Embed Size (px)
Citation preview

Improving Patient Outcomes by Targeting the VEGF/VEGFR Axis
Wells Messersmith, MD, FACPProfessor
Director, Gastrointestinal Medical Oncology ProgramCo-Head, Division of Medical Oncology
Program co-Leader, Developmental TherapeuticsMay 2013

Conflict of Interest:
1. No employment, speaker’s bureaus, stock ownership, royalties, patents, etc
2. Data Safety Monitoring Board for Morphotek
3. Local PI of clinical trials by Genentech/Roche, GSK, AstraZeneca, EntreMed, Pfizer, Millenium, Bayer, Onconova, and NIH/CTEP.
Slides: S. Kopetz (MDACC), Chris Lieu (Colorado)
Outline/Objectives:
1. Introductiona. Angiogenesisb. Ongoing trials in GI cancers
2. Role of PlGF
3. Mechanisms of resistance
Angiogenesis

Angiogenesis Background- Observation that tumor growth can be accompanied by
increased vascularity was reported more than a century ago
- In 1939, Ide and colleagues first postulated the existence of a tumor-derived blood-vessel-growth stimulating factor
- In 1960s, experiments by Greenblatt and Shubik, and Ehrmann and Knoth, provided early evidence that tumor angiogenesis was mediated by diffusible factors produced by tumor cells
- In 1971, Folkman proposed that anti-angiogenesis might be an effective anticancer strategy
C. Lieu, Colorado

VEGF- VEGF family of growth factors and their receptor
tyrosine kinases mediate proangiogenic effects
- Normal endothelial cells engaged in angiogenesis express numerous VEGF receptors, but produce very little detectable VEGF
- Tumor cells express VEGF receptors and also produce VEGF (autocrine mechanisms)
- Classic signaling is via VEGF-A binding to VEGFR-2, stimulating the PI3K/Akt as well as Raf/MEK/MAPK pathways

VEGF Signaling
Kerbel R. N Engl J Med 2008;358:2039-2049
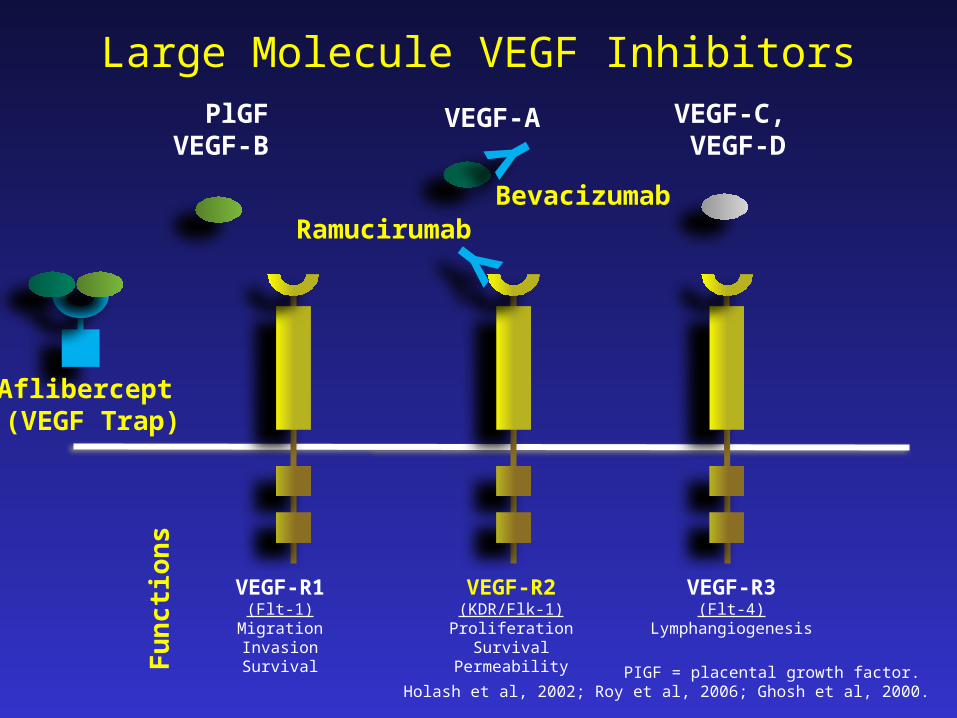
VEGF-A
VEGF-R1(Flt-1)
MigrationInvasionSurvival
VEGF-R3(Flt-4)
Lymphangiogenesis
VEGF-R2(KDR/Flk-1)Proliferation
SurvivalPermeability
PlGFVEGF-B
VEGF-C, VEGF-D
Fu
nct
ion
s
Y
BevacizumabYRamucirumab
Aflibercept (VEGF Trap)
PIGF = placental growth factor. Holash et al, 2002; Roy et al, 2006; Ghosh et al, 2000.
Large Molecule VEGF Inhibitors

