Embed Size (px)
Citation preview

https://www.ResourcesForIntegratedCare.com
Improving Accessibility in Provider Settings
Credit Information§ If you would like to receive continuing education or continuing medical education
credit for today’s event via the Centers for Medicare & Medicaid Service’s Learning Management System, please visit this link for more information:https://resourcesforintegratedcare.com/sites/default/files/CE_Guide.pdf
Audio and Platform Information§ The audio portion of the presentation will automatically stream through your
computer speakers. If you experience challenges with the audio, please click the phone icon at the bottom of the screen for dial-in information.
§ If you are experiencing any technical difficulties with this platform, please use the Q&A feature for assistance or click the help button for additional information.
1

https://www.ResourcesForIntegratedCare.com
February 21, 2018
The 2018 Disability-Competent Care Webinar Series:
Improving Accessibility in Provider Settings

https://www.ResourcesForIntegratedCare.com
Webinar Overview
§ The Lewin Group, under contract with the CMS Medicare-Medicaid Coordination Office, partnered with Christopher Duff and other disability practice experts to develop the 2018 Disability-Competent Care webinar series. This is the first webinar in the series.
§ This webinar series builds on the 2017 Disability-Competent Care webinar series, that introduced the model of care and its seven foundational pillars. To view this series, please visit: https://www.resourcesforintegratedcare.com/DisabilityCompetentCare/2017_DCC_Webinar_Series/Series_Overview
§ Each session will be interactive (e.g., polls and interactive chat functions), with 45 minutes of presenter-led discussion, followed by 15 minutes of presenter and participant discussions.
§ Video replay and slide presentation are available after each session at:https://www.resourcesforintegratedcare.com
3

https://www.ResourcesForIntegratedCare.com
Continuing Education Accreditation
§ The Centers for Medicare & Medicaid Services is accredited by the International Association for Continuing Education and Training (IACET) for Continuing Education Units (CEU) and by the Accreditation Council for Continuing Medical Education (ACCME) for Continuing Medical Education (CME, AMA PRA Category 1 credit for physicians and non-physicians).
4

https://www.ResourcesForIntegratedCare.com
Obtaining Continuing Education Credit
§ Complete the post-test through CMS’ Learning Management System and score a 80 percent or higher by midnight March 12, 2018.
§ https://resourcesforintegratedcare.com/sites/default/files/CE_Guide.pdf
5

https://www.ResourcesForIntegratedCare.com
Support Statement
§ This webinar is supported through the Medicare-Medicaid Coordination Office (MMCO) in the Centers for Medicare & Medicaid Services (CMS) to help beneficiaries dually eligible for Medicare and Medicaid have access to seamless, high-quality health care that includes the full range of covered services in both programs. To support providers in their efforts to deliver more integrated, coordinated care to dually eligible beneficiaries, MMCO is developing technical assistance and actionable tools based on successful innovations and care models, such as this webinar.
§ To learn more about current efforts and resources, visit Resources for Integrated Care at: https://www.resourcesforintegratedcare.com
6

https://www.ResourcesForIntegratedCare.com
Introductions
Christopher Duff Disability Practice and Policy Consultant
Sonya BowenCMS Office of Minority Health
Patrick GoingADA Consultant
7

https://www.ResourcesForIntegratedCare.com
Introductions
Van WilsonColorado Department of Health Care Policy and Financing
Gabriel UribeInland Empire Health Plan
8

https://www.ResourcesForIntegratedCare.com
Webinar Learning Objectives
This webinar will emphasize:§ The multiple components of accessibility and how social
determinants of health and the physical and programmatic barriers experienced by persons with disabilities affect health outcomes
§ ADA and Section 504 laws applicable to health facilities§ Strategies to enhance provider accessibility, including:
§ Surveying primary care clinics for accessibility, and§ Providing accessibility information to participants and care
coordinators
9

https://www.ResourcesForIntegratedCare.com
Agenda
§ Understanding access
§ Federal laws, regulations, and guidelines
§ Strategies to support provider accessibility enhancements
§ Colorado Primary Care Site Accessibility Survey Tool
§ Addressing accessibility challenges
§ Inland Empire Health Plan Accessible Clinics Project
§ Audience questions
10

https://www.ResourcesForIntegratedCare.com
Understanding Access
11
Sonya BowenCMS Office of Minority Health

