Embed Size (px)
Citation preview

Improved outcome of allogeneic haemopoietic stem celltransplantation for children with philadelphia positive acutelymphoblastic leukaemia
Although the prognosis for children and young adults with
acute lymphoblastic leukaemia (ALL) is excellent after modern
intensive treatment, there are several small subgroups who
have a high risk of relapse with conventional chemotherapy
and are candidates for allogeneic haemopoietic stem cell
transplant (allo-HSCT) in first complete remission. One such
group is Philadelphia positive (Ph+ve) ALL, which has a poor
prognosis in both children and adults. It forms <5% of ALL
cases in children but the frequency increases with age to 20–
30% in adults. Although conventional chemotherapy can
induce remission in >90% of cases, the risk of relapse is
exceptionally high if the remission is not consolidated by an
allo-HSCT (Arico et al, 2000). Therefore, first complete
remission (CR1) allo-HSCT is currently recommended as
definitive treatment for all children with Ph+ ALL by the major
childhood ALL study groups.
Recently, however, a US Children’s Oncology Group trial
obtained an excellent early outcome, comparable to that after
allo-HSCT, following treatment with a combination of the
tyrosine kinase inhibitor (TKI), imatinib, and conventional
chemotherapy(Schultz et al, 2009). It is therefore likely that
CR1 allo-HSCT will in future be restricted to sub-groups who
show evidence of resistance to chemotherapy and TKIs.
Essential to identifying a sub-group in whom the benefit of
allo-HSCT might outweigh its risks is availability of data on
current outcomes after allo-HSCT using a related or alternative
donor. We report our experience of transplanting an unse-
lected group of consecutive patients with Ph+ acute leukaemia
diagnosed at our centre over a 12-year period with a minimum
of 12 months follow-up post-transplant.
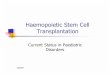
Twelve patients with Ph +ve acute leukaemia (six boys and
six girls) were diagnosed and transplanted at our centre
between May 1998 and April 2010. Individual patient charac-
teristics are described in Table I. Ten patients had ALL, one
had acute myeloid leukaemia (AML) and one mixed pheno-
type acute leukaemia. Nine patients were in CR1 and three
were in CR2. Median age at diagnosis was 10 years (2Æ9–
13Æ4 years) and median white blood cell count at presentation
was 27Æ2 · 109/l (5Æ0–394Æ4). The median interval between
diagnosis and CR1 was 28 d (range 28–75 d). All the patients
received first-line treatment on the then current UK national
trial protocol. In addition, seven patients received imatinib
(six) or dasatinib (one) pre-transplant.
Of the three children who received transplant in CR2, two
did not receive a CR1 transplant because of lack of a suitable
donor and, in the remaining patient, the Ph-status was
determined only at relapse because the diagnostic karyotype
and fluorescent in situ hybridization failed. The relapses
occurred at 32, 38 and 48 months from diagnosis. All three
achieved CR2 after reinduction. One received chemotherapy,
one single agent imatinib and one a combination of both.
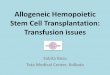
Table II shows individual patient details for the transplant
procedure and outcomes. The median interval between
remission and transplant was 6 months (range 1Æ7–
54 months). Three children received transplant from matched
related donors and nine from unrelated donors. No patient
died of regimen-related toxicity. Eleven children developed
steroid-responsive acute graft-versus-host disease (GVHD)
and one had limited chronic GVHD. Two patients experienced
a relapse post transplant. Patient 5 had an isolated pelvic
relapse 21 months after a matched related donor transplant
and is in a molecular remission 50 months following a second
transplant from a matched unrelated cord blood donor. She
received imatinib before and for 1 year after the second
transplant. Patient 3 relapsed 44 months after matched
unrelated donor transplant and subsequently received donor
lymphocyte infusion (DLI) and imatinib. He remains in CR3
more than 3 years from second relapse on maintenance
imatinib. All 12 patients are in CR at a median follow up of
3.6 years post-transplant (1Æ2–9 years).
