Embed Size (px)
Citation preview
Ciran Rehabilitation,
Agali Mert ([email protected])
Alexander Garschagen
Improving health experience and RTW in patients with chronic pain
and fatigue: clinical effectiveness of bio-psycho-social-spiritual
rehabilitation.

CIRAN• CIRAN: Outpatient Centres for Integrated Rehabilitation and Occupational Activation
with multi-specialist care (The Netherlands).
• Is a foundation
• 5500 patients per year
• 19 out-patient facilities
• 500 employees, 4 physiatrists (of which two retired colonels )
• 7000 teleconferences per year
• Paper free environment

Ciran continued• 40% coverage of outpatient rehabilitation in The Netherlands
– Focus on chronic pain, fatigue, dysfunctioning, oncology, endocrinological problems
• Academic partner of Radboud University Nijmegen
• Rolling out serious gaming– LAKA: serious game on coping strategies
– CAREN motion platform
• 2017 Social Robotics– Structured interviewing combining psychophysiological, visual, EPF data
• 2017 E-health– EPF data, teleconferences, AI-datamining
• Dutch DoD project: spiritual leadership course

Ciran, 19 outpatient clinical facilities in the Netherlands

A few notes on the rehabilitation process

‐ Rehabilitation literally means “redressing” (Latin habitat – dress).
‐ To redress = to set right or repair.
‐ WHO has defined rehabilitation as:
“a process aimed at enabling disabled people to reach and maintain their optimal physical, sensory, intellectual, psychological and social functional levels. Rehabilitation provides disabled people with the tools they need to attain independence and self-determination.”
Rehabilitation

‐ The aim of Rehabilitation has traditionally been seen as facilitating the normalization of human functioning after injury, disease, or due to congenital defects. (bio-psycho-social)
Rehabilitation

The ability to transform oneself and others:
‐ by developing courage in order to better deal with uncertainty
‐ by the training of strength in overcoming adversity
‐ by increasing insight into the ever changing aspects of existence
‐ by striving for the happiness in oneself and others,
‐ by becoming convinced of positive outcomes and
‐ by living with confidence and energy in an open-minded and open-hearted way.
bio-psycho-social-spiritual rehabilitation.
Autonomy, mastery, purpose, solace,connection, meaning, pupose in midst of suffering

“Health is the individual art of reaching the personal, physical, mental and social balance again by being able to anticipate and react to events and
interactions in their own environment"
CIRAN’s definition of (positive) health
Other definitions: e.g. The ability to adapt and self manage, in the face of social, physical and emotional
challenges.
Positive health: covers a.o. autonomy, environmental mastery, personal growth, positive relations with others, having a purpose in life, and self-acceptance

Treatment frame- IT controlled
- e.g. Portals have to be finished before continuation of therapy is possible.
- Integral disciplinary treatment teams
- Psychologist also does physical sessions.
- Bio-Psycho-Socio-Spiritual
- Physiatrist, PT, PS and Spiritual counsellor
- Outcome-driven
- Highly protocolled
- 16 weeks (2x8) program, Treatment modules: neuroplasticity, Transformative dynamics, coping etc.
- appr. 10 hrs analysis prior to start treatment.
- Patients know their complete treatment program from day one on. They know what expect from
us, and they know what we expect from them.
- Therapists follow post-graduate mandatory training which they have to pass

Patient
Patient
Alleviating
pain and
fatique
Alleviating
pain and
fatiqueParticipation
Ciran perspective
Clinical perspective
Mediating and final objective Secondary objective
Mediating objective Final objective
Treatment strategy
Fordyce WE (1976). Behavioral Methods for Chronic Pain and Illness. Saint Louis. The C.V. Mosby Company,
Frank JD, Frank JB (1993). Persuasion and Healing. A Comparative Study of Psychotherapy Baltimore, The John Hopkins University Press.
Bellissimo, A, Tunks E (1984). Chronic Pain. The Psychotherapeutic Spectrum. New York Prager Publishers
Flor H, Turk DC (2011). Chronic pain: An Integrated Biobehavioral Approach. Seattle: IASP press.
Lebow JL (ed) (2008). Twenty-First Century Psychotherapies. Contemporary Approaches to Theory and Practice Hoboken, John Wiley and Sons
Participation

