Embed Size (px)
Citation preview

Improving Depression Screening for AdolescentsWith Type 1 Diabetes
abstractOBJECTIVE: Depression is common among adolescents, but rates in-crease significantly in the presence of chronic health conditions. Out-patient screening for depression is recommended but rarely formallyconducted due to barriers of implementation.
METHODS: To provide a model for depression screening of youth withchronic health conditions, a standard process using a self-administered electronic version of the Children’s DepressionInventory (CDI) was developed. Quality improvement methodologyand traditional analytic approaches were used to test the feasibilityand outcomes of routine screening in patients 13 to 17 years of agewith type 1 diabetes.
RESULTS: Of the 528 eligible adolescents, 509 (96%) received at least 1depression screen during the first year. The process was tested andrefined in over 1200 patient encounters, which resulted in an increasein depression screening rates from ,5% to a median of 85% over theinitial 12 months. Both patients and staff reported acceptance ofscreening on qualitative surveys. Elevated CDI scores ($16) werefound in 8% of the sample; moderate scores (10–15) in 12% of thesample. Low risk scores were found in 80% of the sample. Higher CDIscores correlated with lower blood glucose monitoring frequency andhigher hemoglobin A1c, confirming the link between more depressionsymptoms and poorer diabetes management and control. Suicidalideation was endorsed in 7% of the population.
CONCLUSIONS: Systematic depression screening in adolescents withtype 1 diabetes can be reliably implemented with clinically significantresults. A systematic approach, such as described in this study, canserve as a model for other chronic health conditions. Pediatrics2013;132:e1395–e1402
AUTHORS: Sarah D. Corathers, MD,a Jessica Kichler, PhD,CDE,b Nana-Hawa Yayah Jones, MD,a Andrea Houchen,LISW-S,a Mary Jolly, RN, MBA,a Nancy Morwessel, CNP, CDE,a
Peggy Crawford, PhD,c Lawrence M. Dolan, MD,a and KoreyK. Hood, PhDd
aDivisions of Endocrinology, Cincinnati Children’s HospitalMedical Center and University of Cincinnati Medical Center,Cincinnati, Ohio; bBehavioral Medicine and Clinical Psychology,Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio;cDivision of Neurology, University of Cincinnati Medical Center,Cincinnati, Ohio; and dMadison Clinic for Pediatric Diabetes,University of California, San Francisco, San Francisco, California
KEY WORDSadolescent depression, chronic conditions, type 1 diabetes,quality improvement
ABBREVIATIONSBGM—blood glucose monitoringCDI—Children’s Depression InventoryEMR—electronic medical recordHbA1c—hemoglobin A1cQI—quality improvementPDSA—plan, do, study, act
Dr Corathers conceptualized and designed the study,coordinated and supervised data collection and analysis, anddrafted the initial manuscript, reviewed and revised themanuscript; Dr Kichler contributed to the design of the studyand reviewed and revised the manuscript; Dr Jonesconceptualized and designed the study, designed the datacollection instrument, and reviewed and revised the manuscript;Ms Houchen, Ms Morwessel, and Dr Crawford conceptualizedand designed the study and reviewed and revised themanuscript; Ms Jolly coordinated and supervised data collectionand reviewed and revised the manuscript; Dr Dolan participatedin the design of the study and critically reviewed themanuscript; Dr Hood conceptualized and designed the study,carried out the data analysis, and drafted the initial manuscript;and all authors approved the final manuscript as submitted.
(Continued on last page)
PEDIATRICS Volume 132, Number 5, November 2013 e1395
QUALITY REPORT
by guest on July 5, 2018www.aappublications.org/newsDownloaded from

One out of 5 adolescents in the UnitedStates has a chronic condition thatrequires ongoing treatment and man-agement.1 Advancements in technology,pharmacology, and delivery of multidis-ciplinary specialty care have improvedhealth outcomes, but medical treatmentregimens place significant demandsupon children and families. Type 1 di-abetes is an example of a commonchronic condition in children with a com-plex regimen.2 Management of type 1 di-abetes involves checking blood glucoselevels frequently and coordinating thoselevels with the amount and timing of in-sulin administration, dietary intake, andphysical activity. Effective management ofthese tasks often results in achievingtreatment targets for glycemic control asmeasuredby the hemoglobin A1c (HbA1c)value.3 The landmark Diabetes ControlandComplication Trial demonstrated thatachieving optimal glycemic control pre-vents ordelays the onset of complicationsto the kidneys, blood vessels, eyes, andcardiovascular system over time.4 How-ever, evenwith substantial improvementsin therapeutics and technologies, HbA1cvalues of adolescents in the DiabetesControl and Complication Trial remainedan average of 1% higher than adultcounterparts and globally, glycemic con-trol remains suboptimal for most ado-lescents with type 1 diabetes.5–7
Depression is a contributing factor tosuboptimal health outcomes and iscommon among adolescents. Up to 9.5%of the general population of adolescentsare depressed,8–10 and the rate is 2 to 3times higher for adolescents with type 1diabetes and other chronic health con-ditions.11–16 When present, depressionin adolescents with type 1 diabetes isassociated with less frequent bloodglucose monitoring (BGM),17 higherHbA1c values,18–21 and increased ratesof diabetes-related hospitalizations.22,23
All of these negative health outcomesare associated with higher risk of long-term complications from diabetes and
consequent increase in medical carecosts. Furthermore, depression does nottypically resolve without treatment. Thus,depression during adolescence increasesthe likelihood for depression as anadult.24,25
Given the impact of depression on ad-olescent outcomes (including health),the US Preventative Task Force recom-mended screening adolescents for de-pressionwhen adequate systems are inplace to ensure accurate diagnosis andtreatment.26 Early detection of depres-sed symptoms makes referral for for-mal evaluation possible and has shownto be effective in pediatric primary caresettings.27–30 In a high-risk patient pop-ulation such as adolescents with type 1diabetes, we hypothesized that depres-sion screening would identify risk fordepression and serve as an indicator ofpotential problems with diabetes man-agement. In the present feasibility andoutcomes study, standard depressionscreening was operationalized to detectand address common barriers that pre-vent implementation of routine screen-ing. The specific aimswere to (1) evaluatethe prevalence of depressive symptomsand endorsement of suicidal thoughts ina cohort of adolescents with type 1 di-abetes, (2) quantify the number of socialwork and psychology referrals generatedfrom routine depression screening, (3)evaluate patient and staff acceptance ofdepression screening performed at di-abetes clinic visits, and (4) confirm thedocumented link between depressivesymptoms and glycemic control.
