocular lesion 7. Gradual ESRD 8. Macrothrombocytopenia or granulocy9c inclusinos 9. Diffuse leiomyomatosis of the esophagus 10. Glomerular BM abnormali9es
Mgmt: ACEI’s for proteinuria, no known cure.
Ret Syndrome • MC due to spontaneous muta9nos • Spora9c cases due to muta9on to the _______ gene, located on the X
chromosome.
Findings: -‐ motor/language regression (at ~ 6-‐18mnth) -‐ Au9sm-‐like behavior
ReZ specific findings: -‐ Inconsolable crying fits -‐ Screaming fits -‐ Emo9onal inversion -‐ Speech regression -‐ Sensa9on problems
Ret Syndrome Symptoms worsen and may include… à Hypotonia à Gait difficulty à Dystonia à Chorea à Bruxism
Mgmt: -‐ Surveillance for back problems -‐ Social skills development/work
Vitamin D Resistant Rickets • Muta9on in the _______ gene sequence on Chrom Xp___.
• Leads to inac9vity in the _______ protein.
** Not responsive to vitamin D supplementa9on Males à develop outward bowing of knees Females à inward bowing of legs Mgmt: Oral ____________ + _______________

14-‐02-‐13
24
X-‐linked recessive diseases
• No male-‐to-‐male transmission • Sons of a heterzygous (carrier) mother have a 50% chance of transmission
• Affected males always pass one diseased x gene to the daughters (makes them a carrier)
• ONLY MALES ARE AFFECTED
X-‐linked recessive pedigree
Red-‐Green Color Blindness
• Inability to discriminate red & green hues Cause à Absence of red or green re9nal photoreceptors * Males >>>>> Females
Duchenne Muscular Dystrophy • Muta9on of ____________ gene, which is located on the ____ chromosome.
• Codes for protein ___________, an important structural component of muscle 9ssue.
à Dystrophin connects cytoskeleton of each muscle fiber to underlying basal lamina
Microscopically: varia9ons in muscle fiber shape & size, visualize regenera9ng fibers, see increased amounts of connec9ve 9ssue.

14-‐02-‐13
25
Duchenne Muscular Dystrophy Main PHYSICAL sx: Seen 1st 9me they walk -‐ Eventually lose muscle func9on from neck down Gower’s Maneuver à crawls hands up legs to straighten torso Toe Walking à compensatory adapta9on to extensor muscles of the legs Muscle contractures Progressive walking difficul?es à eventual loss by 12yr Pseudohypertrophy of calves à muscle replaced by faty 9ssue
Duchenne Muscular Dystrophy Diagnosis: -‐ Gower’s sign -‐ Elevated crea9ne kinase -‐ EMG demonstrates muscle weakness (not nerve weakness) -‐ Gene9c tes9ng to ID Xp21 gene errors -‐ Muscle biopsy (ID absence of Dystrophin)
Mgmt: To control sx & improve quality of life -‐ Steroids -‐ Beta2 agonists -‐ No-‐impact ac9vi9es -‐ Orthopedic appliances -‐ Respiratory support
Prognosis: Max 25yr lifespan
Becker’s Muscular Dystrophy • Similar but less severe than Duchenne • Muta9on in ____________ gene that encodes Dystrophin Important difference: Only less Dystrophin made (Duchenne there is none made) à Progressive muscle weakness à Toe-‐walking à Modified Gower’s maneuver
Diagnosis: EMG + Check CPK levels
Hemophilia A • Deficiency of clo�ng factor 8 • Sx vary with severity
Most serious bleeding occurs into: -‐ Joints -‐ Muscles -‐ GI -‐ Brain
Diagnosis: Increased PTT, normal PT & normal bleeding 9me. Mgmt: Severe cases required IV recombinant or plasma concentrate factor ___. Mild cases managed with _________________, which works by released stored factor 8 from the endothelial walls.