Input Process Outcome
Explanation Models:
Diagnostics & Treatment
Health Status:
- Pain and fatigue-Participation- Well-being
Patient Groups:
- Chronic pain - Chronic fatigue- Oncology
Diagnostics and treatment process (1)
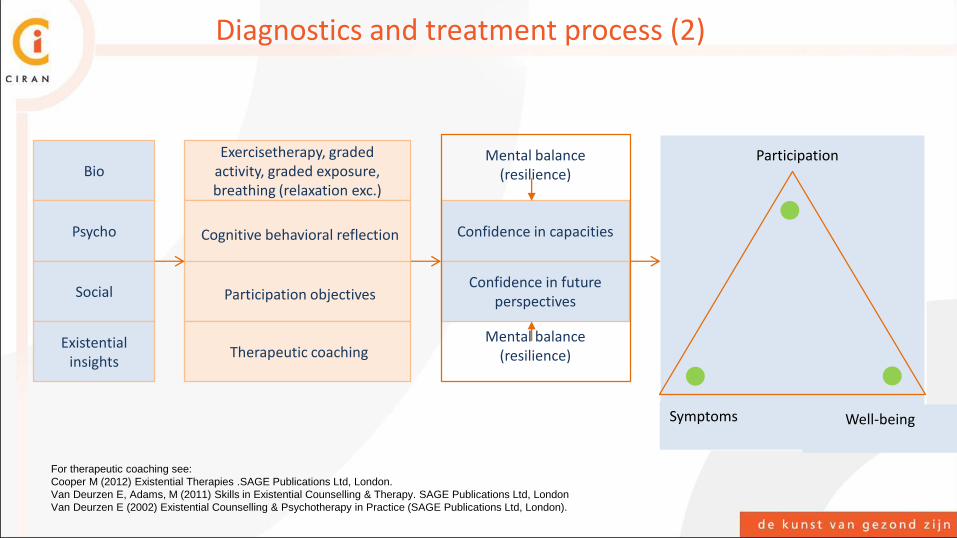
Bio
Psycho
Social
Existential insights
Exercisetherapy, graded activity, graded exposure, breathing (relaxation exc.)
Cognitive behavioral reflection
Participation objectives
Therapeutic coaching
Confidence in capacities
Confidence in future perspectives Zelf-
management
Participation
Symptoms Well-being
Mental balance (resilience)
Mental balance (resilience)
Diagnostics and treatment process (2)
For therapeutic coaching see:
Cooper M (2012) Existential Therapies .SAGE Publications Ltd, London.
Van Deurzen E, Adams, M (2011) Skills in Existential Counselling & Therapy. SAGE Publications Ltd, London
Van Deurzen E (2002) Existential Counselling & Psychotherapy in Practice (SAGE Publications Ltd, London).

Care needs index
Diagnostics and treatment process (3)

Unpredictable environment
Predictable environment
Social judgements infused with negative affect
Social judgements infused with positive affect
Mental balance Participation
P
S E
P
S E
P
S E
P
S E
S = SymptomsE = Existential well-beingP = Participation
What we hope to see
Emotions and cognitions
Dealing with
challenges and changes
Diagram adapted from:
Garschagen, A Steegers, M
Van Bergen A, Jochijms J,
Skrabanja T, Smeets R,
Vissers K:
Pain Pract. 2015
Sep;15(7):671-87
Kent M, River CT, Wrenn G:
Goal-Directed Resilience in
Training (GRIT): A
Biopsychosocial Model of Self-
Regulation, Executive
Functions, and Personal
Growth (Eudaimonia) in
Evocative Contexts of PTSD,
Obesity, and Chronic Pain
Behav. Sci. 2015, 5, 264-304

