Embed Size (px)
Citation preview
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 391S, pp. S231–S243© 2001 Lippincott Williams & Wilkins, Inc.
S231
Low-intensity pulsed ultrasound acceleratesbone healing via upregulation of cartilage for-mation and maturation phases of endchondralbone formation. The current authors evaluatedthe effect of ultrasound therapy on the repair offull-thickness osteochondral defects. Bilateral,3.2 mm diameter by 5.0 mm deep osteochondraldefects were created in the patellar groove of106 adult male New Zealand rabbits. Thedefects were treated with daily low-intensitypulsed ultrasound therapy on the right knee.The left knee was not treated. In Part I, the ef-fect of ultrasound therapy was evaluated at 4, 8,12, 24, and 52 weeks after surgery. In Part II, theeffect of the length of treatment (5, 10, or 40minutes of daily ultrasound therapy) comparedwith standard 20 minute therapy was evaluated.The repair cartilage was evaluated and gradedon a standard scale for the gross and histologicappearance. Ultrasound treatment significantlyimproved the morphologic features and histo-logic characteristics of the repair cartilage com-pared with nontreated controls. Earlier, better
repair with less degenerative changes at latertimes was observed in defects treated with ul-trasound. Doubling the treatment time to 40minutes daily significantly increased the histo-logic quality of the repair cartilage. In the cur-rent animal model, daily low-intensity pulsed ul-trasound had a significant positive effect on thehealing of osteochondral defects.
As many as 650,000 knee surgeries are doneannually to treat articular cartilage damage,including 200,000 with focal chondral defects.Osteochondral defects may occur in any agegroup but occur most frequently in young ac-tive patients.2 Injury commonly is located inthe distal femur or patella and arises frompatellar dislocations, twisting injuries, trauma,or persistent osteochondritis dissecans. Withtime, the injury results in degeneration of the
Improved Cartilage Repair AfterTreatment With Low-Intensity
Pulsed Ultrasound
Stephen D. Cook, PhD; Samantha L. Salkeld, MSE; Laura S. Popich-Patron, BSE; John P. Ryaby, BSE;
Deryk G. Jones, MD; and Robert L. Barrack, MD
From the Tulane University School of Medicine, Depart-ment of Orthopaedic Surgery, New Orleans, LA.John P. Ryaby is an employee of Exogen, Inc, Piscat-away, NJ.Reprint requests to Stephen D. Cook, PhD, Tulane Uni-versity School of Medicine, Department of OrthopaedicSurgery, 1430 Tulane Avenue, SL-32, New Orleans, LA70112.
List of Abbreviations Used
BMP bone morphogenetic proteinEDTA ethylenediaminetetraacetic acidGAG glycosaminoglycanMRNA messenger ribonucleic acidOP-1 osteogenic protein-1TGF-� transforming growth factor-beta

joint surfaces, particularly if the defect is leftuntreated.18
Cartilage is an avascular musculoskeletaltissue with a relatively low capacity for self-regeneration or repair. In the absence of avail-able stem cells, there is little hope for cartilagerepair after injury and the tissue progresses alonga degenerative pathway that destroys the bio-chemical and biomechanical properties. Vari-ous treatments for osteochondral lesions havefailed to achieve universal success. In an at-tempt to bring stem cells into the area of injury,subchondral bone drilling or the microfracturetechnique has been advocated.2,18,19 The fibro-cartilage repair tissue formed has a greaterstiffness, permeability and Type I collagen con-tent, and a significantly reduced GAG contentcompared with hyaline cartilage. The inferiorload bearing capacity of the resulting fibrocar-tilage can result in degeneration of the repairwith time necessitating additional reconstruc-tive procedures.
Mosaicplasty or the transplantation of au-tologous osteochondral plugs from nonweight-bearing portions of the knee to a defect site hashad some success.3,14,22 The technique is lim-ited by availability of donor cartilage. In addi-tion, this is an invasive, technically demandingprocedure with the potential of donor site painamong other reported complications.22 Otherconcerns with the procedure include the neces-sity of the donor plugs to conform to the sur-face geometry of the weightbearing surfaceand the long-term disposition of the interfacebetween the plugs themselves.
Autologous chondrocyte transplantation hasshown early success for the treatment of chon-dral defects.5,6,8 The technique consists of har-vesting a small piece of the marginal articularcartilage from the femoral condyle. Retrievedcells are multiplied in explant culture and laterimplanted at the defect under a periosteal flap.Although the early results with this techniqueare promising, the need for multiple surgeries,cost, and the long-term disposition of the repairtissue may limit the use of this technique.21
The use of growth factors including thosefrom the BMP family have been hypothesized
as a potential method to stimulate cell prolif-eration and expression of cartilage phenotypefor chondral defect repair.9,13,29,30 Initial ani-mals studies in which BMP-2 and BMP-7(OP-1) were implanted have shown somepromise.9,13,30 However, these materials arenot yet clinically available and the extrapola-tion of animal results to use in human clinicalapplication is difficult.
All of these interventions involve a surgicalprocedure. Low-intensity pulsed ultrasoundhas been shown to promote the endochondralportion of fracture healing and may influencethe healing of osteochondral defects withoutsurgical intervention.23,24,32,34 Ultrasound hasbeen shown to accelerate fracture healingwhen applied for 20 minutes daily in the non-thermal, low energy level of 30 mW/cm2 range(Sonic Accelerated Fracture Healing System[SAFHS], Exogen Inc, Piscataway, NJ).10,15,16
In a prospective, randomized, double blind andplacebo controlled study of closed or Grade Iopen tibial fractures, Heckman et al15 reportedan approximate 38% decrease in healing timewith the use of daily ultrasound therapy. In asimilar study, Kristiansen et al16 found accel-eration of each stage of fracture healing in dis-tal radius fractures and a 38% decrease in over-all healing time with the use of ultrasound.
Animal fracture models and in vitro studiesof chondrocytes have been used to elucidatethe role ultrasound plays in advancing end-chondral ossification.23,34 Yang et al34 reportedthat when ultrasound was applied to a rat femurfracture model, there was an increase in the ex-pression of genes encoding cartilage produc-tion and therefore the acceleration of fracturehealing was a result of the earlier synthesis ofextracellular matrix proteins in cartilage result-ing in altered chondrocyte maturation and ear-lier endchondral bone formation. In an in vitrostudy using rat chondrocytes, ultrasound stim-ulation resulted in a significant increase in ag-grecan mRNA levels and proteoglycan synthe-sis although cell proliferation and alpha TypeII procollagen mRNA were not affected.23
These findings suggest the ultrasound has adirect stimulatory effect on cartilage forma-
Clinical OrthopaedicsS232 Cook et al and Related Research

tion, maturation, and extracellular matrix pro-duction.
