Embed Size (px)
Citation preview

1
U.S. Department of Healthand Human Services
National Institutes of Health
Improving Care in ChronicKidney Disease
Andrew S. Narva, MD
CHCANYS Clinical Leadership Conference, May 2008
Improving Care in CKD
• Burden of CKD
• Application of chronic care model to CKDin Indian Health Service
• National Kidney Disease EducationProgram (NKDEP) and community healthcenter initiative
USRDS ADR, 2007
Prevalence of ESRD has been risingsteadily
Incident ESRD patients; rates adjusted for age & gender.
Incidence varies widely by race andethnicity
Rate
per
million
popu
lati
on
Af Am
N AmHispanic
Asian
White
Non-Hispanic
USRDS ADR, 2007
USRDS ADR, 2007
Diabetes and hypertension are leadingcauses of kidney failure
Incident ESRD rates, by primary diagnosis, adjusted for age, gender, & race.
Diabetes (DM) and hypertension(HTN) often coexist in CKD
USRDS ADR, 2006Distribution of CKD, HTN, & diabetic patients in Medicare population, 2004.
2
USRDS ADR, 2006
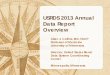
CKD is disproportionately costly
Distribution of costs for CKD, HTN, & diabetic patients in Medicare population, 2004.
26 million Americans have CKDor albuminuria
Coresh, et al., 2007
10.1
15.5
0.7
0
5
10
15
20
25
Persistent
albuminuria with
eGFR ! 60
eGFR of 30-59 eGFR of 15-29
Millions o
f people
CKD is prevalent in CVD
Ix, et al., 2003; Anavekar, et al., 2004; Shlipak, et al., 2004.
0
20
40
60
CADCrCl ≤60 mL/min
AMI GFR <60 mL/min
CHFGFR ≤60 mL/min
23%
46%
33%
Patie
nts
With
CK
D (%
)
In addition to ESRD, CKD leadsto CVD
Go, et al., 2004
2.1
21.8
36.6
11.3
3.7
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
! 60 45-59 30-44 15-29 < 15
Rat
e of
CV
D E
vent
s
eGFR
Age-Standardized Rate of CVD events per 100 person-year.
• Intensive glycemic control lessens progressionfrom microalbuminuria in Type 1 diabetes–goal inType 2 is less clear- DCCT, 1993
- ACCORD, 2008
• Antihypertensive therapy with ACE Inhibitors orARBs lessens proteinuria and progression- Giatras, et al., 1997- Jafar, et al., 2001
• Blood pressure below 130/80 is beneficial - Sarnak, et al., 2005
Effective therapy exists to slowprogression of CKD
Early treatment can make a difference
100
10
0
No Treatment
Current Treatment
Early Treatment
4 7 9 11
Time (years)
Kidney Failure
GFR
(m
L/m
in/1
.73
2)

3
CKD is still not being identified
• Estimated GFR reporting is not universal– 38.4% of all creatinine-reporting labs overall
• CKD is usually not coded as a diagnosis– Less than 40% of patients with eGFR <30
were coded
Stevens, et al., 2005; NKDEP, 2008
People with CKD are not aware of it –even those with eGFR less than 30
0
10
20
30
40
50
60
eGFR of 30-59 eGFR of 15-29
Perc
en
t R
ep
ort
Bein
g A
ware
of
Havin
g W
eak o
r Failin
g K
idn
eys
Men
Women
Coresh, et al., 2007
Adherence to treatment guidelines –room for improvement
0
10
20
30
40
50
60
70
80
95 96 97 98 99 00 01 02 03
The percentage of diabetic CKD patientsreceiving ACE-Is/ARBs has been slow to improve
Perc
en
t of
pati
en
ts
USRDS ADR, 2007
Challenges to improving CKD care
• CKD remains underdiagnosed– Inadequate screening of at-risk patients– Misinterpretation of test results
• Implementation of recommend care is poor– Underutilization of ACE inhibitors and ARBs– Poor achievement of BP goals– Many people poorly prepared for dialysis (poor nutritional status,
little understanding of dialysis choices)
• Many clinicians feel inadequately educated– Perception that CKD is a “specialist” disease– Uncertain about how to interpret diagnostic tests– Unclear about clinical recommendations– Low confidence in their ability to successfully manage CKD
Challenges to improving CKD careThe National Kidney DiseaseEducation Program
NKDEP aims to reduce the morbidity and mortalitycaused by kidney disease and its complications by:
• Improving early detection of chronic kidney disease
• Facilitating identification of patients at greatest risk forprogression to kidney failure
• Promoting evidence-based interventions to slowprogression of kidney disease
• Supporting the coordination of Federal responses tochronic kidney disease