As reported recently by St Jude’s, outcomes of transplant for
children with high risk leukaemia have improved significantly in
the last decade (Leung et al, 2011). We have witnessed a similar
improvement in outcome at our relatively small paediatric
transplant centre as a result of a decrease in transplant-related
mortality (TRM) to 0% after related donor and <10% after
alternative donor transplants (Sorour et al, 2009). For Ph+ ALL,
the results reported here are substantially better than that
reported in a similar number of patients who received an
unrelated donor transplant at a UK centre over a decade ago
(Marks et al, 1998). The improvement in outcome may partly be
a result of all our patients receiving TKIs at some stage, although
the influence of TKIs on transplant outcomes has been
inconsistent (Kebriaei et al, 2011; Rives et al, 2011). With
treatment-related mortality comparable to that associated with
intensive chemotherapy (Arico et al, 2000), CR1 transplant,
therefore, remains a legitimate option for sub-groups of Ph+
ALL who have a high risk of relapse due to resistance or
intolerance to chemotherapy and TKIs. If so, should the
eligibility for alternative donor transplant be restricted to a
Correspondence
ª 2011 Blackwell Publishing Ltd 261British Journal of Haematology, 2012, 157, 249–277

cohort with a higher risk of relapse than would be eligible for a
related donor transplant? Our experience would suggest
otherwise, given that the nine patients in our cohort who
received an unrelated donor transplant remain alive and in CR,
one after DLI and imatinib for post-transplant relapse.
Furthermore, 70% of eligible patients lack a related donor and
Table II. Transplant details and outcome.
Patient
Remission
status BMT Conditioning
Interval between
CR & BMT (months) GVHD
Follow-up from
BMT (years)
Current
status
1 CR2 MUD Cy/TBI/Cam 48 Grade I skin/gut 9 CCR2
2 CR1 MUD Cy/TBI/Cam 9 Grade I skin 8Æ10 CCR1
3 CR2 MUD Cy/TBI/ATG 54 Grade I skin 7Æ4 CCR3
4 CR1 MUD Cy/TBI/ATG 5Æ5 Grade III skin 6Æ4 CCR1
5 CR2 MRD Cy/TBI/ATG 40 Grade II skin/gut 5Æ11 CCR3
6 CR1 MUD Cy/TBI/Cam 6 Grade I skin 3Æ7 CCR1
7 CR1 MUD Cy/TBI/ATG 4 Grade II skin 3Æ6 CCR1
8 CR1 MUD Cy/TBI/ATG 4 Grade I skin 2Æ8 CCR1
9 CR1 MRD Cy/TBI 1Æ7 Grade I skin 2Æ8 CCR1
10 CR1 MUD Cy/TBI/Cam 4 Chronic GVHD 1Æ6 CCR1
11 CR1 MRD Cy/TBI 4 No GVHD 1Æ3 CCR1
12 CR1 MUD Cy/TBI 6 Grade II skin/gut 1Æ2 CCR1
BMT, bone marrow transplant; CR, complete remission; GVHD, graft-versus-host disease CCR, continuing complete remission; MUD, matched
unrelated donor; MRD, matched related donor; Cy, cyclophosphamide; TBI, total body irradiation: Cam, Campath; ATG, anti-thymocyte globulin.
Table I. Patient Characteristics and treatment at diagnosis.
Patient
Age
(years)/sex Diagnosis
WBC at
Dx (109/l) Cytogenetics Treatment received
Interval Dx to
remission (days)
1 15/M ALL 6Æ34 46, XY, t(9;22)(q34;q11) UKALL 97 High risk protocol 34
2 17/F ALL 32Æ6 46, XX, t(9;22)(q34;q11) FRALLE 93 protocol 35
3 22/M ALL 8Æ4 47XY dup(1)(q23;q23) MRC ALL HR1 protocol 28
4 19/M ALL 6Æ5 46, XY, t(9;22)(q34;q11) UKALL 2003/EsPHALL at day 28 28
5 16/F ALL 7Æ9 46, XX, t(9;22)(q34;q11) ALL 97/99 28
6 7/M ALL 5Æ0 46, XY, t(9;22)(q34;q11) ADE · 2 – resistant, UKALL2003
Reg B
35
7 16/M MPAL 63Æ0 46, XY, t(9;22)(q34;q11) UKALL 2003 reg B/EsPhALL
cons. imatinib
28
8 9/F ALL 85Æ3 46, XX, t(9;22)(q34;q11) UKALL2003 reg B. BFM cons.