METHODS
Setting
Cincinnati Children’s Hospital MedicalCenter is an urban tertiary care centerwithanon-siteDiabetesCenter that serves1829 patients with type 1 diabetes. Thediabetes team is composed of physicianand nurse practitioner providers, nurses,dieticians, social workers, education spe-cialists, and a clinical psychologist.
Multidisciplinary ScreeningCommittee and QualityImprovement Methodology
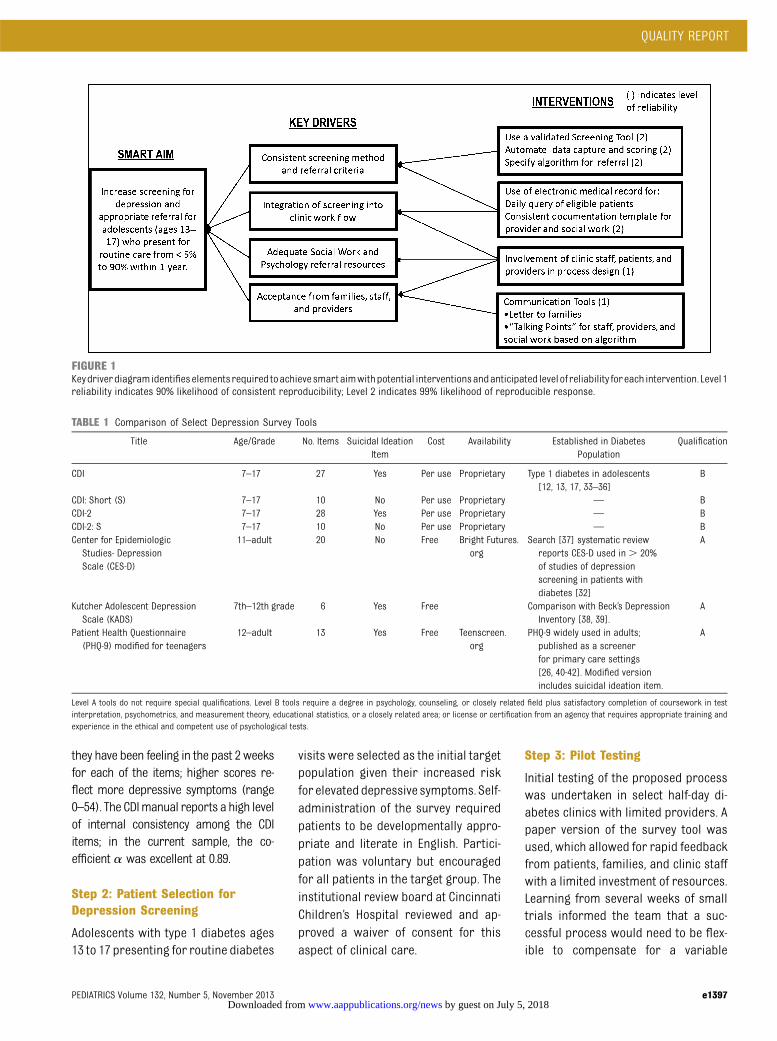
In April 2010, a multidisciplinary com-mittee composed of endocrinologyproviders, pediatric psychologists, andsocialworkerswasestablished. Utilizinga quality improvement (QI) framework,the group identified an overall goal toestablish feasibility and clinical signifi-cance of routine depression screening ina tertiary care diabetes center. A mea-sureable and time bound specific aimwas developed, which was to increasedepression screening and appropriatemental health referral rates from abaseline of 5% to 90% within 1 year. Fourintegral components, or key drivers,wereidentified that were critical for success oftheproject. Foreachkeydriver, a series ofinterventions were identified (Fig 1).Representatives from each step in theproposed process (eg, registration, pointof care testing, nurse intake, providerencounter) were included in the designdevelopment, which included anticipationof possible problems at each step withcorrelated interventions to address thepotential obstacle. Institute of HealthcareImprovement methodology was followedto iteratively test interventions targetedto each of the 4 key drivers with a seriesof plan, do, study, act (PDSA) cycles todefine a reliable process for depressionscreening and referral.
Step 1: Identification of aScreening Measure
Thecommitteeconsideredpublishedvalidmeasures of depression (Table 1) andselected the Children’s Depression In-ventory (CDI) as the screening tool. TheCDI is a 27-item, widely used measure ofdepressive symptoms in children ages 7to 17 (inclusive) in clinical and researchsettings. TheCDI iswritten at a third gradereading level, can be self-administered in15 minutes or less and includes an itemabout suicidal ideation.31 Adolescents se-lect 1 of 3 statements that describe how
e1396 CORATHERS et al by guest on July 5, 2018www.aappublications.org/newsDownloaded from
they have been feeling in the past 2 weeksfor each of the items; higher scores re-flect more depressive symptoms (range0–54). The CDImanual reports a high levelof internal consistency among the CDIitems; in the current sample, the co-efficient a was excellent at 0.89.
