Embed Size (px)
Citation preview

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 20
DOI: 10.14621/tna.20170103
Improving Hospital Performance in Kosovo: Rethinking Accessibility
Bardha Meka*1, Vlora Navakazi1, Elvida Pallaska2
1*Faculty of Civil Engineering and Architecture, University of Prishtina Bregu I Diellit, p.n., 10000 Prishtina, Kosovo; [email protected], [email protected]
2Institute for Spatial Planning Prishtina; Kosovo, [email protected]
Abstract Regional Hospitals in Kosovo are now ageing and becoming less easy to operate, still bothered with many insufficiencies. The large number of alterations and additions, which have taken place over the years, resulted in inefficient layouts with the lack of proper access, orientation and circulation. As a consequence of undifferentiated entrances, emergency departments are crowded. The intersection of paths between different users, both horizontally and vertically is evident, increasing the potential for cross infection. The aim of the study was to investigate this problem in regional hospitals in Kosovo and suggest solutions that comply with modern standards. The research consisted on methods for evaluating performance in use, where, in purpose of gathering all available information, the Post Occupancy Evaluation (POE) was performed. Analyses were based on indirect and direct modalities. In first case, knowledge and information was gained from scientific literature, while in direct phase, interviews and questionnaires were applied. Qualitative and quantitative analyses of systemized data resulted in recommendations for each critical point, which are a valuable tool for hospital planners, designers and decision – making process.
1. Introduction Considering patients expectation in health care, traditional relationships between patients and hospitals are changing fundamentally. A health service, even if careful and delivered through trained personnel, is devalued where the environments, rather than reflect, contradict any attention to the man [1]. In the preamble of the WHO is stated that Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity [2]. In this sense, it is not a matter of improving the performance of the existing system but the need to develop new models of care, where the patient is no longer regarded merely as a “product” being in hospital to get “fixed” [3]. By recognizing the inseparable link between man and built environment, the concept of humanization in designing of hospitals is being promoted. The building of the future hospital speaks a new language which we must learn the new semantics [4]. The paradigm shift towards patient-centered care becomes inevitable. The Planetree organization is often cited as having started the patient-centred care “revolution” witch philosophy is based on the self-empowerment of patients and an increased role of the experience of all the actors involved [5]. The development within the hospital sector in recent decades has gone from the pavilion hospital, via the block hospital, to the “neighbourhood hospital”, representing the hospital model of today [3]. Good example could be St. Olavs Hospital in Trondheim. It is a modern pavilion type and has a pronounced objective of a high degree of patient focus in the hospital development that brings nature, the city, employees and patients together in an unconventional way [6]. Pavilions seem that are being revived. They allow greater flexibility and versatility of use but also create greater accessibility by health professionals from outside the hospital and by members of the public [7]. They “have great potential in terms of open spaces to be used as roads, pedestrian areas and green spaces” [8].
Keywords: Regional hospitals; POE; Access; Orientation; Circulation
Article history: Received: 17 August 2016 Revised: 09 November 2016 Accepted: 03 February 2017

