Embed Size (px)
Citation preview

Immunity, Vol. 14, 105–110, February, 2001, Copyright 2001 by Cell Press
Contrasting Roles of IL-2 and IL-15 Minireviewin the Life and Death of Lymphocytes:Implications for Immunotherapy
nological memory to foreign pathogens, have significantimplications for the development of rational receptor-directed therapeutic approaches that focus on the IL-2/IL-2R or, alternatively, the IL-15/IL-15 R systems.IL-2 and IL-15 in the Life and Death of Lymphocytes
Thomas A. Waldmann,* Sigrid Dubois,and Yutaka TagayaMetabolism BranchNational Cancer InstituteNational Institutes of Health
The immune system is dedicated toward a series ofBethesda, Maryland 20892goals, including (1) the generation of rapid innate (e.g.,NK cell) and adaptive (e.g., antibody and T cell) re-sponses to invading pathogens, (2) the maintenance of
Although IL-2 and IL-15 share two receptor subunits a specific memory response to these pathogens, andand many functions, especially in innate immunity, at (3) the elimination of autoreactive T cells to yield toler-times they provide distinct and contrasting contri- ance to self. Such immune responses are regulated bybutions to T cell–mediated immune responses. IL-2, a series of cytokines that exhibit a high degree of redun-through its pivotal role in activation-induced cell death dancy and pleiotropy. For the IL-2 family of cytokines(AICD), is involved in peripheral tolerance through the that includes IL-2 and IL-15, this redundancy is ex-elimination of self-reactive T cells. In contrast, in general plained by the sharing of common receptor subunits.IL-15 manifests antiapoptotic actions and inhibits IL-2- The common g chain (gc) is shared by IL-2, IL-4, IL-7,mediated AICD and stimulates persistence of memory IL-9, and IL-15 (Lin et al., 1995). IL-2 and IL-15 also sharephenotype CD81 T cells. Humanized monoclonal anti- the IL-2Rb subunit (Bamford et al., 1994; Grabstein etbodies that recognize IL-2Ra, the private receptor for al., 1994). Finally, the high-affinity forms of the IL-2 andIL-2, are being employed to inhibit allograft rejection and IL-15 receptors also involve the private receptor sub-to treat T cell leukemia/lymphoma. Therapies directed units, IL-2Ra and IL-15Ra, respectively (Waldmann,toward inhibiting the actions of the inflammatory cyto- 1991; Giri et al., 1995). As a consequence of their sharingkine, IL-15, have been proposed for an array of autoim- of the receptor elements IL-2Rb and gc and their usemune disorders as well as diseases associated with the of common Jak/STAT signaling elements, IL-2 and IL-retrovirus HTLV-I. 15 also share a number of functions including the stimu-
A major advance in receptor-directed therapy for lation of the proliferation of activated CD42, CD82,many human diseases using monoclonal antibodies was CD4181, CD41, CD81, and gd subsets of T cellsthe definition of new cell surface structures as targets (Grabstein et al., 1994; Waldmann and Tagaya, 1999).for more effective mAb action. One such target for more Furthermore, the two cytokines facilitate the inductionspecific immune suppression in transplantation, autoim- of cytolytic effector T cells including CTL and LAK cellsmunity, and T cell leukemia is the high-affinity IL-2 re- and induce the proliferation and immunoglobulin syn-ceptor, since its expression marks a critical step in the thesis by B cells stimulated by anti-IgM or CD40 ligandactivation of T cells. The scientific basis for the choice (Armitage et al., 1995). They also stimulate the genera-of this target is that resting normal cells do not express tion, proliferation, and activation of NK cells. In additionIL-2Ra, whereas this receptor subunit is expressed by to these shared functions there are, however, distincta proportion of the cells involved in allograft rejection, differences between IL-2 and IL-15 that are especiallythose participating in select autoimmune diseases, and critical in the homeostasis of adaptive immune re-by the abnormal cells in certain lymphoid neoplasias sponses.(Waldmann, 1991). Distinct Actions of IL-2 and IL-15 in AICD and in the
In part as an outgrowth of IL-2R-directed therapeutic Survival of Memory Phenotype CD81 T Cellstrials, two groups simultaneously reported the identifica- Recent ex vivo functional analyses as well as studies
using transgenic mice and those genetically lacking IL-2,tion of a T- and NK-stimulating cytokine, IL-15 (BurtonIL-15, or their specific receptors have been of particularet al., 1994; Grabstein et al., 1994). In T cells, the IL-15value in the definition of the distinct roles played by IL-receptor includes IL-2Rb and gc subunits shared with2 and IL-15 (Sadlack et al., 1994; Willerford et al., 1995;IL-2 (Bamford et al., 1994; Grabstein et al., 1994), asLodolce et al., 1998; Kennedy et al., 2000) (Figure 1).well as an IL-15- specific receptor, IL-15Ra (Giri et al.,Although IL-2 is an important growth and survival factor,1995). As might be anticipated from their sharing of theit also plays a pivotal role in Fas-mediated AICD of CD4IL-2Rb and gc subunits, IL-15 and IL-2 share a numberT cells (Lenardo, 1996; Refaeli et al., 1998; Van Parijs etof biological activities. However, especially in adaptiveal., 1999). Receptor-mediated stimulation of CD4 T cellsimmune responses, they also provide distinct, at timesby antigen at high concentrations induces the expres-competing, contributions to the life and death of lym-sion of IL-2 and the IL-2 receptor that in turn interact tophocytes involved in the immune response (DiSanto,yield T cell activation and cycling. Antigen restimulation1997; Ku et al., 2000; Marks-Konczalik et al., 2000; Mar-of the cycling T cell at this stage through the T cellrack et al., 2000). These distinct roles for IL-2 and IL-15antigen receptor increases the transcription and surfacein the survival of lymphocytes, including those that areexpression of the death effector molecule Fas ligandself-reactive as well as lymphocytes that maintain immu-(Fas L) and suppresses an inhibitor of Fas signaling FLIP(Refaeli et al., 1998). Activation of STAT 5 by IL-2 wasreported to be involved in T cell proliferation, the induc-* E-mail: [email protected].