Step 2: Patient Selection forDepression Screening
Adolescents with type 1 diabetes ages13 to 17 presenting for routine diabetes
visits were selected as the initial targetpopulation given their increased riskfor elevateddepressive symptoms. Self-administration of the survey requiredpatients to be developmentally appro-priate and literate in English. Partici-pation was voluntary but encouragedfor all patients in the target group. Theinstitutional review board at CincinnatiChildren’s Hospital reviewed and ap-proved a waiver of consent for thisaspect of clinical care.
Step 3: Pilot Testing
Initial testing of the proposed processwas undertaken in select half-day di-abetes clinics with limited providers. Apaper version of the survey tool wasused, which allowed for rapid feedbackfrom patients, families, and clinic staffwith a limited investment of resources.Learning from several weeks of smalltrials informed the team that a suc-cessful process would need to be flex-ible to compensate for a variable
FIGURE 1Keydriverdiagramidentifieselementsrequired toachievesmartaimwithpotential interventionsandanticipated levelof reliability foreach intervention. Level1reliability indicates 90% likelihood of consistent reproducibility; Level 2 indicates 99% likelihood of reproducible response.
TABLE 1 Comparison of Select Depression Survey Tools
Title Age/Grade No. Items Suicidal IdeationItem
Cost Availability Established in DiabetesPopulation
Qualification
CDI 7–17 27 Yes Per use Proprietary Type 1 diabetes in adolescents[12, 13, 17, 33–36]
B
CDI: Short (S) 7–17 10 No Per use Proprietary — BCDI-2 7–17 28 Yes Per use Proprietary — BCDI-2: S 7–17 10 No Per use Proprietary — BCenter for Epidemiologic
Studies- DepressionScale (CES-D)
11–adult 20 No Free Bright Futures.org
Search [37] systematic reviewreports CES-D used in . 20%of studies of depressionscreening in patients withdiabetes [32]
A
Kutcher Adolescent DepressionScale (KADS)
7th–12th grade 6 Yes Free Comparison with Beck’s DepressionInventory [38, 39].
A
Patient Health Questionnaire(PHQ-9) modified for teenagers
12–adult 13 Yes Free Teenscreen.org
PHQ-9 widely used in adults;published as a screenerfor primary care settings[26, 40-42]. Modified versionincludes suicidal ideation item.
A
Level A tools do not require special qualifications. Level B tools require a degree in psychology, counseling, or closely related field plus satisfactory completion of coursework in testinterpretation, psychometrics, and measurement theory, educational statistics, or a closely related area; or license or certification from an agency that requires appropriate training andexperience in the ethical and competent use of psychological tests.
QUALITY REPORT
PEDIATRICS Volume 132, Number 5, November 2013 e1397 by guest on July 5, 2018www.aappublications.org/newsDownloaded from
volume of patients and efficient so as toavoid adding time to the visit.
Step 4: Revision to the ScreeningProcess and Implementation
The multidisciplinary committee metbiweekly for the first year. Intervalinteractions with key stakeholderswere conducted periodically to gaininput and provide updates. Trainingsessions between providers and psy-chologists resulted in production oftalking points for outcomes of de-pression screening. The committee de-veloped a revised screening processthrough a series of PDSA ramps andconsideration of the pilot testing results.Additional support from the informationtechnology department and a data pro-grammerwere required to automate thescreening process. Paper forms werereplaced with electronic tablets to im-prove reliability, ensure accuracy of de-pressionscreeningscores,andtoreducestaff burden. The screening process isdescribed below and included in Fig 2.
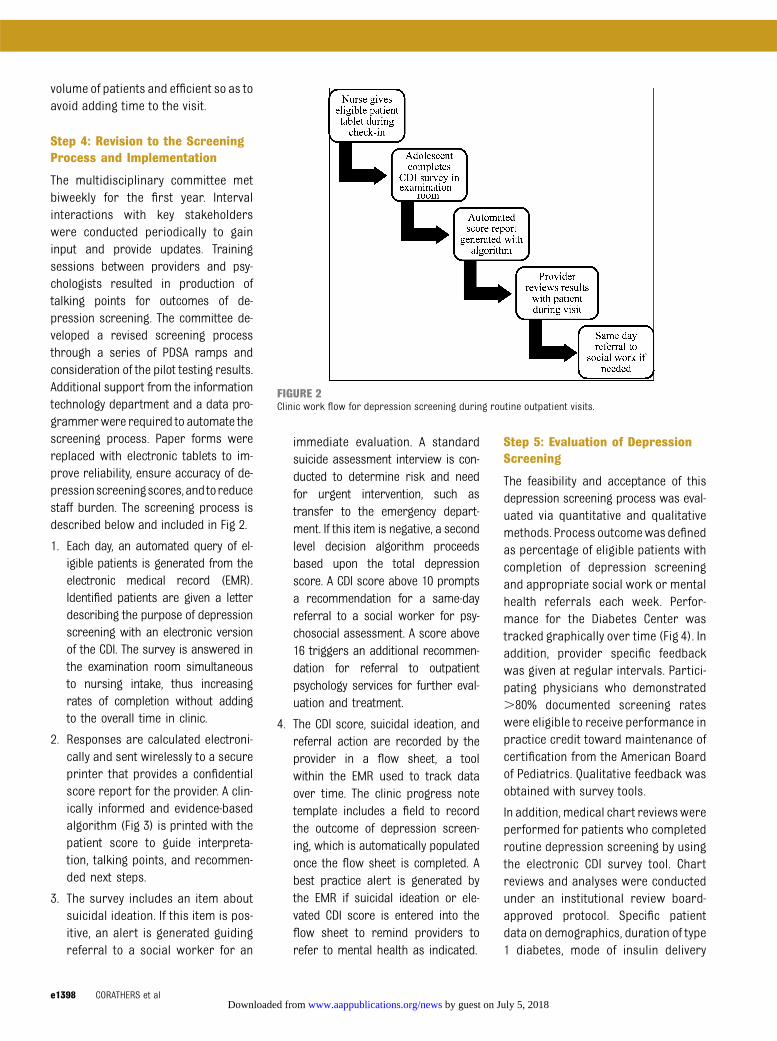
1. Each day, an automated query of el-igible patients is generated from theelectronic medical record (EMR).Identified patients are given a letterdescribing the purpose of depressionscreening with an electronic versionof the CDI. The survey is answered inthe examination room simultaneousto nursing intake, thus increasingrates of completion without addingto the overall time in clinic.