https://www.ResourcesForIntegratedCare.com
Barriers to Care
§ Adults with disabilities are almost twice as likely as other adults to report unmet health care needs due to problems with the accessibility of a doctor’s office or clinic.1
§ Many individuals with mobility limitations face difficulties locating services or otherwise traveling a burdensome distance to physically accessible services.2
§ A recent study of subspecialty practices in four U.S. cities found that 22 percent of practices reported being unable to accommodate a participant in a wheelchair.3
12
Source: 1) Karpan, Michael, and Long, Sharon K. (2015). Most Adults with Medical Debt had Health Insurance at the Time the Debt was Incurred. Urban Institute Health Policy Center.2) Krahn, et al. Persons with Disabilities as an Unrecognized Health Disparity Population. American Journal of Public Health. 2015;105(S2).3) Lagu et al. Access to Subspecialty Care for Patients with Mobility Impairment: A Survey. Ann Intern Med. 2013;158(6):441-446.

https://www.ResourcesForIntegratedCare.com
Health Disparities
Individuals with disabilities are more likely to:4,5
§ Experience worse health outcomes
§ Experience difficulties or delays in receiving necessary health care
§ Have limited knowledge and access to sexual health information
§ Have high blood pressure
Individuals with disabilities are less likely to:4,5
§ Receive comprehensive preventive care, including health screening tests
§ Receive recommended care (due to socioeconomic barriers and industry biases)
§ Have an annual dental visit
13
Sources: 4) Office of the Assistant Secretary for Planning and Evaluation. (2016). Report to Congress: Social Risk Factors and Performance under Medicare’s Value Based Purchasing Programs5) Disability and Health. Healthy People 2020. Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/disability-and-health/ebrs

https://www.ResourcesForIntegratedCare.com
Access – A Participant’s Perspective
§ Disability Rights Educations & Defense Fund (DREDF) health care stories video: Larry Voss
14

https://www.ResourcesForIntegratedCare.com
Understanding Access
Being a disability-competent care provider requires attention to access, in all of its forms. Improving access in a health care setting requires addressing barriers to care that may be experienced by the participant, including physical, social, and cultural barriers.
To improve access to care, it is necessary to consider: 1. Social determinants of health that may affect the participant2. Attitudes, processes, and systems in the care environment,
and barriers that these may present
15

https://www.ResourcesForIntegratedCare.com
Social Determinants of Health
§ Disability contributes to social determinants of health. Thus, disability can have a negative effect on:§ Attaining education§ Work, employment, and income§ Health insurance and medical expenses§ Social inclusion and community supports§ Access to transportation
§ As social inequities rise due to social determinants of health, morbidity and mortality rates increase.
16
Source: 6) Frier et al. Understanding disability and the 'social determinants of health': how does disability affect peoples' social determinants of health? Disabil Rehabil. 2018 Mar;40(5):538-547

https://www.ResourcesForIntegratedCare.com
Access – The Care Environment
The care environment includes any facet of the health care system that a participant may come in contact with when seeking care, such as the following: § Attitudinal§ Communication§ Care process § Programmatic (programs and services)§ Physical (facility and equipment)
These are all interlaced and together account for the barriers experienced by persons with disabilities in accessing care.
17

https://www.ResourcesForIntegratedCare.com
Access to Care – Considerations
18
§ Routes from parking or bus stops into the building
§ Parking§ Entry doors with the required
clearance width§ Restrooms § Signage for people who are
blind or have low vision
Facility Access
§ Scales and exam tables to facilitate a medical exam
§ Treatment and diagnostic equipment
§ Communication support for individuals with sensory or cognitive impairment
§ Staff trained to assess participant needs and safely help participants
Services Access

https://www.ResourcesForIntegratedCare.com
Payment Factors
§ Payers, including Medicare and Medicaid, are increasingly moving from traditional fee-for-service payment toward models that reward value over volume.
§ Disability status and health disparities are often associated with poorer performance on measures that are linked to payment in value-based purchasing programs.
§ On many measures of focus (e.g., cancer screenings, vaccinations, diabetes management), the clinical interventions are straightforward but communications and service delivery for people with disabilities may stretch the disability competence of providers.
§ Improving outcomes for people with disabilities may have a direct impact on revenue for providers and plans.
19
Source: 7) National Academies of Sciences, Engineering, and Medicine. (2017). Accounting for social risk factors in Medicare Payment, Washington, DC: The National Academies Press. doi: 10.1722

https://www.ResourcesForIntegratedCare.com
Federal Laws, Regulations, and Guidelines
20
Sonya BowenCMS Office of Minority Health

