Embed Size (px)
Citation preview

Community Based Reha bilitation
Under Conditions of Political Violence:
A Palestinian Case Study
Sandra Ballantyne
A thesis submitted to the School of
Rehabilitation Therapy
in confomity with the requirements for
the degree of Master of Science
Queen's University
Kingston, Ontario, Canada
May, 1999
copyright O Sandra M Ballantyne, 1999

National Library (*) of Canada Bibliothèque nationale du Canada
Acquisitions and Acquisitions et Bibliographic Senrices secvices bibliographiques
395 Wellington Street 395, rue Welltnglon Ottawa ON K1A ON4 Ottawa ON K 1 A ON4 Canada Canada
Your hb Vofre refersnce
Our tüe Noire reference
The author has granted a non- L'auteur a accordé une licence non exclusive licence allowing the exclusive permettant à la National Library of Canada to Bibliothèque nationale du Canada de reproduce, loan, distribute or sell reproduire, prêter, distribuer ou copies of this thesis in microfom, vendre des copies de cette thèse sous paper or electronic formats. la forme de microfichelfilm, de
reproduction sur papier ou sur format électronique.
The author retains ownenhip of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial extracts fiom it Ni la thèse ni des extraits substantiels may be printed or otherwise de celle-ci ne doivent être imprimés reproduced without the author's ou autrement reproduits sans son permission. autorisation.

ABSTRACT
This study was undertaken to investigate the appropriateness of cornmunity based
rehabilitation (CBR) under conditions of political violence. A qualitative case study was made of
the CBR programme of the Union of Palesthian Medical Relief Committecs. The programme
developed under conditions of military occupation and popular uprising (the Intifada), during which
injuries and new disabilities overwhelmed existing medical and rehabilitation services.
A detailed description is provided of the Palestinian experience of CBR, and of the contlict
conditions that influence. its development. Specifically, conditions of repression and resistruice
affectecl individual elemcnts of CBR, and programme participants responded in a varicty of ways to
the obstacles encountered.
While obstacles were rife, it became apparent that the Intifada presented positive factors
for the development of CBR, such as heightened community capacities and the oppominity for
social change. Using the perspective of CBR as community development, the Capacities and
Vulnerabilities Analysis (CVA) framework provided a theoretical bais by which to explain the
study findings.
The findings of this midy indicated that, for a case within the Palestinian Intifada, where
community social/organizational and attitudinaVmotivationa1 capacities were high, a CBR
programme with a community developrnent approach was successfully developed. The
'<ippropnateness," then, of CBR under conditions of political violence can be understood in terms
of its contribution to cornmunity development. With this in mind, it was concluded that several
factors be assessed before endorsing a CBR initiative in a region of confiict. These factors hclude
the community capacities and wlnerabilities, the type of conflict, the elernents of CBR to be
pnontized in a pa~icular project, and contexaial factors such as culture.

ACKNOWLEDGEMENTS
1 sincerely thank:
my supe~sor, Will Boyce, for his rigour and compassion,
my study respondents, especially Dr. AIlam Jarrar and the UPMRC CBR team rnembea, for
sharing their experiences, knowledge, and insights, in the midst of busy and trying times,
my family and fiiends, for continuing to believe, and
my colleague, confidante and husband, Ibrahim, for giving me data, encouragement, new horizons,
and Khalil.


4.1.4 Summary ..................... .. ....................................................................................... 37 ................................................................ 4.2 Contextual Factors Anecting CBR in Palestine 37
............................................................ 4.2.1 Palestinian Culture - Support and Authority 37 4.2.2 Regional and Community Characteristics - Geo-political and Economic Disparities .. 39
...... 4.2.3 Professionalization and Institutiondiration o f Disability - Privilege of Expertise 40 .......................... 4.2.4 Attitudes Towards People with Disabilities - Tradition and Charity 41
............................................................................................................ 4.2.5 Summary 4 3 ......................................................................................... 4.3 Political Violence and CBR 4 3
......................................................................... 4.3.1 The Conditions of Political Violence 43 .................... 4.3.2 Effects of the Conditions of Confiict upon the CBR Work Environment - 47
4.3.3 Effects of Political Violence on CBR Elements .......................................................... 50 4.3.4 Political Violence and CBR: Surnmary of Findings ................................................... 75
.................................................................................................. CHAPTER 5 DISCUSSION 78
.............................................................................. 5.1 Design Issues and Smdy Limitations 78 ..................................................................................................... 5.2 Discussion of Findings 79
5.2.1 ThcRealmsofCommunity: UnderstandingCBRandtheIntiFada ............................. 80 5.2.2 Capacities and Vulnerabilities, and the UPMRC Response ........................................ 85 5.2.3 Comrnunity Development as Political Action ........................................................... 90
........................................................... 5.2.4 Conflict and Development - a Place for CBR 91 ............................................................................................ 5.3 Conclusion and Implications 93
................................................................................................................ REFE RENCES 9 5
.................... APPENDIX 1 . CAPACITlES AND VULNERABILITIES ANALYSIS 105 ..................................................... APPENDJX II . INTERVIEW QUESTION GUIDE 106
................................................................ APPENDIX III . DATA ANALYSIS TOOLS 108 .................. ................ APPENDIX IV . INFORMATION AND CONSENT FORM .. 1 11

LIST OF TABLES
................................................................ Table 3.1 Description of InterMew Respondenîs 22
Table 4.1 Regional Catchment of CBR Teams .................................................................. 32
......................................................... Table 4.2 Characteristics of UPMRC CBR Workers 36
............................................................................... Table 4.3 CBR Programme Activities 36
........................................................... Table 5.1 CBR Elements as Realms of Comrnunity 81
.......................................... Table 5.2 Capacities in Palestine for the Development of CBR 86
.................................... Table 5.3 Vulnerabilities in Palestine for the Developrnent of CBR 87

LIST OF FIGURES
...................................... Figure 4.1 The Position of CBR within the UPMRC Organization 30
Figure 4.2 Map of the West Bank, Showing Catchent Areas of CBR Projects .................. 31
................................................................................. Figure 4.3 Participants and Linkages 33
Figure 4.4 Structure of the CBR Programme ...................................................................... 35

LIST OF ABBREVIATIONS
AIPPHR
CBR
CNCR
CVA
GUPD (GUDP)
IDs
I L 0
NGO
PASSIA
PHC
RI
RW
UN
UNCTAD
UNDP
UNESCO
lMHCR
UNICEF
UNRWA
UPMRC
VHW
WHO
Association of Israeli and Palestidan Physicians for Human Rjghts
comrnunity based rehabilitation
Central National Cornmittee for Rehabilitation
Capacities and Vulnerabilities Analysis
Gencral Union of Pafestinian Disabled
(Later became the Generai Union of Disabled Palestinians)
identity cards
Internat ional Labour Organization
non-govemmental organization
Palestinian Acadcmic Society for the Study of International Mairs
primary health care
Rehabilitation International
rehabilitation worker
United Nations
United Nations Commission on Trade and Development
United Nations Development Program
United Nations Educational, Scientific and Cultural Organitation
Ulited Nations Hiçh Commission for Refbgees
United Nations Childrcn's Fund
United Nations Relief and Works Agency for Palestinian Refugees
Union of Palestinian Medical Relief Cornmittees
village health worker
World Health Organization
vii

CHAPTER 1
INTRODUCTION
1.1 Statement of the Problem
Worldwide, the scope and impact of war are tremendous. Codict causes disability in
many ways, and it has grave consequences for people witb disabilities who are caught in the
violence. Most conflicts occur in developing countria, where disabled people arc particularly
disadvantaged. While community based rehabilitation (CBR) was estabiished as an approach for
providing accessible rehabilitation services within developing countnes, the appropriateness of the
CBR approach to situations of political violence is unclear. It may be naive to expect communities
that are under extraordinary stress to sustain community based rehabilitation initiatives. On the
other hand, it may be that essential resources are still to be found within families and communities.
1.2 Study Purpose and Questions
The purpose of the current study was to provide a description of a CBR programme that
developed and operated under conditions of political violence. Further, the study \vas to allow
those involved to interpret the elements of CBR within their situation, leading to an understanding
of the relevance of CBR under conditions of conflict. The study sought to answer the questions: 1s
CBR an appropriate rehabilitation response under conditions of political violence, and if so, how is
it appropriate? These questions were answered using a case study of a Palestinian CBR
progranune that was implemented during conditions of occupation and uprising.

1.3 Relevance
Rehabilitation worken who practise, or seek to practise, in regions expenencing violence
will benefit from a description and an explanation of how CBR elements are affectai by such
conditions. The study provides them with greater knowledge with which to judge the suitability of
CBR, allowing more infomed choices in the utilizition of its approach. In addition, this study
contributes to the academic and professional field of rehabilitation theapy by furthering discussion
of the philosophy and practice of CBR. These contributions support the decision-making processes
surroundhg programming and policy-rnaking for rehabilitation efforts occumng in circumstances
of political violence.

CHAPTER 2
LITERATURE REVIEW
2.1 Community Based Rehabilitation
Community based rehabilitation represents a response, in boib developed and developing
countries, to the need for adequate and appropriate rehabilitation services, to be available to a
greater proportion of the disabled population (Peat, 1991, 1997). Within developing nations, CBR
atternpts to meet the ovenvhelming need for rehabilitation services, reaching the tremendous
numbers of disabied pcrsons who have lirnited or no access to such resources. Estimations are that
only 1 to 3% of disabled people living in developing countries who require rehabilitation seMces
receive thern, these services being panicularly inaccessible to the mral majority (World Health
Organization W O J , 198 1 ; H elander et al., 1 989; Peat, 1 997).
What cxactly constitutes the principles of CBR is the subject of much discussion. The
joint position paper of the International Labour Organization (ILO), the United Nations
Educational, Scientific and Cultural Organization (UNESCO) and the WHO (1994) has dcfined
CBR as "a strategy within community development for the rehabilitation, equalization of
opportunities and social integration of al1 people with disabilities ... implemcnted through the
combined efforts of disabled people themselves, their families and comrnunities, and the
appropriate health, education, vocational and social services" (p. 2). The WHO has contrasted
CBR with institution-based and outreach seMces of rehabilitation, in that there is a large-scale
transfer of knowledge about disabilities and of rehabilitation skills to the people with disabilities,
their b i l i e s , and members of the community (Helander et al., 1989). Jn this way, resources are
made available at the community level, and rehabilitation has been "democratized" (p. 3).
Einer Helander (1992) highlights the founding principles of CBR as being equality, social
justice, solidarity, integration and dignity for people with disabilities. In his detailed definition of

CBR, Helander (1993) States that CBR "is a strategy for improving service delivery, for providing
more equitable opportunities and for prornoting and protecting the human nghts of disabled people"
(p. 3). He goes on to Say that
It calls for the hi11 and cuordinated [sic] involvement of al1 lcvels of society: cornmunity, intermediate and national. It seeks the integration of the interventions of al1 relevant secton - educational, health, legislative, social and vocational - and aims at the niII representation and empowerment of disabled people. Its goal is to bnng about a change; to develop a symm capable of reaching al1 disabled people in need and to educate and involve governments and the public, using in each country a level of resources that is realistic and maintainable.
David Werner (1990a) proposes two goals of rehabilitation at the community level. The
first goal is '20 create a situation that allows each disabled person to live as fulfilling, self-reliant,
and whole a life as possible, in close relation with other people," and the second goal is "to help
other people - family, neighbours, school-children, members of the cornmunity - to accept,
respect, feel cornfortable with, assist (only whcre necessary), welcome into their lives, provide
qua1 opportunities for, and appreciate the abilities and possibilities of disabled people" (p. 6). in
addition, Werner stresses the importance of disabled people being leaders and workers in
rehabilitation activities, of rneaningful work and training for disabled people, and of local resources
being used for rehabilitation equipment and aids.
Rehabilitation International (RI) and the United Nations Children's Fund (UNICEF)
Technical Support Programme assert that CBR is based on the development concept of individuals
with disabilities becoming empowered to take action to improve their owvn lives and become
contributors to society (RINNICEF, 1989-90). In Canada, the International Centre for the
Advancement of Community Based Rehabilitation (ICACBR, 1993) has outlined pnnciples of a
CBR programme, which include change in community attitudes towards disability, empowement
of people with disabilities, participation and partnership in programme implementation and
development, and education (see also kat, 1997, p. 32).

Drawing upon an emerging consensus in these sources, then, a usehl list of key elcments
of CBR has been formed. These eight elements provide a framework for discussing CBR within
this study. A CBR programme is characterized by the following key elements:
a) Promoting positive community attitudes towards disability
b) Promoting integration of people with disabilities within society
c) Transferring rehabilitation knowledge and skills
d) Providing participantdirected rehabilitation seMces
e) Implementing the programme with community participation
f) Exhibiting a modcl of partnership among people with disabilities, families, the
comrnunity, and rehabilitation personncl
g) Using locally made rehabilitation aids and equiprnent
h) Participating in a referral network with specialists and institutions, for professional and
technical rchabilitation support.
It has oftcn been statcd that there is no bluepnnt for a CBR project (Peat, 199 1; Helander,
1993). This is bccause countries, regions, and cornmunitics Vary enonnously with respect to their
culture, political structures, populations and their distribution, and financial and workforcc
resources. Each of thesc circumstances will direct the nature of a "community based" programme.
In many societies, however, conditions of political violence overlie or disrupt these circurnstances.
Increasingly, a cornmunity-based approach to rehabilitation has been advocated in such conflict
conditions (ICACBR, 1996; Peat, 1997; Peat et al., 1997; RI/UNICEF, 199 1; UMICR, 1992;
UNRWA, 1992; Werner, 1990b; see also Boyce & Ballantyne, 1997).

2.2 Political Violence - Definition and Scope
In the search for a term that encompasses such diverse States as Ml-scale armed conflict,
rnilitary occupation, or popuiar rebellion, it is helpfûl to use political violence, as described in the
epidemiological work of Zwi and Ugalde (1989, 199 1). In an examination of impacts upon public
health, they discem four major forrns of political violence: stnictural, repressive, reactive, and
combative. These oEer a description of political violence ranging from imposed societal inequities
in resources and power (structural political violence, see also Agerbak, 1996), to the processes of
militarization and war (combative political violence), This framework inchdes violent acts by the
state, or opposition groups, such as political assassinations, torture, disappearances, dçtention, and
harassrnent (repressive political violence). Also included is violence against the state in the forrn of
coups d'etat, gemlla hvarfare, and revolutionary force (rûlctive political violence). It is helpfùl to
use the term political violence, to avoid a narrow interpretation that may arise when considering the
diverse experiences of populations under conditions of 'war.'
A consideration of the conditions and effects of political violence is highly impomt within
our international context, because the crisis is widesprcad. The Unitcd Nations Development
Program (UNDP, 1994, p. 47) notes that 42 countries expcrienced 52 major conflicts in 1993, a
further 37 countnes expcricnced '*political violence", and of these 79 countries, 65 were in the
developing world. In thcse developing countries, victims are from pwr families, who cannot flee,
are therefore at greater risk of death and injury, and are less able to access rehabilitation seMces
(Machel, 1996; RI/UNICEF 1991).
Victims of modem war are largely civilians, and the most vulnerable of these are children
and women. While in World War 1, 5% of casualties were civilians, in Wortd War II this figure
was 50%, and presently 80 to 90% of war victims are civilians (Agerbak, 1996; Ahlstrom, 1991;
Cairns, 1997; UNICEF, 1986a). The technology and tactics of modem conflict target the social
Uifrastructure of the enemy. This entails destroying communication facilities, roads, bridges, and

power generating plants, to shaner the economic base and the morale of the civilian population
(UNICEF, l986a). Civilians are not merely indirectly affectai, but are a strategic focus. Targets
are schools, hospitals, health workers, and children (Machel, 1996; Nixon, 1990; WUNICEF,
199 1; UNICEF, 1994). Atrocities against civilians are designed to undermine the sense of society
which could help to build peace again (Cairns, 1997). Even "low intensity conflict" serves to
burden the enemy with an injurcd and disabled population (Aston, 1992; Carey, 1990; Coupland
and Korver, 199 1 ; Garfield, 1989; Lundgren and Lang, 1989; Werner l99Ob). In such cases, the
violence is designed "to infiict maximum damage while minimizing the nsk of death" (Physicians
for Human Rights, 1988).
UNICEF (1996) has estimated that 400,000 people died per year in wars in developing
countries, fiom 1945 to 1996. Others note a drunatic increase in the last decade, with more than a
million per year for the nineties (Cairns, 1997) and 4 million deaths as a resuk of ethno-political
wars in 1993-94 alone (UNDP 1994, p 49). UNICEF notes that for eveiy child killed by war, three
more are seriously or pemanently disablcd, resuiting in 4 million childrcn physically disabled and
10 million psychologically traurnatized by war during the 1980's (Machel, 1996; UNICEF, 199 1).
Evidcnce fiom Afghanistan showcd that thc incidence of disability nearly doubled among children
living in zones of armed conflict (LTNICEF, 1990).
Despite the great numbers and drastic situation, little data is available regarding injuries
and the extent of rehabilitation nceds. Reasons cited for this include: the lack of tirne and energy
for information collection during the chaos of war, bamcrs irnposed upon personnel which fotbid
travel to remote locations where civiliûns are under attack, the low priority placed upon concems of
disabled individuals (especially women and children), and rnethodological concems (Boyce &
Weera, 1998; WUNICEF, 199 1; Giacaman & Daibes, 1989). In ongoing war, epidemiologists
face the special problems of continuous change where long term planning is virtually impossible,
military sensitivities impeding data collection, and necessary compromise wvith respect to scientific