Immunity106
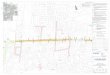
Figure 1. Diagrammatic Model Outlining theDistinct Roles Played by IL-2 and IL-15 in theLife and Death of T CellsIL-2 is required for AICD involved in peripheraltolerance to self-antigen whereas IL-15 inhib-its this process. In addition, IL-15 supportswhereas IL-2 inhibits the survival of memoryphenotype CD81 T cells.
tion of Fas L expression, and AICD, whereas T cell sur- et al., 2000) reported that the division of CD81 T cellsof memory phenotype is stimulated by IL-15 but is inhib-vival was dependent on an IL-2Rb region that is involved
in the activation of Akt and the expression of Bcl-2 (Van ited by IL-2.These conclusions derived from ex vivo functionalParijs et al., 1999). IL-15 in contrast acts to extend the
survival of lymphocytes by acting as a growth factor and studies are supported by an analysis of mice with dis-rupted cytokine and cytokine receptor genes as well asby inhibiting IL-2-mediated CD41 T cell AICD (Marks-
Konczalik et al., 2000). The mechanism underlying this transgenic mice. IL-22/2 and IL-2Ra2/2 null mice devel-oped massive enlargement of peripheral lymphoid or-inhibition of the AICD phemonenon has not been de-
fined. In ex vivo studies, CD41 T cells from IL-15 trans- gans associated with polyclonal T and B cell expansion,which for T cells was related to impaired ACID (Sadlackgenic mice did not manifest IL-2-induced AICD. Of inter-
est in these studies, there was the additional observation et al., 1994). The IL-2Ra-deficient mice developed auto-immune diseases including hemolytic anemia and in-that the inclusion of an anti-IL-15 antibody to the ex
vivo cultures resulted in the restoration of the ability of flammatory bowel disease (Willerford et al., 1995). Thisautoimmune phenotype observed in the IL-2R-deficientIL-2 to induce AICD of the CD41 T cells derived from
the IL-15 transgenic mice (Marks-Konczalik et al., 2000). mouse leads to a concern about the use of IL-2Ra-directed monoclonal antibodies for the treatment ofIn some cases, the anti–cell death action of IL-15 was
associated with the induction of a quiescent phenotype autoimmune diseases. In contrast to the phenotypeobserved with IL-2-deficient mice, mice geneticallycharacterized by the maintenance of the cells in the G0/
G1 phases of the cell cycle with downregulation of CD25 deficient in interleukin-15 (IL-152/2) did not manifestlymphoid enlargement, high immunoglobulin levels, orand CD95 expression (Dooms et al., 1998, 2000). How-
ever, in the presence of appropriate TCR engagement, autoimmune disease (Kennedy et al., 2000). Rather, theydisplayed a marked reduction in the numbers of thymicthe IL-15-induced quiescent cells were both resistant
to TCR-induced cell death and proliferated strongly in and peripheral natural killer (NK) cells, NK T cells, andintestinal intraepithelial lymphocytes (IELs). Further-response to IL-15. Thus, IL-15 may play a role in the
promotion of long-term maintenance of antigen-express- more, they manifested a marked reduction in memoryphenotype CD81 T cells. IL-15Ra-deficient (IL-15Ra2/2)ing CD41 T cells. In addition to its role in inhibiting the
AICD of CD41 cells, IL-15 has been reported to manifest mice also showed a profound defect in NK cells, TCRintraepithelial lymphocytes as well as memory pheno-an antiapoptotic action in a number of other lymphoid
systems; for example, it inhibited dexamethasone and type CD81 T cells that was associated with profoundgeneralized lymphocytopenia (Lodolce et al., 1998). Inanti-IgM-mediated apoptosis of activated B cells as well
as the spontaneous apoptosis of CD4 and CD8 cells in contrast, IL-15 transgenic mice manifested an inhibitionof IL-2-mediated AICD and an increased number of NKHIV-infected individuals by a mechanism involving Bcl-2
(Naora and Gougeon, 1999). cells and memory type CD81 cells (Marks-Konczalik etal., 2000). These mice were not reported to manifestIn addition to their actions in AICD, IL-2 and IL-15
play opposing roles in the control of the homeostasis of autoimmune disease. Taken together, these studiessupport the view that in their special adaptive immuneCD81 memory phenotype T cells. Zhang and coworkers
(Zhang et al., 1998) demonstrated that unlike IL-2, IL- functions IL-2 and IL-15 favor opposing actions thattend to emphasize one or the other of two competing15 provides potent and selective stimulation of memory-
phenotype (CD44hi) CD81 T cells in vivo. Furthermore, major goals of the immune response. IL-2 through itscontribution to AICD for CD4 cells and its interferenceKu, Marrack, and coworkers (Ku et al., 2000; Marrack

