Embed Size (px)
Citation preview

REVIEW
Improving diabetes patient outcomes: Framing research into thechronic care modelSusan Dancer, RN, MSN, FNP1 & Maureen (Reni) Courtney, PhD, APRN, FNP-BC (Associate Professor)2
1 Family Practice of Dr. David Podgurecki, Mansfield, Texas2University of Texas Arlington College of Nursing, Arlington, Texas
KeywordsType 2 diabetes; diabetes; chronic illness; nurse
practitioners; research; chronic illness model;
disease management.
CorrespondenceMaureen (Reni) Courtney, PhD, APRN, FNP-BC,
University of Texas Arlington College of
Nursing, Box 19407, Arlington, TX 76019.
Tel: 817-272-2776;
Fax: 817-272-5006;
E-mail: [email protected]
Received: February 2009;
accepted: October 2009
doi: 10.1111/j.1745-7599.2010.00559.x
Abstract
Purpose: To review recent research findings that improve outcomes for type2 diabetes mellitus (T2DM) patients and frame them within the chronic caremodel (CCM).Data sources: Published research studies and research reviews from multiplecomputerized databases were examined regarding care of patients with T2DM.Conclusions: Improving outcomes for patients with chronic diseases such asT2DM is a healthcare system imperative. Disease management must shift froman incomplete and scattered focus on episodic care to a comprehensive modelof care such as offered by the CCM. This model emphasizes the essential el-ements of health organization, clinical information systems, decision support,delivery system design, self-management support, and community required toeffectively improve care for these patients.Implications for practice: Understanding the comprehensive elementsneeded for quality chronic disease care is essential to improving outcomes. Asnew interventions for improving T2DM outcomes become available, the nursepractitioner (NP) must be able to evaluate these as they relate to elementsof care that comprise the CCM. Framing new research interventions into thismodel allows the NP to assume a multifaceted leadership role in improving thecare and outcomes of these patients.
Type 2 diabetes mellitus (T2DM) is a complex diseaserequiring continuous patient involvement and man-agement by a team of healthcare professionals. Whileguidelines for treatment and disease outcomes have beendeveloped and recognized nationally (American DiabetesAssociation [ADA], 2009), one specific approach foraddressing the multifaceted issues in T2DM care, thechronic care model (CCM), is not yet widely known oraccepted.
The CCM is a model of care specifically defining the es-sential elements of chronic disease care that is well suitedto the management of T2DM. The model provides guid-ance for a shift from an acute, episodic health systemfocus to one that is required for effective chronic dis-ease care. Organizations and professionals specializing inthe management of T2DM are increasingly adapting thisframework to address the many aspects of chronic care(Wagner et al., 2001).
The nurse practitioner (NP) plays a crucial role in man-aging chronic disease patients. Understanding the role
of research and evidence-based interventions within theCCM can assist the NP to assume a leadership role inimproving the care and outcomes of these patients. TheCCM promotes a broad system perspective that permitsthe NP to focus action toward specific system elements asneeded to improve patient outcomes. The NP is no longerlimited to trying to improve care for the T2DM patientusing the framework of a typical 15–20 min episodic visitwhen fully using the CCM to guide care enhancements.The purpose of this article is to review recent researchfindings that improve outcomes for T2DM patients andframe them within the CCM.
Background
Management and care of patients with T2DM is a grow-ing public health concern because of increased incidence,costs, and complexity of care. The incidence of new casesof T2DM among middle-aged Americans has doubledover the last three decades (Fox et al., 2007).
580 Journal of the American Academy of Nurse Practitioners 22 (2010) 580–585 C©2010 The Author(s)Journal compilation C©2010 American Academy of Nurse Practitioners

S. Dancer & M. (Reni) Courtney Chronic Care Model
The cost of diabetes care is a public and personal fi-nancial burden. Cost has been estimated to range from$1700–$2100 annually for adults with diet-controlled di-abetes and no microvascular complications. These costsincrease by 60%–90% as patients progress to insulin useand macrovascular incidents such as myocardial infarc-tion (MI) and stroke (Brandle et al., 2003). Direct medicalcosts of diabetes care in 2006 were estimated to be $22.9billion (American Association of Clinical Endocrinolo-gists, 2007) and can be expected to increase significantlygiven the increasing incidence and progression of thedisease.
