Embed Size (px)
Citation preview

Improving Treatment Success Rates for HCV in a Managed Care Setting
Bruce R. Bacon, MDJames F. King MD Endowed Chair in Gastroenterology
Professor of Internal MedicineDivision of Gastroenterology and Hepatology
Saint Louis University Liver CenterSaint Louis University School of MedicineSaint Louis University School of Medicine
St. Louis, MO
Faculty Disclosure
• The faculty reported the following financial relationships or y grelationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity: – Bruce R. Bacon, MD
• Consultant Fees: Schering Plough/Merck; Gilead Sciences; Three Rivers Pharmaceuticals; Valeant; Vertex; HumanThree Rivers Pharmaceuticals; Valeant; Vertex; Human Genome Sciences
• Fees for Non-CME Services Received Directly from a Commercial Interest or their Agents: Schering Plough/Merck; Gilead Sciences; Three Rivers Pharmaceuticals; Novartis; ISIS
• Contracted Research: Schering Plough/Merck; Roche Laboratories; Gilead Sciences; Bristol-Myers Squibb; Three Ri Ph ti l V l t V t H GRivers Pharmaceuticals; Valeant; Vertex; Human Genome Sciences; Wyeth; Romark Laboratories
Objective
• Assess the clinical challenges of managing patients g g g pwith hepatitis C virus (HCV) within a managed care setting

Agenda
• Status update: hepatitis C virus (HCV) in 2011p p ( )• Complications and mortality of chronic HCV• Effect of treatment on long-term morbidity and
mortality• Importance of adherence
Impact of new agents on HCV treatment in• Impact of new agents on HCV treatment in managed care
• Summaryy

HCV Status Update

Majority of Patients Infected With HCV Progress to Chronic DiseaseHCV Progress to Chronic Disease
Incubation Period: 14-180 Days Acutely Infected Persons14-180 Days
Average of 45 Days 20% to 30% Develop Symptoms
75% to 80% of Newly Infected Develop Chronic HCV Infections
60% to 70% of Those With Chronic HCV Infections Develop
Chronic Liver Disease
10% to 20% With Chronic Liver Disease Develop Cirrhosis Over
20 to 30 Years
Decompensated Cirrhosis5-year Survival Rate: 50%
4% Annual Death Rate
Hepatocellular Carcinoma:1-4% per Year
4% Annual Death RatePost-Cirrhosis
Chen SL, Morgan TR. Int J Med Sci. 2006;3:47-52. Seeff LB, et al. Hepatology. 2002;36(suppl):S35-S46.
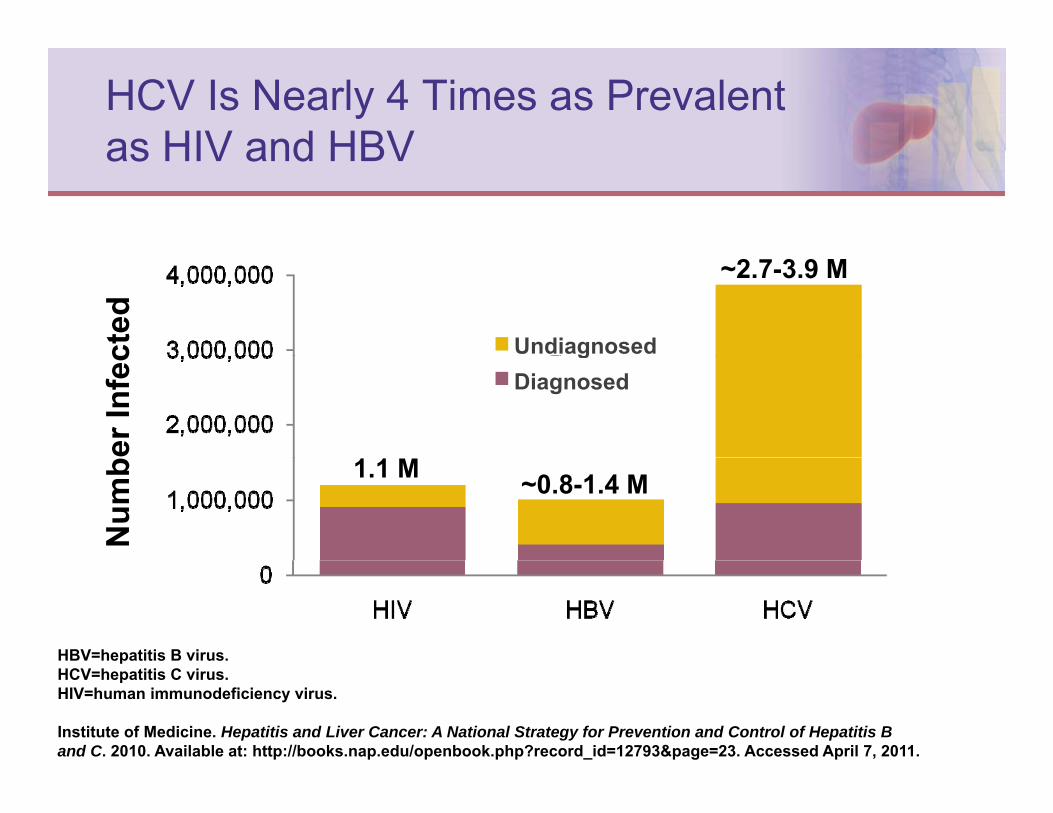
HCV Is Nearly 4 Times as Prevalent as HIV and HBVas HIV and HBV
cted
~2.7-3.9 M
Undiagnosed
er In
fec
Diagnosedg
Num
b 1.1 M ~0.8-1.4 M
HBV=hepatitis B virus.pHCV=hepatitis C virus.HIV=human immunodeficiency virus.
Institute of Medicine. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. 2010. Available at: http://books.nap.edu/openbook.php?record_id=12793&page=23. Accessed April 7, 2011.