https://www.ResourcesForIntegratedCare.com
Federal Disability Rights Laws
§ Federal law prohibits discrimination on the basis of disability, including in health care services:§ Section 504 of the Rehabilitation Act of 1973 with 1992
amendments (Section 504) covers programs and activities receiving federal financial assistance
§ Americans with Disability Act (ADA) of 1990 covers medical care services and the facilities where services are provided§ Title II applies to public hospitals, clinics, and medical offices
operated by state and local governments as programs and activities of public entities.
§ Title III applies to private hospitals or medical offices as places of public accommodation.
§ Health care programs and services receiving federal, state, and local funds are subject to both laws
21

https://www.ResourcesForIntegratedCare.com
Accessibility of Health Care Facilities
§ According to the ADA and Section 504 requirements, individuals with disabilities must have:§ An equal opportunity to participate in and benefit from programs§ Meaningful access to programs and services
§ Health plans and providers must take steps to include:§ Reasonable modifications in policies, practices and procedures§ Effective communication § A designated employee to coordinate efforts to comply with Section
504 and ADA activities§ Grievance procedures to handle complaints of disability
discrimination in programs and activities § Medicare Managed Care rule requires states and plans to provide
auxiliary aids and services to assist enrollees and potential enrollees with disability in communicating with plans and providers.
22

https://www.ResourcesForIntegratedCare.com
Medicaid Data Collection and Reporting Guidelines
§ 2016 Medicaid managed care guidelines provide a framework for scaling up data collection efforts currently underway in a small number of states. The guidelines include a requirement that Medicaid managed care plans’ provider directories include information on the accessibility of network provider offices/facilities.
§ Information on the physical accessibility of health care facilities and services is limited. Currently, there is no national-level database.
§ Several states collect data to monitor provider accessibility, mostly through their Medicaid programs.
23

https://www.ResourcesForIntegratedCare.com
Strategies to Support Provider Accessibility Enhancements
24
Sonya BowenCMS Office of Minority Health

https://www.ResourcesForIntegratedCare.com
Strategies to Increase Accessibility
§ Training for providers and office staff. For example:§ Encourage provider settings to collect information on
participants’ functional limitations or accessibility needs when making appointments. Add this information to participants’ medical records, and verify the information at visits.
§ Reducing financial barriers for providers § Tax incentives to remove accessibility barriers§ 2018 Medicare physician fee schedule: new billing codes for
prolonger preventive services
25

https://www.ResourcesForIntegratedCare.com
Billing for Accessibility Options
The 2018 Medicare physician fee schedule offers new provider billing codes for prolonged preventive services:
§ Beginning January 1, 2018, practitioners can bill prolonged preventive services through Healthcare Common Procedure Coding System (HCPCS) G-codes (G0513 and G0514).
§ These codes can be billed with eligible Medicare-covered preventive services in 30 minute increments for services that extend beyond the typical time assumed for the services.
§ A list of preventive services that can be billed with the prolonged preventives codes is available on the Medicare Physician Fee Schedule (PFS) website: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/
26

https://www.ResourcesForIntegratedCare.com
Colorado Primary Care Site Accessibility Survey Tool
27
Patrick GoingADA Consultant

https://www.ResourcesForIntegratedCare.com
CO Primary Care Site Accessibility Survey Tool
§ CO Department of Health Care Policy and Financing (HCPF) aimed to create a tool to improve disability-competent care at primary care provider facilities across the state. Their goals included:§ Helping practices to identify areas of improvement for serving
participants with disabilities§ Providing assistance and resources to providers to increase
accessibility§ Informing participants of practices that provide disability-competent
care§ Three main sections of primary care access were identified as
focus points for the tool:1. Physical access2. Communication access3. Programmatic access
28

https://www.ResourcesForIntegratedCare.com
CO Primary Care Site Accessibility Survey Tool
§ CO HCPF partnered with local stakeholders to create this tool, including Independent Living Centers, regional care collaborative organizations (RCCOs), participants, and providers.
§ In addition to stakeholder input, the CO HCPF team compiled research and relied on existing accessibility tools: § The CMS Disability-Competent Care Self-Assessment Tool
(DCCAT)§ California Physical Accessibility Review Survey (PARS) § ADA Checklist for Readily Achievable Barrier Removal
29