Care of these patients is becoming more complex andtime consuming. Patients with T2DM list an average offive or more medications for control of glucose, hyper-tension, and hyperlipidemia. Visits lasting longer than20 min increased from 17.8% in 1991 to 20.9% in 2000(Grant, Pirraglia, Meigs, & Singer, 2004).
This increased incidence, cost, and complexity of caredemand an empirical approach to applying evidence-based interventions at all levels of care. Applying isolatedinterventions that address only a single aspect of care failsto address the multifaceted clinical problem of diabetesmanagement.
Relevance for NPs
NPs have an essential role in chronic disease manage-ment. With expanding roles and increased reimburse-ment opportunities, NPs are uniquely positioned to ad-dress issues of increasing incidence, cost, and complex-ity of care (Boville et al., 2007). Consequently, under-standing the CCM and how evidence-based interven-tions fit into this model of care is critical in optimalmanagement of patients with a chronic disease such asT2DM.
Professional groups are increasingly adopting the CCMfor delivering health care to chronic disease patients. TheAmerican Association of Diabetes Educators has recentlyendorsed the CCM as the model of choice for deliveryof care among diabetes educators. This was done in aneffort to begin defining best practices for the delivery ofcare among patients with diabetes (Seminario, Drab, Gab-bay, Gold, & McLaughlin, 2008). As other organizationsincreasingly use the CCM, NPs’ understanding and use ofthe model will need to expand. NPs have been called toaction to adopt the model in practice. Fiandt (2007) de-scribed the CCM as a tool necessary for NPs to apply inpractice and urged NPs to take a leadership role in im-proving quality of care and implementing components ofthe CCM in practice.
Finally, as NPs are increasingly engaged in the designof interventions to improve disease outcomes, they need
to be aware of the broad range of elements to be con-sidered. At the heart of the CCM is the evidence that in-terventions addressing just one aspect of chronic care areinadequate in producing long-lasting positive outcomesfor these patients. NPs are in a position to take the lead inimproving clinical practice by using their skills to select abroad range of appropriate interventions that address allaspects of chronic care.
Chronic care model
The CCM was developed by Wagner et al. (2001) in aneffort to differentiate the needs of chronic care patientsin a system previously designed for episodic care. Sincedevelopment, the CCM has been validated for the careof patients with many chronic diseases such as asthma,congestive heart failure, diabetes, and bipolar disorder(Wagner et al., 2001; Robert Wood Johnson Foundation,2007).
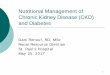
The CCM model is shown in Figure 1. Within the modelare the six major elements that interact to promote high-quality care for patients with chronic disease. The sixelements include: (a) the health system or a health or-ganization, (b) clinical information systems, (c) decisionsupport, (d) delivery system design, (e) self-managementsupport, and (f) community including organizations andresources for patients. Evidence-based interventions arethe main focus and support actions in the componentsof the CCM (Wagner, et al., 2001; Robert Wood John-son Foundation, 2007). The definition of each element,along with recent T2DM interventions and research, isdiscussed below.
Figure 1 Chronic care model.
581

Chronic Care Model S. Dancer & M. (Reni) Courtney
Health system or organization
A specific health system, or an organization of healthcare, is the entity desiring to implement the CCM. It iscomposed of the staff, leaders, operations, values, andgoals of the organization and may vary from a smallfamily practice to a multisite integrated health system.The commitment of the organization must be to imple-ment the CCM to improve chronic disease care, know-ing this will require a careful assessment of the organi-zation and a detailed plan to begin to transform typicalreactive health care to a more proactive, comprehensivecare system. Many organizations are actively consideringhow the CCM can improve their care of T2DM patientsknowing that many patients fail to meet desired criteriafor expected outcomes.
Clinical information system
Clinical information systems in the CCM should con-tain a readily accessible disease-specific database of in-dividual patients (Wagner et al., 2001). This databaseshould alert the provider to needed tests and providetracking and quality improvement data. In accordancewith the main purpose of promoting patient–provider in-teraction, an effective information system for the CCMshould facilitate and promote exchange of informationbetween providers and patients. In addition to individ-ual data, the clinical information system should providea view of a defined population so the practice can assessoverall quality and be proactive in reaching out to pa-tients as needed.