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 21
Hospitals in Kosovo are mainly pavilion type and are built within 60s and 80s. They are ageing now and becoming less easy to meet users' needs, despite some ad hoc renovations. The aim of the study was to gather relevant information regarding regional hospitals in Kosovo, particularly in Peja, to present problems in terms of accessibility, circulation and orientation in outdoor spaces and inside the buildings and to provide recommendations for optimal solution.
The research consisted on methods for evaluating of hospital performance in use, where, in purpose of gathering all available information, the Post Occupancy Evaluation (POE) was performed. Analyses were based on indirect and direct modalities. The first phase involves a literature review related to accessibility and people circulation requirements, while direct phase included field analyses, a walk-through to the complex, photographs, interviews and questionnaire with different types of users (patient, visitor and staff). Analyses of systemized data resulted in recommendations for each critical point, which are a valuable tool for hospital planners, designers and decision –making process.
2. Review of the situation of the regional
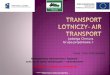
hospitals in Kosovo During 2007/2008, the implementation of secondary health care in Kosova was performed by five medical centers (regional hospitals) and two city hospitals. General hospitals in Prizren, Gjakova, Peja, Mitrovica, Gjilan, Vushtrri and Ferizaj are identified as regional and provide secondary care (Figure 1).
The dynamics of construction of regional hospitals of Kosovo lies in the period, starting from 1872 until nowadays. Number of floors varies from one to five. Total area of the ground floor of the whole hospital complex differs from min. surface 2570.00 m2, to the max. 13.333 m2 [9]. Regional hospital in Peja has the
greatest surface and it will be treated as a case study. Until now, no any long- term redevelopment strategy was implemented, “but rather the carrying out of spot interventions on the individual buildings of the hospital complexes” [8]. All hospital facilities in Kosovo initially were built on the outskirts of cities which later became part of it and are accessed from local streets.
2.1. Access to secondary care services
In terms of access to care, according to Kosovo Health Master Plan 2008 (KHMP), healthcare facilities in Kosovo are generally well located throughout the country. Over 88% of the population has access currently with 45 minutes (Figure 2 and 3). In many countries health systems are arranged to ensure that around 85% of people have access to acute hospital care within 60 minutes. However local road conditions vary and the mode of transport may also vary from patient to patient, so inevitably there is some inherent inaccuracy in this approach. The real access times in the more remote areas may in reality be 2-3 times that indicated on the GIS maps [10]. Access times in various countries vary widely depending on many factors among others, location of the hospital complex, physical access, entries, way findings and circulation are crucial.
2.2. Position of the regional hospitals in
relation to the surrounding urban roads There were identified cases where hospital complex is surrounded on all sides by urban roads (Prizren), on three sides (Gjilan), while others are spread along the road (Peja and Gjakova). First two cases create more alternatives to access the location, while in other two cases access is limited and can create obstacles for the transport of specific target groups of users (Figure 4). There was no “compact” typology encountered, mainly, they belong to the "spread" typology, accommodated into more buildings.
Figure 1. Map of regional hospital Figure 2. Network of health Figure 3. Access time at buildings in Kosovo services national level

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 22
A. The hospital complex in Prizren is
surrounded on four sides by urban roads
B. Hospital complexes in Peja (a) and Gjakova (b) are spread along the urban road
Figure 4. Position of the regional hospitals in relation to the surrounding urban roads
Figure 5. Regional hospital in Peja and municipialities Figure 6. Access time to regional as a part of the region of Peja hospital in Peja
3. Analyses of the accessibility.
Case study: Regional hospital in Peja Regional hospital in Peja has the greatest surface and it will be treated as a case study. The region of Peja covers the western and north-western part of Kosova, located on the valley of Dukagjini, along the border with The Cursed Mountain (Bjeshkët e Nemuna). Municipalities within the area are: Peja, Istog and Klina (Figure 5).
Catchment area to the regional hospital in Peja consists of 53% of users from the city of Peja, while 15,4% are from Istog, 13,8% from Klina, 12% from Decan, and the rest from other neighbour areas. The figure 6 shows that the maximum travel time to the hospital is 40 min, and
this depends, as mentioned above, from the local road conditions and the mode of transport.
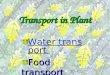
Regional hospital in Peja belongs to the secondary care level. It is located in the western part of the city, approximately 2,5 km from the city Centre. There are 27 wards and units, 433 beds, 11 outpatient clinics and seven diagnostic services, covering five cities with 400,000 inhabitants. Regional hospital in Peja is identified as a type where the hospital complex is spread along a single urban road. Building shapes are of “T type” and “H type”. Main access for pedestrian and vehicles is from the main road, on the southern side of the complex. This entrance is used for all categories of users, including patients, visitors, stuff and ambulance (Figure 7).
D. Hospital complex in Gjilan is
surrounded on three sides by urban roads
C. Access to the hospital in Mitrovica is
through the internal urban road