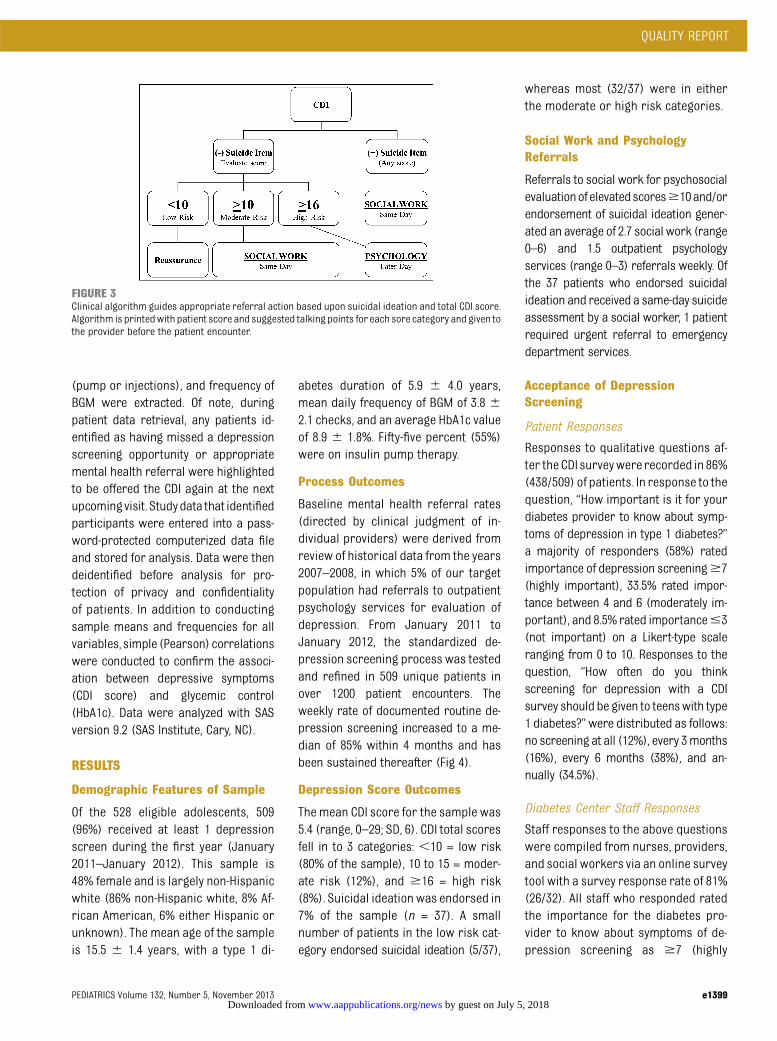
2. Responses are calculated electroni-cally and sent wirelessly to a secureprinter that provides a confidentialscore report for the provider. A clin-ically informed and evidence-basedalgorithm (Fig 3) is printed with thepatient score to guide interpreta-tion, talking points, and recommen-ded next steps.
3. The survey includes an item aboutsuicidal ideation. If this item is pos-itive, an alert is generated guidingreferral to a social worker for an
immediate evaluation. A standardsuicide assessment interview is con-ducted to determine risk and needfor urgent intervention, such astransfer to the emergency depart-ment. If this item is negative, a secondlevel decision algorithm proceedsbased upon the total depressionscore. A CDI score above 10 promptsa recommendation for a same-dayreferral to a social worker for psy-chosocial assessment. A score above16 triggers an additional recommen-dation for referral to outpatientpsychology services for further eval-uation and treatment.
4. The CDI score, suicidal ideation, andreferral action are recorded by theprovider in a flow sheet, a toolwithin the EMR used to track dataover time. The clinic progress notetemplate includes a field to recordthe outcome of depression screen-ing, which is automatically populatedonce the flow sheet is completed. Abest practice alert is generated bythe EMR if suicidal ideation or ele-vated CDI score is entered into theflow sheet to remind providers torefer to mental health as indicated.