Prevalence of Chronic Hepatitis C
• Global prevalence: ~170,000,000 cases p , ,• In the United States:
– 5 million exposed– 3.2 million chronically infected
• Only 25% of these are aware of their HCV status
Institute of Medicine. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. 2010. http://books.nap.edu/openbook.php?record_id=12793&page=23. Accessed April 7, 2011.

Majority of Those With Chronic HCV Are Baby BoomersAre Baby Boomers
Decade of BirthDecade of Birth
Milliman 2009. Consequences of hepatitis C virus (HCV): Costs of a baby boomer epidemic of liver disease. 2009. http://www.vrtx.com/assets/pdfs/Milliman_FactSheet.pdf. Accessed April 7, 2011.
C li ti d M t litComplications and Mortality of Chronic HCV

Cirrhosis Due to HCV Expected to Peak Over the Next DecadePeak Over the Next Decade
1,200,000
1,000,000ents
25%of patients with HCV currently
have cirrhosis, ,
800,000
600,000er o
f Pat
ie
400,000
200,000
Num
be 37%of patients with HCV are
projected to develop cirrhosis by 2020, peaking at 1 million
1990 2000 2010 2020 2030
Adapted from Davis GL, et al. Gastroenterology. 2010;138:513-521.
Year

Although a High Number of Men With Chronic HCV are Projected to Develop Cirrhosis….HCV are Projected to Develop Cirrhosis….
irrho
sis Years since infection
elop
ing
Cce
nt D
eve
Perc
Age at Infection (Years)
Davis GL, et al. Gastroenterology. 2010;138:513-521.

A Large Number of Women With Chronic HCV Are Projected to Develop Cirrhosis as WellAre Projected to Develop Cirrhosis as Well
Y i i f ti
Cirr
hosi
s Years since infection
velo
ping
Crc
ent D
ev
0.5%Per
Davis GL, et al. Gastroenterology. 2010;138:513-521.
Age at Infection (Years)

Complications of Cirrhosis Expected to Increase Over the Next Decadeto Increase Over the Next Decade
160,000140,000
s
120,000100,00080,000r o
f Cas
es
DecompensatedCirrhosis
,60,000
Num
ber
40,00020,000 Hepatocellular Cancer
Y
20,0000
1950 1960 1970 1980 1990 2000 2010 2020 2030
Davis GL, et al. Gastroenterology. 2010;138:513-521.
Year