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 23
Study attempted to identify problems and most critical points based on outcome from the measurements, a walk-through to the complex, photographs, interviews and questionnaire performed on different user experiences. Questions applied were related to accessibility, circulation and way finding from the city to the hospital lot, in outdoor and indoor spaces of the hospital complex.
There are no signs until you get very close to the hospital location. First time visitors coming by foot or by car will spend more time to reach the destination because of asking people for direction. While for those who are willing to use public transport, there is no bus line provided.
Because public transport companies do not provide any bus transport, 50% of users travel by car to the hospital, then 30% on foot and 20% by taxi. One third of users came by foot, most of them are neighbour residents (Figure 8a). How users find the hospital location from the city, 80% claimed that they have been before, while from 20% which visited the site for the first time, 66% were orientated by signs which appear very close to the hospital complex and by asking people (Figure 8b). Results on questions for user’s perception (patient/visitor) about hospital outdoor accessibility and orientation are presented by means of the diagram from Figures 9 and 10.
Figure 7. Regional hospital in Peja: Spatial layout, internal traffic and circulation routes
Figure 8. a) Transportmodalities to the hospital,
b) Question for patients and visitors for the
orientation to the hospital from the city
(a) (b)

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 24
Figure 9. Questions for patients and visitors Figure 10. Questions for patients and visitors about about hospital outdoor orientation hospital outdoor accessibility and orientation
Figure 11. Lack of sidewalks to the building entrances (emergency – left, surgical block – right)
Figure 12. Directional signs inside the hospital complex in Peja Although there is no sign, 67% of respondents consider that the site main entrance was easy identified. This is due to the fact that the hospital complex is spread along a single urban road and there is only one entrance for all users. Other two entrances are from the secondary road, on the northern part of the complex. One is dedicated for technical staff and sometimes auto-ambulance only, while the second one is for Pneumophtysiology department. None of site entrances is marked, nor differentiated for specific types of users. The main site entrance is entrance for all and is access controlled permanently. There is no info board and a
map at the main site entrance. External paths with regard to diversity of users are not differentiated. Pedestrian and vehicular roads are not clearly distinguished in some parts. Half of respondents confirmed lack of sidewalks mainly close to entrances (Figure 11).
Due to the lack of unmarked building entrances and due to the fact that there are more than one entry in the same building, 47% of first time users encountered difficulties to reach the destination. To reach the destination, beside the main site entrance, 27% of users who came by foot pass through the entrance dedicated

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 25
for Pneumophtysiology department only. Some shorter unofficial routs across grass are present and are used by a small number of users (20%), obviously by neighbourhood residents mostly as alternative. Because emergency entrance is acting as a main building entrance, 87% of users use it as a transit to other departments. Our research found that almost 33% of first time patients and visitors asked for directions when they were at the site. Most of the respondents (67%) think that there are not enough locational signs in comparison with directional signs (Figure 10). There is no map and directories on the site. Directional signs inside the complex are old and unattractive (Figure 12).
Although there is a directional sign in the hospital site for the emergency department and other departments, all users use the emergency path toward the emergency department.
This is because of its central position and its entrance in front of the building, while other department entrances (surgical and internal medicine block) are “hidden”, unmarked and behind the buildings. Emergency department, in absence of a main entrance, act as a substitution for it, serving as a first information point and reception desk (Figure 13).
Majority of the respondents (67%), first time users, found it difficult to find their destination once they enter the building, 97% of respondents are not satisfied with the position, number, visibility and legibility of directional signs inside the building. In some cases they were written by hand. There is no map, nor directory inside the buildings.
Only the emergency department entrance has a reception and a waiting area. After being registered, all users use same corridors to reach specific departments,
Figure 13. Schematic presentation of accessibility problems in regional hospital in Peja
Figure 14. Questions for patients and Figure 15. Questions to all users about visitors about hospital outdoor orientation parking places