The purpose of the current study was to ex-amine the effect of daily low-intensity pulsedultrasound therapy on the repair of full-thicknessosteochondral defects in a rabbit model. Theeffect of length of ultrasound treatment andduration of daily ultrasound treatment was in-vestigated using gross and histologic analyses.
MATERIALS AND METHODS
Experimental DesignOne hundred six adult male New Zealand Whiterabbits were used. All animals received bilateral,full-thickness osteochondral defects 3.2 mm in di-ameter and 5 mm deep in the central region of thepatellar groove of the femur. The investigation wasconducted in two parts. Part I used 70 animals toexamine the effect of daily ultrasound therapy us-ing the clinically available ultrasound device and20 minute daily treatment time. The right knee inthese animals was treated with 20 minutes of dailylow-intensity pulsed ultrasound 6 days weekly us-ing the commercially available ultrasound signal.The left knee was not treated. Groups of 12 animalseach were sacrificed at 4, 8, and 12 weeks postop-erative. Eighteen animals were sacrificed at 24weeks postoperative. Three groups of six animalseach were sacrificed after receiving 12, 18, or 24weeks of daily ultrasound therapy. Eight animalsreceived daily ultrasound therapy for 24 weekspostoperative and were sacrificed at 52 weeks post-operative, and a final group of eight animals re-ceived daily ultrasound therapy for 52 weeks andwere sacrificed at 52 weeks postoperative.
Part II of the study used 36 animals and inves-tigated the effect of either shortening or lengthen-ing the daily treatment time. The right knee of allanimals was treated for 20 minutes daily with theultrasound device and in groups of 12 animalseach the left knee was treated with either 5, 10, or40 minutes of ultrasound therapy. All animals inPart II of the study were sacrificed at 4 weekspostoperative.
Animal and Surgical ModelAdult male New Zealand White rabbits weighingapproximately 4 kg at acquisition were used. Allanimals were at least 12 months of age. Specific at-tention was given to selecting animals of uniform
size to limit variability in loading of the osteo-chondral defects.
Using standard aseptic techniques, surgery wasdone with the animals under isofluorane gas anes-thesia. The animals were monitored by electrocar-diogram and heart rate monitors. Both hind limbswere prepared and draped in sterile fashion.Through a median parapatellar incision, the con-nective tissue securing the patella was released par-tially to dislocate the patella and expose the medialfemoral condyle and patellar groove. Using a drillbit, a 3.2 mm diameter by 5 mm deep osteochon-dral defect in the patellar sulcus of the femur wascreated by hand. After irrigation with saline, thejoint was closed in layers. Routine anteroposterior(AP) radiographs were taken after surgery to en-sure proper defect location.
Butorphanol tartrate (Fort Dodge Animal Health,Fort Dodge, IA; 0.2 mg/kg body weight) was ad-ministered subcutaneously as required for pain. An-imals were administered intramuscular antibioticsfor 4 days after surgery. Animals were kept in re-covery cages postoperatively until fully consciousand weightbearing, after which they were trans-ferred to standard cages and allowed unrestrictedmotion.
Ultrasound Device and TreatmentThe standard treatment consisted of 20 minutes ofdaily ultrasound therapy with the above describedultrasound device. The ultrasound device delivers alow level acoustic pressure wave signal with an in-tensity of 30 mW/cm2 at a frequency of 1.5 MHz andburst width of 200 �s (equivalent to the intensityused for diagnostic ultrasound) to the skin for 20minutes daily. The ultrasound therapy was adminis-tered 6 days weekly beginning on postoperative Day3. In Part II of the study, ultrasound therapy also wasinvestigated at 5, 10, and 40 minutes of applicationdaily. Animals were sedated by intramuscular injec-tion of ketamine and xylazine (83 mg/mL Ketasetand 17 mg/mL Rompun, Fort Dodge Animal Health)at the dosage of 0.3 mg/kg body weight to adminis-ter the therapy. This dosage is approximately 1⁄2 of theanesthetic dosage intended to provide sedation only.The ultrasound transducer was placed on the distalfemur at the lateral condyle with ample ultrasoundgel. The sites were shaved periodically to ensurecontact between the transducer, coupling gel, and theskin. Each ultrasound device was tested before usewith a signal detector to ensure that the units wereemitting the appropriate signal.
Number 391SOctober, 2001 Ultrasound Improves Cartilage Repair S233

EvaluationsAnimals were sacrificed by an intravenous barbitu-rate overdose (Beuthanasia-D Veterinary Euthana-sia Solution, Schering-Plough Animal Health, Ke-nilworth, NJ; 0.45 mL/kg body weight). Right andleft distal femurs were harvested en bloc, carefullylabeled, and kept in cool physiologic saline untilgross grading and microphotography was com-pleted.
Each harvested knee with a defect was gradedfor gross appearance according to Moran et al20 in-dependently by two observers blinded to the treat-ment group. This analysis apportions points basedon the formation of intraarticular adhesions,restoration of articular surface, erosion, and ap-pearance of the cartilage. Eight points is the bestpossible grade (Table 1).
The individual specimens then were fixed byimmersion in 4% paraformaldehyde solution. Afterfixation, the specimens were decalcified slowly inEDTA. The defect area was bisected across the di-ameter of the defect. The resulting halves and sur-rounding tissue were embedded in paraffin and sec-tioned across the defect site. At least two sections,5 to 7 �m thick, from three different levels were cutfrom each block. Level 1 was closest to the defectcenter. Level 3 was closest to the defect perimeterand Level 2 was centered between Levels 1 and 3.
One section from each level was stained with eitherGoldner’s trichrome or safranin-o and fast greenstains to indicate GAG content in the matrix.