Men With HCV Have a Greater Burden of Disease Than WomenBurden of Disease Than Women
• Men infected before age 50 show more rapid rates of progression, accounting for 74% of cirrhosis cases in 2009accounting for 74% of cirrhosis cases in 2009
• Women infected before age 50 show slower rates of progression and lower risk for developing chronic infection; only 16% had progressed to cirrhosis by 2009
1,200,000
sis
V >50Men (age at infection, years)
Cirrhosis Prevalence by Sex and Age at Initial HCV Diagnosis
1,000,000
800,000
600,000s of
Cirr
hos
With
HC
V
M
>5031-500-30
Women (age at infection, years)600,000
400,000
200,000
o. o
f Cas
esin
Pat
ient
s Men
Women
>5031-500-30
Davis GL, et al. Gastroenterology. 2010;138:513-521.
No
1950 1960 1970 1980 1990 2000 2010 2020 2030
Women

Failure to Achieve SVR Causes Worsening of Liver DiseaseWorsening of Liver Disease
e of
Firs
tm
e (%
)tiv
e R
ate
al O
utco
mC
umul
atC
linic
a
Ti (Y )
SVR=sustain virologic response.
Time (Years)
Morgan TR, et al. Hepatology. 2010;52:833-844.

Mortality Rate Due to HCV in People Over 35 YearsOver 35 Years
• 123% increase in HCV mortality rates between 1995 - 2004
Age
• Aging of the high prevalence birth cohort (1945 1964) may be reflected in
Year• Aging of the high prevalence birth cohort (1945-1964) may be reflected in
declining mortality seen in the 35-44 age group and an increase in mortality in the 45-64 age group
Wise M, et al. Hepatology. 2008;47:1128-1135.
Effect of Treatment on Long-term Morbidity and Mortalityy y

Why Treat Chronic Hepatitis C?
• The disease– HCV is common, chronic, and potentially progressive– Complications are becoming more common
• Liver failureLiver failure• Hepatocellular carcinoma (HCC)
• The treatmentVi l t i d i l i (SVR) i– Viral cure, or sustained virologic response (SVR), is achievable
– SVR associated with histologic improvement and gradual i f fib i 1regression of fibrosis1
– SVR leads to lower risk for liver failure and HCC, and improved survival2,3
1. Poynard T, et al. Gastroenterology. 2002;122:1303-1313.2. Craxi A, et al. Clin Liver Dis. 2005;9:329-346.3. Shiratori Y, et al. Ann Intern Med. 2005;142:105-114.