https://www.ResourcesForIntegratedCare.com
Pilot Testing the Survey Tool
§ An Independent Living Center funded a one-time contract to administer the survey tool at ten provider clinics. These clinics represented 66 percent of the FFS dually eligible demonstration population in Colorado Springs.
§ Overall:§ Several practices made impactful changes at minimal cost,
such as changing pressure settings on power doors, ADA-compliant signage, and retro-fitting round doorknobs to lever hardware.
§ The survey tool was also provided to clinics in other parts of Colorado by RCCOs.
30

https://www.ResourcesForIntegratedCare.com
Accessibility Challenges Identified
§ Providers and front office staff often lack training to address the unique needs of people with complex medical, psycho-social and disability issues.
§ Participants with disabilities require additional time and resources. Challenges include:§ Transportation§ Availability of personal care attendants§ Non-accessible exam tables§ Need for sign language interpreters§ Extra time to complete exams and treatment
31

https://www.ResourcesForIntegratedCare.com
DCC Improvement Opportunity Template
Description Priority Est. Cost
Raise parking signs (two) to 60”* Immediate $50.00
Main entrance doors adjustment Immediate $0.00
Adjust closers on all doors within clinic Immediate $0.00
Purchase adjustable exam table* Immediate $5,000.00
Accessible scale for people who use wheelchairs* Soon $1,500.00
Create an accessible toilet stall in an unisex restroom in any future office expansion Future TBD
*Apply for tax write-offs
Total $6,550.00
32

https://www.ResourcesForIntegratedCare.com
Addressing Accessibility Challenges
33
Van WilsonColorado Department of Health Care Policy and Financing

https://www.ResourcesForIntegratedCare.com
Addressing Provider Accessibility Challenges
§ Assume positive intent – providers want to do the right thing.§ The ADA can require providers to implement significant
initiatives that carry real cost and resource implications.§ From the state’s perspective, successfully improving
accessibility includes the following considerations:§ The state has a very limited jurisdiction to enforce ADA
requirements§ Strategies must avoid ‘scaring providers away’§ It is important to focus on promoting engagement and
participation§ Actionable, concrete items for providers to improve their
accessibility is ideal
34

https://www.ResourcesForIntegratedCare.com
State Accessibility Challenges
§ Colorado Medicaid expects to maintain network adequacy for all members. The CO Primary Care Site Accessibility Survey Tool was voluntary for providers due to State concerns about the scope of authority.
§ Provider capacity to address opportunity areas identified by the tool remains limited.
§ Overall, engagement with providers has proven difficult:§ Fears of litigation related to potential ADA violations
§ Fear of the “ADA Police” inside their offices
§ Providers resented time/effort spent on an “unfunded mandate” for capital improvement costs
35

https://www.ResourcesForIntegratedCare.com
Lessons Learned in Improving Accessibility
§ A collaborative, non-threatening approach with providers is critical.
§ Providers are more receptive if they can see a business case for improvements and the connection to quality care.
§ Partnering with community organizations (e.g. a Center for Independent Living) is a critical success factor because of their credibility and expertise.
§ Engaging providers with low-cost, practical improvements first may open the door to larger assessment efforts.
§ Proper engagement with providers requires internal champions, time, and money.
36

https://www.ResourcesForIntegratedCare.com
Recent Success in CO
§ Three providers in Colorado Springs have recently committed to improving accessibility in their clinics by adding accessible equipment:§ One program for all-inclusive care for the elderly (PACE) in
Southern Colorado has ordered 10 high-low exam tables§ Two providers have committed to buying accessible exam
tables and Hoyer Lifts, used for lifting people from a wheelchair to an exam table
37

https://www.ResourcesForIntegratedCare.com
Next Steps: Expanding DCC in Colorado
§ HCPF continues to work with stakeholders to determine a more palatable strategy, including provider education and training.
§ HCPF developed a series of seven training videos and materials for providers based on the content of the tool. Topics include communication, programmatic, and physical access. Please visit:
https://www.colorado.gov/hcpf/disability-competent-care
38

https://www.ResourcesForIntegratedCare.com
Inland Empire Health Plan Accessible Clinics Project
39
Gabriel UribeInland Empire Health Plan

https://www.ResourcesForIntegratedCare.com
IEHP Accessible Clinics Project
§ To improve accessibility for participants with disabilities, Inland Empire Health Plan targeted clinics that lacked accessible diagnostic equipment.
§ In California, health plans serving dually eligible beneficiaries and Medicaid beneficiaries are required to assess the physical accessibility of provider sites as part of the California Physical Accessibility Review Survey (PARS). The information collected every three years is provided electronically to all health plans serving the area. One of the criteria evaluated and reported on is exam room equipment for diagnostic and treatment use.
40