Clinical information systems are often contained withinan electronic medical record (EMR). The effects of useof an EMR on measurable outcomes in diabetes dis-ease management are controversial (Crosson et al., 2007;O’Connor et al., 2005; Trapani et al., 2008). Some stud-ies have reported an increase in the number of tests or-dered in adherence to national guidelines, but no actualimprovement in metabolic control. However, a key factorin studies that did demonstrate improved metabolic con-trol is use of the EMR to generate a report to facilitatepatient–provider conversations and review results andgoals (Larsen, Cannon, & Towner, 2003; Trapani et al.,2008).
Decision support
Decision support and evidence-based guidelines shouldbe consistent with scientific evidence and patient pref-erence. Decision-support guidelines should be embeddedinto daily practice and should be shared with patients toencourage participation. Two ways of facilitating both the
utilization and sharing of this information are point-of-care testing (POCT) of hemoglobin A1c (HgA1c) and theuse of treatment algorithms by an extended healthcareteam and by patients themselves. POCT allows for im-mediate decision support at the time of the appointment.Treatment algorithms extend the decision support of theprimary provider to promote flexibility and timely medi-cation changes in response to assessment findings and labwork.
HgA1c/point of care testing. HgA1c should be per-formed at least twice a year in those who are meet-ing treatment goals and quarterly in those with therapychanges or who are not meeting goals (ADA, 2009). Re-sults should be discussed with patients to guide educationand medication management. Despite these guidelines,research shows that patients do not always know andunderstand their HgA1c numbers and results (Heisler,Piette, Spencer, Kieffer, & Sandeep, 2005). POCT canbe used to increase provider/patient sharing of results.Results are made available during the clinical visit andshared immediately with the patient to facilitate conver-sation, goal setting, and understanding of medication ad-justment.
POCT decreases patient anxiety, increases motivationto adhere to treatment and improves patient perceptionof more face-to-face provider–patient exchange (Brown,Harris, Webster-Bogaert, & Porter, 2004). Brown et al.summarized their qualitative study by stating that POCTstrengthens the collaborative working relationship. Thisrelationship is a core feature of the CCM. Patients whoknew their HgA1c more accurately assessed their bloodsugar control and reported they had a better understand-ing of their care (Heisler et al., 2005).
In addition to improved patient perception, POCT test-ing has been shown to result in more frequent intensi-fication of therapy and lowered HgA1c levels in T2DMpatients (Miller et al., 2003). This success in blood sugarcontrol appears to be maintained over a period of time.In another study by Petersen et al. (2007), patients in thePOCT group had significantly lower HgA1c levels duringthe first year and throughout the 3.5 years of the study.
Treatment algorithms. Treatment algorithms areuseful and effective tools for improving glycemic control.Extending use of treatment algorithms to other health-care team members and patients themselves has beenshown to improve outcomes in diabetes care.
Patient involvement in health care was increased whendiabetes treatment algorithms were used by research as-sistants (Williams et al., 2005). These assistants acted inthe role of health coach before the patients met witha provider. Algorithms were used in prompting patientquestions for providers and in clarifying goals for dis-cussion. This patient activation intervention based on
582

S. Dancer & M. (Reni) Courtney Chronic Care Model
treatment algorithms increased ratings of the patient’s ac-tive involvement in the visit.
Independent medication changes by case managers fol-lowing a protocol or treatment algorithm reduces HgA1cmore than any other intervention aimed toward deliv-ery system design. Shojania et al. (2006) reviewed 50randomized controlled trials to compare the effects of ahealthcare delivery design intervention on glycemic con-trol. Eleven quality improvement strategies and interven-tions were identified in these studies. The interventionswith the most striking reduction in glycemic control werethose allowing case managers (NPs, nurses, and pharma-cists) to use an established treatment protocol or algo-rithm to adjust medication use without waiting for physi-cian authorization.
Patients can safely and effectively use treatment andtitration algorithms as well (Davies, Storms, Shut-ler, Bianchi-Biscay, & Gomis, 2005). In a large-scalestudy, 4558 treatment-resistant patients with T2DM werestarted on insulin using either a physician-controlledtitration protocol or a self-managed algorithm protocol.There was no significant difference in hypoglycemia be-tween the two groups. Most noticeably, there was ahigher reduction in HgA1c in the self-managed groupcompared to the physician-controlled group.