There Is a Need to Treat More Patients and to Achieve Improved Outcomesand to Achieve Improved Outcomes
• Disease burden is high and getting worseg g g• New therapies are becoming available• Must increase screening efforts to identify more
patients for treatment• Increased sustained virologic response (SVR) means
improved outcomeimproved outcome• Adherence leads to an improved SVR
McHutchinson JG, et al. Am J Manag Care. 2007;S327-S336.
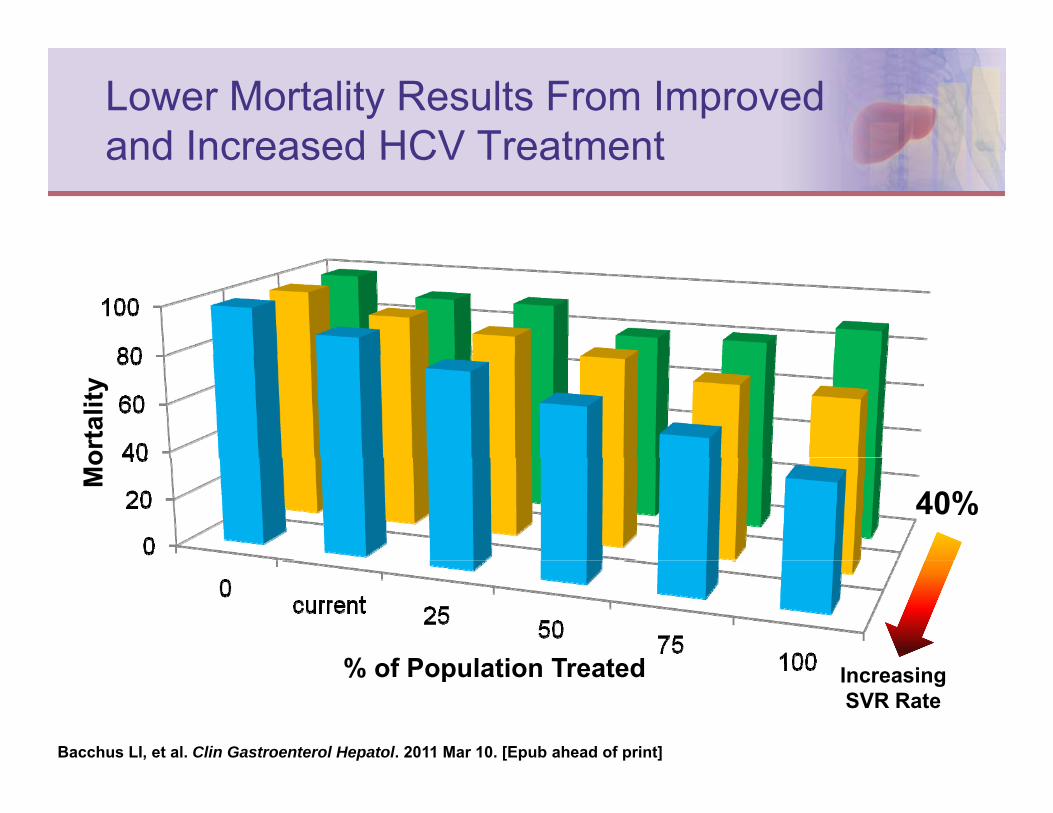
Lower Mortality Results From Improved and Increased HCV Treatmentand Increased HCV Treatment
orta
lity
40%
Mo
% of Pop lation Treated% of Population Treated IncreasingSVR Rate
Bacchus LI, et al. Clin Gastroenterol Hepatol. 2011 Mar 10. [Epub ahead of print]
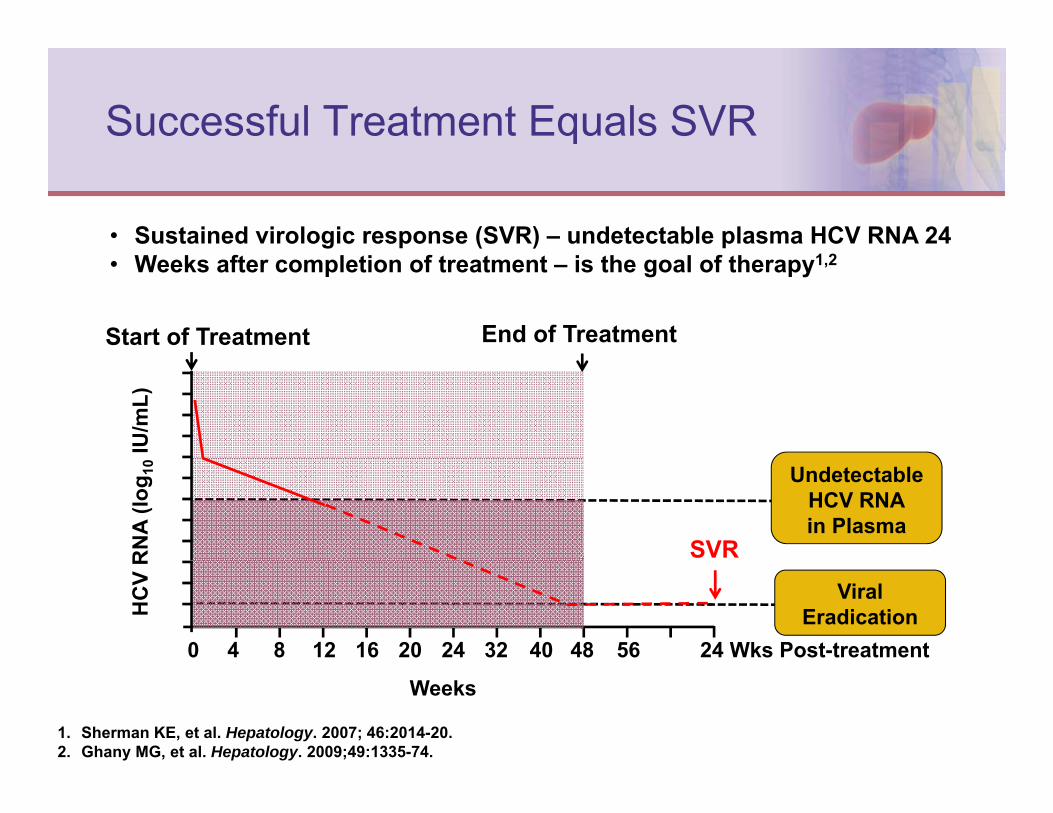
Successful Treatment Equals SVR