14-‐02-‐13
26
Hemophilia B • Muta9on of Factor 9 gene, leading to Factor 9 deficiency • Less common than Hemophilia A • Aka “Christmas Disease”
Findings: -‐ Nosebleeds -‐ Easy bruisability -‐ Blood in urine & stool -‐ Excessive bleeding with minor injury
Diagnosis: Low factor 9, abnormal PTT, normal PT & normal bleeding 9me. Mgmt: Infusion of factor ____.
X-‐Linked Mental Retarda9on
• MC in males • Around ______ genes involved in this type of mental retarda9on
à In MALES, XL mental retarda9on accounts for around ___% of all cases.
X-‐Linked SCID
• MCC of SCID • 2nd MCC of SCID is __________________ def. Defec?ve gene à IL2-‐RG, located at ________ on the X chromosome
à Litle produc9on of ___ cells and ____ cells. à Also leads to defect in B cells
Glucose-‐6-‐Phosphate DH Deficiency
• Disorder of the HMP shunt • The amount of ____________ produced within the RBCs is
low… impairs ___________-‐mediated inac9va9on of free radicals
Findings: -‐ Hemoly9c anemia
Other Causes: drugs, fava beans, infec9ons Microbiology: Peripheral smear demonstrates ______ cells & Heinz bodies.

14-‐02-‐13
27
Ornithine Transcarbamoylase Deficiency
• Is XLR • Urea cycle defect • Due to a few muta9ons in OTC gene
à Body cannot eliminate ammonia à Oro9c acid builds up
Ornithine Transcarbamoylase Deficiency
Findings: -‐ Lethargy -‐ Anorexia -‐ Temp/breath regula9on difficulty Mgmt: Low protein diet à Maintain adequate hydra9on à Nitrogen-‐scavenging meds (Sodium Benzoate, Sodium Phenylbutyrate)
à Bio9n supplementa9on
Mitochondrial diseases
• Transmission is only through the mother • Father doesn’t pass mitochondrial material • All offspring of an affected female may show signs of being diseased
Mitochondrial diseases

14-‐02-‐13
28
High-‐Yield mitochondrial diseases
• Leber’s hereditary op9c neuropathy • DM + Deafness (DAD) – a combina9on • Leigh syndrome • MERFF syndrome (myoclonic epilepsy with ragged red fibers)
Leber’s Hereditary Op9c Neuropathy
à Any of 3 muta9ons in maternal mitochondrial DNA (ND1, ND4, or ND6) genes of complex 1 of the oxida9ve phosphoryla9on chain • Degenera9on of re9nal ganglion cells & their axons
• Leads to acute or subacute loss of central vision
Leber’s
Findings: -‐ Acute onset of visual loss (one eye at a 9me) -‐ Usually in younger adults -‐ Females present 5yr earlier than males -‐ Severe op9c atrophy + permanent visual acquity disturbances
Mgmt: Idebenone
DAD Syndrome
• Associated with ___________ gene Causes: -‐ DM -‐ Sensorineural deafness

14-‐02-‐13
29
Leigh Syndrome
à AKA ‘subacute necro9zing encephalomyelopathy’
à _______-‐1 gene is affected
Findings: -‐ Dystonia -‐ Motor findings (tremor, rigidity, chorea) -‐ Later finding is renal/resp impairment
MERFF Syndrome • Several genes involved à MT-‐TK, MT-‐TL1, MT-‐TH, MT-‐TS1, MT-‐TS2, MT-‐TF
Findings: -‐ Progressive myoclonic epilepsy -‐ Ragged red fibers -‐ Hearing loss -‐ Lac9c acidosis -‐ Short stature -‐ Exercise intolerance
Mgmt: No cure
TRINUCLEOTIDE REPEAT DISORDERS
Trinucleo9de repeat disorders • Diseases that result from trinucleo9de repeat expansions
• The genes are expanded beyond the point which allows them to be stable
• Trinucleo9de repeat disorders demonstrate the phenomenon of ‘an9cipa9on’
An?cipa?on: MOA:

14-‐02-‐13
30
MC trinucleo9de repeat diseases
• Hun9ngton’s disease (discussed earlier) • Spinocerebellar ataxia • Fragile x syndrome • Friedreich’s ataxia • Myotonic dystrophy (DM1 = trinucleo9de, DM2 = tetranucleo9de)
Spinocerebellar Ataxia
• Several varia9ons of this disease • Many genes involved (SCA1, SCA2, SCA3) • All forms of the disease are polyglutamine diseases (CAG repeat)
• Both AD varie9es & AR varie9es
Spinocerebellar Ataxia Findings: -‐ Slow progression of uncoordinated gait -‐ Poor coordina9on of hands/speech/eyes -‐ Inten9on tremor -‐ Cerebellar atrophy -‐ Lack of fine-‐motor coordina9on
Mgmt: no defini9ve cure à Manage symptoms as they occur
Fragile X Syndrome
• MCC of mental retarda9on in males • 2nd MCC of congenital mental retarda9on (auer Down’s)
• Due to expansion of the ______ trinucleo9de repeat on the _______ gene, on the _______ arm of the X chromosome