Minireview107
with the persistence of CD81 memory phenotype T cells addition, a second IL-15 binding and signaling pathwaythat does not share any subunits with the IL-2R systemfavors the elimination of select lymphocytes that are
directed toward self-antigens and thus plays a critical has been defined (Tagaya et al., 1996). This novel IL-15R system uses a signal transduction pathway distinctrole in the maintenance of peripheral self-tolerance. In
contrast, IL-15 through its inhibition of IL-2-mediated from that used by IL-2. Furthermore, IL-15 was shownto deliver a nonproliferative functional signal to colonicAICD and its role in the maintenance of CD81 memory
phenotype T cells favors the maintenance and survival cells in the absence of IL-2Rb (Stevens et al., 1997).However, it must be emphasized that this IL-15 receptor/of CD4 and CD8 T cells. The persistence of memory
phenotype CD81 T cells should be of value in main- signaling pathway has been demonstrated in mast cellsbut not as yet in T cells. Another distinction betweentaining a specific immune response to foreign patho-
gens. However, it carries with it the risk to the organism IL-2 and IL-15 is in their binding interactions with IL-2Rb. Antibodies directed toward this receptor subunitof the survival of autoreactive T cells that could lead to
the development of autoimmune diseases. Indeed, it such as Mikb1 block the functional effects of IL-15 butnot those of IL-2. More likely explanations for the distincthas been reported that IL-15 overexpression is associ-
ated with an array of inflammatory autoimmune dis- actions of IL-2 and IL-15 focus on the private cytokine-specific receptor elements IL-2Ra and IL-15Ra. It haseases. To circumvent this risk of autoimmune disease,
there is a multifaceted control of IL-15 expression been suggested that the response to the cytokines de-pends not only on the interactions of the subunits with(Grabstein et al., 1994; Bamford et al., 1996; Azimi et
al., 1998; Waldmann and Tagaya, 1999). In particular, in the ligand but also on the interactions among the threesubunits themselves. In this regard, the proximity of theaddition to control at the level of transcription IL-15 is
posttranscriptionally regulated by multiple controlling distinct subunits to IL-2Ra alters the conformation ofsignaling elements of the receptors in distinct ways,elements that impede translation, including 11–13 up-
stream AUGs in the different 59 UTR isoforms, two un- thereby altering the nature of the cytokine-mediated sig-nals transmitted to the nucleus. For example, we andusual signal peptides, and the C terminus of the mature
protein (Bamford et al., 1998; Waldmann and Tagaya, others demonstrated that the proximity of the IL-2Rasubunit changes the function of the IL-2Rb subunit to1999). The variety of negative regulatory elements con-
trolling IL-15 expression may be required because of alter IL-2 binding and signaling by mechanisms that donot require binding of IL-2 to the IL-2Ra subunit (Arimathe potency of IL-15 as an inflammatory cytokine. With
its capacity to inhibit AICD, to perpetuate memory phe- et al., 1991; Grant et al., 1992; Kuziel et al., 1993). Finally,there may be distinct signals to the nucleus from thenotype CD81 cells, and to induce the expression of cyto-
kines and chemokines involved in the inflammatory re- private receptor subunits or from other proteins nonran-domly associated with them. For example, it has beensponse if indiscriminately expressed, IL-15 could be
associated with serious disorders including autoim- reported, but as yet not confirmed, that following IL-15addition there is a recruitment of TRAF 2 and Syk kinasemune diseases (McInnes et al., 1997). In terms of a more
positive role for IL-15, we propose that by maintaining to the 37 amino acid cytoplasmic tail of the IL-15Rachain (Bulfone-Paus et al., 1999).a pool of translationally inactive IL-15 mRNA diverse
cells may respond rapidly to an intracellular infection or IL-2- and IL-15-Directed Immunotherapyfor Leukemia/Lymphoma, Select Autoimmuneother stimulus by transforming IL-15 mRNA into a form
that can be translated effectively. The IL-15 protein pro- Diseases, and to Prevent Allograft RejectionIL-2R as a Target for Immunotherapy. Most IL-2/15R-duced and secreted could convert T and NK cells into
activated killer cells that might provide an effective host directed therapeutic approaches have targeted the IL-2Ra subunit (Waldmann et al., 1993; Vincenti et al., 1998;response to an invading infectious organism.