Proposed Mechanism of Anti-Angiogenics
- Inhibition of new vessel growth and vascular regression
- Vascular normalization
- Vascular constriction
- Direct effects on tumor cell function
- Offsetting effects of chemotherapy inducing VEGF levels

ColorectalRecently reported:Regorafenib (“CORRECT”) – positiveAflibercept (“VELOUR”) – positiveBevacizumab 2nd line (“TML”) – positiveBrivinib (with cetux) – negative
OngoingRamucirumab (VEGFR-2 mAb; “RAISE”): NCT1183780
Phase III’s(selected anti-angiogenic agents)

Track Record of TKI’s in Colorectal
Total > 10,000Kopetz, MDACC

Track Record of TKI’s in ColorectalAgent FOLFOX
Irinotecan FOLFIRI
EGFRi + chemo
Other
Sunitinib Phase IIB Phase III Phase I/II
Vandetanib Phase IIB Phase IIB Phase I
Cediranib Phase II/III Phase IIB Phase I
Vatalanib Phase IIIs
Axitinib Phase IIB Bevacizumab
Semaxinib Phase III 5-FU, phase III
Motesanib Phase I Phase I Phase I
Sorafenib Phase IIB Phase IIB Phase I/II Bevacizumab
Pazopanib Phase I Phase I
Brivanib Phase I/II Cetux, Phase III
Regorafenib Phase II Phase II Phase III
Linifanib Phase IIB
Negative
Positive
Ongoing

Track Record of TKI’s in Colorectal
Kopetz, MDACC

Pancreas CancerGem +/- sorafenib “BYPAN” (NCT00541021) - negativeGem +/- bevacizumab (CALGB 80303) - negativeGem +/- Aflibercept (“VANILLA”) - negativeGem +/- axitinib (NCT00471146) – negative
Gastro-esophagealBevacizumab (“AVAGAST”) – negative (overall population)
Ramucirumab (VEGFR-2) vs BSC – positive
Pancreas Islet Cell / CarcinoidSunitinib (NCT00428597) – positiveBev vs Interferon, SWOG 0518 (NCT00569127)
Phase III’s(selected anti-angiogenic agents)

HCC1st LineSorafenib (“SHARP”) – positiveDoxorubicin/Sorafenib vs S, CALGB 80202 (NCT00917384)
Sorafenib vs brivanib (“BRISK FL”) – negative
Sorafenib vs sunitinib (NCT00699374) – negative
Sorafenib vs linifanib (ABT-869) (NCT01009593)
2nd LineBrivanib vs BSC (“BRISK PS”) (NCT 01217034) – terminated
Ramucirumab vs BSC (“REACH”) (NCT01140347)
Phase III’s(selected anti-angiogenic agents)

Outline/Objectives:
1. Introductiona. Angiogenesisb. Ongoing trials in GI cancers
2. Role of PlGF
3. Mechanisms of resistance
Angiogenesis

Role of Placenta Growth Factor- Angiogenic protein in VEGF family involved in cancer,
inflammation, pre-eclampsia, cardiovascular disease- Unlike VEGF, PlGF is undetectable in healthy tissues;
upregulated in tumors- Contributes to angiogenic and inflammatory “switch”- Produced by malignant cells, endothelial cells, smooth-
muscle cells, pericytes, cancer-associated fibroblasts, tumor-associated macrophages, and other stromal cells
- Serum PlGF is prognostic in colorectal cancer (Wei, 2009)
- Also prognostic in gastric cancer (Chen, 2004) and HCC (Ho, 2007)

Mechanism of Placenta Growth Factor
Loges et al, Clin Cas Res 2009. American Association for Cancer Research

Insights on PlGF- Four isoforms of PlGF in humans- PlGF transmits its own signal via VEGFR-1 (results is
phosphorylation of different residues than VEGF-A)- PlGF augments VEGF-A signaling by displacing it from
soluble VEGFR-1 (a negative regulatory mechanism), thereby increasing availability of VEGF-A
- PlGF also causes transphosphorylation of VEGFR-2- PlGF upregulates the expression of proangiogenic
molecules such as VEGF, FGF-2, and MMP-9- PlGF knock-out mice are healthy (unless challenged
with inflammation, cancer, etc)