rigour (Annenian, 1989). Available statistics should also be interpreted carehilly, as they can be
used by opposing sides as 'political wcapons7' (Rigby, 199 1, p. 87).
2.3 Political Violence and Health
The pemicious effects of political violence upon the health of a population are direct, in
t e m of injuw and destroyed health facilities, as well as indirect (Black, 1993; Carballo et al.,
1996; Garfield, 1989; Godfiey & Kalache, 1989; ltyavyar & Ogba, 1989; Lundgren & Lang,
1989; Machel, 1996; Macrae & Zwi, 1994; Rautio & Paavolainen, 1988; Ruff & Ward, 1991;
Siegel et al., 1985; Toole a al., 1993; Zwi & Ugalde, 1989, 1991). The indirect impacts of
political violence greatly outweigh the direct effccts, and daim more victims. Disruptions to food
production and distribution, water and waste systems, shelter, transportation and communication,
health services and the environment have serious and long-lasting consequenccs. Poverty and
persistent econornic trouble are associatcd with high military e'tpenditures, and urban and rural
destruction. When it is considered that most situations of armed conflict occur in developing
nations, the nsks become even more alamingly evident. Conditions of political violence introducc
or wonen malnutrition, starvation, the spread of infectious and pamitic diseases, injury, mental
illness and despair.
2.4 Political Violence and Disability
2.4.1 Direct and Indirect Effccts
Disability can also be a direct or indirect consequmce of political violence (Crisp, 1989;
RIRTNICEF, 1991). Impairrnents and disabilities caused directly by conflict are frequently a result
of orthopaedic trauma (especially of the limbs, and including amputation), spinal cord injury, head
injury, peripheral nerve injury, eye injury and hcaring damage, bums, respiratory complications,

and psychological and emotional trauma (Lundgren & Lang, 1989; WUNICEF, 199 1 ; UNICEF,
1994; Wemer 1 WOb). The nature of these irnpairments depends upon the characteristics of the
wnfiict, and the use of various explosives, landmines, fir~anns, instruments of beating and torture,
and tear gas (Habibi, 1994; Richman, 1995; Schaller & Nightingale, 1992; UNICEF, 1994).
Disabilities which are indirectly causeà or exacerbated by political violence relate prirnanly
to malnutrition (e.g., disabilities resulting fiom vitamin A and iodine deficiency - blindness,
deahess, and mental disability), infectious paediatric diseases (e.g., disabilities resulting from polio
and measles and which could be prevented by immunization programmes), and other infectious
diseases (e.g., disabilities resulting fiom tuberculosis and leprosy, as well as blindness and deahess
resulting fiom untreated eye and ear infections) (Cnsp, 1989; RVLMICEF, 199 1 ; Richman, 1995;
Werner, 1987, 1990b; UNICEF, 1990). Carbailo (1996) and Machel (1996) have also identified an
increase in the number of congenital disabilities attributable to inadequate prenatal care and
screening.
Impairment and disability are worscned by the absence or inadequacy of medical and
rehabilitation facilities, which are usually poorly developcd pnor to hostilities (UNICEF, 1990;
Zwi & Ugalde, 1991) and are ofien unavailable to refugees (Crisp, 1989). There are often delays
in accessing facilities, and in some cases admission to a rnedical facility may be avoided, for fear of
being exposed to arrea or capture (Al-Haq, 1988, 1989; Physicians for Human Rights, 1988). The
inability to travel to a hospital, or to attend rehabilitation programmes on a continuous basis,
worsens the prognosis for the original injury and leads to poor outcornes of treatment (Ballantyne,
1988).
2.4.2 Psvcho-social Trauma
It has been stated that "Psycho-social trauma is the most widespread effect of armed
conflict" (UNICEF, 1990, p. 194). Emotional, psychological and mental trauma which result

directly or indirectly from amed conflict are frequently profound and enduring (Bryce et al., 1989;
COPEDU, 1989; Eade & Williams, 1995, pp. 855-58; Garbarino et al., 199 1; Machel, 1996;
Richman, 1995; Schaller & Nightingale, 1992). Psychological disabilities rnay be relate. to king
the victim of atrocities, witnessing atrocities, feeling that death is imminent, being separated from
family and community, emotional distress comrnunicated through family members, expenencing the
destruction of the elements of normal lifc, or social rcjection as a rcsult of physical disability
(Gibson, 1989; RVUNICEF, 199 1; UNICEF, 1994). These long-lasting psychological effects have
implications for how victims, especially children, devdop attitudes, rclationships, moral values, and
a mental framcwork for undcrstanding life and society (Machel, 1996; UNICEF, 1990). There are
also implications for the possibility of future peaceful resolutions to the conflict (Physicians for
Human Rights, 1988; Rankin, 1991).
In any corn muni^ thçre is a population alrcady living with disabilities, oftcn less
recognized than the newly injured (Ballantyne, 1988; Godfiey & Kalache, 1989; Haramy, 1993;
Richman, 1995). Disability gained through fighting may bring honour (Atshan, 1997; Bruun,
1995; Salem, 1 WO), and esisting rehabiiitation is often gçared to adult men, especially combatants
(UNICEF, 1990). Nonctheless, in circurnstances of political violence, al1 disabled people suffer the
handicapping conditions of poverty, despair, inaccessible physical surroundings, infrastructure and
community breakdown, and facilities (which are oflen of marginal adequacy to begin with) being
taxd beyond the ability to cope (Physicians for Hum,m Rights, 1988; WHO, 198 i). In the context
of ecanomic stress, family breakdown and socid dislocation, disabled persons are also at greater
risk of domestic violence and child abuse (RI/LTNICEF, 199 1). They are increasingly dependent
upon others if it is necessary to flee conflict (Despouy, 1991 ; Richman, 1995). Howvever, negative
attitudes, cultural restrictions and ignorance may further disadvantage disabled women, children,

and the eiderly by leaving them bchind when the community is fleeing, and by puîting them lm in
line for food and medicine (Godfiey & Kalache 1989; RVUNICEF, 1991). Inability, or
unwillingness, to incur the costs of providing and replacing prostheses for growing children is a
cause of fûnher disability to child amputees (Machel, 1996; RUUNICEF, 199 1; UNICEF, 1990).
2.4.4 International Attention
The Gencva Conventions of 1949 addressed the issue of those disabled by war, but a new
concem for the plight of disabled children in arrned conflict was prornpted by the World Summit
for Children (Scptembcr 1990), and by an increased awareness of issues related to disability
emerging fiom the United Nations Decade of Disabled Persons (1 983 - 1992). In 1 Y 86, UNlCEF
became an outspoken advocate on this issue when it made "Children in Especially Dificult
Circumstances" a major focus (UNICEF, l!J86a, l986b, 1990). This included children who have
been physically and psychologically traurnatized by armed conflict or natural disasters. UNICEF
mobilized for the 1990 World Declaration on the SuMvaI, Protection and Development of
Children, which included a cornmitment by nations to:
... work to ameliorate the plight of millions of children who live under especially difficult circurnstances - as victims of apartheid and foreign occupation; orphans and street children and children of migrant workers; the displaced cfiildren and victims of natural and man-made disastcrs; the disabled and the abused, the socially disadvantaged and the exploited.
... work carefully to protcct childrcn from the scourge of war and to take mcasures to prevcnt fùrthçr armcd conflicts, in order to give children evcrywhere a peacefùl and secure future ... The essential needs of children and families must be protected even in times of war and in violence-ridden areas. We ask that pcriods of tranquillity and special rclief corridors be observed for the benefit of children, where war and violence are taking place. (UNICEF, 199 1, p. 56)
Days of Tranquility and Corridors of Peace were negotiated by UNICEF and other
agencies such as the international Cornmitter of the Red Cross, the WHO, appropriate ministries of
health, churches and non-govemmental organizations. These approaches were designed to allow

activities such as imrnunization programmes and the distribution of relief supplies during special
cease-fires, thereby demonstrating an overarching concem for the health of children. Such
strategies have been used successfully in El Salvador, Lebanon, Sudan and Iraq (Machel, 1996;
UNICEF, 1986b, 1990).
In November 1989, the United Nations (UN) General Assembly adopted the Convention on
the Rights of the Child (UN, 1989). In it, Amcle 23 asserts the nghts of mentally and physically
disabled children to dignity, active participation in the cornrnunity, and special care. Articles 38
and 39 outline the rights of children during armed conflicts, with respect to their recruitrnent and
protection, and the treatment of child victims. Building upon the Convention, in 1994 UNICEF
commissioned a study of "The Impact of Armed Conflict on Children," and its extensive report
specifically addrcssed the issues of landmines and disability (Machel, 1996). By 1996, UNICEF
had developed an explicit "anti-war agenda," which included a focus on relief and development
issues.
A special report of the United Nations Commission on Human Rights in 199 1 examineci
human rights and disability. This report recognized violations of hurnan rights and of humanitanan
law as factors causing disability, notcd the suRering inflicted on nonîombatants in situations of
armecl conflict or civil strife, and made particular mention of the situation of those with mental
disability (Despouy, 1991). Disabled Peoples' Intcrnational has pointed to the large nurnbcr of
disabilities tbat rcsult from illegal milita- operations, ill-treatrnent of prisoners of war, refusa1 to
attend to the wounded, and interference with the humanitarian action of civilians (citeâ in Despouy,
1991).
The United Nations High Commission for Refugees (UNHCR) has also addressed the
situation of disabled refugees (Crisp, 1989). In 1992, ü W C R published practical guidelines to be
usPd by their field officers, and others working with refugees, for prevention and treatrnent of
disabling conditions, as well as for rchabilitation (UNHCR, 1992). Areas of focus included

training, attitudes, suppon for disabled rehigees acting as leaders and workers, farnily support,
access and mobility, vocational training, education, and appropriate simplifieci rchabilitation
technology .
In 1989 the RVUNICEF Technical Support Programme conducted a review of the physical
rehabilitation needs of children and women victims of armed conflict, specifically in Angola,
Mozambique, El Salvador, Nicaragua, and arnong disabled Afghan refugees in Pakistan
(RXAJNICEF, 199 1). The report of this study identified how war causes disability, discussed the
magnitude of the problem, and directed attention to specific areas of concem (including needs for
accurate assessment, lack of tnined personnel, culturally-bascd concepts of disability, and equal
participation of disabled persons). Their recornmendations were aimcd towards generating
solutions; promoting cornmunity based rehabilitation, research and prevention, attention towards
women, children and mental disability, and the incorporation of disability issues into international
aid programmes for developmcnt and war and disaster relief.
Thus, various organizations have confronted the issue of disability under conditions of
political violence. nie Palestinian situation provides an example of rehabilitation issues bcing
addressed under circumstances of occupation and uprising.
2.5 The Palestinian Context
nie West Bank and the Gaza Strip are knowvn as the Occupied Temtories, or the Occupied
Palestinian Temtories. This refers to the areas bclonging to the pre-1948 British Mandate of
Palestine that were occupicd by Israel in 1967. Most recent population calculations identify almost
2.9 million Palestinians living in the Gaza Strip (30% of total population), the West Bank (60% of
total) a d East Jerusalem (10% of total) (Palestinian Central Bureau of Sbtistics, 1999; see dso
The Center for Poiicy Analysis on Palestine, 1992; FAFO, 1994).

2 S. 1 Political Violence
There is little doubt that Palestinians demonstrate a society living under conditions of
political violence. From ancient to modem times, the region has ben a place of regular invasion,
conquest and revolt. For Palestinians today, this century has been one of prolonged occupation - by Turkey until 1918, then by Britain until 1948, and then by Israel since 1948 (and, for sorne
Palestinians, by Jordan in the West Bank, and Egypt in the Gaza Strip, from 1948 to 1967) (for
chronology of events, see PASSIA, 1999). Those years of occupation also have been marked by
f u l l - d e regional wars in 1 948, 1956, 1967 and 1973. December 1987 marked the begiming of
the Pdestinian Uprising, called the Intifada (which in Arabic means "to shake off'). At the tirne of
this shidy, the 1993 Declaration of Principles had heralded "peace" between Palestinians and
Israelis, but despite the official end of the Intifada, occupation and resistance activitics continued.
Documentation of the character of Israeli occupation provided foreshadowing of future
troubles. Military administration and the establishment of Israeli settlements had broad negative
repercussions upon Palestinian persona1 status and rights, demographics, social nructurc,
ewnorny, education, and land ownership (Amri, 1983). Meron Benvenisti (1984) exmined West
Bank demography. economy, land use and owncnhip, legal and administrative concems, and Israeli
settlements, cntically analyzing the data in rems of lsraeii policy. Sara Roy's (1995) examination
of the political economy of the Gaza Strip also illuminated the role of lsracli policy and the grave
effects of occupation. Historical and political aspects of occupation provided the background for a
popular upnsing, as explained by Aronson (L990), as wll as The Center for Policy Analysis on
Palestine (1992), and the United Nations Cornmittee on the Exercise of the lnalienable Rights of the
Palestinian People (1 990).
During the Intifada, many organisations and the media reporteci upon lsracli human rights
violations in the Occupied Palestinian Temtories, but of note are two volumes published by the
West Bank affiliate of the International Commission of Jurists (Al-Haq, 1989, 1990). These

detailed violations related to the use of force, detentions, military justice, deportation,
aârninistrative methods of control, house dernolition, curfews, economic and fiscal sanctions, as
well as obstructions to medical care, education and wonhip, repression of organizational activity,
and actions towards women, human rights monitors, and the media. Further research and analysis
of the above issues, as well studies of non-violent civil raistance, and international, Israeli and
socio-histoncal implications of the uprising, were documentai by Hiltemann ( 199 1 ), Lockman and
Bcinin (1989), Nasser and Heacock (I991), and Peretz (1990). Garbarino et al. (1991) and Gibson
(1989) examined the violence with emphasis on the cxperience of Palcstinian children.
b can be seen that occupation and uprising affected vimially every element of Palestinian
life. It was inevitable thût health and disability would also expenence the impact of the conditions
of political violcnce.
2.5.2 Effects on Health
in their evaluation of thc impact of political violence upon public hcalth, Zwi and Ugalde
(1991) use the Palestinian Intifada to illustrate "teactive political violcnce". Initially, Palestinian
hcalth suffered as a result of restrictions by the militan, authorities on hçalth development
(Association of Israeli and Palestinian Physicians for Human Righrs [AIPPHR], 1990; Giacaman,
1984; Smith, 1987; Union of Palestinian Medical Rclicf Cornmittees [UPMRC], 1987). Early in
the intifda, the nature and extent of violence directly causing death and injury were investigated
and were welldocumented by Nison (1990), the international Commission of Jurists (Al-Haq
1989, 1990), and Physicians for Human Rights (1988). The indirect impacts on health of
occupation and uprising resulted pnmarily from dismpted immunization and prenatal health
programmes, curtailed food, water and sanitaiy service provision, and restricted or obstnicted
medical care (AIPPHFt, 1990; Al-Haq, 1989, 1990; Barghouthi & Giacaman, 1990, 199 1 ;
Bellisari, 199 1; Physicians for Human Rights, 1988; Rigby, 199 1 ; UPMRC, 1988).