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 26
Figure 16: Car park crowding at the entrance of the surgical block (left) and emergency department (right)
while vertically, the only stairs and elevator. Intersection of paths between different users, both horizontally and vertically is evident. In other departments, patients and visitors, mainly those who visited the hospital for the first time were disoriented (80%) and more than half (53%) had asked for directions (Figure 14).
Almost half of total number of users (40%) found difficulties somewhere to park. Staff stated that, especially in the summer season, due to increased flux, it becomes very crowded and hard to find a parking place. Results show that 93% of users claimed that there is no differentiation of parking places for different users. Majority, 83%, think that to get from the parking place to their destination does not take long time (Figure 15). The problem is that all intend to park in front of entrances of the buildings, especially in front of emergency department (Figure 16). This impedes the circulation of ambulance. Vehicular access to main entrances of other buildings is possible, but these areas are not organized as drop-off points.
Regarding architectural barriers, respondents were more satisfied with situation in outdoor spaces than inside the buildings. Among others, there are no parking signs for disabilities, neither sidewalks toward the emergency and outpatient clinic entrances, while inside the buildings there are no toilets for persons with disabilities. Furthermore, certain circulation difficulties are caused in the emergency department due to the insufficient width of the corridor where doors open outward. The corridor that links the emergency department to the surgical block is inclined and it creates difficulties in transportation of patients to other departments (Figure 17). It was observed that requirements for disabilities were respected in terms of providing ramps in front of each entrance.
According to staff respondents, users (patients/visitors) have difficulties to orient themselves within the hospital area and they claimed that they were asked for direction. Almost half of respondents confirmed a sufficient number of signs considered as legible. When
Figure 17: Circulation impediments in the emergency department; inclined corridor (top) and insufficient corridor width where doors open outward (bottom)

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 27
asked about the feeling that users got inside the hospital complex, people who visited the site for the first time felt confused. This is due to difficulties in finding the right entrances. Majority of them attempt to find something which is definitely missing: Main Entrance. Inside the building they experienced the same feeling of confusion.
Main critical points related to the issue of accessibility, orientation and circulations, identified through the survey by the use of Post Occupancy Evaluation appears at: emergency entrance, entrance to the surgical block, pathway dedicated to the auto ambulance and interdepartmental circulation (Figure 7).
4. Critical issues and considerations Study highlighted unsatisfying levels of accessibility, identified most critical points and suggested recommendations in which should be reflected on. There are no signs until you get very close to the hospital location. First time visitors coming by foot or by car will be late because of asking people for direction. While for those who are willing to use public transport, there is no bus line provided. Public transport should be implemented in order to reduce the number of users coming by car, which will obviously release parking places at the hospital site. Once a site has been identified, except an access control, site entrance is not marked, nor differentiated for specific types of users. In the wide menu of the criteria foreseen for entrances, the architecture of the site entrance is preferred to be clearly defined and differentiated for different types of access: emergencies, users and visitors, staff, technical/logistics. In order to identify a route to the building, people need to rely on the on- site information, such as a comprehensive info board and a site map, which should be placed next to the site entrance.
Being inside the hospital location, people need to find an appropriate parking area, preferably the nearest to their destination. Although there are several parking places provided in Peja hospital complex, parking problems are present. There is no differentiation of parking places for different users. Parking places should be allocated them near building entrances to prevent long walking and marked clearly. Particular attention should be given in determining parking places for disabled. Pedestrian and vehicular roads are not clearly distinguished in some parts. They should be clearly marked and separated, with priority being given to pedestrian routes. External paths in Peja, in terms of diversity of users are not differentiated. Reaching the specific department remains unclear since entrances to specific departments are not marked. All users use the emergency path toward the emergency department. This is because of its central position and because it is
acting as a reception point and waiting area, which other departments are lacking. Therefore, emergency department becomes crowded and creates problems in terms of intersection of paths between different users, both horizontally and vertically, increasing the potential for cross infection. In addition, lack of proper signs creates disorientation to first time patients and visitors and increases level of stress. There are only a few identified directional signs inside the building, partially in the right position. In some cases they are written by hand. While considering circulation system, special attention should be paid, among others, to separate different user’s paths and to control flow, to provide differentiation by highlighting, marking and defining building entrances, to separate the inpatient and outpatient circulation and to enable way finding for all users by providing proper signs. Through corridors, stairway and lifts, internal traffic for patients, staff, supplies and visitors should remain orderly, without excessive intersection of paths. Regarding architectural barriers, respondent were more satisfied with situation in outdoor spaces than inside the building. It was observed that requirements for disabilities were respected in terms of providing ramps in front of each entrance. Access to the built environment for people with disabilities is required as a civil right. The goal is to develop environments that best provide a barrier-free environment for the independence, convenience and safety of all people with disabilities. The principle of inclusion should be taken into consideration in developing holistic plan for future interventions.
5. Conclusion Kosovo Foundation for Open Society state that “the true meaning of the word ‘health’ has been forgotten in Kosovo”. Being healthy in Kosovo now, implies exactly the state of not suffering from a disease. The proposed solution means efforts that should be taken to make existing hospital complexes accessible and with good wayfinding attributes, to improve patient flow throughout the hospital, to mitigate emergency department crowding and related insufficiencies. To meet patient expectations, patient – centered care elements should be implemented. In this sense, radically “rethinking accessibility” in Kosovo recently, although looks limited, it is possible through collaboration and team work across disciplines, by increasing role of the experience of all the actors involved. By reflecting on recommendations of the study, actual hospital performance would be improved in terms of accessibility and will prevent or minimize stress and anxiety to staff, patients, visitors and to disabilities particularly.