Role of Placenta Growth Factor
Loges et al, Clin Cas Res 2009. American Association for Cancer Research

PlGF in bevacizumab resistance
Fan et al, British J Cancer. Cancer Research UK
- Colorectal cell lines that are chronically exposed to anti-VEGF-A therapy with bevacizumab show upregulation of compensatory pathways, including PlGF
- These “bev-adapted” cell lines are also more metastatic

PlGF and GI Toxicity
Hindryckx et al Lab Invest, ‘10, Fischer, Nat Rev Onc, ’08 ©
In chemically induced models of intestinal injury:Up to 6 fold increase in PlGF in the injured colon (minimal VEGF increase)In PlGF knockout mice (-/-), Substantial intestinal injuryHealing angiogenesis response is absentCan be rescued by PlGF
Increased weight loss and chronic intestinal injury
Wild-type
PlGFKnock-Out(severe injury)
S. Kopetz, MDACC
Outline/Objectives:
1. Introductiona. Angiogenesisb. Ongoing trials in GI cancers
2. Role of PlGF
3. Mechanisms of resistance
Angiogenesis

Resistance- Intrinsic Resistance
- Tumor cells can use existing blood vessels in vasculature-rich organs (lungs)
- Absence of VEGF or VEGF receptors in metastatic tumors
- Acquired Resistance- Induced pro-angiogenic factor substitution (FGF,
PlGF, etc)- Recruitment of bone marrow-derived cells to restore
neovascularization

Resistance Pathways
Numerous compensatory factors and cell typesEllis et al. Clin Cancer Res 2008;14:6371-6375

Preclinical Models of Resistance- Preclinical trials in a mouse model of pancreatic
neuroendocrine (islet cell) cancer, Rip1–Tag2
- Rip1–Tag2 mice were treated with a monoclonal antibody (DC101) that specifically blocked VEGFR signaling (in particular VEGFR2)
- Initial response denoted by tumor stasis and reductions in tumor vascularity
Casanovas et al. Cancer Cell 2005:8;299-309

Preclinical Models of Resistance- Response phase was transitory (10–14 days) and was
followed by tumor regrowth- Dense tumor vasculature restored
Casanovas et al. Cancer Cell 2005:8;299-309