2.5.3 Effects on Disabilitv
Studies of disability in the Occupied Palestinian Tcmtones have revealed a prevalence of
b e ~ n 2 % and 4.5% of the population (Brauelli, 1995; Central National Cornmittee for
Rehabilitation [CNCRJ, 1992; Giafaman, 1991, 1993; Giacaman & Haramy, 1996; Haramy et al.,
1 995; Jarrar & Giacarnan, 1 994), with a most recent national figure of 1.9% (Palestinian Central
Bureau of Statistics, 1997). Nonetheless, nearing the end of the Intifada, the CNCR (1992)
estimateci that 100,000 had been injured by violence, and 1,500 had bcen Icft wiîb permanent
disabilities requiring assistance.
The phenornenon of the Intifada-injured had a significant effect upon Palestinian attitudes
towards disability, introducing the notion of honorific injury, (Atshan, 1997; Mash'al, 1 990).
Mouna Odeh Salem (1 990) examined this intensively, drawing parallels with the Nicaraman,
Eritrean, and South Afncan Apartheid experience. This important change in attitudes gave new
energy to the Palestinian disability movcment (MacGrory, 1996; Salem, 1992) and prompted a
critique of the status of the human rights of Palcstinian persons with disabilities undcr Israeli
occupation (Gaff, 1994).
Early in the Intifada, Palcstinian rehabilitation efforts wcre largely understood and
fashioned in tems of physiothcrapy, although community care was oAen ernphasired (Ballantyne,
1988; Khamis, 1992-93; Krammer, 1990; Vandam, 1989; Verhoeff, 1989). By thc 1 WOs,
however, CBR had become the preferred approach for addressing disability, endorsed by the
CNCR and the United Nations Relief and Works Agency for Palestinian Refugees (UNRWA)
(CNCR, 1992; Coleridge, 1993, chap. 1 1; Forsby, 1995; Giacaman, 1993; Giacaman & Haramy,
1996; Haramy, 1993; Haramy et al., 1995; Jarrar & Giacarnan, 1994; Mendis, 1996; UNRWA,
1992). In their West Bank Rural Prirnary Heaith Care Survey, Barghouthi and Daibes (1993, pp.
324-25) documentcd three organizations providing CBR services, with the Union of Palcstinian
Medical Relief Cornmittees (UPMRC) CBR programme being the most extensive. The UPMRC

h;td undertaken to transfomi its physiotherapy services into a regional CBR programme (Mash'al,
1991, 1993; UPMRC, 1994).
Due to the crisis of the Intifda, CBR had been proposai as a means of addressing the
rehabilitation needs which ovenvheirned available seMces for people with disabilities (Giacaman &
Daibes, 1989). In 1990, however, Mouna Salem asked the question: "how effective will CBR be,
given the constraints in movement imposed by curfews, roadblocks, lack of sense of security, etc?"
@p. 89-90). The current study sought to answer such a question, by allowing the UPMRC CBR
programme partici pane to reflect u pon their experience under occupation and Intifada.
2.6 Relief and Development
Palestinian CBR was initially envisioned as non-govemmental organizations providing
assistance for people with disabilities (CNCR, 1992). Within the 1990s, however, there has been a
cntical re-thinking of how relief assistance should be provided to people sufiering under conflict
conditions (Adams & Bradbury, 1995; Anderson, 1993, 1994b, 1995; Bush, 1996; Commins,
1996; Eade & Williams, 1995; Minear & Weiss, 1993; Mooney, 1995; Weiss & Minear, 1993).
Belief that negative effects of relief interventions should be avoided, and that principles of
development should not be abandoncd, has led to the perspective which advocates greater balance
and less distinction between relief and development efforts. Non-governmental orpizations are
key acton in codict situations, and:
"the experiences of NGOs operating in such situations can provide a valuable base for helping other agencies to identiw development potential within confiict, to review their priorities and capacity for work in different settings, and to present policy challenges to governments and donors. Without an understanding of the ways in which development can and does occur in the midst of conflicts, NGOs will miss opporhmities to strengthen local communities." (Comrnins, 1996, p.8)
In discussions of relief and development, the work of Mary Anderson and Peter Woodrow
is widely cited and used to understand and promote community development in the context of

conflict and natutal disaster (see above works, also von Kotze & Holloway, 1996). Anderson and
Woodrow (1989) assert that any assistance made to communities living in conflict must not simply
provide relief, but must contribute to long-term development. In order to be developmentai, an
agency must recognim existing community capacities and wlnerabilities, and the assistance
provideci must strengthen capacities and d u c e vulnerabilities. To maximire benefits, and to avoid
negative impacts, agencies are encourageci to assess their target beneficiaiy communities according
to a framework callcd the Capacities and Vulnerabilities Analysis (CVA). Using the CVA
framework leads to an appreciation of community capacities and vulnerabilities in three rcalms:
physical/material, sociaVorganizational and attitudinai/motivational (see Appendix 1.). The CVA
can then be used for planning, implementing, and evaluating interventions in emergency conditions.
Anderson and Woodrow's CVA approach is straightfonvard, and is philosophically
attractive in that it shares CBR's focus on ability versus disability, of independence and
interdependence rather thm dependence, and of "participants" as opposed to "victirns." These
factors are in contrast with another possible theoretical framework for "sociological analysis of
collcctive stress situations" (Barton, 1969), which involves analyzing 69 complex interactive
eiements within a "therapeutic community response" (pp. 274-75). Therefore, Anderson and
Woodrow's Capacities and Vulnerabilities Analysis approach ww chosen to aid data analysis in
the WMRC case, because of its wide applicability in international settings, and its rclevance to
CBR.

CHAPTER 3
METHODOLOGY
3.1 Research Design and Rationale
The design of this research is a single qualitative case study. The unit of analysis is the
CBR programme of the Union of Palestinian Medical Relief Cornittees. A case study was chosen
because it i s a study which " investigates a conternporary phenornenon within its real-life context,
when the boundaries bctween phenornenon and context are not clearly evidcnt, and in which
multiple sources of evidence are us# (Yin, 1984; p. 23). Michael Patton (1990) notes that a
qualitative case study is "usefùl where one necds to understand some special people, particular
problem, or unique situation in great dcpth" (p. 54). The intent is to describe, reveal, and provide
an interpretive approach to understanding the meaning of expcricnces (Manhall & Rossman, 1989;
Tesch, 1990), by investigating a case that is "information rich" (Patton, 1990, p. 169; sçe also
Gilgun, 1994).
For qualitative case studies, Robert Stake differentiates between intrinsic case studics, in
which the importance of the Case is emphasized, and instrumental case studies, in which the
importance of the Issues is emphasized (Stake, 1995). In the current research, the case is the
UPMRC CBR programme, but the ei&t CBR elements (previously descnbed) have been uscd to
create the conceptuai framework for the issues under study. Thus, the study is instrumental, since
it follows Stake's recommendation whcn he notes "1 choose to use issues as conceptual structure - and issue questions as rny primary research questions -- in order to force attention to complexity
and contextuality" (Stake, 1995; p. 16).
A qualitative approach is therefore appropnate for the current study. Methods of analysis
have been established (Miles & Hubeman, 1984), and the rigour of the approach is accepte.
within rehabilitation therapy research (Jcnson, 1989; Krefiing, 199 1).

3.2 Location
The research took place in the Occupied Palestinian Temtories. West Bank locations
included the villages of Biddu, Aboud, Zabebdeh, and Ithna, the cities of Qalqilya, RamaIlah, and
Nablus, and the Jenisalem office of UPMRC. InteMews were also conducted in the Palestinian
Self-Rule areas of Icricho (in the West Bank) and within the Gaza Strip. Thcse representcd places
where UPMRC CBR programmes operatcd, or central meeting places for respondents. InteMews
were conducted in clinics, offices? and homes, according to respondents' preference and feasibility
for travel.
3.3 Data Collection
Data collection began September 12, 1994, and was concluded December 16, 1994. Data
was collccted by: 1) revicw of documents, 2) scmi-stnicturcd inteniews, 3) focus group
discussion, and 4) observation of rehabilitation activities and facilities.
Documents rcviewed includcd dozens of UPMRC CBR programme rcports, meeting
minutes, training curricula and activity schedules. In addition, the Palestinian public research
organiration, the Hcalth Dcvelopmcnt Information Project (HDIP), provided the researcher with al1
documents related to Palestinian disability and rehabilitation (approxirnately 18 publications), from
their comprchensive inventory. Documents in Arabic were translateci by cornpetent independent
translators. Documents (and interviews) provided information regarding the UPMRC CBR
programme history, structure, panicipants, activities, and strategies, as well as information about
the development of other Palestinian rchabilitation initiatives.
Therc were 18 in-depth interviews, each lastins approxirnately one to two hours. Most
were held with individuals, although on three occasions interviews were held with two respondents,
who indicated a prcference to be interviewed togethçr with their project team partners. Arabic /
English interpretation was required for three interviews, and \vas provided by colleûgues of the

respondents. Prior to conducting the indepth interviews, a pilot i n t e ~ e w was conducted with an
English-speaking CBR worker who had recently finished working with UPMRC. (The pilot
i n t e ~ e w was not subjected to analysis, nor included in study results.) As a result ofthe pilot
interview, the researcher appreciated the dual nature of political violence, and addressed both
Occupation and Intifada in upcoming interviews. Before bcgiming interviews, the researcher
consulted with UPMRC CBR managers regarding the suitabiiity of English terms to be used, and
some refinements were made (e.g., not using the word "collaboration" for cooperation arnong
organizations, as this term had negative political connotations). Similarly, afler the i n t e ~ e w s the
researcher sought clarification from local resource people regarding the meaning of certain Arabic
terms used.
During the intervicwvs, the researcher posed questions that correspondcd to the previously
identifid list of eight CBR elements (see Appendix II. for interview guidc). Respondcnts were
asked for their perspectives on whether and how the CBR elements were affected by conditions of
Occupation and Uprising, and how the UPMRC programme addressed each CBR elemcnt.
InteMews were audiotapcd (exccpt in two cases, at the request of those respondents), and notes
were taken during interviews. Aftenvards, the rescarcher transcribed tapes and notes.
There were 2 1 interview respondents, chosen as key infamants with guidance fiom the
actingdirector of UPMRC. A description of the respondents is seen in Table 3.1, with their
criteria for selection. There were fiftecn women and six men. One of the respondents was both a
CBR worker and a person with a disability.
AAer interviews were completed, one focus group discussion was held witb ten CBR
workers and one CBR manager. (The CBR manager and seven of the CBR workers had been
previously intervieweci.) The discussion vas organized for the convenierxe of workers attending a
regular weekly programme meeting, and was chaired by the rescarcher. During this discussion,
participants clarified and expanded upon earlier interview responses regarding their wvorking

environment. Specifically, they listed: the obstacles resulting from Occupation and Intifada that
they encountered on a day-to-day basis, the responses they made to each problem, and the positive
aspects of work under those conditions. Audiotape of the session was of poor quality, but notes
were taken on a flip-chait by the researcher during the discussion.
Table 3.1 Description o f Interview Respondents
Respondent category Number Reason for inclusion
Nine rehabilitation workers and four physiotherapists.
13 (Chosen fiom a total of 19 CBR workers, on thc basis of CBR workers lcngth and extent of their expericnce within the
I programme. Twelve women, one man.) l The UPMRC staff responsible for CBR programme
CBR managers 2 management. (UPMRC acting-director and CBR programme manager. Two men.)
Non-LJPMRC Palestinian CBR experts. (Chosen on the basis of their key roles in CBR developmcnt in the West
CBR advisors 3 Bank and in Gaza - two CBR p r o g r m e managers, one Community HealthKBR consultant. Two women, one man.)
From CBR programme participants, rehabilitation 1 PeopQ wiîh dirabilitier 4 workcrs, and the General Union of Palestinian Disabled. 1 (One woman, thrce mm.) I
Observation of rehabilitation propmrne activities and facilities, involving travel to the six
regional projects in the West Bank, providcd the researcher \rith context for interview data. The
researcher took the opportunity to accompany CBR workers at weekly team meetings and dunng
home visits, and to observe CBR activities at day care centres and clinics.
Additional interviews were held with representatives of rchabilitation institutions, of other
CBR programmes, and of international NGO supporters of CBR. These meetings took place in
Jerusalem, Ramallah, Birzeit, and Gaza. The discussions provided information on the broder
context of Palestinian CBR and wu also used to triangulate data received from UPMRC.

3.4 Analysis
Organization of data was facilitated by the ETHNO cornputer sofhvare (Tesch, 1990, pp
2 1 10222)~ and analysis proceeded with manual coding ( s e Miles & Hubenan, 1984, for
qualitative &ta analysis procedure followed). With a theoretical framework based upon the eight
elements of CBR, first level codes were initially fonnulated to refiect these elements, as well as the
experiences of political violence and CBR program activities. As transcribed data was coded, these
initial categories were supplemented and refined. Descriptive codes came to include contexhial
factors, such as culture.
During the second level of coding, or pattern coding, themes were developcd. For example,
individual expericnces of political violence (such as curfews, or the Intifada-injured) were grouped
into larger 'conditions,' and then differentiated into hvo major types (Occupation and Uprising).
Initially, while considering how elements were affected by conditions of political violence, a theme
of chonge ernerged. The data indicated that the role of the CBR workers \vas to create change,
specifically within the categories of the CBR elernents. With this therne as the orgmizing principle,
data was coded for barriers to change, strategies for change, and actions for change, related to
each element. Individual and community leveis of change were identifid. nie concept of change
was also attractive since UPMRC felt the purpose of CBR was not to develop a thing (a service),
so much as to affect a process. In addition, thc CBR programme had undergone significant
transfonation within a context of ongoing political and social change. Howvever, as change could
mean either improvement or detenoration, it became apparent that the themc of positive change, or
development, was more accu rate.
Simple diagranming of the sequence of conditions, elements and responses was made (see
Appendix III for data analysis tools) and the codes for a descriptive case were elaborated. A
sarnple of the code list is also found in Appendix III. Codes identified:

- the conditions of political violence,
- effects of the conditions upon the general work environment of the CBR workers,
- effects of the conditions upon each of the CBR elernents,
- the responses made to these effects,
- other influences, of the Palestinian context, upon the CBR elements.
Data was organired in files according to codes. These files were examined to assess the
content, fiequency, and weight of responses in each category. A consensus of opinion among
respondents became apparent at this time, and is rcflected in reporting of results. Using a series of
matrices to display the s u ~ a r k d data, important conditions, elernents and processes also became
evidcnt (see Appcndix III for an example of matrices created durhg analysis process).
At the next level of analysis, memoing was uscd to explore conceptual intcrprctations of
the findings. Explanations for the findings used the lens of community development to describe
CBR under conditions of political violence. The analysis drew upon a theoretical mode1 for
community devcloprnent that addresses the issue of providing assistance to communities in time of
crisis (Anderson & Woodrow, 1989). The concept of community development was consistent with
the philosophy of the CBR programme and UPMRC. The Anderson and Woodrow approach was
used to reflect upon the responses that the CBR programme made to conditions of Occupation and
Uprising.
3.5 Establishing Trustworthiness
Reliability and validity are tequisites that have been intçrpreted into the qualitative research
context, and as such they have been applied specifically to rehabilitation therapy research (Jenson
1989; Krefting, 199 1). Guba translates the concepts of reliability and validity into trustworthiness
(Krefiing, 1991). Using Guba's criteria of crcdibility, transferability, dependability and

confinnability, Krefting outlines procedures for establishing trustworthiness, and those methods
used for this case study research are as follows:
1. Credibility (tnith value)
'The researcher engaged with respondents, for three months during data collection and two
years during analysis and writing. Data collection methods and data sources were triangulated,
such that remarks that were challenged by other respondents (Le., in the focus group discussion) or
isolated remarks which were not supporied were not included in .he findings. IntcMew techniques
were consistent. (In addition, recognizing that English was not the first language of respondents,
the researcher used familiar English tcrms and simple language when necessary, whilc accuracy
was aided by the researcher havins adequate understanding of the Arabic uscd during translation.)
Processes, categories, interpretations and conclusions were checkcd by participants and peen.
Field joumaling aided self-rcflection.
2. Transfcrability (applicability)
An indcpth description of the case is provided for the reader.
3. Depcndability (consistcncy)
An indepth description of research methods is provided. Data collection mcthods and data
sources were triangulatcd. First- and second-lcvel coding wcre done by the researcher, and re-
coded to confirm categories after a p e n d of one to two months. Coding of two sample interviews
by an outside researcher also confimed the categories. The analysis process was under academic
supervision.
4. Confirmability (neutrality of data)
Triangulation of &ta collection mcthoàs and data sources was followved. Self-reflection
was continuous, and was aided by field joumaling. The research process was under academic
supervision.

3.6 Ethics
From Canada, entry to UPMRC was gained by written request made to the organization,
with submission of the research proposai, which included ethics approval from Queen's University.
In Jerusalem, both the researcher and the study were introduced to CBR workers by the UPMRC
CBR programme manager. Participation in the saidy was voluntary.
informeû consent to participate in the study was obtained from interview respondents, with
each respondent choosing to sign either the English or the Arabic fonn (see Appendix N. for
sample fom). The Arabic form was translated by the UPMRC translater, and accuracy was
confirmed by translation back into English by an independent resource person. At the outset o f
&ta collection, the UPMRC acting-director advised the researcher that the potential for a security
risk to participants, (resulting from exposure of their activities dunng politically-sensitive times)
had been eliminated by the changed political situation and peace initiatives of that time. There were
no refûsals to be intervicwed, atthough two respondents agrecd only on the condition of not bcing
audiotaped, due to their discornfort with that process.
Data was collected and analyçd by the researcher and maintained in confidcntiality.
Audiotaped conversations and field notes were transcribcd directly ont0 cornputer, and tapes and
transcripts were kept in securc storage during transcription and analysis. Transcripts were d e d
for the interviewee's name, and the master file of narnes and codes kcpt in a secure, separate
location. Tapes were then erased.
The researcher \vas required to e.uhibit sensitivity to the cross-cultural element of the
research. Previous expenence of living and working in the region, ongoing consultation with local
people, and common sense were her guide to rnaintaining appropriate behaviour.