International Journal of Contemporary Architecture ”The New ARCH“ Vol. 4, No. 1 (2017) ISSN 2198-7688 ___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ B. Meka, V. Navakazi, E. Pallaska: “Improving Hospital Performance in Kosovo: Rethinking Accessibility”, pp. 20–28 28
References [1] Spinelli F., L’umanizzazione degli spazi ospedalieri
in “Progettare per la Sanita” 96/2006, pp. 28-32.
[2] Jensø M., Haugen T., Usability of hospital buildings, is patient focus leading to usability in hospital building, in Combining Forces Advancing Facilities Management & Construction through Innovation Series, Kähkönen K., Sexton M (ed), pp.347-361.
[3] WHO. Preamble to the constitution of the World Health Organization as adopted by the International Health Conference. New York: 19–22 June, 1946; 1948; signed on 22 July 1946 by the representatives of 61 states (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948.
[4] Pellitteri, G., Belvedere, F., Characteristics of the hospital buildings: changes, processes and quality, Proceedings, ARCC/EAAE 2010 International Conference on Architectural Research, 23-26 June 2010, Washington DC USA.
[5] Malkin, J. Healing Environments as the Century Mark: The Quest for Optimal Patient Experiences. In C. Wagenaar (Ed.) The architecture of hospitals (pp. 258-265). Rotterdam: NAi Publishers, 2006.
[6] The Norwegian Centre for Design and Architecture, Case: St. Olavs Hospital Architecture,
http://doga.no/en/news/case-st-olavs-hospital-architecture
[7] Cole, J. Strategic Planning for Healthcare Facilities. In C. Wagenaar (Ed.) The architecture of hospitals (pp. 356-361). Rotterdam: NAi Publishers, 2006.
[8] Giofrè F. Barriers between hospital and city: seven Ita lian case studies, in Health spaces, Hospital outdoor environments, Giofrè F., Dukanovic Z. (ed), pp 238- 261.
[9] Meka B., Navakazi V., Pallaska E., Contribution to the History of Hospital Facilities Construction Basic Typology of the Regional Hospital Facilities in Kosovo, Proceeding Book 1, Proceedings of the 2nd ICAUD International Conference in Architecture and Urban Design, Epoka University, Tirana, Albania, 08-10 May 2014, Paper No. 205.
[10] Coper L., Parkes A., Current secondary care configuration, Kosovo Health Master Plan, Health System Network Master Plan – Executive Summary, October 2008, pp. 97-101
[11] Giofrè F. 2002. Innovazione nel progetto delle aree a elevata complessità tecnologica, in Baglioni A., Tartaglia R. (ed) Ergonomia e ospedale, il sole 24 ore Italia, pp. 52-56.
[12] Terranova F. (ed), Edilizia per la Sanità, 2005, UTET, Turin, pp. 83.