Histologic sections were graded according toCaplan et al,7 which apportions points based on thenature of the repair cartilage, structural characteris-tics, and cellular changes (Table 2). Six sectionsfrom each specimen were evaluated independentlyby two observers blinded to treatment group. Theobserver determined the histologic grade for eachspecimen after examining all of the sections fromthat specimen. Examination of intraobserver errorshowed that the grades from each observer could beaveraged together and a composite grade for eachspecimen could be determined.
Clinical OrthopaedicsS234 Cook et al and Related Research
TABLE 1. Gross Grading SchemeUsed in the Evaluation of theOsteochondral Defects
Intraarticular adhesions GradesNone 2Minimal with fine loose fibrous 1
tissueMajor with dense fibrous tissue 0
Restoration of articular surfaceComplete 2Partial 1None 0
Erosion of cartilageNone 2Defect site or site border 1Defect site and adjacent normal 0
cartilageAppearance of cartilage
Translucent 2Opaque 1Discolored or irregular 0
Total score 8 possible points
TABLE 2. Histologic Grading ScaleUsed in the Evaluation of Sections FromEach Experimental Defect
Cell morphologic features GradesNormal 4Mostly hyaline cartilage 3Mixed hyaline and fibrocartilage 2Mostly fibrocartilage 1Some fibrocartilage, most 0
nonchondrocytic cellsReconstruction of subchondral bone
Normal 3Reduced subchondral bone 2
reconstructionMinimal subchondral bone 1
reconstructionNo subchondral bone 0
reconstructionMatrix staining
Normal 4Slightly reduced 3Reduced 2Significantly reduced 1No staining 0
Filling of defect (cartilage layer)100% 250% or 150% (overfill or underfill) 10% 0
Surface regularityRegular, smooth 1Irregular 0
BondingBoth interfaces bonded 2One interface or partial bonding 1Neither interface bonded 0
Total 16 possible points

Statistical AnalysisBy pairing a nontreated control defect site with anexperimental treatment site within each animal re-duces the effect of individual variations in animalhealing and allows for matched paired compar-isons. One way and two way analysis of variance(ANOVA) was used to screen for any effects of an-imal to animal variance and intraobserver variance.Once shown that neither variable significantly in-fluenced the means, data were pooled. One way andtwo way ANOVA for the evaluation period, treat-ment effect, and length of treatment were used todetermine significance of gross and histologic data.Subsequent post hoc analysis consisted of matchedpaired Student t tests to determine the influence ofultrasound treatment within each evaluation pe-riod. When multiple t test comparisons were made,the Bonferroni correction was used. For all statisti-cal tests, significance was defined as p � 0.05(95% confidence interval).
RESULTS
The animals tolerated the surgical and ultra-sound treatment procedures well. In Part I of thestudy, one animal from the 52 week group died19 days before the scheduled sacrifice date;however, statistical analysis showed that the re-sults from this animal could be pooled with oth-ers in the 52-week group. One animal was elim-inated from the gross and histologic analysis inthe 24-week group because of poor surgical
placement of a defect. Two animals were elim-inated from the 4-week histologic evaluationbecause of infections. One specimen from the8-week histologic analysis was eliminated be-cause of improper histologic sectioning. In PartII of the study, one animal in the 5-minute treat-ment group died at 17 days postoperative ofcomplications related to the administration ofketamine. This animal was not replaced. Twoanimals in the 10-minute treatment group alsowere excluded from the analysis. One animalhad a wound infection at sacrifice. The other an-imal was eliminated because of improper surgi-cal placement of the defect.
Part 1: The Effect of Daily UltrasoundTreatmentUltrasound treated defects had significantlyimproved gross appearance grades at 4, 8, and12 weeks and significantly improved histo-logic grades at 4, 12, 24, and 52 weeks post-operative compared with nontreated controls(Tables 3, 4). Two-way ANOVA for the effectof time and experimental treatment showedthat the postoperative healing period did notsignificantly influence the mean gross or his-tologic grade (p � 0.2968 and p � 0.1315,respectively). The experimental ultrasoundtreatment significantly affected the meangross and histologic grade (both p � 0.0001).Two-way ANOVA found no effect caused by
Number 391SOctober, 2001 Ultrasound Improves Cartilage Repair S235
TABLE 3. (Part I ) Gross Grading Results at Each Evaluation Period, Pair-WiseWithin Animal t Test
Treatment Groups Ultrasound Control p Value
4 weeks 6.6 � 1.0 (12) 5.0 � 1.5 (12) 0.00448 weeks 7.1 � 1.1 (12) 5.9 � 1.4 (12) 0.033312 weeks 6.6 � 1.1 (12) 5.7 � 1.1 (12) 0.049224 weeks (12 weeks of treatment) 6.8 � 1.2 (6) 6.8 � 0.5 (6) NS24 weeks (18 weeks of treatment) 6.3 � 1.0 (5) 6.1 � 0.7 (5) NS24 weeks (24 weeks of treatment) 7.0 � 0.5 (6) 6.3 � 0.8 (6) NS24 weeks pooled 6.7 � 0.9 (17) 6.4 � 0.7 (17) NS52 weeks (24 weeks of treatment) 6.8 � 1.0 (8) 6.3 � 1.4 (8) NS52 weeks (52 weeks of treatment) 6.7 � 1.7 (8) 6.1 � 1.5 (8) NS52 weeks pooled 6.7 � 1.4 (16) 6.2 � 1.4 (16) NS
All groups pooled 6.7 � 1.1 (69) 5.9 � 1.3 (69) 0.0001
*NS � p � 0.05; (mean � standard deviation [sample size]).
increasing the number of ultrasound treat-ments (12, 18, or 24 weeks of ultrasound ther-apy evaluated at 24 weeks, and 24 or 52 weeksof ultrasound therapy evaluated at 52 weeks)on the mean gross and histologic grade (p �0.2386 and p � 0.8550, respectively). How-ever, the ultrasound treatment significantlyimproved the mean gross and histologic grades(both p � 0.0001).