CHAPTER 4
RESULTS
In this chapter, the results of data collection are presented. At the outset, thcre is a
description of the UPMRC CBR programme. Following this, the programme is further
contextualized by presenting factors that were noted to affect CBR in Palestine.
This background material is followed by a description of political violence and CBR. The
conditions of political violence of this case are outlined. Following this, there is a description of
how the conflict conditions specifically affccted the CBR workers of UPMRC in the day-to-day
performance oftheir duties. The remainder of the chapter is then devoted to assessing the impact
of the Israeli Occupation and Palestinian Uprising on CBR. In this assessment, the eight elements
of CBR are presented individually. For each one, there is a brief explanation of how the element
was demonstrated within this w e . This explanation is followed by a discussion of how the conflict
conditions affectai that element, and CBR programme responses. The presentation of results is
concluded with a final surnmary.
4.1 Description of the CBR Programme of UPMRC
Data for the following case description was obtained through document review and
discussions with CBR managers and advisors.
4.1.1 Evolution of CBR within UPMRC
The Union of Palestinian Medical Relief Cornmittees was established in 1979, in response
to inadequate health seMces provideci to Palesthians by Israeli authorities. At that tirne,
Palestinian physicians of UPMRC began offering primary health care services on a voluntary bais
to remote and unseniced areas in the West Bank and Gaza Stnp. Subsequently, village health

workers were trained, and medical, dental and laboratory services wre expanded. The
infrastnicture that underlay these widcspread health activities was covert, because these were ipso
facto in resistance to military rule. In 1986, prompte. by the unavailability of rchabilitation
seMces to people with disabilities in the rural areas, a physiotherapy component was incorporateci
into the medical services. The focus on rehabilitation was soon reinforced by the emergence of the
Intifada, which bcgan in 1987, since the high number of injuries increascd need for services and
raised the profile of disability in Palestine.
Thc physiotherapy programme of UPMRC evolved into CBR over the pars that followed.
Onginally, physiotherapy scnices were provided in selected regions. Therapists from Europe and
Canada were recruited and supported by international development NGOs. Village hcaltb workcrs
(VHWs) informally assisted the physiotherapists. Shortly thcreafter, UPMRC incorporated a
formal rchabilitation component into the VHW training. By 1990, UPMRC had adoptcd a CBR
philosophy, this being consistent with its primary health care focus and the community mobilization
of the Intifada. As the Intifada continucd through the early 1990s, transition to CBR occurred
within each physiotherapy project arca according to its oun regional chanctcristics and resources.
Most of the CBR projccts flourishcd, wvith rchabilitation workers trained and CBR teams created
for rehabilitation service dclivery and community development that addrcsscd disability.
CBR was explicitly endorsed by UPMRC and other NGOs in the Occupied Temtories.
International CBR activists, such as Einar Helander and David Werner, wçre invited to the region,
and their visiîs further promoted the CBR approach.
4.1.2 CBR in Palestine
With other rehabilitation providers and consumes, UPM RC was instmmcntal in forming
the Central National Conuniîîee for Rehabilitation (CNCR) in 1989, and integrating CBR into that

body's mandate. The aim of the CNCR \vas to build a comprehensive Palestinian rehabilitation
system. It was a forum of both institutional and cornrnunity organizations, and was particularly
important because under the Israeli military administration there existed no government support for
such programmes. Through the CNCR, rehabilitation activities were cmrdinated on a regional
basis. The four regions were the North, South and Central West Bank, and Gaza (with its own
Gaza National Cornmittee for Rehabilitation).
Community based rehabilitation programmes were implemented according to this regional
plan. Various NGOs took responsibility for CBR in each region, dcpending upon the organizations'
presence and previous activities. The NGOs that implemented CBR were local hcalth and
development organizations (such as the Red Crescnt Society and UPMRC), as well as Christian
and Islamic organizations and charitable societies. In this way, WMRC took a icading role in the
devclopmcnt of CBR in Palestine.
4.1.3 Thc UPMRC Programme
4.1.3.1 Organization and covcrage
Thc full orgmization of UPMRC constituted one of the largest Palestinian health NGOs,
working in all regions of the Occupied Temtories. lu pnmary h d t h a r c (PHC) componcnt
involved 28 community hcaith centres, with over 200 staff and 1000 volunteers. Its CBR
component was srnalier, but was nonetheless the most extensive Palestinian CBR programme. It
was active in 77 towvns and villages in the West Bank, representing a population of 200,000 people.
The position of CBR wvithin the UPMRC organization is indicatcd in Figure 4.1.

Figure 4.1 The Position of CBR within the UPMRC Organization
HK=
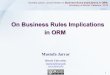
The CBR Programme was implemented through six regional project tcams. The catchent
area of these tearns is shown in Figure 4.2. This figure also illustrates the ho-part nature of the
Jenin project .
- i
I
, CBR
.

Qalqiliy
Biddu d Jericho
O Bethlehem
Figure 4.2 Map of the West Bank, Showing Catchment Areas of CBR Projects (shaded)

nie programme catchent area was extensive, though not al1 of the project areas had
undergone a disability survey, and therefore coverage Mas not cornprehensive. The number of
villages per project is shown in Table 4.1.
Table 4.1 Regional Catchment of CBR Tearns
1 Regional team Number of villages I 1 Biddu 9
Qalqilya 8
4.1.3.2 Participants and Linkages
The UPMRC CBR programme cooperated with Palestinian NGOs through CNCR, but it
also had other important links and pamerships. These are shown in Figure 4.3, and descnbed
below.

Figure 4.3 Participants and Linkages
b
r UPMRC - PHC
International md physiotherapy Speciaiists and partners institutions
Central National . Committee for
Rehabilitation
UPMRC Health care providers participated in the CBR programme through the
organization's PHC structures and personnel. Referrals were made through UPMRC
Peopk with disabili ties
village health workcrs, nurses, fmily doctors and specialists. The CBR programme was
also complemented by two UPMRC specialired physiotherapy clinics, each of which acted
as a referral centre. In Nablus, the UPMRC physiotherapy clinic initiated CBR work in
cooperation with the Palestinian Red Crescent Society, while in Gaza the physiotherapy
clinic cooperated with the CBR programme of the Gaza National Cornmittee for
Rebabilitation.
Institutions and outside specialists cooperated with the CBR programme, providing
medical, surgical and rehabilitation services.
Academic support

Academic support was provided by Birzeit University's Community Heath Unit, which
assistai the CBR programme with policy, planning, education, and research. Research and
logistical support Hpre dso provided by the Health Development tnfomation Project.
People with disabilities provided advice to the CBR programme and were represented
arnong the rehabilitation workers. The General Union of Palesthian Disabled (GUPD)
was supported in its formation by the UPMRC CBR programme, and maintained a close
relationship with UPMRC. UPMRC was instrumental in gaining forma1 representation for
the GUPD on the CNCR.
Community input to the CBR programme was characteristic of each project region
Regions differed in several characteristics (to be described later), and thus the degree and
nature of comniunity involvernent varied. In some cases, formal involvement occurred
through local heal th or rehabilitation committees, or other structures such as women's
committees. Community resources were also offered by merchants, teachcrs, craftspeople,
vocational training facilities, and conununi ty activists.
Partnerships were developed with international development NGOs, which provided
ongoing financial, persorinel, educational and moral support to the CBR programme.
These NGOs included the Organisation Canadienne pour la Solidarité et le Developpement,
Diakonia (Sweden), Gmppo Volontariato Civile (My), Nomsme (Noway), and the Third
World Relief Fund (Belgiurn). International governments and developmcnt NGOs were
the primary sources of funding for UPMRC's programmes.
4.1.3.3 Personnel
The Executive Cornmittee of UPMRC provided administrative direction to al1 programmes
within the organization, including CBR. The six CBR teams w r e supervised by the CBR
Programme Manager. This organizational structure of the CBR programme is shown in Figure 4.4

UPMRC Executive Cornmittee m ( CBR Programme Manager 1
Figure 4.4 Structure of the CBR Programme
At the time of this snidy, each of the reejonal CBR projects had a team of CBR workers,
compriscd of one physiothcrapist and a varying numbcr of rehabilitation workers. Nationality and
educational characteristics of thcse personnel are outlincd in Table 4.2. There werc 30 Palestinian
CBR workers, and 3 foreigners. The CBR worken were mostly women, and Uicluded people with
disabilities. While the physiotherapists were not from the regions in which thcy wvorked (with the
exception of one), the rehabilitation workcrs wcre local to their projects. Thc rchabilitation
workers had various backgrounds, including village health and social work. Thcy had undergone
their CBR training within a cooperative training programme with rchabilitation workers of other
NGOs.
Jericho T m
. Jenin Team
Qalqilya Biddu Team
Aboud Nablus J Team A Tearn J . Team

Table 4.2 Characteristics of UPMRC CBR Workers
1 Type of CBR worker 1
Training
NationaMy
University degree in Training through Swedish NGO Diakonia, physiotherapy7 foreign and local universities, using adapted WHO universities or Bethlehem rnaterials. (Cornrnunity development input University (three with UPMRC from UPMRC) scholarships)
Physiotherapists Rehabilitation workers (RWs) . 1
Palestinian and European Paiestinian
4.1.3.4 Programme Activities
CBR activities were carried out through home Msits, community programmes and resource
centre activities. In addition, the teams met weekly in a central location, together with the
Programme Manager, to share experiences, problerns and ideas, and to discuss plans. Table 4.3.
shows programme components in t e m of activities and with thcir main contributors.
Table 4.3 CBR Programme Activities - -
Location Act ivi t ies Contributors
ActiMties of Daily Living skills RWs, family membcrs, Home visits Social integration physiotherapists
Environment adaptations (e.g. home, school, workplace) RWs, physiotherapists, community
Cornrnunity Public and school education members, programme volunteers Media promotion Recreation activities
Day Care Centre: play groups, pre- RWs, children, family members, school education, mothers' meetings programme volunteers,
Resourcc: physiotherapists Centre
Physiotherapy: assessment, trament, Physiotherapists, people seeking referral consultation

4.1.4 Surnmary
In surnmary, the CBR programme of UPMRC evolved out of a primary health care NGO,
and this comrnunity health link remained strong. in addition, the programme was implemented with
the participation of several other secton of Palestinian society. UPMRC actively pursued a
national plan for rehabilitation in cooperation with other NGOs.
Funding for UPMRC operations was provided by international partners, but the
organization was proactiveiy reducing its reliance upon foreign physiotherapists. A combination of
professional and non-professional personnel promoted a community development mode1 for
disability.
Adoption of a communiîy developrnent philosophy 'nad caused the CBR programme to
mdie CBR training based upon the WHO rnodel. At the sarne time, CBR irnplementation
necessarily took into consideration the context of Arab culture, Palestinian regionai characteristics,
and local perceptions and approaches to disability .
4.2 Contextual Factors Affecting CBR in Palestine
There were several contextual factors that affcctçd CBR, in addition to those of political
violence. These were the factors of Palestinian culture, regional and community charactenstics,
professionalization and institutional ization of disability, and attitudes towards disabled people.
4.2.1 Palestinian Culture - Support and Authorih,
Respondents described Palestinian comunities as behg formed of "strong families,"
meaning that they were close-knit, with supportive, extended family structures. The strength of
fmily ties was considered to be a positive factor for CBR. At the same tirne, the traditional large
family size posed a challenge. Mothers were the primary caregivers, and they typically cared for

many children. Ttiis left them with limited resources of time, energy and money to devote to the
ne& of a farnily member with a disability.
Traditional Arab culture also maintained clear and separate roles for women and men, and
this was very apparent in villages. The rehabilitation workers (RWs) were mostly women, and werc
respected comrnunity members, which hcilitated home visiting to mothers and childrcn.
Nonetheless, the RWs occasionally faced censure from men in traditional homes. It was not
unusual for husbands to restrict the activities of their wives outside the family, and some feared that
the relationships developed between their wives and the RWs represented an undesirable outside
influence. A CBR worker described one husband's concems, saying, "he didn't want her to be opçn
on the life." Social segregation also influenced CBR such that public meetings on programme
issues were sometimes held separately for women and men.
Shared cultural values and religious beiiefs encouraged Palestinians to "hclp the disabled."
However, this widespread charitable approach was identifiai by respondcnts as undcnnining the
strength of people with disabilities. (This will be discusscd below, specifically considering aîtitudes
to disability). Family eldcrs sometimes took responsibility for making decisions about members
who were disabled, seeking help from respected local community leaders such as the sheikh of the
mosque, or taking the person to traditional healçn. In this context, CBR workers providd public
disability education that addressed the local traditionai practices and belicfs.
Respondents frcquently described Palesthian socicty as "hierarchical and authoritarian,"
and explained that this influenccû working relationships. A CBR worker larnented. "we are a
wmrnunity that you can't function unless you have somebody supervising you." It was noted that
efforts to work democratically in CBR occurred within a swiety that was neither egalitarian nor
democratic. It \vas also said that risid upbringing and schooling practices impeded creativity, by
discouraging expression and innovation among children. A CBR manager said that this negatively
afEected CBR, explaining, for esample, that "appropriate technology is dependent upon creativity."

Finally, respondents pointcd out that the philosophy of CBR implied working for change,
and change usually occurred slo~vly. A CBR worker, reflecting upon integration of people with
disabilities, comrnented, "we are a conservative socieîy, h t m a s it's very hard to bring social
change, on any level."
4.2.2 Reaional and Cornmunitv Characteristics - Geo-political and Econom tc Disparities
It was apparent that communities varied across the country, and respondents noted that
elements of CBR were strongly infl uenced by regional characteristics. ïhe main differences were
describeci between the regions of the North, South, and Central West Bank, and Gaza. and
differences were also mentioned between rural, urban and refigee camp settings. Ar; a CBR
worker reflected, "even we are one Palestinian society, but there arc small socicties within."
Within Palestine thcre were rcgional disparities of wealth and institutional resources for
disability. The Central region, with the cities of Jerusalem, Ramallah and Bethlehem, \vas notably
richer in econornic resources. With the advanbge of more rehabilitation services, integration for
people with disabilities was often easier in those cities.
Historical and geographical differences were also evident within CBR. Previous
govemment administration of Gaza (by Egypt) and the West Bank (by Jordan) was said to have
influenced their CBR programmes, in that the hvo Occupied Temtories had dinering concepts and
methods of administration and bureaucracy. Diffenng regional concentrations of refugee
populations also influenced community needs and CBR methods. This stemmed fiom refugee
camps representing politicizcd and organized groups, with their own mechanisms for receiving
health seMces from the United Nations. Finally, geographical differences were relevant to
accessibility and integration, as a CBR worker illustrated when commenting upon the challenges
posed to wheelchair users by the mountains of Nablus and the rough terrain of villages.

Communities differed rnarkedly in their degree of isolation, their scnse of cohesion, and
their leaden and activists for disability. A CBR worker provided an example of one town,
characterized by its few but very strong families, in which people al1 h e w one another and this was
reflected in supportive community participation in the CBR programme. In contrat, another
village made a CBR worker welcome only after years of slowly gaining trust through unobtrusive
home visits.
It is relevant to note that the factor of regional difference is not cornpletely independent of
the conditions of political violence. Palestinians shared similar expcnences of Occupation, but the
violence of the Intifada differed in nature and seventy across different regions and comrnunities.
Nablus, for example, was considered "hottcr" than Jcricho, in terms of violent resistance and the
number and profile of Intifada-injured. Accordingly, respondents in Jericho noted that attitudes
towards disability werc not changcd radically during the Intifada, as they had been in Nablus.
4.2.3 Professionalization and lnstitctionalization of Disabilitv - Privile- of Ex~crtise
Palestinian efforts to develop CBR took place against a backdrop of a medical mode1 of
disability, emphasizing services providcd by professionals and institutions. Mcdical professionals
were considered the cxpcrts and, uritil recently, the spokespersons for disability. A CBR manager
commenteci that disability had been "an able-bodied type of business." Families sought curative or
residential institutional care, and ofien expressed reluctance when first approached to engage in
CBR, being unconvinced that they should perforrn what they believed to be the role of a health
professional. At the s m e tirne, there were very few occupational therapists, speech therapists, or
special education teachers. Therefore there was reliance upon doctors, and upon a growing number
of physiotherapists .

The institutions and 'sheltcrs' for people with disabilities were frequently described as being
of exceptionally poor quality - lacking skilled staff', with "conditions like a prison," fostering low
levels of self-esteem and ambition among residents. Despite this, introducing the CBR approach
was still a challenge, since a change fiom reliance upon professional care was interpreted as a great
nsk. Indeed, a CBR manager confirmed that CBR was an innovation, and that UPMRC was
building a new and alternative mode1 for rehabilitation.
4.2.4 Attitudes Towards Peo~lc with Disabilities - Tradition and Charity
Respondents described attitudes (or "the mentality") towards disability that were generally
negative; feelings of shame, pity, and even hopelessness. The very descriptive Arabic word
"haraam" was fiequently used regarding people with disabilities. "Haraarn" invokes a great pity
and sadness towards a hclpless person - "Haraam, pity, pwr person, you have a disability, you
can't do anything." As one CBR workcr explained, "Our people, they ignore the disabled people.
They donPt take care of thcm. They don? think that they have needs like others. They don't like to
confess that they have disabled people. They feel asharncd from k m . "
Respondents noted that such feelings arose primariiy fiorn a lac& of knowledp about
disability. Farnilies oficn attributcd a child's disability to the mother, blarning her behaviour dunng
pregnancy (such as excning henelf, or eating certain f d s ) or for making herself or the child
susceptible to contagious illness (even a respiratory infection). However, disability was also
fkquently explained as God's will. In this sense, disability was understood to be a test of patience
and faithfulness, or, less ofien, a curse. In general, the causes of acquired physical disabilities were
better understood, while ignorance sunounding mental disabilities and epilepsy led ro fear, and to
p a t e r isolation for those with mental disabilities, multiple disabilities, andlor seizures.

Respondents aitributed the stigrna of disability to differences in personal appearance, but
also to the Fdct that disabled people were without a full role in society, particularly an economic
role. A family member with a disability was seen as a wegiving burden (especially upon the
mother) and a financial burden. A CBR manager reported this rationale: 'You don't want to have
them because they're a burdcn. It's a poor society, that camot afford to care for people who are not
producing."
Respondents' descriptions of isolation, neglect and abuse of persons with disabilities,
usually inflicted by farnily membcrs, reflected how disabled people wcre sometimes considered less
than human, unable to do anything, and nat counted as family mcrnbers. They were often hidden
inside the home, which was especially tme for wornen and girls, for whom outside activities were
already culturally restricted. Farnilies believed that if neighbours knew of thcir disabled family
member, this would lessen marriage oppominities for sistcrs. "There is fmr of hereditaiy
disability," explained a CBR worker. Outside the home, negative attitudes fostercd discrimination
within education and employrnent scttings.
At the samc rime, the cornmitment to care for pcople with disabilities, which arose fiom a
arong mode1 of charity, \vas responsible for many charitable socicties and institutions, devcloped
and sustained by the wealthy and the generous. lnherent in this contradiction was the attitude that
the individual was a poor person, deserving of pity and help because of al1 he or she could not do.
Activists within the disability movement expressed discouragement with how, even within their own
constituencics, a lack of awareness led disabled people themselves to accept the charitable model.
CBR workers pointed out that of course iiot al1 people, or families, were the sarne. Within
a society of negative attitudes towards disability, individuals and families varied in characteristics
relevant to their outlook on disability. Receptiveness, understanding, willingness, cooperation,
adaptability, commitrncnt and motivation were mentioned, with religion and education also having
an influence. CBR workçrs made such observations:

It's different fiom family to another family. Sometimes they have a handicapped person, and they have the money and they have the ability to help him, but mentally they refuse to hclp him. Oppositely another family she doesntt have any kind of money but she needs to help her child .... It depends on the mentality of the people here, and their education or cultural situation.
4.2.5 Summarv
Within the Palestinian contexq, some fhctots hcilitated the developmcnt of CBR, such as
tight-knit communities and extended families. In general, however, the contcxt could not be
mnsidered conducive to the development of CBR when consideMg the authoritarian aspect of the
culture, die yrevailing medical mode1 of disabilig, and negative attitudes towards disabled people.
While these contextual factors were similar to othçr Arab countries, political circumstances
for Palestinians were different. These political conditions led to a unique expenence of CBR, in
which dissatisfaction with the above negative factors could be raiscd and rnobilized within an
atmosphere of social change.
4.3 Political Violence and CBR
4.3.1 The Conditions of Political Violence
Respondents described wo types of political violence: that imposed by the occupying
Jsraeli forces, and the teaction by Palestinians. The resulting conditions were generally referred to
as "Occupation" and "Intifada." niese conditions occurred simultaneously during the period
considered by tbis research.
It was also common for the words "Occupation" and "Intifada" to refer to periods of tirne,
with the former existing h m 1967 onwards, and the latter existing from 1987 until 1993.
Therefore, to avoid confusion, 1 refer to the conditions as "conditions of Israeii repression" and
"conditions of Paiestinian resistance."