imatinib
28
9 15/F ALL 394Æ4 46, XX, t(9;22)(q34;q11) MRC AML 15 protocol,
FLAG-dasatinib
75
10 13/F AML 21Æ9 46, XX, t(9;22)(q34;q11) [1]/
48,idem,add(9)(p1),+add(9)
(p1),+der(22)t(9;22)(q34;q11)
[16]/46,XX[3]
UKALL 2003 reg B. imatinib 28
11 11/M ALL 225 46, XY, t(2;4)(p11q1),add(6)(q2),
t(9;22)(q34;q11.2),)15,
+mar[17]/46,XY[3]
UKALL 2003 reg B EsPhALL
cons. imatinib
28
12 15/F ALL 29Æ6 46, XX [20].nuc ish(ABL1x3,BCRx2)
(ALB1 con BCR x1)(78/143)
UKALL2003 EsPhALL cons.
imatinib
28
WBC, white blood cell count; Dx, diagnosis; ALL, acute lymphoblastic leukaemia; MPAL, mixed phenotypic acute leukaemia; AML, acute myeloid
leukaemia; FLAG, fludarabine, cytarabine; ADE, cytarabine, daunorubicin, etoposide; Reg, regimen; EsPhALL cons., European intergroup study on
post-induction treatment of Ph+ ALL consolidation; FRALLE, French-paediatric protocol; UKALL, UK National trial protocol for ALL; MRC,
Medical Research Council; BFM cons., Berlin-Frankfurt-Munster consolidation.
Correspondence
262 ª 2011 Blackwell Publishing LtdBritish Journal of Haematology, 2012, 157, 249–277

there is tentative evidence for a more potent graft-versus-leukaemia
effect from unrelated donor transplants (Cornelissen et al, 2001)
resulting in a comparable outcome despite a higher TRM.
TRM is not the sole consideration when comparing
the merits of transplant versus chemotherapy for high-risk
paediatric leukaemia and the late side effects of total body
irradiation (TBI) remain a major disadvantage of transplant
over chemotherapy. Most chemotherapy protocols recom-
mend cranial radiotherapy as standard central nervous system-
directed treatment for all patients with Ph+ ALL not eligible
for transplant (Schultz et al, 2009), but the burden of late side
effects is considerably higher following TBI than cranial
radiotherapy. However, just as the availability of TKIs might
allow cranial radiotherapy to be omitted from future chemo-
therapy protocols for Ph+ ALL, their use before and after
transplant might permit the development of novel reduced-
intensity conditioning regimens that do not contain TBI (Ram
et al, 2011).
Acknowledgements
AV designed the study, analysed the data and wrote the paper.
AG, AS and JW analysed the data. All authors contributed to
care of the patients included in this study and helped write the
paper.
Anshu Garg
Adhithya Sankar
Janet Williams
Emma Astwood
Jeanette Payne
Jenny Welch
Shan Rush
Julie Marples
Sharon Barrott
Ajay Vora
Department of Haematology, Sheffield Children’s Hospital, Sheffield, UK.
E-mail: [email protected]
Keywords: acute lymphoblastic leukaemia (ALL), Philadelphia
positive acute leukaemia, children.
First published online 25 November 2011
doi: 10.1111/j.1365-2141.2011.08953.x
References
Arico, M., Valsecchi, M.G., Camitta, B., Schrappe,
M., Chessells, J., Baruchel, A., Gaynon, P., Silv-
erman, L., Janka-Schaub, G., Kamps, W., Pui,
C.H. & Masera, G. (2000) Outcome of treatment
in children with Philadelphia chromosome-po-
sitive acute lymphoblastic leukemia. The New
England journal of medicine, 342, 998–1006.
Cornelissen, J.J., Carston, M., Kollman, C., King, R.,
Dekker, A.W., Lowenberg, B. & Anasetti, C.
(2001) Unrelated marrow transplantation for
adult patients with poor-risk acute lymphoblastic
leukemia: strong graft-versus-leukemia effect and
risk factors determining outcome. Blood, 97,
1572–1577.