A critical issue that remains to be resolved is how Waldmann and O’Shea, 1998). The scientific basis forthis target choice is that IL-2Ra is not expressed bytwo cytokines, IL-2 and IL-15, that share two signaling
receptor subunits and utilize a common Jak3/STAT5 normal resting cells but is constitutively expressed bythe malignant cells in an array of T and B cell leukemias,signaling pathway manifest a number of contrasting
functions. Many alternatives have been suggested as by T cells involved in select autoimmune diseases, andby those T cells that participate in organ allograft rejec-explanations for these differences. The two cytokines
are produced by quite different cells and tissues (Wald- tion. Early human clinical trials involving IL-2Ra-directedtherapy focused on HTLV-I-associated adult T cell leu-mann and Tagaya, 1999). Their synthesis and secretion
are controlled in distinct fashions. Furthermore, their kemia (ATL). The retrovirus HTLV-I encodes a 42 kDaprotein termed tax that is responsible for the transactiva-private specific receptors, IL-2Ra and IL-15Ra, have
different cellular distributions. In particular, IL-2Ra and tion of numerous host genes including those encodingIL-2, IL-2Ra, IL-15, and IL-15Ra that are involved in Tthe high-affinity IL-2 receptor are predominantly ex-
pressed on activated monocytes T, B, and NK cells. cell activation and, potentially, HTLV-I-mediated leuke-mogenesis (Azimi et al., 1998). In the early phases ofHowever, the high-affinity IL-15 receptor and all eight
isoforms of IL-15Ra have a much wider cellular distribu- the disease in patients with ATL, there is evidence sup-porting an autocrine loop involving IL-2 and IL-2Ra thattion. IL-15R expression is observed in T cells, B cells,
macrophages, and in thymic and bone marrow stromal participates in the expansion of the leukemic cells(Maeda et al., 1987). We demonstrated that therapy withcell lines as well as in such tissues as liver, heart, spleen,
lung, skeletal muscle, and activated vascular endothelial an unmodified murine version of the anti-Tac mAb thatblocks the binding of IL-2 to IL-2Ra led to a partial orcells. This widespread distribution is one of the mecha-
nisms underlying the pleiotrophy of IL-15 and may con- complete remission in 6 of the 19 patients with ATLtreated (Waldmann et al., 1993). Effective action of thistribute to the differences in IL-2 and IL-15 action. In

Immunity108
monoclonal antibody in some cases appears to be due peripheral blood mononuclear cells, and the stabiliza-tion or amelioration of the neurological disease (Lehkyto the interdiction of the interaction of IL-2 with its
growth factor receptor leading to cytokine deprivation- et al., 1998). Continuous mAb administration was re-quired to maintain the desired clinical effects.mediated apoptotic cell death. However, neither IL-2
mRNA nor IL-2 protein is expressed in the later phases IL-15/IL-15R-Directed Therapy for AutoimmuneDisease and to Prevent Allograft Rejectionof acute ATL including some cases where anti-Tac has
provided effective therapy. In these cases, prevention Although IL-2Ra-directed therapy has met with consid-erable success in the treatment of leukemia, select auto-of autocrine stimulation by blocking IL-2 interaction with
IL-2R could not be the mode of effective antibody action. immune disorders, and in the prevention of allograftrejection, approaches directed toward this receptorFurthermore, IL-2Ra-directed monoclonal antibodies
were shown to provide effective therapy in a murine subunit have limitations. In particular, antibodies to IL-2Ra, the private receptor for IL-2, do not inhibit themodel of human ATL by an FcR-requiring mechanism
other than blockade of IL-2/IL-2R interaction (Phillips et actions of IL-15, a cytokine that does not bind to thissubunit. Another limitation of IL-2Ra-directed therapyal., 2000). In these cases, effective action that requires
the complete antibody may involve its binding to the is that antibodies directed toward this receptor do notact on resting NK- or NK-T cells that express IL-2Rb andFcRIII present on monocytes and macrophages. This
conclusion is in accord with those emerging from the gc but not IL-2Ra. An additional limitation is suggested byour discussion above on the special functions of the IL-elegant studies of Clynes and coworkers that demon-
strated that FcR-I and/or III are required for effective in 2/IL-2Ra system. In particular, inhibition of IL-2-medi-ated AICD by anti-IL-2R-directed therapy may preventvivo monoclonal antibody action against tumor targets
in many systems including those directed toward HER-2 the generation of AICD-associated peripheral toleranceto both self and to transplantation antigens. The genera-neu using trastuzumab or toward CD20 using retuximab
(Clynes et al., 2000). tion and maintenance of such tolerance could be ofvalue in the treatment of autoimmune disease and inA humanized antibody to IL-2Ra (humanized anti-Tac,