The following conditions m r e commoniy identified by respondents as being relevant to the
developrnent of CBR. Thcy do not represent a comprehensive list of conditions of political violence
that were experienced at this time.
4.3.1.1 Conditions of Rcpression - The Occupation
Israeli authorities utilized a number of strategies to impose and maintain militas,
occupation.
a) Military administration of the Palestinian population.
Palestinians' livcs and affairs were govemed by Israeli rnilitary rule. With no self-
govcmance, there was a lack of social assistance programmes for the necdy, no control of
govemrnent education facilities, inadequate education funding, no control of govemment health and
rehabilitation services, and govemment health insurance that was both expensive and arbitrarily
adrninistercd. Lack of self-govemance contributed to Palestinian econornic underdevelopment, de-
development, and economic depcndence upon Israel. Palestinians cxperiçnccd high Icvels of
unemployment, and reliance upon "cheap labour" jobs in Israçl. Ultimately, poverty was the result.
This was combincd with inadequate government hcalth and rehabilitation senices, insufficiently
bolstered by health and social seMces that were provided &y NGOs in a fragmented manner.
b) Population dislocation.
Al1 regions in which the CBR programme operated had populations of Palestinian refugees.
These refugees were from areas that came to be within the state of Israel, and many still lived in
camps that were established aAcr the 1948 war. Basic services were provided to them by
UNRWA.
c) Administrative bamers.
The primary barrier was the requirement to attain written permits (called "permissions")
from the Israeli Military Authonty offices of Civil Administration. These included: permissions to

travel; permissions for CBR workers or children with disabilities to enter, attend or make
environmental adaptations within a schooi; licemes to open and operate a business. There were
many bureaucratic obstacles to aquiring permissions. Travel restrictions were enforced through a
cornplex system of colour coded identity car& (IDs), which were carried by every pcrson. Other
administrative bamers included taxation that was irnposed to inhibit development of business and
industxy.
d) Policies of civilian control and punishment.
These includcd closures and curfews, which were enforced by checkpoints and Street
soldicn. Restrictions were placed on movemcnt within and between the West Bank and Gaza, and
imluded long-term closures of the temtories. Control and collective punishment were also imposed
through school closures, blockades of roads and building entrances, house dcrnolitions, and land
cmfïscation. Gatherings of people were forbidden, and there was limited access to the mass media.
People were detained or arrested under a variety of military orders.
e) Violent military actions.
These differed from the above in that they were violent acts by Isracli soldiers, though
actually encouraged by officia1 policy. Actions against al1 members of Palcstinian society hcluded
shootings, tear gas use, forced entry, beatings, anests, threats, humiliation and harassment.
Soldiers used these actions against individuals and families, in homes, in public, in places of work
and education, and in clinics and hospitals. Violent actions resulted in injuries, disabilities, and
deaths. Medical problerns and disabilities were also found among released prisoners.
4.3.1.2 Conditions of Resistance - The intifada
The Paleainian people, acting as mernbers of organizations or as individual civilians,
responded with a vanety of strategies and actions.

a) Non-violent community resistance activities.
Resistance to Occupation coalesced into volunteer comniunity mobilization, beginning in
the late 1970s and the 1980s. Grassroots movements were fonned, for the purpose of organizing
social structures and services (for example, in economics, health, agriculture, women, culture, and
education). These movements accelerated dunng the hifada, with neighbourhood and national
cornmittees (NGOs) being cstablished. Non-traditional leaders ernerged, such as youth and women.
Non-violent resistance was also demonstratcd by acts of civil disobedience (for example, operating
a c h i c without a iiccnse), strikes, dcmonstrations, and the Israeli product boycott. However,
because motivation for nacional resistance was high, groups that espoused disparate political
affiliations crcated thcir otvn cornmittees and NGOs, along party lines. This factionalism within
community mobilization led to cornpetition for the peoples' loyalty and for ouüide resources.
b) Violent resistance actions.
The most cornmon form of violence \vas stone throwing, which was primarily camed out
by Palcstinian youth and children against Israeli soldiers. Stones were also throtm at settlcrs,
whose vehicles had yellow licensc plates (signi%ng Israeli or Jerusalem registration). There was
less fiequent use of gas bombs and fireams, resulting in injury, disability and dcath.
C) Escalating injury and disability of the Intifada.
Injuries were inflicted by Israeli soldiers pnmarily through shootings and beatings. These
usually, but not aiways, occurred during rcsponse to both non-violent and violent resistance
activities. Medical facilities and communities stniggied to cope with acute demands resulting fiorn
severe traumatic injuries and a sliarp risc in disability.
The "Intifada-injurcd" were in one sense a result of rcpression and resistance conditions,
yet Palestinians considered them to be far more than a group of casualties. They becarne a symbol
of resistance and a catalyst for further resistance due to their nurnbers and their status gained
through self-sacrifice. It a a s often said that every family had an Intifada-injured member.

ci) Intemational support.
The impact of international support was so significant that it became part of the social
fibric for the respondents. In this way, international aid and endorsement was more than simply a
consecpence of the political situation. UNRWA had been providing education, fôod and health
seMces for registered Palestinian refugees since 1948. Throughout the Occupation and
increasingly during the Intifada, the international community responded to the Palcstinian crisis
with relief and development assistance, often as expressions of political solidanty. Worldwide
publicity of Intifada-injuries stirnulated a sharp rise in support for rchabilitation initiatives,
including donations of money, equipment and technical expertise. International support spurred
institutional and cornrnunity rehabilitation programmes.
4.3.1.3 Summary
Aithough the repression conditions were severe, they were countered on a social and
motivational level by the resisîance atrnosphere. This interaction between repression and resistance
had widespread repercussions on social and community development in Palestine, affecting the
environment for CBR work and the actual development of CBR elements.
4.3.2 Effects of the Conditions of Conflict mon the CBR Work Environment
Working conditions of al1 Palestinians were very much afTected by the conditions of
political violence. The CBR workzn' daily duties revolved around such activities as home visiting,
public education sessions, cornmunit). and team meetings, and contacting refera1 agencies. Under
the circumstances of conflict mentioned above, there were significant persona1 and logistical issues
to be managed in getting CBR work done.

4.3.2.1 Conditions of Repression - Bamers and Threats
Since the CBR workers' duties involvexi accessing people with disabilities within the
community, the prime obstacles to their activities were the travel restrictions from checkpoints,
curfews, ciosures, permanent road blockades, and stri kes. Thesc were cornmon and m u e n t
hindrances in al1 regions.
CBR workers remained wlnerable to military actions even afier managing to rcach their
work setting. CBR team workers, like al1 mernbcrs of the community, were subjected to
harasment, threats, and use of tcar gas by soldiers. In addition, it was reported that soldiers on
occasion entered clinics and stopped CBR work.
Regular CBR activities were frequently precluded by disruptions ansing from the
Occupation and Intifada. When an arrest was made within a family that the CBR team visited, the
family was distrcsscd and pre-occupied. Whcn a villager w u killed, demonstrations and curfews
followed. Thcn,when the curfew !vas lifted, mcrnbcrs of the community, including the CBR
workers, set aside rcgular activities and sat in condolence with the farnily for several days,
according to custom.
4.3.2.2 Conditions of Resistance - CBR as Soiidarity
UPMRC7s programmes, and other NGO health initiatives, were pan of a cornmunity non-
violent resistmce strategy. Thus, despite the above dificulties, CBR workers remarked that a
sense of cohesion \vas fostered as they worked together, sharing successes and failorcs under
adverse circumstances. They described their own heightened self-rcliance, creativity and pride, in a
job ba t offered great challenge and interest due to the hardship. In addition, CBR workers
perceived that they demonstratcd thcir solidarity wvith the overall Palestinian political stmggle by
helping the Intifada-injurcd. As one worker explained, "we are part of them."

Violent community resistance rarely affected the CBR work. Occasionally CBR workers
who used cars with ycllow license plates (which indicated lsraeli or Jerusalem registration) risked
having their vehicln stoneû, if they were mistaken for Israeli settlers while driving through the
West Bank. This was rare, however, as the CBR workers became well hown within thcir districts.
4.3.2.3 Responses of CBR Workers - Belonging and Adapting
In response to the rnany travel restrictions imposed by thc Occupation, the CBR workers
adapted their methods of travel. Using their own initiative and knowiedge of their cornmunities,
CBR workers eventually ovcrcamç most restrictions with a combination of techniques, such as
avoiding checkpoints by using altemate routes, circumventing long lines by using yellow license
plated cars, or negotiating with soldiers to gain their way through.
In response to thc risk of stoning, the CBR workers adaptcd their rncthods of travel. Those
with ycllow-platcd cars rclied on siçns that idçntificd them as Arab drivcrs, which werc wcll
undc r s td within the cornmunity. These included placing a kirfi-ve (Palcstinian traditional scarf) on
the dashboard, and exhibiting "Medical Relief' signs in Arabic and English.
In responsc to military actions and vioience, the CBR workers expandcd thcir rolcs, botb as
comunity members and as UPMRC staff. They providcd social support to affected families, and
they assisted at the PHC clinics for the emergency medical needs that resultcd during disruptions.
4.3.2.4 Summary
The conditions of repression creatcd a very challenging environment for the CBR workers,
providirig obstacles and disruptions to their daily duties. However, these trials reinforced the view
that CBR was in solidarity with the Intifada, and participation in community rcsistance provided a
positive motivating aspect to the work. Overall, CBR workers adapted to their work environment

through flexibility, innovation, and role expansion. At the same t h e , howvever, the conditions of
confiict had significant impact upon vanous elements of the CBR programme itself.
4.3.3 Effects of Political Violence on CBR Eiernents
4.3.3.1 Promoting Positive Community Attitudes towards Disability and People with
Disabilities
Respondents stressed CBR's emphasis on creating positive and lasting changes within
cornrnunity beliefs, kelelings, and behaviours towards people with disabilitics. LJPMRC
incorporated this goal into al1 aspects of its CBR activities, fiom CBR worker interactions in the
home and neighbourhood, to policy directions taken by the organization. This reflected the
community development aspect oFCBk in that attitudinal change was at least as important as the
provision of rehabilitation services.
4.3.3.1.1 Conditions of repression - Sustaining negativity
Occupation was noted to negatively affect the promotion of positive attitudes towards
disability, in two ways. First, respondents noted that the severe economic repercussions of
Occupation caused both families and society to relegate disability concems to a low priority.
Negative attitudes towards people wvith disabilities were arnplified because of the financial burden
of their care on families who already experienced economic hardship.
Secund, policies oCOccupation hindered CBR efforts to improve attitudes. Restrictions on
public gatherings and lack of access to the mass media obamcted public education activities of
people with disabilities and the CBR tearn. Also, special permissions were required fiom the
authorities for the CBR team to enter the schools for public disability awareness and education. It
was a difficult process to obtain permissions, and they were rarely granted.

4.3.3.1.2 Conditions of resistance - Catal yst for change
In contrast to the above, conditions of resistance positively influenced CBR's promotion of
positive attitudes. The symbolism of the Intihda-injured and non-violent community resiçtance
each played significant roles.
Respondents widely reported that public consciousness of the Intifada-injured improved
attitudes towards disability. The Intifada-injured were called a "wake up" to socicty, and a
stimulus towards disability awareness. Whereas they were previously hidden, peuple with
disabilitics became suddçnly far more visible as a result of the large number of Intifada-injured.
They wcre also proud to be seen in the streets, for society considered them "heroes" who had
acquired their disability through personal sacrifice to the political cause. A CBR advisor
expiainai, "Because of the passion, and the confrontation, and the heroisrn of w h t Our young
pcople passed through, and they became disabled aAer their injury, aficr ihcir beating, after their
shooting - sa, they became aware that the disability is some kind of honour for thcrn."
Signifimtly, respondcnts with disabilities declarcd that the statu of the Intifada-injured
markedly improved attitudes ivithin the disability community itself. ïhis was echoed by a CBR
advisor, who said, "The most important change has becn in the gradua1 shifi in the attitudes of the
disabled themselves."
In direct response to conccm for the Intifada-injured, local and foreign contributions were
made to improve institutional rchabilitation services, which ultimatel y bencfitted al1 people with
disabilities. A CBR worker noted that this lcd to a broader perspective towards disability amongst
health and rehabilitation workers. This "new, open-rninded" approach to disability, which was
introduced by foreign rehabilitation initiatives, was noted by a CBR manager to have provided an
impetus to attitude change within society.

Esteem for the Intifada-injured, however, did not simply convert negative attitudes towards
disability into positive oncs. A CBR worker rematked of people's feelings towards the heroes,
"They give them this status, but ioside they are feeling vezy pity, very sad." Though sorne
respondents claimed that al1 people with disabilities benefined to the point of being considered
qua1 to the "heroes," most respondents noted that the status of the injured induced a fom of
discrimination between categories of disability. Thus, it was suggestcd that people with disabilities
gained unequally fiom the positive changes in society. One CBR manager assessed the inequality
by saying, "It dwsn't give any kind of advantage to those who are not Intifada cases, in terms of
their position in the community, of the perception of people towards hem, which reflects their own
self-esteern and their own self-redization." Similarly, a CBR advisor expressed reservation; "1
dont know how much attitude has changed gencrally, within Palestinian society." Overall,
respondents prcsented a balanced optimism regarding the long-tcrm cffcct of the Intifada-injured
upon society's attitudes.
At the same time, non-violent resistance of the Intifada charactcrized by widesprcad
community mobilization, positively affectcd the CBR team's ability to affcct change in attitudes.
Respondents said that the spirit of resistance and grassroots activisrn made society more responsive
and less rigid. Responsiveness and ddmamisrn facilitated comunity work, in this case the CBR
initiatives towards raising populûr awûreness of disability issues. Thus, a CBR manager said this
aspect of the work was made easier d u h g the political cnsis: "lt's easier. It's not more difficult.
Easier because people are more mobilized, more able to perceive, more positive in terms of reaction
to initiative, and more socially linked, interactive.. . . Bccause you are talking about resistance herc."
4.3.3.1.3 CSR programme responses - Building upon awareness
In response to the hindnnces nhich Occupation policies placed upon initiatives to improve
attitudes, the CBR team adûpted its methods of accessing community members. People were

contacted individually or in srnall groups, outside controlled locations and governmental
organitations such as schools.
In response to the genenlly positive attitudes towards the Intifada-injured, UPMRC
adapted its CBR mandate by expanding its focus to include the Intifada-injured within their rural
rehabilitation work. They joined with other Palesthian organizations in publicizing the political
cnsis affecting health and disability, including the situation of the Intifada-injured. Capitalizhg
upon improved awareness and attitudes, bey acquired and distributed benefits equally to children
and adults with disabilities, without prefercnce to the Intifada-injured. At the same time, CBR
workers adaptcd their methods of working with the Intifada-injured, in light of thcir new status.
CBR workers encouraged individuals by reminding them, "You are respectcd by al1 the community,
and you have rights."
4.3.3.1.4 Sununary
While repressive conditions of Occupation helped to sustain prevalcnt negative attitudes
towards disability, the lntifada had a great impact towards tmnsforming hem. Cornmunity
mobilization, which encouraged public disability awarcness initiatives, was no doubt important, but
the esteern in which the Intifada-injured were held was key in improving attitudes. It was clear,
however, that a tmly far-reaching impact was undermincd by general society's emerging distinction
between the herocs and other people with disabilities. Nonetheless, positive changes in attitude
were substantial within the disability cornrnunity and among those working with people with
disabilities, which was an auspicious beginning for the development of positive community
attitudes to disability.