Delivery system design
Delivery system design involves how care delivery ser-vices are organized, staffed, and delivered. This elementis typically where care innovations are implemented andrepresents an important opportunity to improve qualityof care and health outcomes for patients. Revised deliverysystems may include maximizing patient access to health-care providers. Interventions addressing this aspect of theCCM include expanding methods of care via Internet ac-cess, implementing group visits, and also using team careand planned visits. Delivery of team health care with NPsin key roles has also been shown to optimize outcomes.
Internet access. Consistent use of a patient manage-ment website to upload blood glucose monitoring and re-ceive feedback from providers via the Internet was as-sociated with a decrease in HgA1c when compared witha control group without this access (McMahon et al.,2005). In another study (Meigs et al., 2003), 291 patientswere given access to personal clinical data and treatmentadvice via the Internet for a period of 1 year. HgA1cdecreased modestly (0.2%) in the intervention group,but rates of completed testing (e.g., foot care and lipidmeasurement) in accordance with national guidelines in-creased significantly. Subjective measures of patient sat-isfaction and psychosocial outcomes were not measured;however, patient satisfaction in the general population
with web access and provider feedback has been foundto be high (Ralston et al., 2007).
Group care. Group care, shared appointments, andplanned appointments are another way of increasing pa-tient access to care. Models of delivery vary, but groupsof two to four patients with similar concerns and needsare seen together by a provider. They are able to askquestions and also interact with other patients regardingcommon concerns and needs. Studies on group care andshared appointments have produced conflicting resultsregarding metabolic control (Weinger, 2003). However,they have been shown to increase disease knowledge,quality of life, and concordance with national guidelines(Clancy, Cope, Magruder, Huang, & Wolfman, 2003).Other studies of group care have shown decreased pri-mary care office wait times and more positive percep-tions about care (Clancy, Yeager, Huang, & Magruder,2007). Approximately 79% of patients in shared medicalappointments ranked their visit as “excellent” (Bronson& Maxwell, 2004).
Healthcare team. The benefits of team care in de-livery system design have been established and guide-lines have been published by the Centers for DiseaseControl and Prevention (2001). Specific practice modelsfor delivering this type of care are discussed by Boden-heimer and Laing (2007) in an article about the team-let (little team) model of care. This model uses a healthcoach in pre- and postvisit encounters to expand uponthe usual 15 min of care (i.e., typical appointment time)provided in primary care practice. Health coaching wasan aspect of care that was incorporated into a large ran-domized study completed by Glasgow et al. (2004) forpatients with T2DM. Brief (8–10 min) coaching sessionsbefore the provider appointment prompted discussion ofpatient goals as well as development of strategies to over-come barriers to achieving goals. Patients in these groupsshowed improvements in depression and quality of lifewhen compared to the control group.
Nurse practitioners. Delivery system designs thatinclude NPs consistently outperform practices employingphysician assistants (PAs). NPs were twice as likely to as-sess HgA1c and 37% more likely to have patients whomeet lipid-treatment guidelines than were physicians orPAs (Obman-Strickland et al., 2008). Both HgA1c and pa-tient satisfaction with care are higher when care is deliv-ered by physician/NP teams when compared to care pro-vided by physicians alone (Litaker et al., 2003).
Planned visits with an NP resulted in improvedglycemic control, lipid management, and hypertensioncontrol. In an intervention utilizing the CCM as a guide,researchers found that 30-min planned visits with NPsimproved glycemic and blood pressure control (Bovilleet al., 2007). The main goals of this program were to
583

Chronic Care Model S. Dancer & M. (Reni) Courtney
achieve recommended test guidelines for patients and toinitiate medication intensification and assist in patientgoal setting.
Self-management support
Providing self-management support to patients withT2DM within the framework of the CCM expands upontraditional didactic methods of teaching to emphasize thepatient’s role in managing health. Providers must com-municate and nurture the patient’s crucial role in dis-ease management. They also must use established self-management techniques such as mutual goal settingand action planning (Robert Wood Johnson Foundation,2007). Historically, these interventions have focused onvarious methods of teaching such as group classes, skilldevelopment, and various lifestyle behaviors. More re-cent interventions have focused on the effectiveness ofcomputer-aided diabetes teaching.