Kebriaei, P., Saliba, R., Rondon, G., Chiattone, A.,
Luthra, R., Anderlini, P., Andersson, B., Shpall,
E., Popat, U., Jones, R., Worth, L., Ravandi, F.,
Thomas, D., O’Brien, S., Kantarjian, H., de Lima,
M., Giralt, S. & Champlin, R. (2011) Long-term
follow-up of allogeneic hematopoietic stem cell
transplantation for patients with Philadelphia
chromosome-positive acute lymphoblastic leu-
kemia: impact of tyrosine kinase inhibitors on
treatment outcomes. Biology of Blood and Marrow
Transplantation, doi:10.1016/j.bbmt.2011.08.011.
[Epub ahead of print]
Leung, W., Campana, D., Yang, J., Pei, D., Coustan-
Smith, E., Gan, K., Rubnitz, J.E., Sandlund, J.T.,
Ribeiro, R.C., Srinivasan, A., Hartford, C., Trip-
lett, B.M., Dallas, M., Pillai, A., Handgretinger,
R., Laver, J.H. & Pui, C.H. (2011) High success
rate of hematopoietic cell transplantation
regardless of donor source in children with very
high-risk leukemia. Blood, 118, 223–230.
Marks, D.I., Bird, J.M., Cornish, J.M., Goulden, N.J.,
Jones, C.G., Knechtli, C.J., Pamphilon, D.H.,
Steward, C.G. & Oakhill, A. (1998) Unrelated
donor bone marrow transplantation for children
and adolescents with Philadelphia-positive acute
lymphoblastic leukemia. Journal of Clinical
Oncology, 16, 931–936.
Ram, R., Storb, R., Sandmaier, B.M., Maloney, D.G.,
Woolfrey, A., Flowers, M.E., Maris, M.B., Laport,
G.G., Chauncey, T.R., Lange, T., Langston, A.A.,
Storer, B. & Georges, G.E. (2011) Non-my-
eloablative conditioning with allogeneic hema-
topoietic cell transplantation for the treatment of
high-risk acute lymphoblastic leukemia. Haema-
tologica, 96, 1113–1120.
Rives, S., Estella, J., Gomez, P., Lopez-Duarte, M., de
Miguel, P.G., Verdeguer, A., Moreno, M.J.,
Vivanco, J.L., Couselo, J.M., Fernandez-Delgado,
R., Maldonado, M., Tasso, M., Lopez-Ibor, B.,
Lendinez, F., Lopez-Almaraz, R., Uriz, J., Melo,
M., Fernandez-Teijeiro, A., Rodriguez, I. &
Badell, I. (2011) Intermediate dose of imatinib in
combination with chemotherapy followed by
allogeneic stem cell transplantation improves
early outcome in paediatric Philadelphia
chromosome-positive acute lymphoblastic leu-
kaemia (ALL): results of the Spanish Cooperative
Group SHOP studies ALL-94, ALL-99 and ALL-
2005. British Journal of Haematology, 154, 600–
611.
Schultz, K.R., Bowman, W.P., Aledo, A., Slayton,
W.B., Sather, H., Devidas, M., Wang, C., Davies,
S.M., Gaynon, P.S., Trigg, M., Rutledge, R.,
Burden, L., Jorstad, D., Carroll, A., Heerema,
N.A., Winick, N., Borowitz, M.J., Hunger, S.P.,
Carroll, W.L. & Camitta, B. (2009) Improved
early event-free survival with imatinib in Phila-
delphia chromosome-positive acute lympho-
blastic leukemia: a children’s oncology group
study. Journal of Clinical Oncology, 27, 5175–
5181.
Sorour, Y., Williams, J., Rush, S., Barrott, S. & Vora,
A. (2009) Improved outcomes of paediatric
allogeneic haemopoietic stem cell transplantation
following implementation of standardised trans-
plant procedures in preparation for JACIE
accreditation (Abstract). Bone Marrow Trans-
plantation, 43, S229.
Correspondence
ª 2011 Blackwell Publishing Ltd 263British Journal of Haematology, 2012, 157, 249–277