4.3.3.2 Promoting Integration of People with Disabilities within Society
The second element of CBR is strongly linked to the first. Positive attitudes are a first step
towards the integration of people with disabilities, and integration may be an indication of positive
attitudes. Integration is the process of becorning active within society, particularly in assuming
accepted roles within the fmily, school, and workplace. The UPMRC CBR programme
emphasized that society should become inclusive of people with disabilities, not simply expect
people with disabilities to lcam skills for adapting to the status quo. At the same tirne, integration
was also influenced by the availability of adaptive equipment and medical rehabilitation services,
which will be considered in the final hvo CBR elements.
4.3.3.2.1 Conditions of rcpression - Blocking employment and education
Repressive conditions invariably had a negative effcct upon the integration of people with
disabilities within society. Specifically, travel restrictions, economic undcrdcvelopment and
unemployment, administrative barriers and military administration werc idcntifiçd by rçspondcnts
as inhibiting factors to integration.
Travel restrictions scriously hindcred the abilil of people with disabilities to be active
outside the home, to gain access to jobs, and to meet togcther. Vocational training and employment
were often available only outside their o\vn villages, and CBR workers fiequently notcd that those
with disabilities had fcwcr and lcss flesi bfe options for transportation. Furthemore, people with
disabilities descnbed their dificulties in meeting togcthcr to create disability organizations, citing
problems in gaining petmissions to travel, in extra travel required to avoid closed areas, and
harat ion in having to continuously alter $iris in the face of curfcws and disruptions.
Although high unemployment affected the entire population, people with disabilities were
noted again to be particularly hard hit. Obstacles sternming fiom negative attitudes and
inaccessibility meant that options for gainfil emplo.ment were fewer. In addition, most jobs open

to Palestinians in Israel were noted to be in rnanual labour and construction, which were unlikely to
be offered to people with disabilities.
For disabled children, administrative barries pose. a significant bar-ier to integration by
limiting access to govemment schools. Regulations required headrnasters to show that speciaI
permissions fiom the Civil Administration had been aquired by the parents. As noted earlier,
while permissions could be obtained, the process was long, difficult, and fiequently unsuccessfiil.
Within the Civil Administration, bureaucrats created obstacles to obtaining al1 permissions.
A CBR worker described how the appropriate authority would absent himself repcatedly when he
was approached to receive applications. Another CBR worker described how a rnilitary official
had denied permission for a child's entry into a regular classroorn. In that case, the official had
simply stated that regular school tvas unsuitable for a disabled child and that she must find a
special school in the Central rcgion.
Likcwise, for structural adaptations to irnprove physical accessibility, and for the CBR
workers to assist teachers with integration of children, the same bamer was encountercd. A CBR
worker explained, "it was difficult, in some places it was evcn impossible, to entcr schools, because
we need to have a special permission." Finally, schools suffered from a lack of education fùnding,
equipment and support, so that teachcn were largely unable to absorb students with extra needs. A
CBR worker concludcd that for those reasons, the disabled child "tvill cnd up swing at home."
Integration \vas also affected by military administration, undcr which there were no laws
regarding nghts for people with disabilitics. CBR workers expressed the need for mandated
disability rights and services, for example the right to accessible schools. Military rule precluded
irnplementation of disability legislation that had been draAed by Palestinian lcgal and human rights
advocates. Respondents cited this powerlessness as contributing to the maintenance of
discrimination in tmsportation, ernployment, education, and accessibility. At the same time,
Palestinians were becoming aware of the legal protection and broad social assistance available to

people with disabilities in Israel. Respondents noted that cornparisons with Israel elicited various
reactions, ranging fiorn discouragement and bittemess, to a cornmitment to create similar
advantages for Palestinians .
4.3.3.2.2 Conditions of resistance - Deserving a place
In c o n t r a to the above, the status of the Intifada-injured positivcly affected integration.
The number and the pnde of injured persons made disability more visible, and respondcnts
observeâ that society came to accept that people with disabilities would assume the social roles that
were available to non-disabled people. One CBR worker noted how segregation was confrontai,
saying, "You don't isolate the hero. On the contrary, he has to be a good example for the society."
Respondents noted that being injured in the Intifada allowed people with disabilitics to become
contributing members of their fmilies, highly visible on the streets, and active within schools and
universities. This in tum encouraged the same participation from other pcople with disabilities.
The Intifada-injured were usually young men, previously able-bodied and active, who were
a syrnbol of strcngth and, owing to their self-sacrifice in resistance, were considered entitled to
demand accommodation by Palestinian society. They sparked the development of the General
Union of Palestinian Disabled, whose membcrs said that the improved awarcness and attitudes
encouraged by the Intifada-injured "aimulated us to move." With this catalyst, the GUPD set out
an agenda that focused upon disability iegislation and integration issues. For example, despite the
lack of legal requirements for making public places accessible, new construction began to
incorporate these features after the GUPD, which formally represented disabled people, approached
the leaden of municipalities and educational institutions.

4.3.3.2.3 CBR programme responses - Advocacy and support
Many of the obstacles to integration irnposcd by the Occupation, such as economic
restrictions, were considerd beyond the CBR programme's ability to address. However, in
response to administrative bamers, CBR worken stressai their advocacy role. With families, they
penisted in applying to thc Civil Administration for school permissions. In addition, CBR workers
approached school personnel, outside the school buildings and on a personal basis, to support the
cases of individual childrcn.
LJPMRC also rcspondd to lack of legislative ability, at the same time capitalizing upon Ùie
momentum created by the Intifada-injured within the disability movemcnt. UPMRC incorporated
within its mandate a strengthcning of the GUPD, and this was camed out at both UPMRC's
administrative and local levels. For exarnple, UPMRC used its position among hecilth and
rehabilitation NGOs to endorse the full status of the GUPD on the CNCR. Regionally, the CBR
workers facilitatcd development of local branches of the GUPD. Thus, UPMRC acted both in
response to the disability movement, and in direct support of its formation. Mcmbers of the GUPD
identified extensive UPMRC logistical and moral suppon, both in public and in private, sayuig that
CBR was its "first fiend."
4.3.3.2.4 Sumrnary
The repressivc mcasures of Occupation had a marked detrimental impact upon integration,
especially within the ernployment sector. In the face of serious restrictions and economic
challenges, the CBR programme lacked successful measures to achieve integration in the
workplace. However, the conditions of rcsistance, chanctenzed by impetus from the
intifada-injured, assisted the CBR programme and the new disability movement to make gains in
the integration of people with disabilities, notably into family and social life.

4.3.3.3 Transferring Rehabilitation Knowledge and Skills
This element was undcrstood as the training function of C B S which involved teaching
people with disabilities and their family members how to utilize rehabilitation principles and
exercises to achicve hproved phy sical and social hinctioning. Transfer of knowlcdge and skills
was particularly emphasized by the CBR workers, who were intensively involved as trainers on a
&ily basis, mostly during home visiting.
4.3.3.3.1 Conditions of repression - Unable to deter
Interestingly, repressive conditions were not notcd to impcdc the transfer of rehabilitation
knowledge and skills, once the CBR workers were able to reach the home. One CBR worker made
this clear: "When it cornes to this, there is no direct effect of the Occupation. Thcy cannot corne
inside the housç with a frunily and prevent us, the rehabilitation worker, from teaching the skilts to
the family. They cannot do this."
4.3.3.3.2 Conditions of resistance - Motivation for independence
Upnsing conditions had a positive influence upon rehabilitation training, though indirectly?
in the sense that those disabled du ring resistance activitics had a high motivation for regaining
independence. Since both the Intifada-injured and their socich, interprcted their injuries as hcroic,
they gained a scnse of power and a will to rctum to society. A CBR workcr detailed how many
Intifada-injured young men, aAer an initial pcriod of shock and depression, wantcd to reassert their
strenyi: 'They want to prove that they are still strong, and they can still be a member of the
society with the same power .... The role now is how to go back to society with the maximal
capacity. And you will see them learning so fast Very quickly, and they are willing to leam."
It was also suggested, though by few respondents, that the cornmunity mobilization of non-
violent resistance may have assisted self-help initiatives in which there was a transfer of knowledge

and skills. The general spirit of self-reliance was thought to have enhanced people's receptiveness
to training that could lead to greater independence.
4.3.3.3.3 CBR programme responses - A political spirit
Responding to the ideal of Palcstinian self-reliance, CBR workers linked the transfer of
skills with self-sufficiency. They encouraged people with disabilities and their families to use the
education and training resources that the CBR programme offcred, implying that a spirit of
independence was irnperative within the political circumstances. A CBR worker said that she
asserted this during home Msits, when she would Say: Who else will do this for you? Because no
care is provideci to us, you must do what you can on your own.
4.3.3.3.4 Surnmary
Other than hindranccs to tnvel, which the CBR workers generally overcame, thc training
element was not significantly affected by the conditions of repression or resistance. Cases of
Intifada-injury werc not predominant within the CBR programme, so thcir overall influence upon
this element likely was limited. Other reported positive cffects of resistance were not widely
endorsed.
4.3.3.4 Providing Participant-Directed Rehabili~tion Services
UPMRC CBR services were available in each regional project, and included physiotherapy
assesment, disability education and training, assistance rvith acquiring equipment, refenal, and
support in dealing with public and rnilitary authorities. This CBR element reflected the ability of
programme participants to express their disability needs and thereby direct rehabilitation services.
During in te~ews, this concept rvas contrastecl with situations in which predetenined seMces
were imposed, based only upon the prionties of service providers.

4.3.3.4.1 Conditions o f repression - Learned helplessness
Respondents suggested that political powerlessness expcrienced while living under military
administration had resulted in Palestinians being unprepared in general to define their own needs,
and to initiate, plan, and control their lives. This was also true for disability ne&, an4 despite the
awarcness of some people with disabilities about the disparity of services betwecn Israelis and
themselves, many Palestinians ~vcrc ignorant of what services could be made available. A
respondent with a disability cornmented that the military authontics ignored rehabilitation issues in
order to prevent social development: 'They like the situation as it is: people are not aware of what
they need."
4.3.3.4.2 Condirions of rcsistance - A stronger voice
The Intifada stimulated a powerful awarencss of disability and rehabilitation neais, which
gave an opportunity for these to be esprcssed. At the individual level, the Intifada-injured were
considerd entitled to make demands of rehabilitation services. A CBR manager illustrated this,
emphasizing integration issues:
Now, the Intifada has brought a stronger pcrson. The stronger person is a penon who hm faced soldiers. He is arong in that, so why not to look at him also as strong person while he is disabled? ... So they started to speak out, even to speak out about their necds - 1 want a wheelchair. 1 want to go back to my university. 1 want to go back to the school.
At the organizational level, new international support brought sophisticated rehabilitation
faciiities and equipment. While these institutional services were ultimately available to al1 people
with disabilities, priorities were initially set in Palestinian society for the care of the
Intifada-injured. Thus, spccial arrangements which were made for those injured by violence
reinforced thcir status, and meant that they were more likely than other disabled persons to have

their rehabilibtion needs met. A CBR worker stated the situation simply, "Because of the Intifada,
if they need somcthing for disabled person they know that they'd get it. They keep asking for it."
4.3.3.4.3 CBR programme responses - Pragrnatism and vision
In reaction to the disability needs of the Intitada-injured becoming a priority over others,
the CBR programme adapteci its mandate to balance the interests of both groups. Howevcr, a CBR
manager noteû that the programme wvas "aware of the fact that people with Intifada-injury need
certain amount of cxtra a re , because of national reasons mainly. Political rcasons." Thcrefore,
although UPMRC explicitly identified the Intifada-injured as beneficiaries, it continucd to channel
resources primarily towards rural areas and cliildhood disability. In addition, UPMRC sought to
know, addrcss, and balance both the long-term strategic needs and the shon-term imrnediate needs
of those receiving services.
4.3.3.4.4 Summary
In addressing participants' direction of services, respondcnts focusscd upon how
Occupation and Uprising afEected people's knowledge and expression of their needs. The ability of
Occupation to prevent disabled people from being aware of possible services \vas a factor in
isolated villages and places where NGOs and charities were not working. At the same time, the
Intifada-injured were a potent factor throughout the country for increasing awareness of disability
needs and demanding service provision. UPMRC's approach addressed the concern that this
awareness and articulation of need disproportionately benefitted the Intifada-injured, in contrast to
others with disabilities.

4.3.3 -5 Implementing the Programme with Community Participation
This element addressed the 'community-based' aspect of CBR. Community was usually
interpreted geographically, as the residents of the village or town where the CBR t m was
working. Respondents rarely addressed specific concepts of community accountability or
decision-making within the programme, preferring a broader discussion of community involvement
or cooperation. Participation ranged from endorsement and moral support, to volunteering and
contributing to CBR activities.
4.3.3.5.1 Conditions of repression - Depleted capacities
The severe economic repercussions and stressfil violent events that communities faced
under occupation were cited by respondents as affecting participation in CBR. It was natural, they
said, that many community rnembers addrcssed their otw pressing econornic and social concems
ahead of the disability necds of others, and fcw were able to commit themselves to volunteer
activities.
Rcspondcnts also indicated that the refugee expenence had a marked c f k t upon the
Paiestinian community, resulting in prolonged dependence upon UN relief mcasures, which
hindered community participation and self-reliance.
Ironically, thouph, it \vas suggested that lack of self-government also implied an absence of
bureaucratic obstacles that can characterize operations through sovemment oficials. A CBR
advisor commented that this allowed CBR programmes to benefit from the work of communiiy
activists: "But here, active peopie with initiative, motivated people can al1 have a Say. People can
affect change. A broader spectrum of people."

4.3.3.5.2 Conditions of resistance - Activisrn in the stiadow of partisanship
Increasing resistance to Occupation positively influenced community involvement in CBR.
Non-violent community resistance, characterized by the grassroots movements of issue-based
popular cornmittees and NGO formation and cooperation, also ârew community mernbers into
disability work. People joined organizations in a spirit of resistance and cornmitment, which a
CBR advisor explained by saying, "People were aware that without unity at lcast - with the daily
life ne&, with the problems of everyday, disability, poverty - without uni- they can do nothing."
In this environment, the Intifada-injured were a common focus of concern and caring, and a catalyst
to community action in disability.
Howcver, it was noted that conununity mobilization marred by political factionalism,
when some cornmittees and NGOs sought political gain fiom their rehabilitation service activities.
A CBR advisor noted the impact of factionalism upon CBR when using the WHO village
cornmittee model:
You know you form a cornmittee in this countn, immediately the formation is political. You choose this part and that part, and you get the wrong people - mcn who are in political power. And they think they want to take over this project and use it for their own purposes. And the next thing o u know, it ignites fights among the people.
Factionalism occasionally led to cornpetition among rehabilitation organizations, however
respondents noted that its impact was less, and cooperation greater, witliin CBR than with other
health and social initiatives. This was perhaps due to consensus surrounding the cause of
disability, as syrnbolized by the Intifada-injured.
4.3.3.5.3 CBR programme responses - Building new models
In response to the economic pressures upon community members, UPMRC exarnined and
rnodified the CBR model of voluntcerism. CBR workers were paid. In addition to enlisting

conventional volunteer support, a CBR advisor explained how they worked to "reconstmct the
notion of volunteer in tems of 'selective assistant at times'." This involved cornmunity members
assisting with the CBR programme by donating tirne and talent within their oivn employment. This
assistance could mean, for ewmple, transportation from taxi dnvers, apprenticeship with
craftspeople, or g d s from merchants
UPMRC reacted to, but was also a major player within, the general community
rnobilization during the Upnsing. UPMRC invited participation in the CBR programme by
approaching communities as partners in resistance, to address disability needs through CBR.
According to a CBR manager, it was casy for UPMRC to start a dialogue with communities bascd
upon thc sharcd assumption that, under the constraints of Occupation, people's necds could only be
met by coopcrative action.
Organizations working in rehabilitation chose CBR as a kcy mcthod of addressing
disability issues and providing services. A CBR worker explained how political resistance and
community responsibility were linkcd in rchabilitation initiatives: 'We t a n t to control our life.
We want to be indcpcndcnt from thcm. We wiII not wait for tbat [Israelij Civil Administration
corne with project for disabled. No, we will do it for ourselves."
In response to the risks of political factionalism, WMRC adaptcd its usc of local disability
cornmittees. lnstead of initiating projccts with local cornmittees, regional teams gained infomal
cooperation of local people who were aircady active in disability issues and who were accepted
within their communities. CBR work procccdcd with this nucleus of committcd pcoplc (usually
women, often moihcrs of children with disabilities) who participated in project decision-making
with the team. Links were thcn made with community leaders for validation of the process. in
addition, UPMRC addressed factionalism by forrnally cooperating with the CNCR and the GUPD.
UPMRC partnered with a second health NGO, integrating staff and responsibilities in the creation
of a CBR project in the North rqion. The CBR team also dealt wvith factionalism at the project

level, by convening village meetings in which a balanceci representation of all concemed groups
focused on addressing disability n e d s in a cooperative m e r .
4.3.3.5.4 Summary
Conflict conditions had signifiant effect upon c m u n i t y participation in CBR.
Repression conditions challengeâ and oAen overame people's capacities for volunteering, since
they were pre-occupied with simply meeting personal and family needs. In response, the Intifada
set the stage for CBR, building on the essential component of community mobilization in the
resistance. Strong political motivation for high-profile social action initiatives triggered community
response to disability issues, which then developed into CBR initiatives. This also rcsulted in
innovation in CBR conmittee models and partnership approaches. And tvhile community
involvement in CBR was threatened by vulnerability to political divisivcncss, factionalism did not
overcome cooperative work in disability.
4.3.3.6 Exhibiting a Modcl of Partnership among Pcople with Disabilities, Familics, the Cornrnunity, and Rehabilitation Personnel
Partnership within CBR was explained in ternis of meaningful contribution and equal
status among CBR participants, within their differing roles. Respondcnts were asked to what
degree the programme treated all participants equally and with respect. In order to clan& the
question, this concept was contrasted with a scenario in which a hierarchy existed, with the doctor
most senior, followed by the physiotherapist, the rehabilitation wvorker, the family, and finally the
person with a disability.
Respondents from al1 categories clcarly identifid with this concept and indicated that their
perspectives and opinions were valued by others. However, many respondcnts explained that
cultural faftors within Palestinian society (previously noted) were also at play, obstructing a tmly