Preclinical Models of ResistanceThe relapsing tumors were found to express higher levels of the mRNAs for the pro-angiogenic factors fibroblast growth factor 1 and 2
Tumor-derived cells subjected to hypoxic conditions similarly upregulated most of the genes
Casanovas et al. Cancer Cell 2005:8;299-309
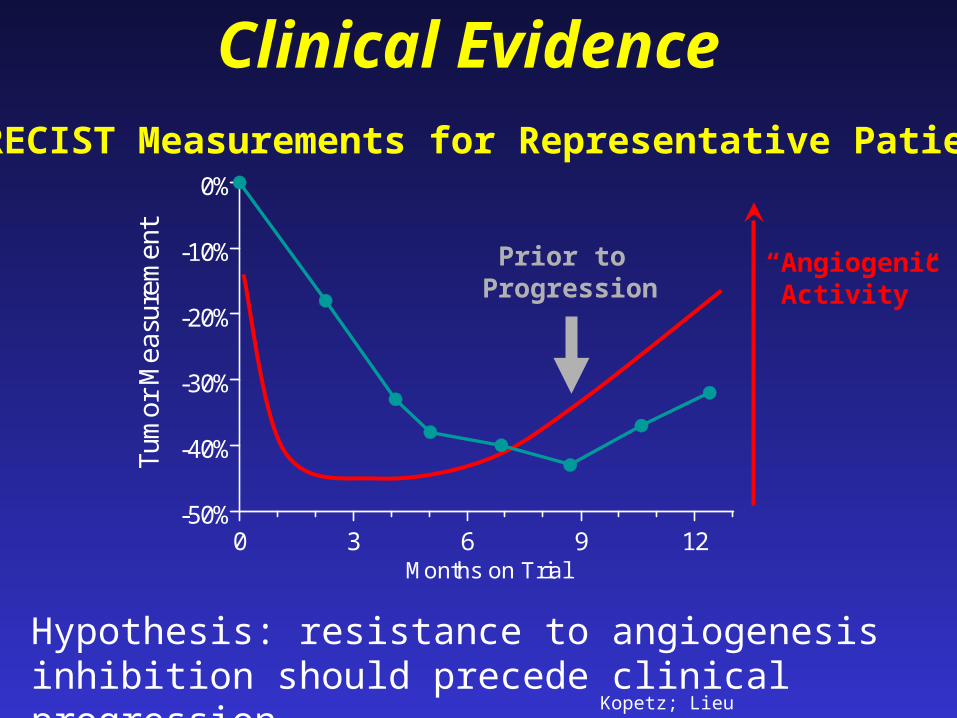
Clinical Evidence
Hypothesis: resistance to angiogenesis inhibition should precede clinical progression
Kopetz; Lieu
0 3 6 9 12-50%
-40%
-30%
-20%
-10%
0%
Months on Trial
Tum
or M
easu
rem
ent
Prior to Progression
RECIST Measurements for Representative Patient
“AngiogenicActivity”
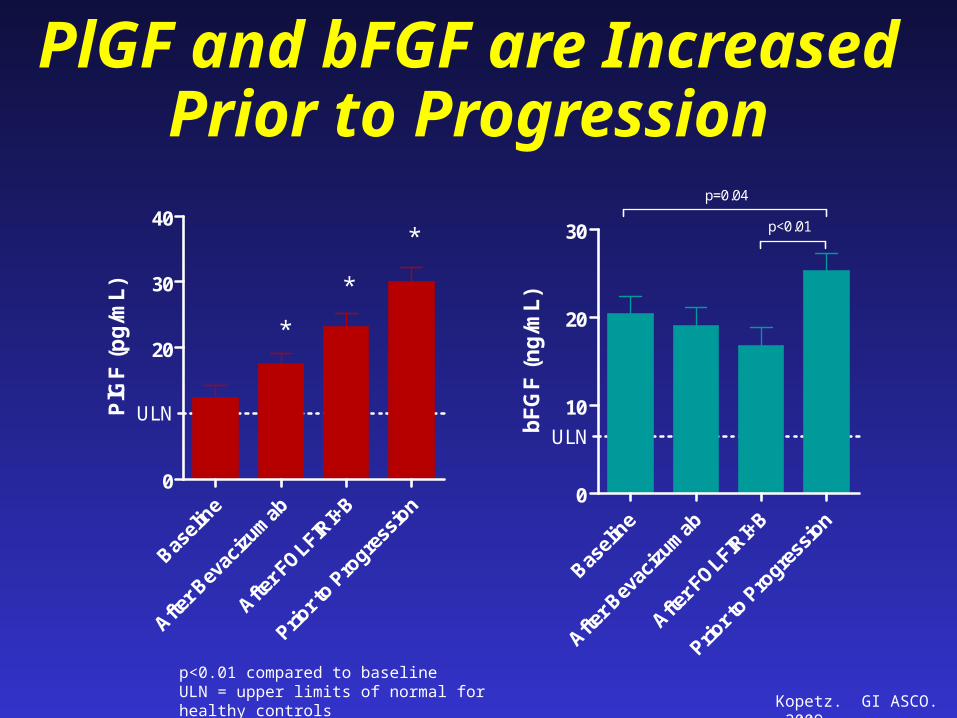
PlGF and bFGF are Increased Prior to Progression
Basel
ine
After B
evac
izum
ab
After F
OLFIRI+
B
Prior t
o Pro
gress
ion
0
20
30
40
ULN
*
*
*
PlG
F (
pg
/mL
)
Basel
ine
After B
evac
izum
ab
After F
OLFIRI+
B
Prior t
o Pro
gress
ion
0
10
20
30
ULN
p=0.04
p<0.01
bF
GF
(n
g/m
L)
p<0.01 compared to baselineULN = upper limits of normal for healthy controls
Kopetz. GI ASCO. 2009

Conclusion- Inhibition of angiogenesis results is modest but
meaningful benefit for multiple tumor types, including colorectal cancer.
- Dearth of biomarkers for who benefits; who is harmed; how resistance occurs
- VEGF-A has been the main focus, but the role other angiogenic signaling proteins (such as PlGF) under active study and drug development
- Overcoming resistance via multiple bypassing pathways may be challenging







![Role of targeted therapy in metastatic colorectal cancer · the VEGF family bind to three variants of receptors, VEGFR-1 (FLT-1), VEGFR-2 (FLK-1/KDR), and VEGFR-3 (FLT-4)[24,25]](https://img.pdfslide.net/doc/110x75/605c4af6a50bd930d55d2836/role-of-targeted-therapy-in-metastatic-colorectal-cancer-the-vegf-family-bind-to.jpg)






