Grossly, at 4, 8, and 12 weeks the ultra-sound treated defects had significantly greatergrades compared with the contralateral non-treated control defects (Table 3). Figure 1 is an
example of the gross appearance of a pair ofosteochondral defects from an animal evalu-ated at 4 weeks. From 8 to 12 weeks, there waslittle improvement in the gross appearance ofthe defects regardless of treatment. The meangross grades for ultrasound and nontreatedcontrol defects improved at 24 weeks over the12 week mean gross grades but the differencewas not statistically significant. From 24 to 52weeks, the ultrasound treated and nontreatedcontrol mean gross grades decreased slightlybut again this did not represent a statisticallysignificant effect. It was difficult to detect ev-
Clinical OrthopaedicsS236 Cook et al and Related Research
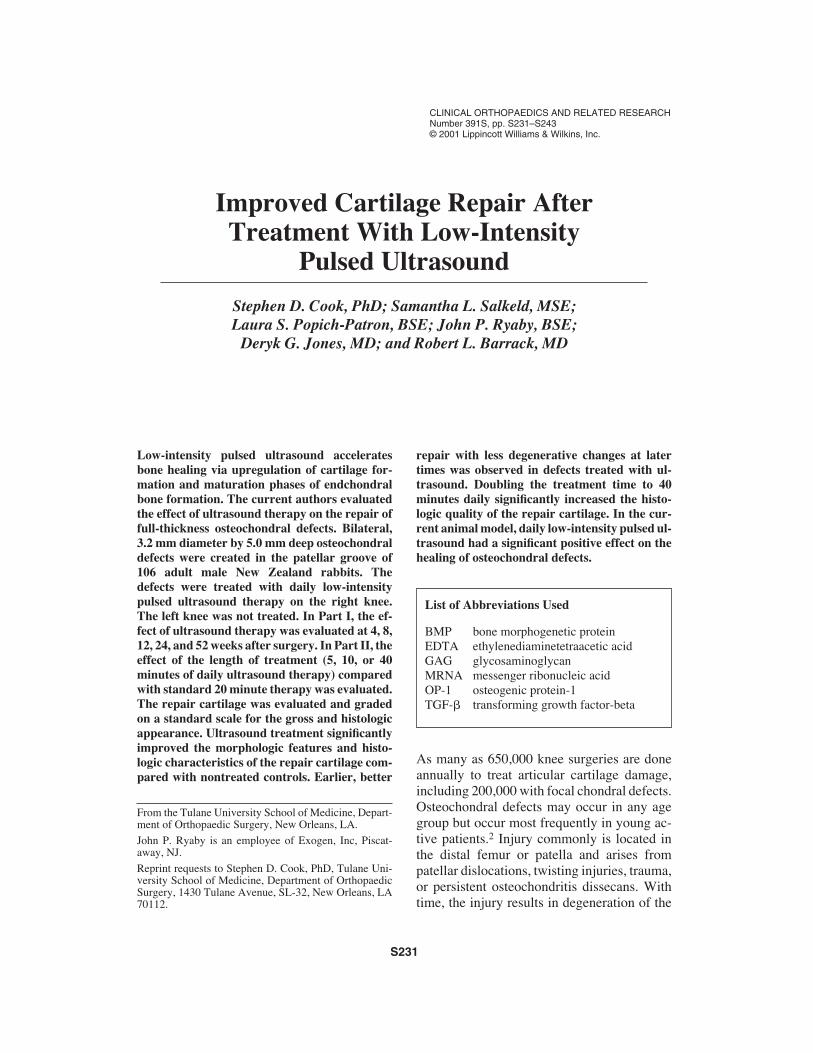
TABLE 4. (Part I) Histologic Grading Results at Each Evaluation Period, Pair-WiseWithin Animal t Test
Treatment Groups Ultrasound Control p Value
4 weeks 9.2 � 2.8 (10) 6.8 � 2.4 (10) 0.01298 weeks 9.4 � 2.9 (11) 9.0 � 2.8 (11) NS12 weeks 9.9 � 1.9 (12) 8.1 � 2.2 (12) 0.000924 weeks (12 weeks of treatment) 10.0 � 3.3 (6) 7.0 � 3.0 (6) 0.013124 weeks (18 weeks of treatment) 9.2 � 1.8 (5) 7.8 � 2.6 (5) NS24 weeks (24 weeks of treatment) 9.7 � 2.4 (6) 7.7 � 2.7 (6) 0.015224 weeks pooled 9.6 � 2.6 (17) 7.5 � 2.7 (17) 0.000252 weeks (24 weeks of treatment) 9.1 � 1.0 (8) 7.3 � 2.1 (8) 0.006852 weeks (52 weeks of treatment) 8.8 � 3.5 (8) 7.6 � 3.7 (8) NS52 weeks pooled 8.9 � 2.4 (16) 7.4 � 2.9 (16) 0.0100
All groups pooled 9.4 � 2.5 (66) 7.7 � 2.7 (66) p � 0.0001
*NS � p � 0.05; (mean � standard deviation [sample size]).
Fig 1A–B. (A) The gross appearance of a nontreated control defect at 4 weeks postoperative. The de-fect is not yet covered with cartilage. The repair tissue is disorganized and easily differentiated fromthe host cartilage. (B) The gross appearance of the contralateral osteochondral defect treated with 4weeks of daily ultrasound. The defect margins are difficult to discern from the host cartilage. The re-pair cartilage has a smooth homogenous appearance.
A B

idence of degeneration grossly in the long-term evaluation because differences were sub-tle and better elucidated from the histologicobservations.
Increasing the number of ultrasound treat-ments did not significantly affect the meangross grades. Osteochondral defects treatedwith ultrasound throughout the 24-week eval-uation had increased mean gross grades com-pared with defects treated with 12 and 18weeks of therapy evaluated at 24 weeks. How-ever, the difference in means was not statisti-cally significant. Figure 2 is an example of the24-week postoperative appearance of a pair ofosteochondral defects from an animal treatedwith 12 weeks of ultrasound therapy. Simi-larly, there was no significant improvement inthe gross appearance of defects treated for 52weeks of ultrasound compared with defectstreated with 24 weeks of ultrasound and eval-uated at 52 weeks.