non-hierarchical programme. It was apparent that this issue was a sensitive one, perhaps because
the ideal of an equitable society lay at the k a r t of Palestinians' struggle for democracy.
4.3.3.6.1 Conditions of repression - Reinforcing divisions
Respondcnts noted b a t curfews, travel restrictions, and security concems caused CBR
teamwork to become fragmented. There were many occasions when the full team was unable to
work together, threatening cohesion and partnership. This occurred when team mcmbers with
cerrain IDs or car license plates were not permiîted entry to villages. Disruption aiso resulted fiom
the threat to male workers, including doctors, who were at greater risk of arrcst by soldiers than
wornen health and rehabilitation workers.
4.3.3.6.2 Conditions of rcsistance - Ideals of equity
Partncrship was facilitated by thc elcvatcd stanis of the Intifada-injurcd and the rcsulting
improved attitudes towards people with disabilities. Thcy, and their fmilics, bccame confident in
taking new roles within thc CBR prccess. A CBR worker notcd, "They want us to go to their
houses, to work with thcrn like a team. They arc sharing, and we are sharing wvith thcrn."
At the same time, conccp!s of democracy, social equity and participation that underlay the
grassroots movcments were rcinforced during the Intifada. Popular committees and NGOs sought
to convey these concepts into action, by recruiting people fiom al1 leveis of society to coopcrativcly
address broad social needs. In this wvay, UPMRC gained a committed group of CBR worken.
Significantly, while women, young people and people with disabilities began to express their views
and shape society in challenge to lsraeli milita^ authorities, they at the same time challengecl their
own authorhian culture.
A few respondents, from al1 categones, assertcd that there was no discrepancy in status
within UPMRC's CBR programme, with al1 participants being equal and respected. Another view

was expressed, perhaps a more realistic one, that a tme mode1 of partnership \vas still an ideal,
though UPMRC was attempting to realize it. A CBR manager, himself a male doctor, s u m e d this
up by saying, "Our goal is not a hierarchy, but actual life is something different. There are good
steps with this in Medical Relief, but the culture is authontarian and hierarchical."
4.3.3.6.3 CBR programme responses - Interdependence among workers
The fragmentation of CBR tearnwork caused by curfews and travel restrictions
necessitated a sharing of duties. Each person Iearned others' roles, and, by covenng for one
anothcr, understood and appreciated each other's work. This response produced a positive result in
tems of partnership.
Similarly, CBR workcrs' responsc to sccunty problems had a positive effect for pamicrship
within the team. While male doctors wcrc concalcd, female CBR and village health workcrs were
respectcd for working more visibly, and for challenging soldien who tried to arrest the men. Thus,
within the UPMRC PHC and CBR teams, there emerged an equalizing force between female
workers and the tradi tionally powerfil male doctors.
4.3.3.6.4 Summary
Conditions of Occupation were not highly relevant to the issue of incquity in working
relationships, although responses to repressive measures created a positive environment for
partncrship. Palestinian culture itself was considered to be the prima. impcdiment againa a mode1
of partnership within CBR, indeed within society. Against this bamer, the dernocraiic ideals
underiying the grassroots movements of the Intifada exerted a positive influence upon CBR
programme participants, and made some impact.

4.3.3.7 Using Locally Made Rehabiiitatic:: Aids and Equipment
The UPMRC CBR programme made extensive use of both simple, village-made items, and
more sophisticated items that m e fiom larger Palestinian workshops. Simple rehabilitation aids
were usually fibncated fiom wood by a village carpenter, and included standing and seating
equipment for children. Items such as prostheses, orthoses and wheelchain were made in
institutional workshops. Educational equipment and therapeutic toys were obtained fiom sources
within villages and the central region. The evolution of this system was largely due to political
factors, as will be shown.
At the s m c time, the programme accessed a wide variety of imported rehabilitation
equipment, such as exercise equipment and wheelchairs, particularly for thc physiotherapists'
work. High technology rehabilitation equipment, such as cornputer-assisted dcvices, was not
accessed by the CBR tcarn from any source.
4.3.3.7.1 Conditions of rcpression - Small-scale technology options
Overall, the econornic and travel conditions of the Occupation lefi the population with little
choice but to use simple, village-made options. Poverty contributed to families' inability to afford
rehabilitation aids. A CBR worker comrnented, "the rnoney which are not enough, they go to more
basic life needs - like food, like rent." So, although some charities offered assistance, most people
with disabilitics went without assistive devices. At the sarne time, lack of cconomic development
and investment discouraged the establishment of equiprnent workshops, thus ensunng reliance upon
Israeli and imported rehabilitation products for the few who could afford them. The presence of
sophisticated and espensive items sometimes elicited dissatisfitction with simple local products that
were offered within the CBR programme. A CBR advisor explained, 'While we are talking about
tree branches in Gaza, people know that there is an electronic wheelchair half an hour away .... And
they dont want to have one and cannot afford the other, and therefore will end up with nothing."

Manufacture of ans equipment beyond very simple aids was dcpendcnt upon skilled
craftspeople and adequate materials. Vanous economic factors had caused a scarcity of skilled
craftspeople, which was said to have "depleted the foundation for technology." These factors
included the tendency for a large number of workers to be &y-labourers in Israel, and family
pressure for professional education for young men, so that they might have the ability to eam more
money and perhaps emigrate. And while curfews, closures and stnkes limitcd the availability of
rnaterials, they also preventcd CBR workers from gaining additional training in making
rehabilitation equipment. This was illustrated by a CBR advisor: 'We established a workshop for
muiufacturing the wheclchairs. Three of the workers hcre were selectcd. Thcy had to take thcir
course in Jenisalem. The course passed, and we didn't get pcmits for them to go."
nius, travel restrictions highlighted the impracticality of reliance upon outside resources.
Simple alternatives w r e developed because it was difficult to acquire or maintain sophisticatcd
rchabilitation equipmcnt.
4.3.3.7.2 Conditions of resistance - Sophisticated relief versus self-sufliciency
Uprising conditions both discouragcd and fostered Palestinian self-sufficiency in
rchabilitation tcchnolo~. Prirnarily, the intcmational rcsponse to the well-publicized needs of the
Intifada-injured had a large impact.
international donations of rnoney and rchabilitation equipment, though greatl y appreciated,
discouraged development of local rehabilitation technology. For example, the high profile of the
Intifada-injured initially singled them out to receive sophisticated equipment, either directly or
through special fùnding for equipment purchases. As a result, the Intifada-injured generally
aquired supenor equipment, in cornparison with other disabled persons. So, while injuly in the
Intifada increased disability awarencss and prompted Palestinians to meet their rehabilitation

equipment ne&, the influx of assistance discouraged the development of sustainablc village-made
options.
Similarly, international groups and organizations also provided equipment to Palestinian
rehabilitation programmes which served the needs of al1 disabled persons. Such programmes
included UPMRC CBR. A CBR worker remarked, "If we have no choice, we go back to them
[simple ai&] and we are really making good use of that. But, in other way, we are not using al1 the
[local] resources, because we have access to better."
Nonetheless, and fortunately in a sense, foreign-made rehabilitation equipment was
frcquently found to be inappropriate within the Paleainian context, particularly to withstand the
harsh environment of village homes and streets. ïhis incompatibility encouragcd initiatives to
develop more suitable local products. Substantial international devclopment support then hciped to
establish manufacturing workshops within Paiest inian rehabili tation institutions . Europcan
govemments and NGOs were larsc contributors to institutions located in the central arca - in
Jcrusalem, Rarnallah and Bethlehem. It was thcn possible to produce necdcd products, such as
orthotics and prosthctics, at a cost lower than imports. It also crcated a source of trained workers
in rehabilitation technology. A CBR worker spoke of these institutional initiatives: "During the
Intifada we got more support from abroad to build this selfdependence, independence, on our own
human resourccs or our own technology - instcad of importing it frorn Isracl and frorn abroad.
Organizations, for political rasons sornctimes, they hclpcd us to be independent from Israel."
4.3.3.7.3 CBR programme responses - Keeping options open
The CBR programme responded in two ways to international actions in the arca of
rehabilitation technology. On one hand, the programme took advantage of donatcd equipment, and
solicited funds to purchase imponed goods. On thc other hand, it supported the technology

initiatives of Palestinian institutions and their international partners, and accessed those local
resources.
In response to a lack of skilled local worken, CBR workers sought local carpenters to
mate rehabilitation ai& and equipment. The CBR worken guided the manufacture, which was
described as being "by copying, but not by imagination."
in response to travel restrictions that impeded movement of goods, UPMRC used their
network of linked PHC and CBR tcams to supply needed rehabilitation aids and equipment fiom
central locations. It was noted that this was not difficult since UPMRC had gained expertise in the
distribution of essential drugs throughout the Intifada.
4.3.3.7.4 Sumrnary
The conditions of Occupation and Upnsing provided the CBR programme with a compler
scenario of inccntivcs and disinccntivcs to using local rehabilitation tçchnoiogy. What emcrgcd in
this situation was a flesiblc and broad definition of 'local.' Equipment was considcrcd local if
Palestinian labour and materials were usd. Accordingly, local equipment included simple, village-
made itcms, as well as the more sophisticated items fiom Palcstinian institutional workshops in the
central region. The latter became availablc only through international developrnent assistance.
Thc CBR programme used both local and irnported quipment, according to what was
appropriate, neccssary, or easy under the overall conditions. Local products were chosen over
importcd oncs when they werc available and at lower cost, and because political sentiment
encouraged this practice.

4.3.3.8 Participating in a Refcrral Network with Specialists and Institutions, for Professional and Technical Rehabilitation Support
A referral nehvork was defined as the link between the CBR programme and medical
specialists, tcrtiary care Fdcilities, rehabilitation hospitals and physiotberapy clinics. Such a
network was not conceivable pnor to the IntiFadq due to the lack of rnany of thesc services for
Palesthians.
With substantial international assistance, the Uprising spurred the dcvelopment of tertiary
services, and a referral network began to be established. UPMRC CBR participatcd in this
network. Relations between the comrnunity programme and rehabilitation specialists were
characterized by mutual respect and open communication. At tbe time of study, CBR participants
were identifjing the necd for rcgional intemcdiate lcvel seMces to be developcd, providing
occupational, speech and physical thcnpy.
4.3.3.8.1 Conditions of rcprcssion -- lmpeding dcvelopment and acccss
Occupation conditions were invariably reported to negatively affcct thc development of a
rcferral network. Bcfore the Intifada, the cornponents needcd for a refcrral system wcre largcly
unavailable, such as rehabilitation institutions and adequate professionals. Latcr, whcn specialized
services were developed, repressive conditions continued to obstruct access by comrnunity
p r o g m e s .
The only rehabilitation services provided by the military authorities were small
physiotherapy depaitments in a few of the governent hospitals. Limited care \as available for
people with disabilities, provided primarily within smali institutions run by charitable societies. A
CBR advisor highlighted thc repressive cffcct of military administration on this elernent of CBR,
saying that a comprehensive approach to rehabilitation "lies within thc establishment of structures
through which CBR could link, so that services could be provided, and needs could be met .... It is

very difficult for this to happen under Occupation, because there must be a state structure that has
a clear policy."
In very serious cases, referral to medical and rehabilitation facilities in Israel was made.
The mst of such treatment, however, was extremely hi&. Few Palestinians were covered by the
necessary Israeli health insurance and if they were, there was no guarantee of receiving the benefits,
as the process was subject to the arbitrary management of the Isracli authority7s office of Civil
Administration. When referrals were made, CBR workers described communication between
themselves and Israeli hospitals as being virnially impossible.
Later, when Palestinian rehabilitation institutions were created and expanded, rcpressive
conditions of curfkws, closures, strikes, and lack of travd permissions made the institutions
inaccessible to the vast majority of Palestinians. A CBR advisor spoke of their cooperation with
the new facilities: "There are no problems with the service. But the problcm is with how to reach
[them]." Even when those in need could reach the institutions, thcrapists and doctors were hindered
in reaching their place of work, and specialists were similarly restricted in rnaking regional
outreach visits. A CBR worker described such incidents: '%en I cal1 them to refer some of the
w e s to hem, they will tell me, 'I'm sorry. 1 cannot accept your case because that person is not
available. He is stuck in his a r a - curfew'."
4.3.3.8.2 Conditions of resistance - Capacity-building and cooperation
In contrast to the above, conditions of resistance spurred the development of a referral
systern. Individual institutions, programmes and resources were developed, along with a process of
coordination. This was due to international development assistance, directed towards Palestinian
projects, which increased substantially at the time of the Intifada. Money and resources, given
primanly by European governments and NGOs in response to the disability needs of the
Intihda-injureci, supported the creation, operation and expansion of secondary and tertiav

rehabilitation facilities. These institutional services were established in the central area, in the
cities of Jenisalem, Bethlehem and RamaIlah. UPMRC CBR workers noted that they relied heavily
upon these institutions for referrals, because this supported Palestinian facilities, and because the
quality of service was high.
The govemment of Swveden was a particularly responsive international actor, supporting
rehabilitation through the Swedish NGO Diakonia. A CBR advisor explained how political
circumstances created the background for rehabilitation enorts:
Diakonia came to this country to support the building of the Abu Rayya Rehabilitation Centre, in 1989 as a response to the [Swedish] foreign minister and his visit here and the big problems with the Intifada. Later on therc were several initiatives by diffcrent NGOs to stan some CBR activities and pilot things here that are more on the cornrnunity level, and try to find out what is the CBR model for us. Diakonia expressed interest to support that.
Diakonia went on to provide technical, financial and logistial support towards the organization of
the CNCR and regional CBR projects.
In addition to international support, other aspects of the Intifada ûiso encouragcd the
refenal element of CBR. Thc high profile of the Intifada-injured was said to have provided a
mutual cause for local and outside organizations, which clicited the cwperation necessary to create
a rehabilitation system. The spirit and structures of Intifada cornmunity resistancc also facilitated
formal cooperation in CBR.
4.3.3.8.3 CBR programme responses - Contribution to an infrastructure
UPMRC's response to the jack of rehabilitation services provided under Occupation was an
aspect of its community resistance activity. To compensate for the lack of a Palestinian
government, and to meet the increased disability needs of the Intifada-injured, UPMRC and other
NGOs and medical organizations took the initiative to mate and coordinate services. UPMRC
contributed to the nehvork of services through its CBR tearns, as well as through rnedical and

physiotherapy c h i c facilities. Links establishd within the CNCR allowed for the development of
a referral neh~cirk, which was being created with international support.
On a practicd level, CBR workers were required to respond to the travel restrictions that
impeded the r e f e d system. CBR workers expanded their duties beyond rehabilitation, providing
transportation for individuals to health institutions and medical specialists when essential. A CBR
worker reporteci, 'We take a patient ounelves, in our own cars. Because it's easier for a woman in
a yellow-plate4 car. But it's difficult - we're not supposed to do it. It's not in CBR, but, to get
things done, especially in cases that really need it, we do it."
4.3.3.8.4 Sumrnary
Conditions of repression were formidable obstacles to a rehabilitation refeml system,
mostly through creating barriers to access through restricted travel. On the other hand, resistance
conditions, particularly international development support, were largely responsible for the
evolution of a functioning refenal system. Political solidarity elicited needed extemal support and
intemal cooperation for a referral system, though one that remained vulnerable to obstacles of the
Occupation.
4.3.4 Political Violence and CBR: Summaw of Findings
The case of UPMRC shows clearly that CBR was affected by the political conditions of
repression and resistance. Some conditions were more important than others, and the elements of
CBR were affected in different ways, and to varying degrees.
The principle conditions of repression to affect the development of CBR were travel
restrictions, administrative bamers upheld by requiring IDs and permissions, and the lack of self-
govemance and econornic implications of military administration. The most important conditions

of resistance were non-violent cornmunity resistance, the status and synbolisrn of the Intifada-
injured, and international development assistance to Palestinian rehabilitation programmes. Thus,
confiict conditions had an influence in both hindering and helping CBR. Overall, however, the
repressive conditions were detrimental towards CBR, and resistance conditions were facilitatory.
In addition, the individual elernents of CBR were affected to diffcrent dçgrces. Some
elernents were strongly affected by the conditions of conflict. These includcd attitudes towards
disability, integration of disabled people, cornmunity involvernent in the CBR programme, and the
development of a referral network. Other elernents were less affected, such as the modei of
partnership among participants, and provision of participant-directed services. Not surprisingly,
some elernents were affectcd both negatively and positively. For example, community involvement
in CBR was strongli, inhibited by rcpressive conditions, but strongly positivcly affccted by
resistance conditions. Thc element of training was not significantly affccted, and the ovcrall effiect
upon the element of local tcchnology wvas neither clearly positive nor negativc.
Overall, UPMRC undcrtook effective responses to the conditions of political violence.
CBR workers took pridc in thcir rcsourcefulncss in ovcrcoming travel restrictions. In the face of
insurnountable obstacles (such as those imposed by military administration, economic factors and
administrative barriers), the programme used innovative tactics which addressed CBR concems
using alternative mcthods, such as strengthcning Palestinian institutions likc the CNCR and the
GUPD. Important in this regard c s i s that UPMRC was effective in complemcnting its local
community efforts with initiatives at the highcr organizational level.
As well as responding to the dificult political conditions, the CBR programme took
advantage of the positive cffects officred by non-violent community resistance and international
support. Concem for the Intifada-cases was balanced with a broader focus on disability issues, de-
ernphasizing the popular focus on youthfùl heroes.

TU understand why CBR elernents were affected differently, aiid how the UPMRC CBR
programme was appropriate to conditions of political violence, CBR can be viewcd fiom a
comrnu~ty development perspective. Such an approach addresses capacities and vulnerabilities of
a comunity dunng time of codict.