4
The Chronic Care Model (CCM)
• Summarizes basic elements for improving care in healthsystems (community, organization, practice, patient levels)
• Originated from a synthesis of scientific literature done byMacColl Institute for Healthcare Innovation in early 1990s– Extensively reviewed by advisory panel of experts; compared with
features of leading U.S. chronic illness management programs– Refined and published in its current form in 1998
• Improving Chronic Illness Care, a national program of theRWJF, launched in 1998 with the CCM at its core– ICIC and Institute for Healthcare Improvement developed the
Chronic Care Breakthrough Series Collaboratives, which gave riseto HSRA’s Health Disparities Collaboratives
The Chronic Care Model
The Chronic Care Model
• Self-Management Support
• Goal: Empower and prepare patients to manage theirhealth care– How do we help patients live with their conditions?
• Change concepts– Emphasize the patient’s central role in managing his or her health
– Use effective self-management support strategies: assessment,goal-setting, action planning, problem-solving, and follow-up
– Organize internal and community resources to provide ongoingself-management support to patients
Model Elements
The Chronic Care Model
• Delivery System Design
• Goal: Assure the delivery of effective, efficient clinical careand self-management support– Who is on the healthcare team?– How does the team interact with patients?
• Change concepts– Define roles and distribute tasks among team members
– Use planned interactions to support evidence-based care
– Provide clinical case management services for complex patients
– Ensure regular follow-up by the care team
– Give care that patients understand and that agrees with theircultural background
Model Elements
The Chronic Care Model
• Decision Support
• Goal: Promote care consistent with scientific data andpatient preferences– What is the best care?– How do we make it happen every time?
• Change concepts– Embed evidence-based guidelines into daily clinical practice
– Share evidence-based guidelines and information with patients toencourage their participation
– Use proven provider education methods
– Integrate specialist expertise and primary care
Model Elements
The Chronic Care Model
• Clinical Information Systems
• Goal: Organize data to facilitate efficient and effective care– How do we capture and use critical information for clinical care?
• Change concepts– Provide timely reminders for providers and patients
– Identify relevant subpopulations for proactive care
– Facilitate individual patient care planning
– Share information with patients and providers to coordinate care
– Monitor performance of practice team and care system
Model Elements

5
What It Means for CKD
• The Chronic Care Model provides a much-needed paradigmfor how to improve CKD detection and management
• Offers a systematic way to identify needs and set priorities
• A convenient “shorthand” to use in communicating with avariety of audiences– Makes it clear which elements we need seeking to address– Aligning CKD initiatives with established CCM change concepts helps
us demonstrate their broader value
AI/AN and CKD
• American Indians: a “sentinel” population– Epidemic of diabetes– Epidemic of CKD and ESRD
• Indian Health: a model of a public healthorganization serving high risk populations
USR
DS
USRDS 2002 adr
Trends in incident rates, by race/ethnicity &primary diagnosis adjusted for age & gender
1991199519991991199519990
100
200
300
400
500
600
700
Diabetes
Hypertens ion
Glomerulonephritis
Cystic kidney
199119951999 199119951999199519971999
White Black Native AmericanAsian Hispanic
The IHS Experience
• A chronic-care approach to a high-risk population– Not the Chronic Care Model per se, but similar elements
• The community is the patient
• Integrated primary care system
• Multidisciplinary clinics
• Community outreach– Screening– Patient education
Indian Health Service
• Agency of US Public Health Service
• Mission: to improve health status of AI to highestpossible level
• Service population: 1.9 million
• Budget: $3.1 billion
• Capitated expenditure: $2158 vs. $5921 for UScivilian population
• Public health model
Special Diabetes Program for Indians
Diabetes Clinical Infrastructure
%
Source: IHS National Diabetes Program SDPI Evaluation, 1997-2005