daclizumab) was generated that addressed limitations the prevention of organ allograft rejection. Kirk and co-workers (Kirk et al., 1999) demonstrated that relativelyinherent in the use of the murine version of this mono-
clonal antibody including its immunogenicity, its ineffec- short-term administration of an anti-CD40 ligand anti-body provided long-term protection against renal allo-tiveness in recruiting human host-effector functions,
and its short in vivo survival (Queen et al., 1989). Follow- graft rejection in nonhuman primates. However, the ad-dition of agents such as tacrolimous (FK506) anding encouraging results in animal models and in phase
I/II trials, two phase III randomized, placebo-controlled cyclosporin A that inhibit signaling through the T cellreceptor and thereby inhibit IL-2 synthesis antagonizedclinical trials were performed that included 535 evalu-
ated patients to determine the value of humanized anti- the long-term tolerogenic effect of the anti-CD40 ligandantibody (Kirk et al., 1999). In light of these observations,Tac (daclizumab, Zenapax) in the prevention of renal
allograft rejection (Vincenti et al., 1998). In each trial, an evaluation should be made of anti-IL-2Ra monoclonalantibody therapy such as that used in organ (e.g., isletpatients received placebo or daclizumab in addition to
the standard immunosuppressive regimen. The acute cell) transplantation for its potential to inhibit AICD andthereby to preclude the induction of the desired antigen-graft rejection rate at 6 months was significantly lower,
and renal allograft retention was significantly higher in specific allograft tolerance.Due to these limitations in IL-2 receptor-directed ther-the patients treated with daclizumab (p # 0.01). On the
basis of these phase III trials, FDA approval was ob- apy, IL-15 receptor-directed therapy is being developedfor use in organ transplantation protocols, for applica-tained for the use of daclizumab in the prevention of
acute kidney transplant rejection. In a similar extensive tion to the treatment of autoimmune disorders as wellas diseases caused by the retrovirus HTLV-I. Abnormali-randomized trial, it was shown that basiliximab, a chime-
ric antibody also directed toward IL-2Ra, was associ- ties of IL-15 expression have been reported in diverseinflammatory and neoplastic diseases (Waldmann andated with reduced numbers of acute rejection episodes
in renal allograft recipients (Nashan et al., 1997). This Tagaya, 1999). In particular, abnormally high levels ofIL-15 transcription and translation were observed inagent also received FDA approval for the prevention of
renal allograft rejection. In addition to its use in renal HTLV-I-associated diseases such as adult T cell leuke-mia as well as the autoimmune disorder, tropical spastictransplantation protocols, daclizumab was included in
the spectrum of immunosuppressive agents for gluco- paraparesis (TSP) (Azimi et al., 1999). The HTLV-I taxprotein through a mechanism involving NFkB inducedcorticoid-free immunosuppression administered in an
islet cell transplantation protocol used for patients with the expression of IL-15 and IL-15Ra. In addition, abnor-malities of IL-15 expression were described in inflamma-type 1 diabetes mellitus that provided excellent meta-
bolic control (Shapiro et al., 2000). In addition, we and tory autoimmune disorders including rheumatoid arthri-tis, inflammatory bowel disease, multiple sclerosis,our collaborators have shown that daclizumab (Human-
ized anti-Tac) is of value in the therapy of select T cell– chronic liver disease, and pulmonary sarcoidosis. Forexample, McInnis and coworkers (McInnes et al., 1997)mediated autoimmune disorders. In particular, the mAb
provided effective treatment for noninfectious interme- reported abnormalities of IL-15 in rheumatoid arthritisand suggested that IL-15 expression may precede thatdiate and posterior uveitis in a clinical trial (Nussenblatt
et al., 1999). Furthermore, daclizumab therapy of pa- of TNFa and that IL-15 may be at the apex of a cytokinecascade that includes downstream IL-1, IL-6, GM-CSF,tients with the neurological disease, HTLV-I-associated
HAM/TSP, led to a reduction in HTLV-I viral load, a de- as well as a series of inflammatory chemokines includingMip1a, Mip1b, and IL-8. Other groups demonstrated IL-crease in the ex vivo spontaneous T cell proliferation of

Minireview109