14-‐02-‐13
31
Fragile X Syndrome Findings: -‐ Short-‐term memory deficits -‐ Visual memory deficits -‐ Visual-‐spa9al rela9onship difficul9es • Verbal abili9es rela9vely normal
Other Findings: -‐ Mild to severe mental retarda9on -‐ Elongated face -‐ Short height -‐ Joint laxity -‐ Scoliosis -‐ High-‐arched palate -‐ Large protruding ears -‐ Hypotonia -‐ Macroorchidism -‐ MVP
Friedreich’s Ataxia • GAA repeats of the _____ gene • Affects the _____________ protein, which is an iron-‐binding protein
• Sclerosis & degenera9on of the dorsal root ganglion, spinocerebellar tracts, lateral CS tracts, & posterior columns
What does a low level of Frataxin lead to? Where is the primary site of pathology?
Friedreich’s Ataxia Signs & Anatomical Problems: In the limbs à Dorsal columns à LMN lesions à Pyrimidal à Cerebellar findings à Cardiac à Endocrine à Skeletal à * Death on average by 35th year of age
Myotonic Dystrophy
• Chronic, slow-‐progressing, mul9systemic • 2 types (1 = Steinert disease, 2 = Proximal myotonic myopathy)
Characterized by: -‐ Muscle was9ng -‐ Cardio/endocrine/visual disturbances

14-‐02-‐13
32
Myotonic Dystrophy Type 1: Steinert’s disease -‐ Affected gene is the _______ gene on the long arm of Chrom _____
-‐ Encodes the myotonic dystrophy protein kinase -‐ CTG triplet repeat
Type 2: PROMM -‐ Defect in the ______ gene on Chrom ____ -‐ Tetranucleo9de repeat disorder of CCTG nucleo9des
MONOSOMIES & TRISOMIES
MONOSOMIES – Turner Syndrome • 45XO (one x chromosome is missing) • MCC is non-‐disjunc9on
Common findings: à à à à à
MONOSOMIES – Cri-‐du-‐chat syndrome
• Par9al dele9on of short arm of chromosome 5 • MCC by spora9c muta9on
Findings: à à à à à à

14-‐02-‐13
33
TRISOMIES – Patau Syndrome
• Extra copy of chromosome 13 • Caused by Robertsonian transloca9on
Findings: à à à à
TRISOMIES – Edward’s Syndrome
• Trisomy 18 • Rocker-‐botom feet
Findings: à à à à
TRISOMIES – Down’s Syndrome
• Trisomy 21 • MC chromosomal abnormality • 2nd MCC of mental retarda9on
à Triple test at 16-‐18 weeks gesta9on… we are looking for low levels of ____________
Organ-‐Specific Findings… Cardiac :
Vascular: Cancer:
Thyroid:
Gastrointes9nal:
Infer9lity:
Neurological:

14-‐02-‐13
34
Klinefelter Syndrome • 47XXY karyotype • Due to meio9c non-‐disjunc9on during gametogenesis
Will cause: à Eunuchoid body habitus: à Cogni?ve findings: à
DiGeorge Syndrome
• Dele9on of long arm of chromosome 22 (22q11.2) • Thymic aplasia and failure of parathyroid forma9on • Caused by defec9ve embryonic development of the 3rd and 4th pharyngeal pouches
Findings: Ini?al presenta?on: CATCH 22:
IMPRINTING
HY Imprin9ng
Beckwith-‐Wiedemann: Angelman syndrome: Prader-‐Willi:

14-‐02-‐13
35
ALZHEIMER’S DISEASE
Alzheimer’s Disease • Early onset (<60yr) • Late onset (>60yr)
Muta?ons associated with early onset: 1. 2. 3. Muta?ons associated with late onset: à ε4 allele of Apolipoprotein E (causes senile plaques)
HARDY-‐WEINBERG GENETICS
Assump9ons
In order to maintain HW equilibrium, we assume the following: 1. 2. 3. 4.

14-‐02-‐13
36
Major viola9ons to the HW equilibrium
Inbreeding: Small pop’n size: Assor9ve ma9ng:
Hardy-‐Weinberg Equilibrium
HWE p = q = p^2 = q^2 = 2pq =