It should be noted here that self-management supportas shown in the CCM model overlaps into both health-care system and community. It is discussed here as an ele-ment of healthcare system, but because self-managementsupport uses elements that are found in the community,some of the interventions may contain elements of bothself-management support and community.
Computer-aided diabetes teaching. Computer-aided diabetes teaching uses technology to teach patientshow to manage their disease as well as testing diseaseunderstanding and providing feedback. Such programsinclude interactive touch-screen programs, computer-assisted consultations, and computerized blood glucosetracking programs. Two major literature reviews ofcomputer-assisted education for patients with diabetesare discussed below.
Boren, Gunlock, Santosh, and Kramer (2006) reviewed19 trials evaluating computer-based patient educationprograms and concluded that 84.2% of the trials showedsignificant benefits in outcomes measured. Measurableeffects on HgA1c were noted in 13 of these trials withthree of these demonstrating significant improvement.Five of the remaining trials showed no significant differ-ence and the rest either did not analyze between groupsor did not calculate significance level.
Jackson, Bolen, Brancati, Batts-Turner, and Gary(2006) reviewed 26 studies involving interactivecomputer-assisted technology, including Internet learn-ing, telephone contact, and computer-assisted integrationof clinical information. Six of 14 studies showed a signif-icant decrease in HgA1c with other measured outcomesshowing mixed results.
While the impact of computer-assisted technology onHgA1c is still being established, the psychosocial and
patient knowledge benefits of such programs are moreclearly defined. Jackson et al. (2006) found an increaseacross psychosocial measurements such as satisfactionwith interventions, support, and quality of life. Further,with computer-aided diabetes teaching, disease under-standing and management knowledge were significantlyincreased (Boren et al., 2006; Jackson et al., 2006).
Community
The community element of the CCM involves linkingand using community resources that support healthcareefforts by clinicians. The use of church-based supportgroups, local community health programs, and clinic-based support groups are acceptable community inter-ventions shown to be helpful and effective in diabetescare (ADA, 2007). Often, the healthcare practice can bea catalyst in identifying and coordinating community re-sources; NPs are often leaders in this effort.
The use of the Internet as a community support tool is amore recent development. Zrebiec (2008) established andevaluated an Internet-based community bulletin boardfor T2DM patients that provided emotional support forpatients and their families. Participants rated the websiteas having a positive effect on coping and hope in dealingwith the disease.
Linking patients with T2DM to one another throughan interactive phone system was investigated in the Vet-eran’s Health Adminsitration (Heisler & Piette, 2005).Patients with poor glycemic control were matched withother patients based on their management needs andwere encouraged to call each other weekly using a toll-free calling line. Patients reported that the calls werehelpful and assisted them in improving self-care. Quan-titative measurements of depressive symptoms, self-careefficacy, and self-management behaviors were shown tosignificantly improve as well.
Summary
As the incidence, cost, and complexity of care of pa-tients with T2DM continues to rise, new models of caremust be considered. With a role that emphasizes collabo-rative care, prevention, and promotion of patient auton-omy and self-management, NPs are uniquely situated toaddress these challenging issues. Evidence shows collab-orative care with NP involvement improves both phys-iological outcomes and patient-centered aspects of care.It is imperative that NPs recognize the importance of im-plementing evidence-based interventions that encompasseach aspect of chronic care within the CCM. Understand-ing T2DM management interventions within the CCM al-lows the NP to more broadly identify gaps, define needs,
584

S. Dancer & M. (Reni) Courtney Chronic Care Model
and design and implement new healthcare strategies toimprove patient outcomes. By understanding and usingthis model, NPs are better able to assume a leadershiprole in health system transformation for chronic diseasecare.
References
American Association of Clinical Endocrinologists. (2007). State of diabetes
complications in America: A comprehensive report issued by the American
Association of Clinical Endocrinologists. Retrieved February 17, 2008, from
http://multivu.prnewswire.com/mnr/AACE/2007/docs/Diabetes
Complications Report.pdf
American Diabetes Association. (2009). Standards of medical care in
diabetes-2009. Diabetes Care, 32(1), S13–S61.