Step 5: Evaluation of DepressionScreening
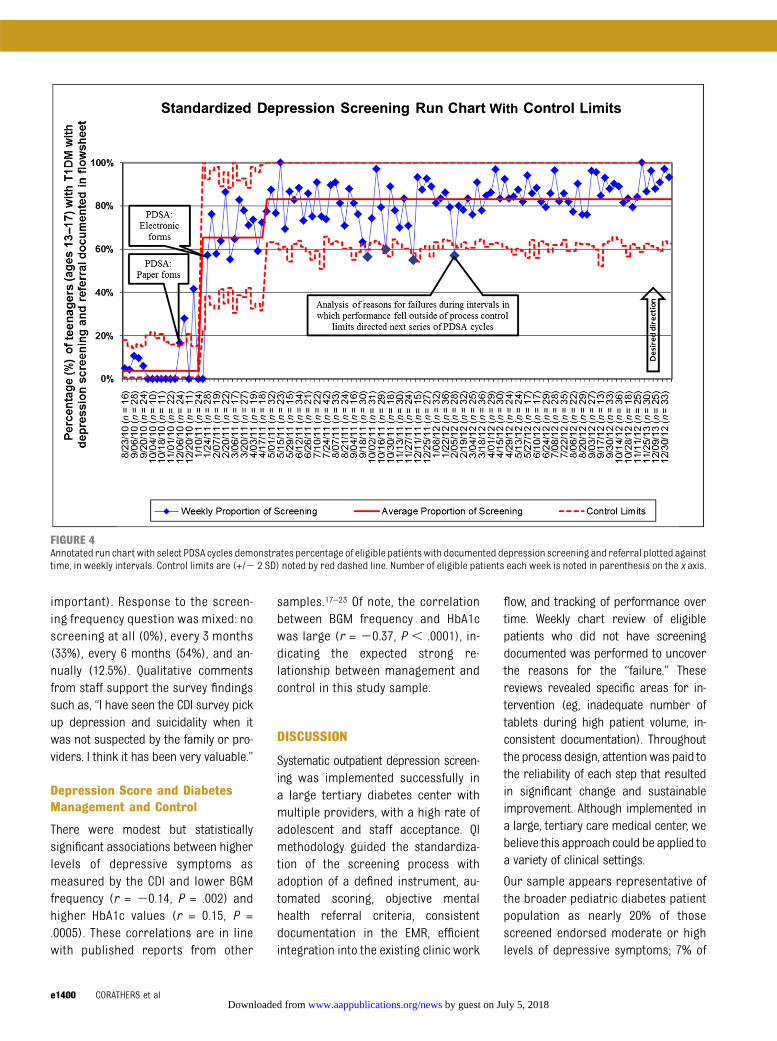
The feasibility and acceptance of thisdepression screening process was eval-uated via quantitative and qualitativemethods. Process outcomewasdefinedas percentage of eligible patients withcompletion of depression screeningand appropriate social work or mentalhealth referrals each week. Perfor-mance for the Diabetes Center wastracked graphically over time (Fig 4). Inaddition, provider specific feedbackwas given at regular intervals. Partici-pating physicians who demonstrated.80% documented screening rateswere eligible to receive performance inpractice credit toward maintenance ofcertification from the American Boardof Pediatrics. Qualitative feedback wasobtained with survey tools.
In addition, medical chart reviewswereperformed for patients who completedroutine depression screening by usingthe electronic CDI survey tool. Chartreviews and analyses were conductedunder an institutional review board-approved protocol. Specific patientdata on demographics, duration of type1 diabetes, mode of insulin delivery
FIGURE 2Clinic work flow for depression screening during routine outpatient visits.
e1398 CORATHERS et al by guest on July 5, 2018www.aappublications.org/newsDownloaded from
(pump or injections), and frequency ofBGM were extracted. Of note, duringpatient data retrieval, any patients id-entified as having missed a depressionscreening opportunity or appropriatemental health referral were highlightedto be offered the CDI again at the nextupcomingvisit. Studydata that identifiedparticipants were entered into a pass-word-protected computerized data fileand stored for analysis. Data were thendeidentified before analysis for pro-tection of privacy and confidentialityof patients. In addition to conductingsample means and frequencies for allvariables, simple (Pearson) correlationswere conducted to confirm the associ-ation between depressive symptoms(CDI score) and glycemic control(HbA1c). Data were analyzed with SASversion 9.2 (SAS Institute, Cary, NC).
RESULTS
Demographic Features of Sample
Of the 528 eligible adolescents, 509(96%) received at least 1 depressionscreen during the first year (January2011–January 2012). This sample is48% female and is largely non-Hispanicwhite (86% non-Hispanic white, 8% Af-rican American, 6% either Hispanic orunknown). The mean age of the sampleis 15.5 6 1.4 years, with a type 1 di-
abetes duration of 5.9 6 4.0 years,mean daily frequency of BGM of 3.8 62.1 checks, and an average HbA1c valueof 8.9 6 1.8%. Fifty-five percent (55%)were on insulin pump therapy.
Process Outcomes
Baseline mental health referral rates(directed by clinical judgment of in-dividual providers) were derived fromreview of historical data from the years2007–2008, in which 5% of our targetpopulation had referrals to outpatientpsychology services for evaluation ofdepression. From January 2011 toJanuary 2012, the standardized de-pression screening process was testedand refined in 509 unique patients inover 1200 patient encounters. Theweekly rate of documented routine de-pression screening increased to a me-dian of 85% within 4 months and hasbeen sustained thereafter (Fig 4).
Depression Score Outcomes
The mean CDI score for the sample was5.4 (range, 0–29; SD, 6). CDI total scoresfell in to 3 categories: ,10 = low risk(80% of the sample), 10 to 15 = moder-ate risk (12%), and $16 = high risk(8%). Suicidal ideation was endorsed in7% of the sample (n = 37). A smallnumber of patients in the low risk cat-egory endorsed suicidal ideation (5/37),
whereas most (32/37) were in eitherthe moderate or high risk categories.