6
IHS Kidney Disease Program
• Established 1989 to:– Promote prevention of CKD– Optimize care for people with CKD– Facilitate access to excellent ESRD care– Provide “in house” nephrologic expertise to IHS
and to tribes• Intent to enhance existing diabetes care to
provide better CKD care
IHS Kidney Disease Program
1. Screen for CKD as part of primary care: routineeGFR (2003), UACR (2006)
2. Broaden Diabetes Standards of Care
IHS Standards of Care for Diabetes and Kidney Disease: Goals
Identify, manage and monitor patients with diabetesand CKD (GFR<60 and/or proteinuria)
Initiate appropriate treatment for anemia ,malnutritionmetabolic bone disease, hyperlipidemia
Provide appropriate nutritional counseling for CKD
Provide patient education on IHS CKD educationalobjectives
Provide appropriate preparation for renalreplacement therapy including education on treatmentchoices, early referral for vascular access andtransplantation
IHS Kidney Disease Program
3. Implementation promoted through continuingeducation for all healthcare professionals
4. Promote case management• Workshop• Guidelines, protocols, patient ed materials,
treatment protocols online
IHS Kidney Disease Program
5. Modify medical information system• Implementation tools (eGFR)• Clinical documentation (PCC+)• Quality improvement
IHS Diabetes Care & Outcomes Audit
Testing for Kidney Disease 2007
Source: www.dmaudit.com/index.html

7
IHS Diabetes Care & Outcomes Audit
Hypertension Control 2007
Source: www.dmaudit.com/index.html
IHS Diabetes Care & Outcomes Audit
Testing for Kidney Disease 1996-2005
Source: IHS National DiabetesProgram Statistics 1996-2005
year
%
USRDS 2004 ADR
Prevalent counts & adjusted rates by raceESRD: Age-adjusted incidence,1990-2001 Network 15
6. Age-specific ESRD-DM incidence trends6. Age-specific ESRD-DM incidence trendsamong Native Americans with diabetesamong Native Americans with diabetes
20-44
45-64
65+
Incidence Trends
• Incidence peaked 1999• DM-ESRD peaked 1999• Age adjusted DM-ESRD incidence has decreased
20% since 1999• Between 1993 and 2001 ESRD incidence among
diabetics decreased 31%

8
Lessons Learned
• CKD is part of primary care• Changing patterns of care requires changing “the
system” (Chronic Care Model)• Improvement in care results from changes
implemented by physicians and non-physicianhealth professionals
• One size does not fit all due to differences inpatient populations and healthcare deliverysystems
More Lessons Learned
• Implemented through diabetes care deliverysystem ; Not specialty clinic based
• Surveillance and prevention are part ofmultisystem chronic disease control
• Professional education designed to enableexisting health care professionals to feelcomfortable with kidney patients and delivernecessary care
• Emphasis on ensuring that patient received carefrom competent and interested individual, notreferral
The Chronic Care Model
UACR/GFRpad fordiabeteseducators
Patient-edpad on GFR;
NKDEPwebsite
Providercontent on
NKDEPwebsite
Educating PCPsto help them
better manageCKD prior to
referral
Where NKDEP Activities Fit In
KICC:Better
coordinatedFederal
response
LaboratoryWorkingGroup
Raisingpublic
awareness
Promoting and supporting use of eGFR
Laboratory Community• Encouraging laboratory community to routinely report eGFR• Facilitating creatinine standardization to improve accuracy• Responding to inquiries from lab communityHealth Care Professionals/Primary Care Settings• Promoting use in CHCs• Facilitating eGFR patient education in primary care settings• Providing resources to diabetes educators and other professionals
to help them understand and explain results• Promoting eGFR at health professional meetings—NPs, diabetes
educators, nurses, community health centersAt Risk Patients• Encouraging at-risk patients to get their GFR (and urine protein)
checked routinely in all materials
• Straightforward, culturallyappropriate messages andmaterials
Educating people at risk
• Encourages families to talk about connection betweendiabetes, high blood pressure, and CKD
– Raise awareness among family members at risk
– Family Reunion Health Guide has information, approaches,and talking points
• Targeted outreach to reunion planners and familyinfluencers
– Organizational outreach
– Kidney Sundays
– Online promotion
Educating people at risk
African American Family Reunion Initiative