15 production by endothelial cells in rheumatoid tissues, in AICD it may lead to the death of T cells that recognizeshowed that intraarticular injection of IL-15 led to T cell antigens expressed on the tumor cells. That is, theseaccumulation in rheumatoid arthritis synovial tissues en- cells may interpret the tumor cells as self. Futhermore,grafted into SCID mice in vivo, and that such injections the inhibition mediated by IL-2 on the survival of memoryof IL-15 led to the recruitment of activated T cells into T cells directed toward the tumor is not desired. Thus,the synovial membrane, possibly contributing to the IL-15 with its inhibitory action on AICD and its stimula-pathogenesis of the arthritis (Oppenheimer-Marks et al., tory role in the persistence of memory CD81 T cells may1998). On the basis of these observations, a number of be superior to IL-2 in the treatment of cancer and asnew therapeutic approaches directed toward IL-15, its a component of vaccines directed toward cancer orreceptor, or to Jak3, a critical element in its signaling infectious agents.pathway, are being developed for use in the therapy of In conclusion, our emerging understanding of the IL-inflammatory autoimmune disorders. The administration 2/IL-2R and IL-15/IL-15R systems including the defini-of an IL-15 inhibitor, the soluble high-affinity IL-15Ra tion of the actions that these cytokines share as well asreceptor chain, prevented the development of murine those functions where their roles are distinct opens newcollagen-induced arthritis and inhibited allograft rejec- possibilities for the development of more rational im-tion (Ruchatz et al., 1998). Furthermore, an IL-15 recep- mune intervention that may be of value in the preventiontor antagonist produced by mutation of a glutamine resi- of allograft rejection, in the treatment of lymphocyticdue within the C terminus of IL-15 to aspartic acid leukemia/lymphoma, diseases associated with the ret-competitively inhibited IL-15-triggered cellular prolifera- rovirus HTLV-I, as well as T cell–mediated autoimmunetion (Kim et al., 1998). This IL-15 mutant markedly at- disorders.tenuated antigen-specific delayed hypersensitivity re-
Selected Readingsponses in Balb/c mice and enhanced the acceptanceof pancreatic islet cell allografts (Kim et al., 1998). Our
Arima, N., Kamio, M., Okuma, M., Ju, G., and Uchiyama, T. (1991).own IL-15-directed therapeutic approaches have fo-J. Immunol. 10, 3396–3401.
cused on the IL-2Rb receptor subunit shared by IL-2Armitage, R.J., Macduff, B.M., Eisenman, J., Paxton, R., and
and IL-15 in an effort to yield more profound immuno- Grabstein, K.H. (1995). J. Immunol. 154, 483–490.suppression than can be achieved by inhibition limited
Azimi, N., Brown, K., Bamford, R.N., Tagaya, Y., Siebenlist, U., andto the action of a single cytokine such as IL-2 or by an Waldmann, T.A. (1998). Proc. Natl. Acad. Sci. USA 95, 2452–2457.antibody directed toward a private receptor such as IL- Azimi, N., Jacobson, S., Leist, T., and Waldmann, T.A. (1999). J.2Ra (Tinubu et al., 1994; Waldmann and O’Shea, 1998). Immunol. 163, 4064–4072.Our initial trials involved Mikb1, an antibody directed Bamford, R.N., Grant, A.J., Burton, J.D., Peters, C., Kurys, G., Gold-toward IL-2Rb that inhibits IL-15 action on T and NK man, C.K., Brennan, J., Roessler, E., and Waldmann, T.A. (1994).cells. A humanized version of this antibody prolonged Proc. Natl. Acad. Sci. USA 91, 4940–4944.renal allograft survival in cynomolgus monkeys (Tinubu Bamford, R.N., Battiata, A.P., Burton, J.D., Sharma, H., and Wald-et al., 1994). In our initial clinical trial, we are evaluating mann, T.A. (1996). Proc. Natl. Acad. Sci. USA 93, 2897–2902.
Mikb1 in the therapy of patients with T cell type large Bamford, R.N., DeFilippis, A.P., Azimi, N., Kurys, G., and Waldmann,T.A. (1998). J. Immunol. 160, 4418–4426.granular lymphocytic leukemia associated with hemato-
cytopenia. The monoclonal large granular lymphocytes Bulfone-Paus, S., Bulanova, E., Pohl, T., Budagian, V., Durkop, H.,Ruckert, R., Kunzendorf, U., Paus, R., and Krause, H. (1999). FASEB(LGLs) involved in this disease express IL-2Rb and gcJ. 13, 1575–1585.but not IL-2Ra (Tsudo et al., 1987) and respond to IL-Burton, J.D., Bamford, R.N., Peters, C., Grant, A.J., Kurys, G., Gold-15. Finally, as a substitute for the present IL-2/IL-2R-man, C.K., Brennan, J., Roessler, E., and Waldmann, T.A. (1994).directed therapeutic agents, IL-15/IL-15R-directed ther-Proc. Natl. Acad. Sci. USA 91, 4935–4939.apy should be evaluated in clinical trials involving organClynes, R.A., Towers, T.L., Presta, L.G., and Ravetch, J.V. (2000).allografts in light of the reported success of this ap-Nat. Med. 6, 443–446.proach in preclinical models (Tinubu et al., 1994; Kim etDiSanto, J.P. (1997). Curr. Biol. 7, R424–R426.al., 1998). Such therapy focusing on IL-15 is supportedDooms, H., Desmedt, M., Vancaeneghem, S., Rottiers, P., Goossens,in part by the desire to inhibit the stimulatory actionV., Fiers, W., and Grooten, J. (1998). J. Immunol. 161, 2141–2150.normally played by IL-15 on activated T and NK cells.Dooms, H., Van Belle, T., Desmedt, M., Rottiers, P., and Grooten,Furthermore, as discussed above, an objective of suchJ. (2000). Blood 96, 1006–1012.therapy directed toward the IL-15/IL-15R system wouldGiri, J.G., Kumaki, S., Ahdieh, M., Friend, D.J., Loomis, A., Shane-be to interfere with the IL-15-mediated persistence ofbeck, K., DuBose, R., Cosman, D., Park, L.S., and Anderson, D.M.CD81 memory phenotype T cells and to eliminate the(1995). EMBO J. 14, 3654–3663.