https://www.ResourcesForIntegratedCare.com
IEHP Accessible Clinics Project
§ IEHP capitalized on the PARS data to identify clinics lacking accessible diagnostic equipment. The lack of equipment can result in common diagnostic procedures (such as Pap tests and mammograms) being skipped or overlooked for participants with disabilities.
§ The IEHP accessible clinics project:§ Funded accessible exam table/weight scale combos to network
primary care and specialty providers§ Required training in the use of the new equipment§ Offered tips on mitigating common barriers to care for
participants with disabilities§ Promoted IEHP’s disability resource and referral program
41

https://www.ResourcesForIntegratedCare.com
IEHP Accessible Clinics Project –Benefits to Clinics
§ Program grants do not require repayment. IEHP is investing in the community and in their provider network to improve the quality of care of IEHP members.
§ Practices can be marketed as an “accessible provider.” This allows clinics to target more participants with disabilities and activity limitations.
§ Changes support more effective treatment plans and better outcomes. Equipment to adequately examine participants improves early detection.
§ Participants can transfer themselves or be assisted in transfer, which empowers participants to take charge of their health care experience.
§ Program provides comprehensive training for all equipment which can help reduce workplace injuries.
42

https://www.ResourcesForIntegratedCare.com
Identifying Provider Sites – Provider Survey
To identify clinics best suited for this project, IEHP sent participation forms to all network providers to be completed, if the site was interested in participating. Survey topics included:§ Building accessibility at the practice§ Current medical equipment§ Training§ Accessible medical equipment needs§ Types of services provided
43

https://www.ResourcesForIntegratedCare.com
Identifying Provider Sites –Prioritization Criteria
The following criteria were used to prioritize provider sites:§ PARS data
§ Does the provider meet all critical elements?§ Do they currently have accessible equipment?§ Is the provider a primary care provider, ancillary, specialist, etc.?
§ Geography§ Is the applicant provider site within 10-25 miles of another site?§ What is the membership density at the site of the provider practice?
§ Specialty/network needs§ Specialist type§ Ancillary services
44

https://www.ResourcesForIntegratedCare.com
IEHP Training
§ Provider sites selected for the Accessible Clinics Project were asked to participate in a training partnership.
§ IEHP contracted with Western University Center for Disability & Health Policy. Together they developed:§ Training guides§ Training videos§ On-site provider training at award sites
§ Training elements included:§ Equipment use§ Safety§ Cultural competency§ Senior and disability community resource linkage§ Review of health plan accessibility and language access features
45

https://www.ResourcesForIntegratedCare.com
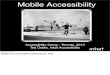
Accessible Clinics Project Results
§ Prior to the Accessible Clinics Project, participants often traveled >30 miles from town centers to find a provider with an accessible exam table.
§ Following the project, providers with accessible exam tables are available within 30 miles of most town centers (within the IEHP service area).
46
Number of Accessible Exam Tables
Provider Category Pre-Clinics Project Post-Clinics Project
All IEHP providers 19 (total)+65 Primary care sites
+35 Specialist care sites119 (total)
IEHP providers in regions with high need* 8 >50
*At least 1,500 members who are dually eligible beneficiaries, seniors, or who have disabilities (combined).

https://www.ResourcesForIntegratedCare.com
Accessible Clinics Project –Lessons Learned
The IEHP accessible clinics project:§ Provided accessible exam tables to five percent of IEHP’s
provider network.§ Trained 95 provider sites on barrier mitigation and disability
disparities in health care.Lessons learned:§ Providers are likely to participate in barrier mitigation when
incentivized.§ About 25 percent of awardees had minor barriers that needed
attention (barriers that were relatively easy to address).
47

https://www.ResourcesForIntegratedCare.com
Accessible Clinics Project – Next Steps
Health plan services:§ Health education§ Ensure physical access to all health plan programs§ Virtual program access
Online features:§ Accessible mobile apps§ Virtual primary care visits§ Multimedia content (how-to, education, marketing)
Continuous improvement:§ Responsiveness to evolving environment
48

https://www.ResourcesForIntegratedCare.com
Audience Questions
49

https://www.ResourcesForIntegratedCare.com
Next Webinar
Serving Adults with Disabilities on the Autism SpectrumDate: February 28th, 2018Time: 2:00pm-3:00pm ET
50