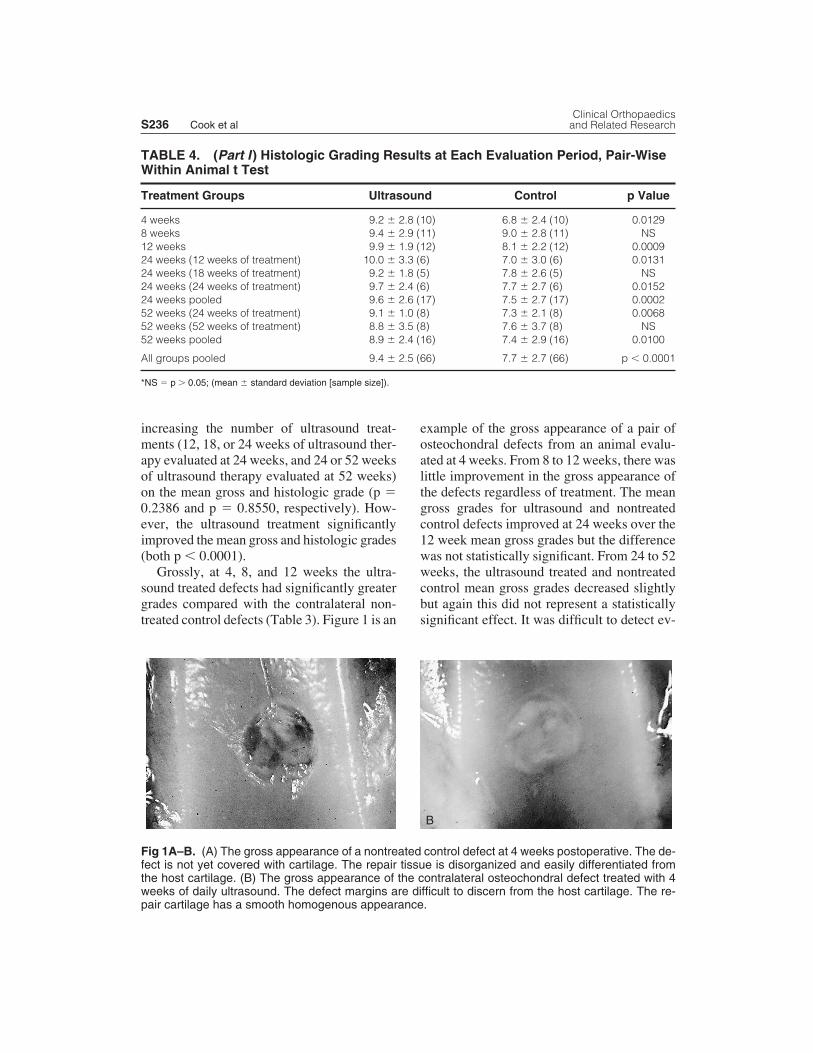
At 4 and 12 weeks postoperative, the ultra-sound-treated defects had significantly greaterhistologic grades compared with contralateralnontreated control defects (Table 4, Fig 3). At8 weeks, the ultrasound-treated defects had aslightly greater mean histologic grade com-pared with controls; however, the differencewas not statistically significant. The mean his-
tologic grades for ultrasound-treated and non-treated defects at the 24 and 52 week evalua-tions did not change significantly from the 12week grades. Similar to the gross results, in-creasing the postoperative ultrasound treat-ment duration from 12 or 18 weeks to 24weeks or from 24 to 52 weeks also did not sig-nificantly affect the mean histologic grades.Figure 4 is a microphotograph of an osteo-chondral defect evaluated at 24 weeks after re-ceiving 12 weeks of ultrasound therapy andthe contralateral nontreated control defect.Statistical analysis showed that, when pooled,the mean total histologic grade for all defectstreated with ultrasound evaluated at 24 weeks(12, 18, and 24 weeks of daily treatment) wassignificantly greater than the mean grade forcontralateral control defects (Table 4). Simi-larly, the pooled histologic grade for the ultra-sound treated defects evaluated at 52 weekswas significantly greater than the mean histo-logic grade for nontreated controls (Fig 5).
Analysis of the subscores of the histologicgrading scale (cell morphologic features, re-construction of subchondral bone, matrixstaining, filling of the cartilage defect, surfaceregularity, and bonding) was done to elucidatethe dynamics of the cartilage repair and dete-rioration process. Specifically, the effect of ul-
Number 391SOctober, 2001 Ultrasound Improves Cartilage Repair S237
Fig 2A–B. (A) The 24-week gross appearance of a nontreated control defect. Although the defect iscovered with repair tissue, the repair has a swollen appearance and is not integrated with the host car-tilage. A large pannus of opaque tissue is present. (B) The 24-week gross appearance of the con-tralateral osteochondral defect treated with 12 weeks of daily ultrasound. The repair cartilage is translu-cent and well integrated with the host cartilage. There is little evidence of degenerative changes andthe articular surface is relatively smooth.
A B
Clinical OrthopaedicsS238 Cook et al and Related Research
trasound treatment was examined in the mark-ers for cartilage regeneration (cell morpho-logic features, matrix staining, cartilage fill-ing) or in the reduction of markers for cartilagedegeneration (matrix staining, surface regular-ity, and bonding).
Initially, it was hypothesized that the im-proved histologic grades in the ultrasound-treated defects was a reflection of earlierrestoration of subchondral bone and subsequentearly reformation of the new cartilage layer.Time and the experimental treatment had a sig-nificant effect on the subchondral bone histo-logic subscore (p � 0.00001 and 0.0120, re-spectively). Although the mean subchondralbone grade was greater at all evaluations in ul-trasound defects, matched paired t tests at eachevaluation period of the mean subchondralbone grades were not statistically significant.
Ultrasound treatment significantly im-proved the surface regularity of the repair car-tilage compared with nontreated controls at 24and 52 weeks postoperative (p � 0.0085 andp � 0.0183, respectively). The surface regu-
larity did not decrease significantly with timein defects treated with ultrasound. However,for nontreated control defects, the mean sur-face regularity grade decreased significantlyfrom 4 weeks to 12, 24, and 52 weeks (p �0.05, 0.05, and 0.01, respectively). Bonding ofthe repair cartilage with the intact host carti-lage also was improved significantly with ul-trasound treatment compared with nontreatedcontrols at 4 and 52 weeks (p � 0.0499 and p� 0.0001, respectively). At 52 weeks, themean grade for bonding in nontreated controlsdecreased significantly from 8 and 12 weekvalues (p � 0.01 and 0.05, respectively). Incontrast, the mean bonding grade at 24 and 52weeks for ultrasound-treated defects was notsignificantly different from earlier periods.The ultrasound-treated defects also had moreanatomic filling of the cartilage defect layercompared with controls at the 24 week evalu-ation (p � 0.0438). Intensity of the extracellu-lar matrix staining for proteoglycans was im-proved significantly in the ultrasound-treateddefects compared with nontreated controls at
Fig 3A–B. (A) A photomicrograph of a nontreated control defect at 4 weeks postoperative. The defectmargins are noted by arrows (Original magnification, �5). A thin layer of subchondral bone has beenregenerated and marrow is present in the defect. The repair layer overlying the early subchondral boneis made up of undifferentiated cells and coarse horizontally oriented fibrous tissue. There is no pro-teoglycan staining within the repair using safranin-o staining. (B) A photomicrograph of a histologic sec-tion of the contralateral osteochondral defect treated with 4 weeks of daily ultrasound (Original magni-fication, �5). The defect margins are noted by arrows. The subchondral bone layer is nearly restoredto its normal height. The repair cartilage is not yet fully organized but has a hyalinelike appearance andintense safranin-o staining. The repair cartilage is bonded to the host cartilage.