Bodenheimer, T., & Laing, Y. (2007). The teamlet model of primary care.
Annals of Family Medicine, 5, 457–461.
Boren, S. A., Gunlock, T. L., Santosh, K., & Kramer, T. C. (2006).
Computer-aided diabetes education: A synthesis of randomized controlled
trials. American Medical Informatics Association, 2006, 51–55.
Boville, D., Jones, R. R., Saran, M., Radwany, S. M., Salam, J. K., Sweet, D. B.,
et al. (2007). An innovative role for nurse practitioners in managing
chronic disease. Nursing Economics, 25(6), 359–364.
Brandle, M., Smith, B. K., Zhou, H., Smith, B. K., Marriott, D., Burke, R., et al.
(2003). The direct medical cost of T2DM. Diabetes Care, 26, 2300–2304.
Bronson, D. L., & Maxwell, R. A. (2004). Shared medical appointments:
Increasing patient access without increasing physician hours. Cleveland
Clinic Journal of Medicine, 71(5), 369–376.
Brown, J. B., Harris, S. B., Webster-Bogaert, S., & Porter, S. (2004).
Point-of-care testing in diabetes management: What role does it play?
Diabetes Spectrum, 17(4), 244–248.
Centers for Disease Control and Prevention. (2001). Team care: Comprehensive
lifetime management for diabetes. Atlanta, GA: U.S. Department of Health and
Human Services, Public Health Service, Centers for Disease Control and
Prevention, National Center for Chronic Disease Prevention and Health
Promotion.
Clancy, D. E., Cope, D. W., Magruder, K. M., Huang, P., & Wolfman, T. E.
(2003). Evaluating concordance to American Diabetes Association
standards of care for T2DM through group visits in an uninsured or
inadequately insured patient population. Diabetes Care, 26(7), 2032–2036.
Clancy, D. E., Yeager, D. E., Huang, P., & Magruder, K. M. (2007). Further
evaluating the acceptability of group visits in an uninsured or inadequately
insured patient population with uncontrolled T2DM. The Diabetes Educator,
33(2), 309–315.
Crosson, J. C., Ohman-Strickland, P. A., Hahn, K. A., Dicicco-Bloom, B.,
Shaw, E., Orzano, A. J., et al. (2007). Electronic medical records and
diabetes quality of care: Results from a sample of family medicine practices.
Annals of Family Medicine, 5(3), 209–215.
Davies, M., Storms, F., Shutler, S., Bianchi-Biscay, M., & Gomis, R. (2005).
Improvement of glycemic control in subjects with poorly controlled T2DM:
Comparison of two treatment algorithms using insulin glargine. Diabetes
Care, 28(6), 1282–1287.
Fiandt, K. (2007). The chronic care model: Description and application for
practice. Retrieved February 4, 2008, from Medscape Web Site:
http://www.medscape.com/viewarticle/549040
Fox, C. S., Coady, S., Sorlie, P. D., D’Agostino, R. B., Pencina, M. J., et al.
(2007). Increasing cardiovascular disease burden due to diabetes mellitus.
Circulation, 115, 1544–1550.
Glasgow, R., Nutting, P. A., King, D. K., Nelson, C. C., Cutter, G., Gaglio, B.,
et al. (2004). A practical randomized trial to improve diabetes care. Journal
of General Internal Medicine, 19, 1167–1174.
Grant, R. W., Pirraglia, P. A., Meigs, J. B., & Singer, D. E. (2004). Trends in
complexity of diabetes care in the United States from 1991 to 2000. Archives
of Internal Medicine, 164(10), 1134–1139.
Heisler, M., & Piette, J. D. (2005). I help you and you help me: Facilitated
telephone peer support among patients with diabetes. Diabetes Educator,
31(6), 869–879.
Heisler, M., Piette, J. D., Spencer, M., Kieffer, E., & Sandeep, V. (2005).
The relationship between knowledge of recent HgA1c values and
diabetes care understanding and self-management. Diabetes Care, 28,
816–822.
Jackson, C. L., Bolen, S., Brancati, F. L., Batts-Turner, M. L., & Gary, T. L.
(2006). A systematic review of interactive computer-assisted technology in
diabetes care. Journal of General Internal Medicine, 21(2), 105–110.