Social Work and PsychologyReferrals
Referrals to social work for psychosocialevaluationofelevatedscores$10and/orendorsement of suicidal ideation gener-ated an average of 2.7 social work (range0–6) and 1.5 outpatient psychologyservices (range 0–3) referrals weekly. Ofthe 37 patients who endorsed suicidalideation and received a same-day suicideassessment by a social worker, 1 patientrequired urgent referral to emergencydepartment services.
Acceptance of DepressionScreening
Patient Responses
Responses to qualitative questions af-ter the CDI surveywere recorded in 86%(438/509) of patients. In response to thequestion, “How important is it for yourdiabetes provider to know about symp-toms of depression in type 1 diabetes?”a majority of responders (58%) ratedimportance of depression screening$7(highly important), 33.5% rated impor-tance between 4 and 6 (moderately im-portant), and 8.5% rated importance#3(not important) on a Likert-type scaleranging from 0 to 10. Responses to thequestion, “How often do you thinkscreening for depression with a CDIsurvey should be given to teenswith type1 diabetes?”were distributed as follows:no screening at all (12%), every 3months(16%), every 6 months (38%), and an-nually (34.5%).
Diabetes Center Staff Responses
Staff responses to the above questionswere compiled from nurses, providers,and social workers via an online surveytool with a survey response rate of 81%(26/32). All staff who responded ratedthe importance for the diabetes pro-vider to know about symptoms of de-pression screening as $7 (highly
FIGURE 3Clinical algorithm guides appropriate referral action based upon suicidal ideation and total CDI score.Algorithm is printedwith patient score and suggested talking points for each sore category and given tothe provider before the patient encounter.
QUALITY REPORT
PEDIATRICS Volume 132, Number 5, November 2013 e1399 by guest on July 5, 2018www.aappublications.org/newsDownloaded from
important). Response to the screen-ing frequency question was mixed: noscreening at all (0%), every 3 months(33%), every 6 months (54%), and an-nually (12.5%). Qualitative commentsfrom staff support the survey findingssuch as, “I have seen the CDI survey pickup depression and suicidality when itwas not suspected by the family or pro-viders. I think it has been very valuable.”
Depression Score and DiabetesManagement and Control
There were modest but statisticallysignificant associations between higherlevels of depressive symptoms asmeasured by the CDI and lower BGMfrequency (r = 20.14, P = .002) andhigher HbA1c values (r = 0.15, P =.0005). These correlations are in linewith published reports from other
samples.17–23 Of note, the correlationbetween BGM frequency and HbA1cwas large (r = 20.37, P , .0001), in-dicating the expected strong re-lationship between management andcontrol in this study sample.
DISCUSSION
Systematic outpatient depression screen-ing was implemented successfully ina large tertiary diabetes center withmultiple providers, with a high rate ofadolescent and staff acceptance. QImethodology guided the standardiza-tion of the screening process withadoption of a defined instrument, au-tomated scoring, objective mentalhealth referral criteria, consistentdocumentation in the EMR, efficientintegration into the existing clinic work
flow, and tracking of performance overtime. Weekly chart review of eligiblepatients who did not have screeningdocumented was performed to uncoverthe reasons for the “failure.” Thesereviews revealed specific areas for in-tervention (eg, inadequate number oftablets during high patient volume, in-consistent documentation). Throughoutthe process design, attentionwas paid tothe reliability of each step that resultedin significant change and sustainableimprovement. Although implemented ina large, tertiary care medical center, webelieve this approach could be applied toa variety of clinical settings.
Our sample appears representative ofthe broader pediatric diabetes patientpopulation as nearly 20% of thosescreened endorsed moderate or highlevels of depressive symptoms; 7% of
FIGURE 4Annotated run chart with select PDSA cycles demonstrates percentage of eligible patientswith documented depression screening and referral plotted againsttime, in weekly intervals. Control limits are (+/2 2 SD) noted by red dashed line. Number of eligible patients each week is noted in parenthesis on the x axis.
e1400 CORATHERS et al by guest on July 5, 2018www.aappublications.org/newsDownloaded from

the sample endorsed suicidal ideation.Consistentwith the literature, therewerepositive correlations between higherdepressive symptom scores and worsediabetes management and control, sup-porting our hypothesis that depressionscreeningprovides an indicationof youthat-risk for suboptimal diabetes-specifichealth outcomes. Furthermore, qualita-tive provider feedback indicated that anobjective survey score facilitated con-versation with families about psychoso-cial conditions affecting diabetes care.Routine screening enabled providers toidentify patients at risk for more signif-icant depression and refer for mentalhealth evaluation and treatment. Earlieridentification and treatment of depres-sion is predicted to remove barriers toadherenceandimprovecopingskillswithchronic illness thus leading to more ef-fective self-management behaviors andimproved outcomes.
The “lessons learned” from this processhighlight a critical point; the integrationof depression screening into a busy clin-ical setting is challenging but feasible. Interms of cost, an investment of $4800 tocover the initial expense of computertablets, data programming time, andproprietary materials was required,which translates to approximately $4.00per encounter for the first year. Themaintenance cost for the proprietarycharge of the screening instrument isapproximately $2.00 per encounter. Theclinic is located within a hospital setting,which supports the staffing and refer-ral resources, including clinical social
workers and pediatric psychologists in acollaborating division (Behavioral Medi-cine and Clinical Psychology) to ensureaccurate diagnosis and treatment of de-pression and/or suicidal ideation whenidentified. The role of social workers inthe Diabetes Center is well established.Interpretation and discussion of elevatedCDI scores falls within their current jobdescription. Equivalent resources maynot be available in all clinics, althoughresearch and clinical data indicate theoverwhelming need for these psychoso-cial services.