• Sustained virologic response (SVR) – undetectable plasma HCV RNA 24 • Weeks after completion of treatment – is the goal of therapy1,2
Start of Treatment End of Treatment
IU/m
L)R
NA
(log 1
0 UndetectableHCV RNAin Plasma
SVR
0 4 8 12 16 20 24 32 40 48 56 24 Wks Post-treatment
HC
V R
ViralEradication
1. Sherman KE, et al. Hepatology. 2007; 46:2014-20.2. Ghany MG, et al. Hepatology. 2009;49:1335-74.
Weeks
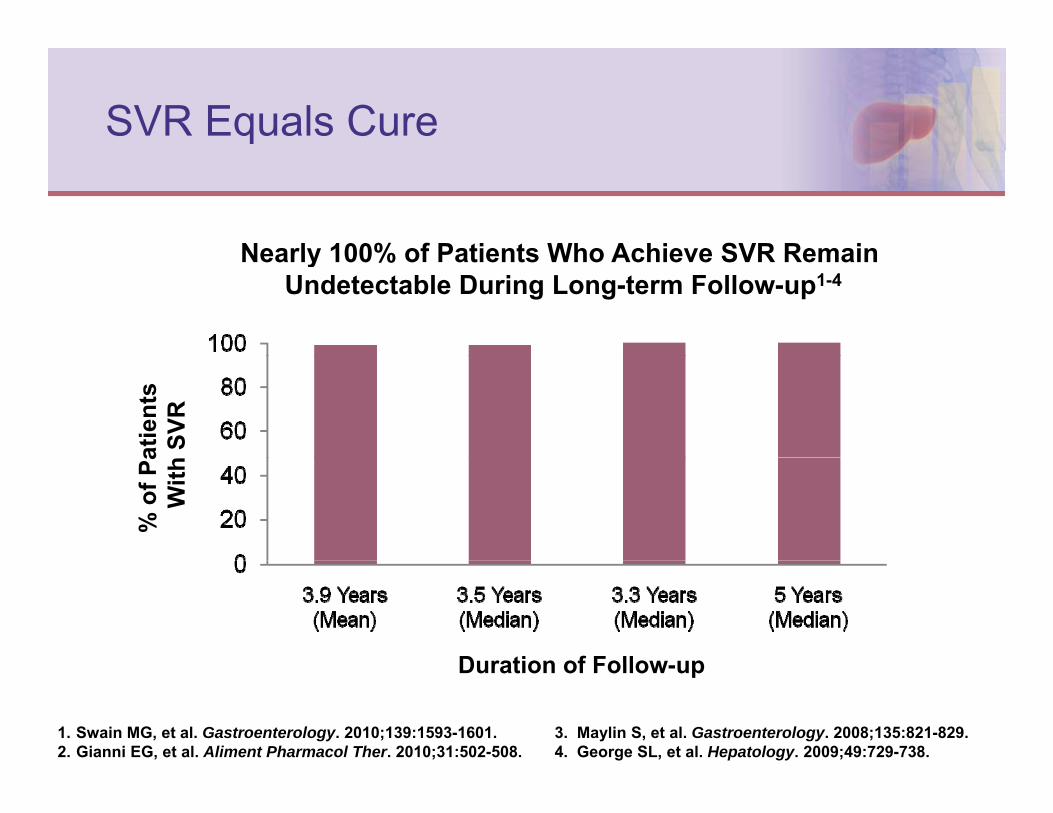
SVR Equals Cure
Nearly 100% of Patients Who Achieve SVR RemainNearly 100% of Patients Who Achieve SVR Remain Undetectable During Long-term Follow-up1-4
atie
nts
SVR
% o
f Pa
With
Duration of Follow upDuration of Follow-up
1. Swain MG, et al. Gastroenterology. 2010;139:1593-1601.2. Gianni EG, et al. Aliment Pharmacol Ther. 2010;31:502-508.
3. Maylin S, et al. Gastroenterology. 2008;135:821-829.4. George SL, et al. Hepatology. 2009;49:729-738.