inhibitory action normally played by IL-15 on IL-2-medi-Grabstein, K.H., Eisenman, J., Shanebeck, K., Rauch, C., Srinivasan,
ated AICD. These agents that inhibit IL-15 action could S., Fung, V., Beers, C., Richardson, J., Schoenborn, M.A., Ahdieh,be of value in other situations where self-tolerance is of M., et al. (1994). Science 264, 965–968.value such as in the treatment of autoimmune diseases or Grant, A.J., Roessler, E., Ju, G., Tsudo, M., Sugamura, K., and Wald-in allograft protocols where the development of peripheral mann, T.A. (1992). Proc. Natl. Acad. Sci. USA 89, 2165–2169.tolerance to the graft is desired. Kennedy, M.K., Glaccum, M., Brown, S.N., Butz, E.A., Viney, J.L.,The Use of IL-15 in the Therapy of Cancer Embers, M., Matsuki, N., Charrier, K., Sedger, L., Willis, C.R., et al.and as a Component of Vaccines (2000). J. Exp. Med. 191, 771–780.IL-2 has been approved for use in the treatment of pa- Kim, Y.S., Maslinski, W., Zheng, X.X., Stevens, A.C., Li, X.C., Tesch,tients with metastatic renal cell carcinoma or with meta- G.H., Kelley, V.R., and Strom, T.G. (1998). J. Immunol. 160, 5742–
5748.static melanoma. It has also been used as a componentof vaccines for cancer. However, due to its pivotal role Kirk, A.D., Burkly, L.C., Batty, D.S., Baumgartner, R.E., Berning,

Immunity110
J.D., Buchanan, K., Fechner, J.H., Jr., Germond, R.L., Kampen, R.L., Waldmann, T.A., and O’Shea, J. (1998). Curr. Opin. Immunol. 10,507–512.Patterson, N.B., et al. (1999). Nat. Med. 5, 686–693.
Waldmann, T., and Tagaya, Y. (1999). Annu. Rev. Immunol. 17, 19–49.Ku, C.C., Murakami, M., Sakamoto, A., Kappler, J., and Marrack, P.(2000). Science 288, 675–678. Waldmann, T.A., White, J.D., Goldman, C.K., Top, L., Grant, A., Bam-
ford, R., Roessler, E., Horak, I.D., Zaknoen, S., Kasten-Sportes, C.,Kuziel, W.A., Ju, G., Grdina, T.A., and Greene, W.C. (1993). J. Immu-et al. (1993). Blood 82, 1701–1712.nol. 8, 3357–3365.Willerford, D.M., Chen, J., Ferry, J.A., Davidson, L., Ma, A., and Alt,Lehky, T.J., Levin, M., Kubota, R., Bamford, R.N., Flerlage, A.N.,F.W. (1995). Immunity 3, 521–530.Soldan, S.S., Leist, T.P., Xavier, A., White, J.D., Brown, M., et al.
(1998). Ann. Neurol. 44, 942–947. Zhang, X., Sun, S., Hwang, I., Tough, D.F., and Sprent, J. (1998).Immunity 8, 591–599.Lenardo, M.J. (1996). J. Exp. Med. 183, 721–724.
Lin, J.X., Migone, T.S., Tsang, M., Friedmann, M., Weatherbee, J.A.,Zhou, L., Yamauchi, A., Bloom, E.T., Mietz, J., John, S., and Leonard,W.J. (1995). Immunity 2, 331–339.
Lodolce, J.P., Boone, D.L., Chai, S., Swain, R.E., Dassopoulos, T.,Trettin, S., and Ma, A. (1998). Immunity 9, 669–676.
Maeda, M., Arima, N., Daitoku, Y., Kashihara, M., Okamoto, H., Uchi-yama, T., Shirono, K., Matsuoka, M., Hattori, T., Takatsuki, K., et al.(1987). Blood 70, 1407–1411.