Results

Excluded from treatment: 1.226 (=14%)
Referred
clients
in 2013 - 2014:
8.889 (=100%)
Included in rehabilitation:
7.663 (=86%)
ITT
Stops duringtreatment:
1.266 (= 14%)
Completedtreatment:
6.397 (= 72%)
CT
Client flow
Completeness, accuracy and statistical analyses audited by Profess BV and Osinga Actuarial Consulting BV in commission of Radboudumc , January 2016
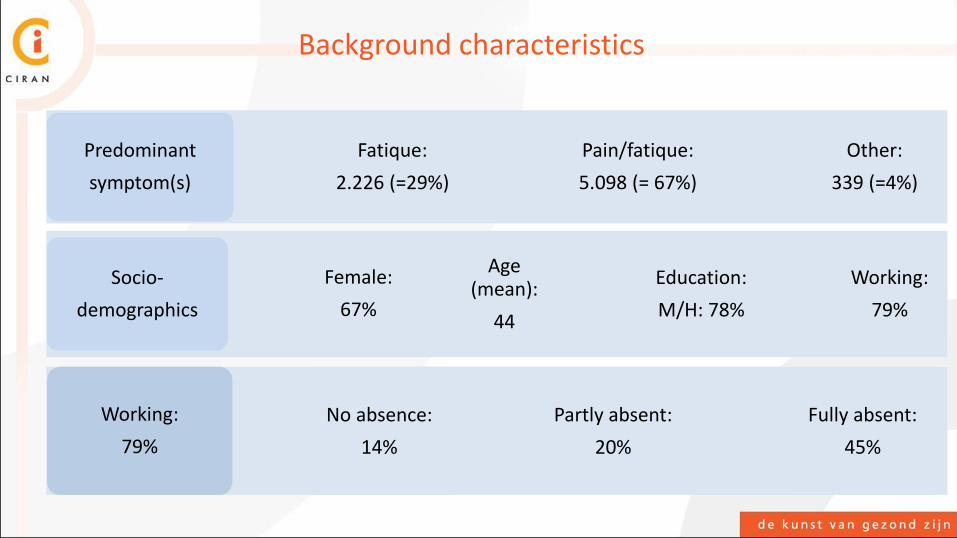
Predominant
symptom(s)
Fatique:
2.226 (=29%)
Pain/fatique:
5.098 (= 67%)
Other:
339 (=4%)
Socio-
demographics
Female:
67%
Age(mean):
44
Education:
M/H: 78%
Working:
79%
Working:
79%
No absence:
14%
Partly absent:
20%
Fully absent:
45%
Background characteristics
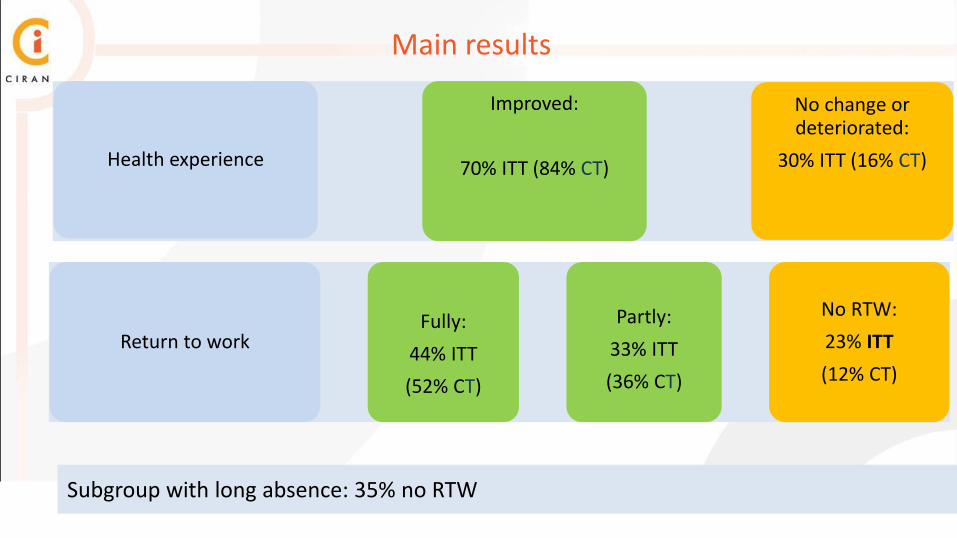
Health experience
Improved:
70% ITT (84% CT)
No change ordeteriorated:
30% ITT (16% CT)
Return to workFully:
44% ITT
(52% CT)
Partly:
33% ITT
(36% CT)
No RTW:
23% ITT
(12% CT)
Subgroup with long absence: 35% no RTW
Main results

1. 84% of clients who complete treatment improve
2. Large observational effect sizes in prolongued fatigue, pain intensity and pain cognitions (pre post standardized mean differences > 1)
3. Benefits of RTW instead of Qualys serve as operational indicator for cost-effectiveness. (Client: income. Employer: productivity and wages. Disability insurer: deferred payments. Health insurer: ?)
4. Important caveat: results measured directly post treatment
Summary
Schultz IZ, Stowell AW, Feuerstein M, Gatchel RJ. (2007), Models of return to work for musculoskelletal disorders. J Occup Rehabil. 2007 Jun;17(2):327-52.
Gatchel RJ, Okifuji A ( 2006). Evidence-Based Scientific Data Documenting the Treatment and Cost-Effectiveness of Comprehensive Pain Programs for Chronic Nonmalignant
Pain. The Journal of Pain, Vol 7, No 11 (November), 2006: pp 779-793
Thank you





