Histologic Improvement After Successful Anti-HCV TherapySuccessful Anti-HCV Therapy
Long-term follow-up biopsyPretreatment biopsy: Long term, follow up biopsy obtained from the same patient 57
months after end of treatment:Trichrome stain with
Pretreatment biopsy: Trichrome stain with Ishak stage 3 fibrosis
(portal-to-portal bridging)Ishak stage 1 fibrosis
(p p g g)
George S, et al. Hepatology. 2009;49:729-738.
Patient Characteristics Predictive of SVRSVR
• Patients with these characteristics may have a higher y glikelihood of achieving SVR following treatment with pegylated-interferon and ribavirin:
Non African American race1 2– Non-African American race1,2
– Age <40 years1
– Lower body weight (≤75 kg)1,2y g ( g)– Absence of insulin resistance1,2
– Normal fasting glucose level2
P l hi i IL 28B 3– Polymorphism in IL-28B gene3
1. Ghany MG, et al. Hepatology. 2009;49:1335-1374.2. McHutchison JG, et al. N Engl J Med. 2009;361:580-593.3. Thompson AJ, et al. Gastroenterology. 2010;139:120-129.

Disease Characteristics Predictive of SVRSVR
• Patients with these disease characteristics may yhave a higher likelihood of achieving SVR with pegylated-interferon and ribavirin:
Non genotype 1 HCV1– Non-genotype 1-HCV1
– Low baseline viral load (≤600,000 IU/mL)1,2
– Absence of bridging fibrosis/cirrhosis1,2g g– Absence of steatosis2
– Elevated baseline ALT (3xULN)1
1. Ghany MG, et al. Hepatology. 2009;49:1335-1374.2. McHutchison JG, et al. N Engl J Med. 2009;361:580-593.3. Thompson AJ, et al. Gastroenterology. 2010;139:120-129.
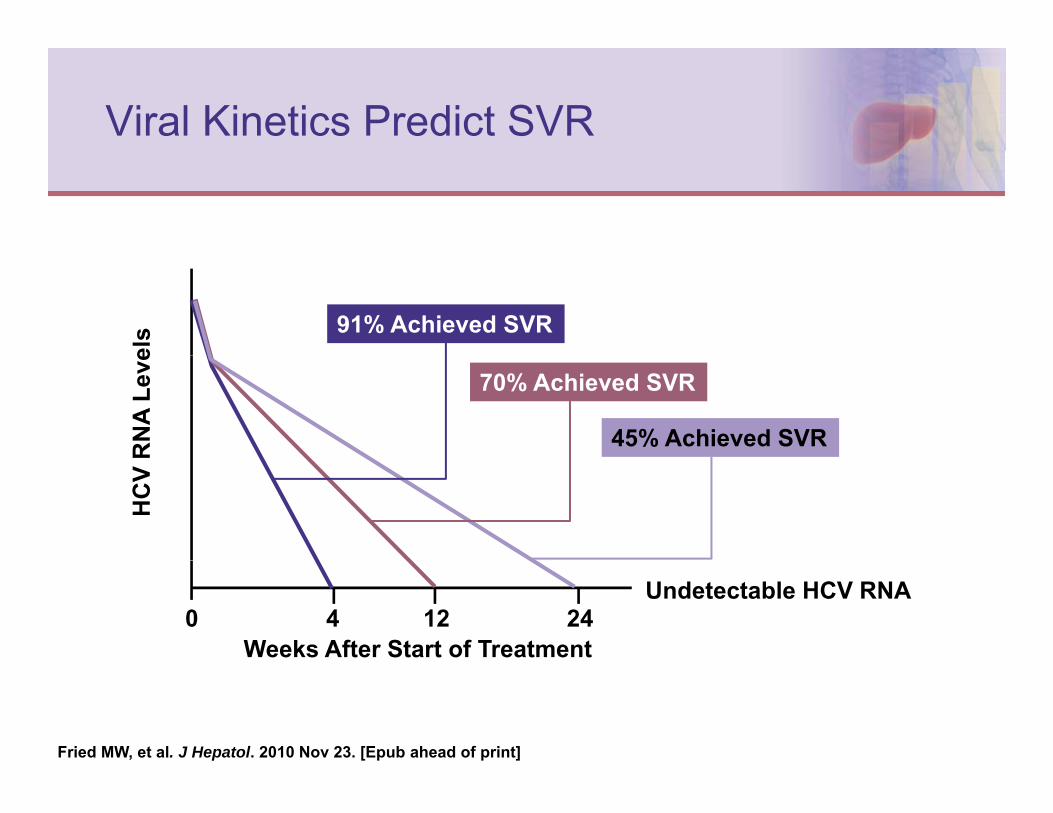
Viral Kinetics Predict SVRel
s 91% Achieved SVR
RN
A Le
ve 70% Achieved SVR
45% Achieved SVR
HC
V
0 4 12 24Undetectable HCV RNA
Weeks After Start of Treatment
Fried MW, et al. J Hepatol. 2010 Nov 23. [Epub ahead of print]