Marks-Konczalik, J., Dubois, S., Losi, J.M., Sabzevari, H., Yamada,N., Feigenbaum, L., Waldmann, T.A., and Tagaya, Y. (2000). Proc.Natl. Acad. Sci. USA 97, 11445–11450.
Marrack, P., Bender, J., Hildeman, D., Jordan, M., Mitchell, T., Mura-kami, M., Sakamoto, A., Schaefer, B.C., Swanson, B., and Kappler,J. (2000). Nat Immunol 1, 107–111.
McInnes, I.B., Leung, B.P., Sturrock, R.D., Field, M., and Liew, F.Y.(1997). Nat. Med. 3, 189–195.
Naora, H., and Gougeon, M.L. (1999). Cell Death Differ. 6, 1002–1011.
Nashan, B., Moore, R., Amlot, P., Schmidt, A.G., Abeywickrama, K.,and Soulillou, J.P. (1997). Lancet 350, 1193–1198.
Nussenblatt, R.B., Fortin, E, Schiffman, R., Rizzo, L., Smith, J., van-Veldhuisen, P., Sran, P., Yaffe, A., Goldman, C.K., Waldmann, T.A.,et al. (1999). Proc. Natl. Acad. Sci. USA 96, 7462–7466.
Oppenhimer-Marks, N., Brezinschek, R.I., Mohamadzadeh, M., Vita,R., and Lipsky, P.E. (1998). J. Clin. Invest. 101, 1261–1272.
Phillips, K.E., Herring, B., Wilson, L.A., Rickford, M.S., Goldman,C.K., and Tso, J.Y. and Waldmann, T.A. (2000). Cancer Res. 60,6977–6984.
Queen, C., Schnieder, W.P., Selick, H.E., Payne, P.W., Landolfi, N.F.,Duncan, J.F., Avdalovic, N.M., Levitt, M., Junghans, R.P., and Wald-mann, T.A. (1989). Proc. Natl. Acad. Sci. USA 86, 10029–10033.
Refaeli, Y., Van Parijs, L., London, C.A., Tschopp, J., and Abbas,A.K. (1998). Immunity 8, 615–623.
Ruchatz, H., Leung, B.P., Wei, X.Q., McInnes, I.B., and Liew, F.Y.(1998). J. Immunol. 160, 5654–5660.
Sadlack, B., Kuhn, R., Schorle, H., Rajewsky, K., Muller, W., andHorak, I. (1994). Eur. J. Immunol. 24, 281–284.
Shapiro, A.M.J., Lakey, J.R.T., Ryan, E.A., Korbutt, G.S., Toth, E.,Warnock, G.L., Kneteman, N.M., and Rajotte, R.V. (2000). N. Engl.J. Med. 343, 230–238.
Stevens, A.C., Matthews, J., Andres, P., Baffis, V., Zheng, X.X., Chae,D.W., Smith, J., Strom, T.B., and Maslinski, W. (1997). Amer. J.Physiol. 35, G1201–G1208.
Tagaya, Y., Burton, J.D., Miyamoto, Y., and Waldmann, T.A. (1996).EMBO J. 15, 4928–4939.
Tinubu, S.A., Hakimi, J., Kondas, J.A., Bailon, P., Familletti, P.C.,Spence, C., Crittenden, M.D., Parenteau, G.L., Dirbas, F.M., Tsudo,M., et al. (1994). J. Immunol. 153, 4330–4338.
Tsudo, M., Goldman, C.K., Bongiovanni, K.G., Chan, W.C., Winton,E.F., Yagita, M., Grimm, E.A., and Waldmann, T.A. (1987). Proc. Natl.Acad. Sci. USA 84, 5394–5398.
Van Parijs, L., Refaeli, Y., Lord, J.D., Nelson, B.H., Abbas, A.K., andBaltimore, D. (1999). Immunity 11, 281–288.
Vincenti, F., Kirkman, R., Light, S., Bumgardner, G., Pescovitz, M.,Halloran, P., Neylan, J., Wilkinson, A., Ekberg, H., Gaston, R., et al.(1998). N. Engl. J. Med. 338, 161–165.
Waldmann, T.A. (1991). J. Biol. Chem. 266, 2681–2684.









![1 1 1 1 1 1 1 ¢ 1 , ¢ 1 1 1 , 1 1 1 1 ¡ 1 1 1 1 · 1 1 1 1 1 ] ð 1 1 w ï 1 x v w ^ 1 1 x w [ ^ \ w _ [ 1. 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 ð 1 ] û w ü](https://img.pdfslide.net/doc/110x75/5f40ff1754b8c6159c151d05/1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-w-1-x-v.jpg)











![[XLS]fmism.univ-guelma.dzfmism.univ-guelma.dz/sites/default/files/le fond... · Web view1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1](https://img.pdfslide.net/doc/110x75/5b9d17e509d3f2194e8d827e/xlsfmismuniv-fond-web-view1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1-1.jpg)