https://www.ResourcesForIntegratedCare.com
Thank You for Attending!
§ The video replay, slide presentation, and a summary of the Q&A will be available at:
https://www.resourcesforintegratedcare.com
§ For more information about obtaining CEUs or CMEs via CMS’ Learning Management System, please visit: https://resourcesforintegratedcare.com/sites/default/files/CE_Guide.pdf
§ Questions? Please email [email protected]
51

https://www.ResourcesForIntegratedCare.com
Webinar Evaluation Form
§ Your feedback is very important! Please take a moment to complete a brief evaluation on the quality of the webinar. The survey will automatically appear on the screen approximately a minute after the conclusion of the presentation.
52

https://www.ResourcesForIntegratedCare.com
Send Us Your Feedback
Help us diversify our series content and address current Disability-Competent Care training needs – your input is essential!
Please contact us with your suggestions [email protected]
What We’d Like from You:§ How best to target future Disability-Competent Care webinars to
health care providers and plans involved in all levels of the health care delivery process
§ Feedback on these topics as well as ideas for other topics to explore in webinars and additional resources related to Disability-Competent Care
53

https://www.ResourcesForIntegratedCare.com
Sources
1. Karpan, Michael, and Long, Sharon K. (2015). Most Adults with Medical Debt had Health Insurance at the Time the Debt was Incurred. Urban Institute Health Policy Center.§ http://hrms.urban.org/briefs/Most-Adults-with-Medical-Debt-Had-Health-Insurance-at-the-Time-the-Debt-Was-
Incurred.pdf2. Krahn, et al. Persons with Disabilities as an Unrecognized Health Disparity Population.
American Journal of Public Health. 2015;105(S2).§ http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2014.302182
3. Lagu et al. Access to Subspecialty Care for Patients with Mobility Impairment: A Survey. Ann Intern Med. 2013;158(6):441-446.§ http://annals.org/aim/article-abstract/1667265/access-subspecialty-care-patients-mobility-impairment-
survey?doi=10.7326%2f0003-4819-158-6-201303190-000034. Office of the Assistant Secretary for Planning and Evaluation. (2016). Report to Congress:
Social Risk Factors and Performance under Medicare’s Value Based Purchasing Programs§ https://aspe.hhs.gov/system/files/pdf/253971/ASPESESRTCfull.pdf
5. Disability and Health. Healthy People 2020. § https://www.healthypeople.gov/2020/topics-objectives/topic/disability-and-health/ebrs
6. Frier et al. Understanding disability and the 'social determinants of health': how does disability affect peoples' social determinants of health? Disabil Rehabil. 2018 Mar;40(5):538-547§ https://www.ncbi.nlm.nih.gov/pubmed/27927028
7. National Academies of Sciences, Engineering, and Medicine. (2017). Accounting for social risk factors in Medicare Payment, Washington, DC: The National Academies Press. doi: 10.1722
54

https://www.ResourcesForIntegratedCare.com
ADA Resources
§ For more information about the ADA, including downloadable resources:§ Visit www.ada.gov§ Call the Department of Justice’s ADA Information Line at 1-
800-514-0301 or 1-800-514-0383 (TTY)§ The ADA National Network provides information, guidance
and training on how to implement the ADA: https://adata.org/§ CMS Office of Minority Health developed an issue brief
which provides an overview of laws enacted to promote accessibility: https://www.cms.gov/About-CMS/Agency-Information/OMH/index.html
55

https://www.ResourcesForIntegratedCare.com
Additional Resources
1. Americans with Disabilities Act: Access to Medical Care for Individuals with Mobility Disabilities§ https://www.ada.gov/medcare_mobility_ta/medcare_ta.htm
2. The CMS Disability-Competent Care Self-Assessment Tool (DCCAT)§ https://www.resourcesforintegratedcare.com/physical_disability/dcc/tools/self
_assessment3. California Physical Accessibility Review Survey (PARS)
§ http://www.dhcs.ca.gov/formsandpubs/Documents/MMCDAPLsandPolicyLetters/PL2011/PL11-013.pdf
4. ADA Checklist for Readily Achievable Barrier Removal§ https://www.ada.gov/checkweb.htm
5. Colorado Department of Health Care Policy and Financing Disability-Competent Care videos§ https://www.colorado.gov/hcpf/disability-competent-care
56