RVR Predicts SVRU
/mL)
NA
(log 1
0IU
91% of patients who reach undetectable HCV RNA at
HC
V R
N Week 4 achieved SVR
Undetectable HCV RNA in Plasma
24 WeeksPost-treatment
End ofTreatment
Week 4 ofTreatment
Start ofTreatment
RVR=rapid virologic response.
Fried MW, et al. J Hepatol. 2010 Nov 23. [Epub ahead of print]
Importance of Adherence to Treatment

Adherence to Therapy Is Critically Important to Improving OutcomesImportant to Improving Outcomes
Treatment Dosing
1Peg-interferon1 Q week
Ribavirin2 BID
Protease inhibitor• boceprevir3
t l i 4TID
Q8 h• teleprevir4 Q8 hours
1. Peginterferon alfa-2a Prescribing Information. Genentech, Inc. February 2011.2. Ribavirin prescribing information. http://www.drugs.com/pro/ribavirin.html. Accessed April 11, 2011.3. Bacon B, et al. N Engl J Med. 2011;364:1207-1217.4. Jacobson IM, et al. Presented at the 61st AASLD. Boston, MA. October 29-November 2, 2010. Abstract 211.

Self-reported Adherence to Treatment With Peg-IFN and RBVTreatment With Peg-IFN and RBV
)en
ts (
%Pa
ti
(n=369) (n=348) (n=327) (n=208) (n=170)
Smith SR, et al. Ann Pharmacother. 2007;41:1116-1123.
Weeks on Treatment

A Multidisciplinary Approach Is Required to Enhance Patient Adherenceto Enhance Patient Adherence
Educate and empower
patients about disease state
Anticipate and manage medication side effects
Id tif
disease state side effects
Increased adherence,
Identify financial and psychosocial
resources
Improve Dosing
Strategies ,which results
in effective treatment
resources
Gujral H, et al. Clev Clin J Med. 2004;71:S33-S37.

Impact of New Agents on HCV Treatment in Managed CareTreatment in Managed Care

HCV Treatment Continues to Evolve
Infergen10/97
Expected telepravirand boceprivir reviewSingle-source
Rib i i
Copegus12/02
2012P i t 2000 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
10/97
Rebetol6/98
Ribasphere4/04
Ribavirin1/03Pegasys
10/02PegIntron1/01
2012Prior to 2000 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009

Current and Emerging Therapies Will Be Combined to Increase SVRBe Combined to Increase SVR
• Newer agents such as the oral protease inhibitors are g pemerging
• However, treatment regimens will continue to rely on interferon and ribavirin (RBV) for at least another few yearsRegardless of the regimen patients must be adherent• Regardless of the regimen, patients must be adherent for efficacy and to prevent/limit resistance
Asselah T, Marcellin P. Liver Int. 201;(31 Suppl 1):68-77.

Ribavirin Is Critical to the Success of HCV Combination TherapyHCV Combination Therapy
• RBV will continue to play an important role in p y psuccessful antiviral therapy– Antiviral and immunomodulatory activity
R d d lik lih d f l– Reduced likelihood of relapse• Can we optimize treatment by fine tuning the use
of RBV?of RBV? – How important is the initial dose of RBV?– Do we need to maintain the RBV dose for the duration
f t t t?of treatment?
Dusheiko G, et al. Antivir Ther. 2008;13(suppl 1):23-30.