The generalizability of the previouslydescribed depression screening processto other clinical locations may be limitedby differences in institutional supportand regional mental health referralresources.However, themodelpresentedhere can be modified to fit local resour-ces. The critical step to achieving im-proved rates of routine depressionscreeningandmentalhealthreferrals foradolescents was to identify a standardprocess and set of expectations. A varietyof screening tools are available (Table 1)at no cost both with and without an itemassessing suicidal ideation. Translationinto additional languages may be avail-able with permission of the publisher. Arecent systematic review providesa comprehensive listing of instrumentsused for screening of depression in type1 and type 2 diabetes.32 The decision ofwhich tool is most appropriate fora clinic should be guided by localresources. In our study, clear recom-mendations including talking points and
indication for referral for further evalu-ation based upon the output of the as-sessment tool gave providers a platformto discuss mental health topics ina medical setting. Consistent documen-tation via a common template ensuredstandard assessment and facilitatedtracking of scores over time.
CONCLUSIONS AND FUTUREDIRECTIONS
The described QI initiative to implementroutine depression screening for ado-lescents with type 1 diabetes addressesa significant gap between national rec-ommendations and widespread clinicalpractice. Implications of this researchare wide reaching as this process mayserve as a model for integration of de-pression screening across a variety ofclinical settings for youth with chronichealth conditions.
Further research is needed to determinelongitudinal diabetes and psychologyoutcomes. Future studies will includeevaluation of the uptake and outcome ofpsychology referrals in reducing de-pressivesymptomsand improvinghealthoutcomes. In addition, cost-effectivenessanalysis of depression screening andintervention in this population should beexplored. Based upon our current re-search, it isrecommendedthatscreeningoccur at least annually and be examinedwithin the context of how depressionscores relate to diabetesmanagement toinform health-promoting clinical inter-ventions.
REFERENCES
1. Modi AC, Pai AL, Hommel KA, et al. Pediatricself-management: a framework for re-search, practice, and policy. Pediatrics.2012;129(2). Available at: www.pediatrics.org/cgi/content/full/129/2/e473
2. Liese AD, D’Agostino RB Jr, Hamman RF,et al; SEARCH for Diabetes in Youth StudyGroup. The burden of diabetes mellitusamong US youth: prevalence estimates
from the SEARCH for Diabetes in YouthStudy. Pediatrics. 2006;118(4):1510–1518
3. Miller KM, Beck RW, Bergenstal RM, et al;T1D Exchange Clinic Network. Evidence ofa Strong Association Between Frequency ofSelf-Monitoring of Blood Glucose and He-moglobin A1c Levels in T1D Exchange ClinicRegistry Participants. Diabetes Care. 2013;36(7):2009–2014
4. DCCT Research Group. Diabetes Controland Complications Trial (DCCT). Update.Diabetes Care. 1990;13(4):427–433
5. Mortensen HB, Hougaard P; The Hvidøre StudyGroup on Childhood Diabetes. Comparison ofmetabolic control in a cross-sectional study of2,873 children and adolescents with IDDMfrom 18 countries. Diabetes Care. 1997;20(5):714–720
QUALITY REPORT
PEDIATRICS Volume 132, Number 5, November 2013 e1401 by guest on July 5, 2018www.aappublications.org/newsDownloaded from

6. Danne T, Mortensen HB, Hougaard P, et al;Hvidøre Study Group on Childhood Di-abetes. Persistent differences among cen-ters over 3 years in glycemic control andhypoglycemia in a study of 3,805 childrenand adolescents with type 1 diabetes fromthe Hvidøre Study Group. Diabetes Care.2001;24(8):1342–1347
7. Springer D, Dziura J, Tamborlane WV, et al.Optimal control of type 1 diabetes mellitusin youth receiving intensive treatment. JPediatr. 2006;149(2):227–232
8. Lewinsohn PM, Rohde P, Seeley JR, Klein DN,Gotlib IH. Natural course of adolescent majordepressive disorder in a community sample:predictors of recurrence in young adults.Am J Psychiatry. 2000;157(10):1584–1591
9. Costello EJ, Mustillo S, Erkanli A, Keeler G,Angold A. Prevalence and development of psy-chiatric disorders in childhood and adoles-cence. Arch Gen Psychiatry. 2003;60(8):837–844
10. Merikangas KR, He JP, Burstein M, et al.Lifetime prevalence of mental disorders inU.S. adolescents: results from the NationalComorbidity Survey Replication—Adoles-cent Supplement (NCS-A). J Am Acad ChildAdolesc Psychiatry. 2010;49(10):980–989
11. Grey M, Whittemore R, Tamborlane W. De-pression in type 1 diabetes in children:natural history and correlates. J Psycho-som Res. 2002;53(4):907–911
12. Hood KK, Huestis S, Maher A, Butler D, Volk-ening L, Laffel LM. Depressive symptoms inchildren and adolescents with type 1 diabetes:association with diabetes-specific character-istics. Diabetes Care. 2006;29(6):1389–1391
13. McGrady ME, Laffel L, Drotar D, Repaske D,Hood KK. Depressive symptoms and glycemiccontrol in adolescents with type 1 diabetes:mediational role of blood glucose monitor-ing. Diabetes Care. 2009;32(5):804–806