A B

12 and 24 weeks (p � 0.0014 and p � 0.0040).The matrix staining subscore mean decreasedsignificantly with time for the ultrasound andnontreated control defects (p � 0.0451 and0.0159, respectively). However, a significantreduction in the matrix staining grade did notoccur until 52 weeks postoperative from the12 week results in the ultrasound treated de-fects (p � 0.05), whereas matrix staining de-creased significantly from 8 to 24 weeks in thenontreated control defects (p � 0.05).
Part II: Evaluation of the Length of DailyUltrasound TreatmentDifferences in the paired mean gross and his-tologic grades for the 5 and 10 minutes of ul-trasound therapy compared with the standard20-minute ultrasound treatment were not sta-tistically significant (Tables 5, 6). However,when gross grading results were pooled, treat-ment with 20 and 40 minutes of ultrasoundsignificantly improved the mean gross gradeover nontreated controls (p � 0.05 and 0.01,
Number 391SOctober, 2001 Ultrasound Improves Cartilage Repair S239
A B
C D
Fig 4A–B. (A) The 24-week postoperative histologic appearance of a nontreated control osteochon-dral defect near the interface of the host cartilage (arrow, gross appearance shown in Figure 2A). Chon-drocyte clusters have formed at the interface and safranin-o intensity is decreased markedly. Cystsalso have formed (Stain, safranin; original magnification, �32). (B) A high power (�80) view of the re-pair tissue in the center of the same defect showing an absence of safranin-o staining, irregular paral-lel arrangement of the collagen fibers, and the absence of a tidemark region into the subchondral bone.(C) The 24-week postoperative histologic appearance of the contralateral defect treated with 12 weeksof ultrasound therapy (Original magnification, �32; gross appearance shown in Figure 2B). The newlyregenerated cartilage layer is slightly thinner than the host cartilage (arrow at the defect margin). How-ever, both are stained with safranin-o in a normal pattern and intensity. (D) A high power (�80) viewof the repair tissue in the same defect showing the columnar arrangement of the chondrocytes, intensesafranin-o staining, a normal tidemark and calcified cartilage zone. Collagen fibers appear to have anorderly arrangement perpendicular to the surface of the subchondral bone.

Clinical OrthopaedicsS240 Cook et al and Related Research
TABLE 5. (Part II ) Gross Grading Results Comparing Ultrasound TreatmentDuration to the Standard 20 Minute Treatment, Pair-Wise Within Animal Comparisons
Standard 20 Minute Treatment Treatment Groups (contralateral defect) p Value
5 minutes 5.7 � 1.0 (11) 6.7 � 0.9 (11) NS10 minutes 6.2 � 1.5 (10) 6.2 � 1.2 (10) NS40 minutes 6.5 � 0.8 (12) 6.0 � 1.2 (12) NS
*NS � p � 0.05; [mean � standard deviation (sample size)].
TABLE 6. (Part II) Histologic Grading Results Comparing Ultrasound TreatmentDuration to the Standard 20 Minute Treatment, Pair-Wise Within Animal Comparisons
Standard 20 Minute Treatment Treatment Groups (contralateral defect) p Value
5 minutes 7.2 � 2.6 (11) 8.2 � 2.5 (11) NS10 minutes 7.8 � 2.9 (10) 7.8 � 2.8 (10) NS40 minutes 8.4 � 2.5 (12) 6.4 � 2.1 (12) 0.0195
*NS: p � 0.05; [mean � standard deviation (sample size)]
Fig 5A–B. (A) A photomicrograph of a histologic section from a nontreated control osteochondral de-fect at 52 weeks postoperative. There is an elevation of the subchondral bone layer in the area of thedefect (arrows at the defect margins). The thin cartilage layer is fibrous and fibrocartilaginous tissue.Safranin-o staining is minimal and severe delamination of the repair from the subchondral bone hasoccurred (Original magnification, �5). (B) A photomicrograph of the contralateral osteochondral defecttreated with 52 weeks of daily ultrasound. The subchondral bone layer is fully restored to its normallevel. The repair cartilage layer is well bonded to the host cartilage and there are few degenerativechanges at the interface. However, there is little safranin-o stain present in the repair which appears tobe a combination of cartilage and fibrocartilage (Original magnification, �5).
A B

respectively). The 40-minute ultrasound treat-ment resulted in the highest mean histologicgrade obtained at 4 weeks postoperative. Dou-bling the ultrasound treatment time from 20 to40 minutes daily significantly improved thehistologic appearance (p � 0.0195) comparedwith the standard 20 minute treatment time(Table 6). However, the difference in the meanhistologic grades for the 5- and 10-minutetreatment lengths compared with the standardtreatment time was not statistically significant.