Cumulative RBV Exposure >60% of the Initially-assigned Dose>60% of the Initially-assigned Dose
Treatment Weeks 0-12 vs Weeks 0-48
Sulkowski M, et al. J Hepatol. 2008; 48:S370.Sulkowski M, et al. Gastroenterol. 2010; 139:1602-1611.

Milestones in IFN-based HCV Therapy
RBV in Combination With Interferon-
50
602000s
Led to Marked Improvements in SVR Rate*
30
40
VR (%
)
1990s
10
20SV
1990s
0IFNα-2b+RBV
24 wksPegIFNα-2b
+ RBV 48 wksIFNα-2b24 wks
PegIFNα-2a 48 wks
IFNa-2b=interferon alpha-2b. RBV=ribavirin.IFNa 2b interferon alpha 2b.PegIFNa-2a=peglyated interferon alpha-2a.
RBV ribavirin.SVR=sustained virologic response.
Hayashi N, et al. J Gastroenterol. 2006;41:17-27.
*In patients infected with HCV genotype 1, high viral load.

Reduction of RBV Dose Associated With Stepwise Increase in Relapse Rate
M RBV D Si ifi tl
Stepwise Increase in Relapse Rate
Mean RBV Dose Significantly Correlated With Relapse (P<.0001)
se (%
)R
elap
s
Mean RBV Dose (mg/kg/d)
Hiramatsu N, et al. J Vir Hepat. 2009;16:586-594.
Mean RBV Dose (mg/kg/d)

RBV Is Critical for Protease Inhibitor Combination Therapy
100
Combination Therapy
PROVE-21 PROVE-32
)
80 SPRINT-13
67
SVR
(%)
40
60
24%29%
31%67
5360
2036 36
24
0T12PR12
(n=82)T24PR48
(n=13)T24P24(n=111)
T12P12(n=78)
PBR48 (n=103)
PBLowR48 (n=59)
= Telaprevir + Peg-Interferon + RibavirinPROVE=Protease Inhibition for Viral Evaluation
1. Hezode C, et al. N Engl J Med. 2009;360:1839-1850.2. McHutchison JG, et al. N Engl J Med. 2010;362:1292-1303. 3. Kwo P, et al. Lancet. 2010; 376:705-716.
Telaprevir Peg Interferon Ribavirin= Telaprevir + Peg-Interferon = Boceprevir + Peg-Interferon + Ribavirin= Boceprevir + Peg-Interferon + Low-dose
Ribavirin (400mg-1000mg/d)
PROVE=Protease Inhibition for Viral Evaluation.SPRINT=Serine Protease Inhibitor Therapy.

Impact of Newer Agents on HCV Treatment in Managed CareTreatment in Managed Care
• Approval of new agents such as the oral protease pp g pinhibitors will require HCV treatment guidelines to be updated
New guidelines will require managed care reimbursement– New guidelines will require managed care reimbursement algorithms to be created to define eligibility criteria
• Stakeholders should work to reduce the lag following approval of these new agents, the revision HCV practice guidelines, and subsequent managed care reimbursement guidancereimbursement guidance
McHutchinson JG, et al. Am J Manag Care. 2007;S327-S336.
Summary

Summary
• Prevalence of HCV increasing g• Disease burden can be reduced through better patient
identification and treatment designed to increase SVR• Increased SVR equals improved outcomes• Adherence is critical for increasing SVR
Regimens that combine ribavirin with a protease• Regimens that combine ribavirin with a protease inhibitor improve SVR
• Availability of new agents will require treatment y g qguidelines and managed care reimbursement algorithms to be revised
![Elizabeth Sherman, PharmD, AAHIVPhivaidsinstitute.med.miami.edu/documents/...HIV-HCV...• SVR rates similar to HCV monoinfected [1,2] • In HCV/HIV coinfection, treat HCV as though](https://img.pdfslide.net/doc/110x75/5fbc30e57653e03e261e9924/elizabeth-sherman-pharmd-aa-a-svr-rates-similar-to-hcv-monoinfected-12.jpg)