14. Ji L, Lili S, Jing W, et al. Appearance con-cern and depression in adolescent girls
with systemic lupus erythematous. ClinRheumatol. 2012;31(12):1671–1675
15. Szigethy E, Levy-Warren A, Whitton S, et al.Depressive symptoms and inflammatorybowel disease in children and adolescents:a cross-sectional study. J Pediatr Gastro-enterol Nutr. 2004;39(4):395–403
16. Kovacs M, Goldston D, Obrosky DS, BonarLK. Psychiatric disorders in youths withIDDM: rates and risk factors. Diabetes Care.1997;20(1):36–44
17. Hilliard ME, Herzer M, Dolan LM, Hood KK.Psychological screening in adolescentswith type 1 diabetes predicts outcomes oneyear later. Diabetes Res Clin Pract. 2011;94(1):39–44
18. Hassan K, Loar R, Anderson BJ, Heptulla RA.The role of socioeconomic status, de-pression, quality of life, and glycemic con-trol in type 1 diabetes mellitus. J Pediatr.2006;149(4):526–531
19. Lernmark B, Persson B, Fisher L, RydeliusPA. Symptoms of depression are importantto psychological adaptation and metaboliccontrol in children with diabetes mellitus.Diabet Med. 1999;16(1):14–22
20. Bernstein CM, Stockwell MS, Gallagher MP,Rosenthal SL, Soren K. Mental health issuesin adolescents and young adults with type 1diabetes: prevalence and impact on glycemiccontrol. Clin Pediatr (Phila). 2013;52(1):10–15
21. Van Tilburg MA, McCaskill CC, Lane JD, et al.Depressed mood is a factor in glycemiccontrol in type 1 diabetes. Psychosom Med.2001;63(4):551–555
22. Rewers A, Chase HP, Mackenzie T, et al.Predictors of acute complications in chil-dren with type 1 diabetes. JAMA. 2002;287(19):2511–2518
23. Stewart SM, Rao U, Emslie GJ, Klein D, WhitePC. Depressive symptoms predict hospital-ization for adolescents with type 1 diabetesmellitus. Pediatrics. 2005;115(5):1315–1319
24. Copeland WE, Shanahan L, Costello EJ,Angold A. Childhood and adolescent psy-chiatric disorders as predictors of youngadult disorders. Arch Gen Psychiatry. 2009;66(7):764–772
25. Kovacs M, Lopez-Duran N. Prodromalsymptoms and atypical affectivity as pre-dictors of major depression in juveniles:implications for prevention. J Child PsycholPsychiatry. 2010;51(4):472–496
26. US Preventive Services Task Force. Screen-ing and treatment for major depressivedisorder in children and adolescents: USPreventive Services Task Force Recommen-dation Statement. Pediatrics. 2009;123(4):1223–1228
27. Valuck RJ, Anderson HO, Libby AM, et al.Enhancing electronic health record mea-surement of depression severity and sui-cide ideation: a Distributed AmbulatoryResearch in Therapeutics Network (DART-Net) study. J Am Board Fam Med. 2012;25(5):582–593
28. Ham P, Allen C. Adolescent health screeningand counseling. Am Fam Physician. 2012;86(12):1109–1116
29. Hermanns N, Caputo S, Dzida G, Khunti K,Meneghini LF, Snoek F. Screening, evalua-tion and management of depression inpeople with diabetes in primary care. PrimCare Diabetes. 2013;7(1):1–10
30. Zuckerbrot RA, Maxon L, Pagar D, Davies M,Fisher PW, Shaffer D. Adolescent depressionscreening in primary care: feasibility andacceptability. Pediatrics. 2007;119(1):101–108
31. Kovacs M. The Children’s Depression, In-ventory (CDI). Psychopharmacol Bull. 1985;21(4):995–998
32. Roy T, Lloyd CE, Pouwer F, Holt RI, SartoriusN. Screening tools used for measuring de-pression among people with Type 1 andType 2 diabetes: a systematic review. DiabetMed. 2012;29(2):164–175
(Continued from first page)
www.pediatrics.org/cgi/doi/10.1542/peds.2013-0681
doi:10.1542/peds.2013-0681
Accepted for publication Jul 16, 2013
Address correspondence to Sarah D. Corathers, MD, Division of Endocrinology, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, MLC7012, Cincinnati,OH 45219. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURES: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICTS OF INTEREST: Dr Hood reports consultancy with Fortis Spectrum Medical Education Group: One time advisory panel for development ofprofessional education materials for those working with teenagers with type 1 diabetes; the other authors have indicated they have no potential conflicts ofinterest to disclose.
e1402 CORATHERS et al by guest on July 5, 2018www.aappublications.org/newsDownloaded from

originally published online October 14, 2013; Pediatrics Hood
Mary Jolly, Nancy Morwessel, Peggy Crawford, Lawrence M. Dolan and Korey K. Sarah D. Corathers, Jessica Kichler, Nana-Hawa Yayah Jones, Andrea Houchen,
Improving Depression Screening for Adolescents With Type 1 Diabetes
ServicesUpdated Information &
013-0681http://pediatrics.aappublications.org/content/early/2013/10/09/peds.2including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 5, 2018www.aappublications.org/newsDownloaded from
originally published online October 14, 2013; Pediatrics Hood
Mary Jolly, Nancy Morwessel, Peggy Crawford, Lawrence M. Dolan and Korey K. Sarah D. Corathers, Jessica Kichler, Nana-Hawa Yayah Jones, Andrea Houchen,
Improving Depression Screening for Adolescents With Type 1 Diabetes
http://pediatrics.aappublications.org/content/early/2013/10/09/peds.2013-0681located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 5, 2018www.aappublications.org/newsDownloaded from





