9
Health care professionals
• Primary care professionals can play a significantrole in early diagnosis, treatment, and patienteducation
• Therapeutic interventions for diabetic CKD aresimilar to those required for optimal diabetes care
• Control of glucose, blood pressure, andlipids
• A greater emphasis on detecting CKD, andmanaging it prior to referral, can improve patientoutcomes
CKD is Part of Primary Care
What can primary care providers do?
• Recognize and test at-risk patients :Monitor eGFRand UACR
• Screen for anemia (Hgb), malnutrition (albumin),metabolic bone disease (Ca, Phos, PTH)
• Treat cardiovascular risk, especially with smokersand hypercholesterolemia
• Refer to dietitian for nutritional guidance
• Educate patients about CKD and treatment
• Encourage labs to report estimated eGFR andurine albumin/creatinine ratios

10
Promoting and supporting patienteducation in primary care setting
• Developed 4 key concepts in patient education andsuggested talking points– Talk to patients about their kidneys, CKD, and their risk– Communicate the importance of testing and how CKD is diagnosed– Explain the progressive nature of CKD and the basis of treatment– Begin speaking to patients with CKD about dialysis and transplantation
• Developing tools to support education– GFR pad with key messages for patients and education concepts for
health care professionals (HCPs)– Patient education section for HCPs on NKDEP website
• Initial focus on promotion among diabetes educators
GFR Pad:Patient tear-off sheet(front)
GFR Pad:Patient tear-off sheet(back)
GFR Pad –Provider back side

11
Community Health Centers
• Focusing on opportunities to implement these types ofprograms in the community health centers
• Health centers are an ideal partner– Care for 16 million patients—many of whom are at risk for CKD– A track record of working to improve care in a systematic way
• Pilot project with 8 CHC’s to implement improved CKD carefor their diabetics
Performance Measures
Measures: Objective 1
Improve screening of at-risk patients (i.e., patients with DMand/or HTN)
Core Measures• % DM patients with estimated GFR in past year• % DM patients with urine albumin (UACR) measured in past
year• % DM patients with both GFR and UACR measured in past
year
Measures: Objective 2
Improve blood pressure control among patients with DM
Core Measures• % DM patients diagnosed with HTN or clinical proteinuria
(UACR >300 mg/g) on ACEI or ARB• % DM patients with BP controlled to <130/80
Measures: Objective 3
Improve screening of patients with DM and diagnosedCKD for complications
Core Measures• % DM patients with GFR <60 screened in past year for:
– anemia (Hgb)– malnutrition (albumin)– metabolic bone disease (Ca, PO4)– lipid disorders (Tchol, LDL, HDL, TG)
Measures: Objective 4
Improve education of patients with (or at increased riskfor) CKD
Core Measure• % patients with GFR <60 or UACR >30 mg/g with
documented education on CKD

12
NKDEP and Community Health Centers
• Improving the care of people with CKD requires changingclinical practice
• Providers change their practice based on scientific evidenceand the expectations of their patients
• CHCs are at the cutting edge of implementing excellentmanagement of chronic disease in high risk populations
• NKDEP will collaborate closely with CHCs to developeffective models for CKD intervention in the primaryhealthcare setting
Questions and comments