DISCUSSION
The concept of using biophysical stimulationat a cellular level to modulate tissue formationand repair is not new. Pulsed electromagneticfields, used in the promotion of bone nonunionhealing, may influence the formation of carti-lage and extracellular matrix during endchon-dral bone formation.1 Pulsing direct currentwith a resultant electric field across tissue alsohas been shown to enhance bone and cartilageformation.4,17
Low-intensity pulsed ultrasound is a formof mechanical energy transmitted into the bodyas high frequency acoustic pressure waves pro-ducing micromechanical stresses in tis-sues.11,12 Ultrasound is thought to promotebone formation in a manner comparable withthat first postulated by Wolff ’s Law.33 Bone’sphysiologic response to mechanical force in-cludes the formation, deposition, and resorp-tion of bone. As a result, it not surprising thaton a cellular level, low-intensity ultrasound hasbeen shown to increase 45Ca uptake in cartilageand bone cell cultures, and plays a role in themodulation of TGF-� synthesis and parathy-roid hormone response in mesenchymal andosteoblast cells.25–28 In chondrocytes, ultra-sound upregulates the expression of extracel-lular matrix proteins and collagen phenotypes,precursors in endchondral bone formation.23
It has been shown that daily therapy with low-intensity pulsed ultrasound is safe and beneficialin the treatment of fractures.15,16 In rabbits andhumans, ultrasound accelerates the early eventsof endchondral bone healing.10,11,16,24,32,34 In the
animal model used in the current study, daily ul-trasound therapy had its greatest effect early, be-fore 24 weeks of healing. The gross appearanceof osteochondral defects treated with ultrasoundtherapy was most improved over controls at 4, 8,and 12 weeks. Histologically, the improvementalso was significant at early evaluations. How-ever, at 24 and 52 weeks postoperative as the his-tologic appearance of untreated controls beganto degenerate, less degeneration occurred in theultrasound-treated defects. The early regenera-tion and improved quality of the repair cartilagein the ultrasound-treated defects may help pre-vent or at least delay the degenerative process.
Analysis of the histologic subscores showedthat ultrasound treatment improved markers fordegeneration of the repair tissue particularly atevaluations after 12 weeks. Surface regularitywas improved with ultrasound treatment com-pared with nontreated control defects. In ultra-sound-treated defects, bonding of the repaircartilage to the host cartilage also was main-tained with time and had significantly greaterbonding grades compared with controls at 4 and52 weeks. Surface regularity and bonding de-creased significantly with time in nontreatedcontrol defects. The presence of metachromaticstaining of the extracellular matrix is an indica-tor of hyaline cartilage, whereas the absence ofstaining is indicative of degeneration via pro-teoglycan loss and change in the biochemicalcomposition of the tissue. Significantly in-creased matrix staining and a delay in the re-duction of matrix staining with time was ob-served in ultrasound-treated defects comparedwith controls.
In the current rabbit model, 12 weeks of ul-trasound treatment seemed to be adequate tosee the sustained benefit of daily therapy.When evaluated at 24 weeks, there was no sig-nificant improvement in the quality of defecthealing when ultrasound was applied beyondthe first 12 weeks postoperative, with 18 and24 weeks of therapy having equivalent meangross and histologic grades compared with 12weeks of treatment. Similarly, there was nosignificant increase in mean gross and histo-logic grades when defects were evaluated at
Number 391SOctober, 2001 Ultrasound Improves Cartilage Repair S241

52 weeks after receiving 52 weeks of ultra-sound therapy compared with those treatedwith just 24 weeks of therapy. With time, therewas no significant change in the ultrasoundgroup results from 24 to 52 weeks, indicatingthat perhaps the crucial effects of ultrasoundoccur before 24 weeks of healing. The effectof the number of ultrasound treatments re-quired to see a sustained benefit in this animalmodel also seems to depend on the applicationof therapy within the first 12 weeks of healing.
Part II of the study was a first attempt at op-timizing the daily ultrasound treatment time todetermine whether shorter (or longer) therapytime is required to observe the benefits of thetreatment. Decreasing the number of treatmentsand the length of each treatment is desirable indeveloping a clinical ultrasound therapy regimethat ensures patient compliance. Increasing thetreatment time from the standard 20 minutes to40 minutes resulted in a statistically significanthistologic improvement. Overall, there was atrend toward improved cartilage repair with in-creasing daily ultrasound treatment time (Fig6). These findings are in agreement with obser-vations in models of bone healing after treat-
ment with ultrasound. In a rabbit fibular os-teotomy model, Tsai et al31 compared the rateof bone formation after treatment with dailylow intensity ultrasound for either 5, 15, or 25minutes. They reported that at 4 weeks aftersurgery the amount of bone formed increasedsignificantly with the length of the ultrasoundtreatment, where 25 minutes of therapy gener-ated the most bone formation. The results of thecurrent study indicate that the effects of treat-ment with low-intensity pulsed ultrasound maybe dose dependent. In this experimental model,optimal histologic results were observed with a40-minute daily treatment. The results also in-dicated a minimum 12-week duration. Thiswould be a reasonable treatment protocol; how-ever, trials in humans will best determine theoptimum therapy balancing issues of patientcompliance and clinical outcomes.
The exact biologic mechanism is not yetfully understood, although it generally is ac-cepted that low-intensity pulsed ultrasound in-fluences the cartilage formation and matura-tion phases of fracture healing.23,34 The currentstudy has shown that ultrasound therapy canpositively influence the healing of articulardefects, particularly those involving the sub-chondral bone, and may prove to be an adjunctto procedures such as mosaicplasty and sub-chondral drilling. Ultrasound may impart ac-celerated and improved quality of the repair,slowing the possible degenerative process as-sociated with these defects. These improve-ments may lead to a faster postoperative re-covery period and greater functional scores inintermediate and long-term followup.
References1. Aaron RK, Ciombor DM: Therapeutic effects of
electromagnetic fields in the stimulation of connec-tive tissue repair. J Cell Biochem 52:42–46, 1993.
2. Blevins FT, Steadman JR, Rodrigo JJ, et al: Treat-ment of articular cartilage defects in athletes: Ananalysis of functional outcome and lesion appear-ance. Orthopedics 21:761–768, 1998.
3. Bobic V: Arthroscopic osteochondral autograft trans-plantation in anterior cruciate ligament reconstruc-tion: A preliminary clinical study. Knee Surg SportsTraumatol Arthrosc 3:262–264, 1996.
4. Brighton CT, Unger AS, Stambough JL: In vitrogrowth of bovine articular cartilage chondrocytes in
Clinical OrthopaedicsS242 Cook et al and Related Research
Fig 6. Graphic summary of the mean histologicgrades comparing 0, 5, 10, 20, and 40 minutes ofultrasound treatment at 4 weeks postoperative. Atrend in increasing mean grade was observed withincreasing ultrasound therapy treatment time.

various capacitively coupled electrical fields. J Or-thop Res 2:15–22, 1984.
5. Brittberg M, Lindahl A, Nilsson A, et al: Treatment ofdeep cartilage defects in the knee with autologous chon-drocyte transplantation. N Engl J Med 331:889–895,1994.