Larsen, D. L., Cannon, W., & Towner, S. (2003). Longitudinal assessment of a
diabetes care management system in an integrated health network. Journal
of Managed Care Pharmacy, 9(6), 552–558.
Litaker, D., Mion, L. C., Planavsky, L., Kippes, C., Mehta, N., & Frolkis, J.
(2003). Physician-nurse practitioner teams in chronic disease management:
The impact on costs, clinical effectiveness, and patient’s perception of care.
Journal of Interprofessional Care, 17(3), 223–237.
McMahon, G. T., Gomes, H. E., Hohne, S. H., Hu, T. M., Levine, B. A., &
Conlin, P. R. (2005). Web-based care management in patients with poorly
controlled diabetes. Diabetes Care, 28(7), 1624–1629.
Meigs, J. B., Cagliero, E., Dubey, A., Murphy-Sheehy, P., Gildesgame, C.,
Chueth, H., et al. (2003). A controlled trial of web-based diabetes disease
management. Diabetes Care, 26(3), 750–757.
Miller, C. D., Barnes, C. S., Phillips, L. S., Ziemer, D. C., Gallina, D. L., Cook, C.
B., et al. (2003). Rapid HgA1c availability improves clinical decision-
making in an urban primary care clinic. Diabetes Care, 26(4),
1158–1163.
Obman-Strickland, P. A., Orzano, A. J., Hudson, S. V., Solberg, L. I., O’Malley,
D., Tallia, A. T., et al. (2008). Quality of diabetes care in family medicine
practices: Influence of nurse-practitioners and physician’s assistants. Annals
of Family Medicine, 6(1), 14–22.
O’Connor, P. J., Crain, A. L., Rush, W. A., Sperl-Hillen, J. M., Gutenkauf, J. J.,
& Duncan, J. E. (2005). Impact of an electronic medical record on diabetes
quality of care. Annals of Family Medicine, 3(4), 300–306.
Petersen, J. R., Finley, J. B., Okorodudu, A. O., Mohammad, A. A., Grady, J.
J., & Bajaj, M. (2007). Effect of point-of-care on maintenance of glycemic
control as measured by HgA1c. Diabetes Care, 30(3), 713–715.
Ralston, J. D., Carrell, D., Reid, R., Anderson, M., Moran, M., & Hereford, J.
(2007). Patient web services integrated with a shared medical record:
Patient use and satisfaction. Journal of the American Medical Informatics
Association, 14, 798–806.
Robert Wood Johnson Foundation. (2007). Improving chronic illness care.
Retrieved January 22, 2008, from Robert Wood Johnson Foundation Web
Site: http://www.improvingchroniccare.org/
Seminario, L. M., Drab, S. R., Gabbay, R. A., Gold, K., McLaughlin, S. (2008).
AADE position statement: Diabetes educators: Implementing the chronic
care model. The Diabetes Educatior, 34(3), 451–456.
Shojania, K. G., Ranji, S. R., McDonald, K. M., Grimshaw, J. M., Sundaram,
V., Rushakoff, R. J., et al. (2006). Effects of quality improvement strategies
for T2DM on glycemic control: A meta regression analysis. Journal of the
American Medical Association, 296(4), 427–440.
Trapani, G. A., Palermo, G. A., Ramacca, G. C., Palermo, F., Messina, M. C.,
Fulantelli, M., et al. (2008). Five-year impact of a continuous quality
improvement effort implemented by a network of diabetes outpatient
clinics. Diabetes Care, 31(1), 57–62.
Wagner, E. H., Austin, B. T., Davis, C., Hindmarsh, M., Schaefer, J., & Bonomi,
A. (2001). Improving chronic illness care: Translating evidence into action.
Helath Affairs, 20(6), 64–78.
Weinger, K. (2003). Group medical appointments in diabetes care: Is there a
future? Diabetes Spectrum, 16(2), 104–107.
Williams, G. C., McGregor, H., Zeldman, A., Freedman, Z. R., Deci, E. L., &
Elder, D. (2005). Promoting glycemic control through diabetes
self-management: Evaluating a patient activation intervention. Patient
Education and Counseling, 56, 28–34.
Zrebiec, J. F. (2008). Internet communities: Do they improve coping with
diabetes? The Diabetes Educator, 31(6), 825–828.
585