6. Brittberg M, Nilsson A, Lindahl A, et al: Rabbit ar-ticular cartilage defects treated with autologous cul-tured chondrocytes. Clin Orthop 326:270–283, 1996.
7. Caplan AI, Elyaderani M, Mochizuki Y, et al: Prin-ciples of cartilage repair and regeneration. Clin Or-thop 342:254–269, 1997.
8. Chen FS, Frenkel SR, DiCesare PE: Chondrocytetransplantation and experimental treatment options forarticular cartilage defects. Am J Orthop 26:396–406,1997.
9. Cook SD, Rueger DC: Osteogenic protein-1: Biol-ogy and applications. Clin Orthop 324:29–38, 1996.
10. Cook SD, Ryaby JP, McCabe J, et al: Accelerationof tibia and distal radius fractures healing in patientswho smoke. Clin Orthop 337:198–207, 1997.
11. Duarte LR: The stimulation of bone growth by ultra-sound. Arch Orthop Trauma Surg 101:153–159,1983.
12. Dyson M, Brookes M: Stimulation of bone repair byultrasound. Ultrasound Med Biol 2 (Suppl):61–66,1983.
13. Grgic M, Jelic M, Basic V, et al: Regeneration ofarticular cartilage defects in rabbits by osteogenicprotein-1 (bone morphogenetic protein-7). Acta MedCroatica 51:23–27, 1997.
14. Hangody L, Kish G, Karpati Z, et al: Mosaicplasty xfor the treatment of articular cartilage defects: Appli-cation in clinical practice. Orthopedics 21:751–756,1998.
15. Heckman JD, Ryaby JP, McCabe J, et al: Accelera-tion of tibial fracture-healing by non-invasive, low-intensity pulsed ultrasound. J Bone Joint Surg76A:26–34, 1994.
16. Kristiansen TK, Ryaby JP, McCabe J, et al: Acceler-ated healing of distal radial fractures with the use of spe-cific, low-intensity ultrasound. A multicenter, prospec-tive, randomized, double-blind, placebo-controlledstudy. J Bone Joint Surg 79A:961–973, 1997.
17. Lippiello L, Chakkalakal D, Connolly JF: Pulsing di-rect current-induced repair of articular cartilage in rab-bit osteochondral defects. J Orthop Res 8:266–275,1990.
18. Mankin HJ, Mow VA, Buckwalter JA, et al: Form andFunction of Articular Cartilage. In Simon SR (ed). Or-thopaedic Basic Science. Rosemont, IL, AmericanAcademy of Orthopaedic Surgeons 1–44, 1994.
19. Mitchell N, Sheppard N: The resurfacing of adultrabbit articular cartilage by multiple perforationsthrough the subchondral bone. J Bone Joint Surg58A:230–233, 1976.
20. Moran ME, Kim HK, Salter RB: Biological resur-facing of full-thickness defects in patellar articularcartilage of the rabbit: Investigation of autogenous
periosteal grafts subjected to continuous passive mo-tion. J Bone Joint Surg 74B:659–667, 1992.
21. Nehrer S, Spector M, Minas T: Histologic analysis oftissue after failed cartilage repair procedures. ClinOrthop 365:149–162, 1999.
22. Outerbridge HK, Outerbridge AR, Outerbridge RE:The use of a lateral patellar autologous graft for therepair of a large osteochondral defect in the knee. J Bone Joint Surg 77A:65–72, 1995.
23. Parvizi J, Wu CC, Lewallen DG, et al: Low-intensityultrasound stimulates proteoglycan synthesis in ratchondrocytes by increasing aggrecan gene expres-sion. J Orthop Res 17:488–494, 1999.
24. Pilla AA, Mont MA, Nasser PR, et al: Non-invasivelow-intensity pulsed ultrasound accelerates bonehealing in the rabbit. J Orthop Trauma 4:246–253,1990.
25. Ryaby JT, Bachner EJ, Bendo JA, et al: Low inten-sity pulsed ultrasound increases calcium incorpora-tion in both differentiating cartilage and bone cellcultures. Trans Orthop Res Soc 14: 15, 1989.
26. Ryaby JT, Duarte-Alves P, Pilla AA: Ultrasound andstatic mechanical force affect second messenger ac-tivity in bone cell cultures. Trans Orthop Res Soc15:131, 1990.
27. Ryaby JT, Matthew J, Duarte-Alves P: Low intensitypulsed ultrasound affects adenylate cyclase andtransforming growth factor-beta synthesis in os-teoblastic cells. Trans Orthop Res. Soc 17:590, 1992.
28. Ryaby JT, Matthew J, Pilla AA: Low IntensityPulsed Ultrasound Modulates Adenylate CyclaseActivity and Transforming Growth Factor-Beta Syn-thesis. In Brighton CT, Pollock SR (eds). Electro-magnetics in Biology and Medicine. San Francisco,San Francisco Press 95–100, 1991.
29. Sellers RS, Peluso D, Morris EA: The effect of re-combinant human bone morphogenetic protein - 2(rhBMP-2) on the healing of full-thickness defects ofarticular cartilage. J Bone Joint Surg 79A:1452–1463,1997.
30. Sellers RS, Zhang R, Glasson SS, et al: Repair of ar-ticular cartilage defects one year after treatment withrecombinant human bone morphogenetic protein-2(rhBMP-2). J Bone Joint Surg 82A: 151–160, 2000.
31. Tsai CL, Chang WH, Liu TK: Preliminary studies ofduration and intensity of ultrasonic treatments onfracture repair. Chin J Physiol 35:21–26, 1992.
32. Wang SJ, Lewallen DG, Bolander ME, et al: Low in-tensity ultrasound treatment increases strength in arat femoral fracture model. J Orthop Res 12:40–47,1994.
33. Wolff J: The Law of Bone Remodeling (Das Gesetzder Transformation der Knochen). English transla-tion by Maquet P, Furlong R. Berlin, Springer Ver-lag 1982.
34. Yang KH, Parvizi J, Wang SJ, et al: Exposure to low-intensity ultrasound increases aggrecan gene expres-sion in a rat femur fracture model. J Orthop Res14:802–809, 1996.
Number 391SOctober, 2001 Ultrasound Improves Cartilage Repair S243