CHAPTER S
DISCUSSION
5.1 Design Issues and Study Limitations
The qualitative case study design was appropriate to this investigation, howvevcr thcre werc
some inevitable dificulties in defining boundàries of the case. For example, UPMRC's CBR
programme was not a hornogenous or stable entity. As the Intifada progressed and as CBR models
bewne more well known and desired, the programme undenvent transformation. This change
provided a challenge to some rcspondents in surnmarizing their expenence of CBR over the yean.
Also, one of the CBR projects was implemented in partnenhip with another NGO, which made the
UPMRC programmatic boundary less dcfined.
Limitations of the study included the language diffcrence bchveen rcsearcher and
rcspondents. The rescarcher had a basic understanding of Arabic, and many rcspondcnts were
highly cornpetcnt in English. When requircd, Arabid English interprctcrs werc used, choscn on the
b a i s of their ability, thcir fdmiliarity wvith the programme, and the comfon of the interviewee. The
interpreters were UPMRC collcagucs of CBR workcr rcspondents, and volunteercd their services.
Despite these factors, some depth of meaning \vas likely lost, both in the cases of intcrpretation and
when rclying upon the flucncy of respondcnts who spoke English as a second language.
A second study limitation was that data analysis did not commencc until data collection
was complete. Analysis could have beguii and proceeded concurrently with interviews, in order for
interviews to be more responsive to emer~ing categorics and themes. However, the researcher
chose to sacrifice flexibility for the sake of consistency of data collection technique.

5.2 Discussion of Findings
ln order to discover whether CBR is an appropriate rehabilitation response under
conditions of political violence, 1 have desctibed the w e of a Palestinian NGO that developed a
CBR programme within such a situation. Not surprisingly, findings showed that the conflict
conditions did affect CBR, that some of the conflict conditions had greater impact than others, and
that individual clements of CBR wcre affected differently. Some questions, however, are r a i d :
Why did resistance conditions actually facilitate CBR, and facilitate certain elemcnts in particular?
In addition, how can CBR programme rcsponses be assessed for their appropriatcncss under such
conditions?
In answenng these questions, CBR is considercd outside the sphere of rehabilitation
medicine, and vicwed fiom the perspective of community developrnent . UPM RC's CBR
programme was orientcd beyond service provision, towards comunity dcvcloprncnt, in ordcr to be
most relevant and responsive to prevailing circumstanccs.
This discussion presents the central idea of CBR as community developrnent. by
reintroducing Anderson and Woodrow's tenet that assistance in conditions of conflict must
contribute to, and not undermine, community dcvclopment. Their concepts and analflical
fiamework will be used to expiain the significance of the findings in the case of CBR. UPMRC's
CBR programme, implcmented as a fonn of assistance under conditions of political violence, will
illustrate Anderson and Woodrow's critcria for an appropnate response, through the organization's
developrnental focus. The discussion will conclude by offering perspectives for agencies wishing to
pursue CBR in conditions of conflict.

5.2.1 The Realms of Comrnunitv: Understandinn CBR and the Tritifada
Why did resistans conditions actuaily facilitate C B S and certain elements of CBR in
particular? The answer lies in observing what the Intifada specifically offered CBR, in. texms of a
supportive environment.
As introduced in Chapter Two, Anderson and Woodrow (1989) assert that any assistance
made to cornmunities living in confiict must not simply provide relief, but must contribute to long-
term development. In order to be developmental, the assistance must respond to esisting comrnunity
capacities and vulnerabilities, strengthening the former, and reducing the latter. Accordingly,
comrnunity capacities and vulnerabilities cm be divided into three categories, or realms:
physicalfmaterial, socia~organizational, and motivationaVattitudinal. Anderson and Woodrow's
(1989) Capacities and Vulnerabilities Analysis (CVA) incorporates these realms into planning and
evaluation of programmes which assist communities dçaling with emergcncies of conflict or
disaster.
Before esamining the CVA frarnework itself, the three realms - physical, social and
attitudinal - can be considered in a wider sensc. Anderson and Woodrow have provided guidelines
for defining the three realms (see Appendix L), noting that the categories are neither discrete nor
exclusive. A conceptual application of these realms provides insight into the rclationship between
conflict conditions and CBR. Following the guidelines of Anderson and Woodrow, 1 have
categorized the CBR elements into realms, as shown in Table 5.1.

Table 5.1 CBR Elements as Realms of Community
CBR element CVA realm I attitudes attitudinal / motivational 1
srnial / organizational attitudinal/ motivational
training physical 1 material 1
part icipant-dirccted services social l organizational
cornmunity participation social / organizational
partnershi p attitudinal / motivational
technology physicai / material 1 referral network social / organizational
physical 1 rnaterial
The above table shows that the CBR elements arc reflected in al1 three realms, indicating that a
broad CBR programme may address physical, social and attitudinal aspects of community. In
addition, the table allows us to more carefùlly consider four important elements, Le. those elements
that were noted to be most strongly affected by conflict conditions. As noied in the surnmary of the
study findings, the important elements of CBR in this study were:
- promoting positive community attitudes, - promoting intepration of people with disabilities, - implementing with community participation, and - participating in a referral network.
It is remarkable that these elements of CBR were strongly facilitated by resistance
conditions. From the literature, it was expected that social and health programmes wouid suffer
under conflict conditions, and indeed repressive conditions did exert negative effects. Table 5.1,
however, illustrates that these four elements largely reflect attitudinailrnotivational and

sociaVorganizationa1 realms of conununity. These four CBR elements were positively affectai by
resistance conditions because the Intifada itself was an event of collective motivation and
organization.
The Intifada grcw from a widespread popular resistance movement. The "national
movement" was supported by "mass organizations," especially of women, workers, students and
youth (Taraki, 1990; Hiltermann, 199 1). Their activities were political, social and cultural, and
politically afiliatcd cornmittees also undertook medical and agrkul~ral relief work. The Intifada
itself spawned popular committees (ncighbourhood cornmittees), whose volunteers provided and
coordinated education, hcalth, food storage, agriculture and security for the community (Nassar &
Heacock, 1990). Taraki dcscribcs these collective actions as the development of political
consciousness arnong Palestinians, while Nassar and Heacock speak of the revolutionary
transformation of Palestinians. Clcarly, anihidina! and social factors reinforced one anothcr.
National identity was assencd and strengthcned through community mobilimtion and organization,
demonstrating how '.i community cm build community cohesion through joint action" (Anderson
& W d r o w 1989, p. 14).
Consistent with documentation on the Intifada, the current study of UPMRC CBR revealed
that resistance conditions were primarily expressions of the attitudinal and social rcalrns of
community. An important example, as noted earlicr, were the Intifada-injured, who were not
simply individuals with wounds. Thosc who bccarne permanently disablcd werc heroes of the entire
community, synbolizing Palcstinian rcsistance since "disability \vas conceptualized as martyrdom"
(Atshan, 1997, p. 5 5). The emotions that the Intifada-injured elicited fiom Palestinians included
pnde, anger, and sadncss. It is essential to appreciate that these emotions were expenenced
collectively as w c l l as individunlly, with grcat intensity because Palestinians considcred the injured
to be their childrcn and brothers. These emotions catalyzcd collective and individual action that
resulted in violent and non-violcnt resistance to Occupation. Non-violent resistance activities, such

as rnass demonstrations, strikes, and the development of new responsive organizational structures
with non-traditional leaders, uicreased social cohesion and a sense of national identity among
community members. Such a 'comrnunity-building' environment in turn supported the .
development of elernents of CBR h t require attinidinal and social change. Within this politicized,
energetic and supportive environment, social change was pro-active and rapid. Thus, CBR as an
innovat ive and practical concept for rehabilitation emerged and flou rished not onl y during the
Intifada, but because of the Intifada.
IIhis is not to Say that physical factors were unimportant. Indeed, the significant economic
impact of Occupation was stressed by respondents, and has been the subject of much study (e.g.,
GrahamBrown, 1986; Heiberg & Ovensen, 1994; Roy, 1995; Saleh, 1990; see also UNCTAD,
1993; World Bank, 1993). There were grave econornic impacts on the Pôlestinians frorn Israeli
controt of such material factors as land, water, investment, trade and taxicion. But development
and underdevclopment are more than issues of economic growth or stagnation. In her pivotal work
in the Palestinian context, Sara Roy (1995) emphasizes the political, social and cultural aspects of
development, and she proposes a theory of dedevelopment to descnbe the result to Palestinians of
Israeli policies of occupation. Differentiated fiom underdevelopment, dedevelopment "not only
distorts development but forestalls it entirely, by depriving or ridding the economy of its capacity
and potential for rational structural transformation and preventing the emergence of any self-
correcting rneasures" @. 128, whereas underdevelopment allows for "needed structural change
within the weaker penpheral entity, although that change is disarticulateci, onented to, and shaped
by the expansion of the dominant extemal economy to which it is subordinate." p. 129). Israeli
policies that have resulted in Palestinian dedevelopment include expropriation, dispossession, and
deinstitutionalisation, and "were designed to secure military, political, and economic control over
Gaza and the West Bank, and to protect Israel's national interests" (p. 135; see also Benveniai,
1984). Roy's research makes clear that econornic impacts, though rnatenal, arose fiom lsraeli

social and ideological factors. Similarly, Palestinian resistance to occupation was not priniarily a
response to econornic hardship. As Saleh (1990) atteN, "The essence of the conflict between the
Palestinians and the occupation is, however, not economic but political" (p. 48).
Anderson and Woodrow note that most assistance in conflict and disasters is concentrated
upon physical ne& of the so-called "viaims," because it is material suffering that compels
outsiders to act. However, in t e m of providing assistance that will contribute to, and not
undennine long-tenn community development, they Say that "experience shows that it [the physical
1 matenal realmj is often iess important than the other two areas" (p. 13). Similarly, findings of the
current case study show that the CBR elements of the physicaUmatenal rcalm - training and
technology in particular - were affected to some degree by the conflict conditions, but their
development proceeded without overall hindrance or help from the conflict. This suggests that
lirniting CBR assistance to the provision of material rehabilitation services would bc shortsighted,
as this would demonstrate an understanding of community only in terms of its physical realrn.
In sumrnary, two key aspects of the Uprising - collective action and the Intifada-injured -
directly underlay two key elements of Palestinian CBR - community participation and
transforrning attitudes towards disability. Resistance conditions of the Intifada facilitated CBR by
providing a dynamic community environment of organizational and motit ational strength. The
organizational and motivational elements of CBR grew, and benefitted the most, fiom the unified
action and common purpose that charactenzed this environment.
Political motivations of the Intifada led to actions that ubimately promoted cornmunity
development. It will be seen (Section 5.2.3.) that a poiiticited and community development
approach to health, dernonstrated by the primary health care initiatives of UPMRC, infiuenced
rehabilitation efforts, with CBR emerging as a stmng choice of health activists. Yet Anderson and
Woodrow contend that supporthg community development specifically involves increasing

capacities and reducing wlnerabilities. The UPMRC case can now be examined to see how CBR
ftlfilled these criteria.
5.2.2 Ca~acities and Vulnerabilities. and the UPMRC Response
How cm CBR programme responses be assessed for their appropriatencss under
conditions of political violence? The CVA framework was developed for use within situations of
disaster or conflict, as a tool for programme planning, implementation and cvaluation (Anderson 8;
Woodrow 1989). The fmcwork was derived from the experience of both local and international
NGOs, and thc current UPMRC case provides an example of the use of this framcwork for CBR
programmes .
Findings of the UPMRC case study exposed a variety of comrnunity capacities and
vulnerabilities, which crncrged from both contestual factors and political conditions. The following
tables sumrnarize study findings, showing the most important capacities and wlncnbiliiies, and
indicate how Palcstinian dcvclopmcnt of CBR can be piciured within Anderson and Woodrow's
CVA h e w o r k .


Table 5.3 Vulnerabilities in Palestine for the Development of CBR
physical / mate rial
Type of influence 1 Vuinerability
I
regional factors i Economic underdevelopment and poverty were characteristic of rural areas.
1
I
professionalization and i Shelten and institutions were considered the : appropriate place for people with disabilities. institutionalization of 1
disability / cultural factors j Therc were few rehabilitation institutions i offering adequate, high quality senices. I
repressive conditions i Physical impositions included: travel : restrictions, economic under- and de- i development, administrative bamers through i system of permissions, lack of self-govcmance, i lack of health and rehabilitation facilities, i I collective punishment, military actions. I .
resistance conditions i Violcnt resistance activities caused disruption. I
i There was a rise in the nurnber of injured and i disabled people. International relief that was i characterized by donations fostcred dependence.
social / organizational
cultural factors i Large nuclear fmilics strcsscd mothcrs caring i for disabled members. Charity to people with i disabilities undermined their estecm and power. I
i Authoritarian, hierarchical and conscrvative i culture w s inflexible with respect to new approaches and roles for disabled persons.
8 1 I
professionalization and i Authority and control in rehabilitation lay in the institutional izat ion of i hands of nondisablcd people. disability
I
1
,
resistance conditions i , Factionalism hindered fùll cooperation in i community activism. 1 l 8 I
I attitudes motivational i Underlying attitudes towards people with i disabilities were negative and pityng.

Thcse tables illustrate that Palestinian society demonstnted both capacities and
vulnerabilities for addressing disability needs. These capacities and vulnerabilities were influenced
by contextual factors as well as by the conditions of political violence. Not surprisingly, some
factors were not solely positive or solely negative. For example, the fact that there were available
skilled rehabilitation personnel, and that professionals controlled disability initiatives, indicates
both a capacity and a vulnerability. It is within this cornplex scenario of capacities and
wherabilities that the appropriateness of CBR programme responses is demonstrated.
Assistance provided during conflict risks increasing the wlncrabilities and ignoring, if not
undermining, the capacities of the people (Anderson & Woodrow, 1989). A CBR programme is
equally susceptible to this danger, and would be considered an inappropriate response to the
conditions if it did so. The WMRC CBR programme, implernented under conflict conditions,
illustrates how the Anderson and Woodrow criteria can be applied. Responses of the CBR
programme to the capacities and vulnerabilities presented by both contextual and conflict
conditions are appropriate in that they promote long-tcnn community devclopment by working to
increase the capacities and rcduce the wlncrabilitics.
The CBR programme increased observed capacities in a number of w y s . It expandcd
available rehabilitation skills, by sponsoring university physiotherapy studcnts and training
rehabilitation workers. It cooperated with international partners, guiding resources towards
community rehabilitation needs. It worked within the supponive farnily structure. Finally, it
panicipated iri the non-violent community resistance movement, using the Intifada to catalyze
positive change for people with disabilities.
By its very nature, CBR directly addresseci many of the vulnerabilities that were observed
to aise fiom contextual factors. For example, it provided rehabilitation services that were
appropriate to poor areas, offered an alternative to institutionalized care and the charitable

approach, promotcd positive atîitudes towards disability, and put greater control of disability issues
in the han& of community members.
In addressing vulnerabilities arising fiom repression and resistance conditions, the CBR
workers and the UPMRC programme relied heavily upon communil knowledge and community
interaction. The UPMRC response balanceâ participants' needs, accounted for political
sensitivities, mdified community rnodels and approachcs, and overcame logistical obstacles
through innovation. While many physical vulncrabilities were insurnountable, responses utilized
strengths dcrived fiom social and attitudinal capacities.
In sumrnary, UPMRC put a community development philosophy of CBR into action. In
doing so, the Anderson and Woodrow CVA h e w o r k provides an illustration of how CBR
programme responses can be assessed for their appropriateness undcr conflict conditions. The
CVA ftamework would be a uscful tool for CBR, to guide the incorporation of comrnunity
development goals into programrne planning, irnplerncntation and evaluation. In the planning
phase, an outline of existing capacities and vulnerabilities could be cstablished through observation
and consultation, and disaggregated for certain community groups, such as people with disabilitics
or women. Specific means of incrcasing those capacities and reducing the vulnerabilities would be
proposed, and undertaken within programme implçmentation. Indicators of programme
effectivcness would incorporate these factors for cvaluation. The frarnework has the advantages of
being easy to use, of leading to apprcciation of capacities, and of allowing uscrs to discem and
weigh factors of conflict and contcst. Thc CVA fiameivork was not creatçd for CBR, but its
flexibility would allow it to be applicd to such a rehabilitation programme.

5 2 . 3 COmnunihf Deveio~rnent as Politicai Action
In many ways, Palestinian community development efforts were the by-product of a
political process. At the outset, UPMRC did not set out to develop a CBR progranmq. However,
as the Intifada continued, UPMRC and other NGO sector activists dçveloped CBR as a preferred
method for rehabilitation initiatives. Yet it is clear that UPMRC's choicc of CBR had wider
implications than simply finding a solution to the crisis of increasing disability. Within the
Palestinian context, health and rehabilitation issues were politicized, as were al1 social issues.
Primary health care had emcrged within the context of political resistance, and as a component of it
(Barghouthi & Giacaman, 1990). But the goal was more far-reaching than simply ending
Occupation. Building a civil society based upon national identity was considercd nccessary to
actors such as UPMRC (Barghouthi, 1994). Also, as noted early in the Intifada, "...the
Paiestinian hcalth agenda must reflect the social content of the Palestinian aruggle - both to
liberatc the nation and to build an equitable society where good health and access to health care are
a fiindamental human right" (Barghouthi & Giacaman, 1990, p. 84).
As in their work promoting primaiy health m e , WMRC's community dcveloprnent
approach to CBR was directly anributable to the prcvailing political and social situation. The
CBR programme of UPMRC has been considered an exemplary mode1 of social development,
particularly in tems of gendcr issues, and UPMRC itsclf has been terrned a "new social
movement" (Craissati, 1996). At a 1992 UPMRC-sponsored confcrence, CBR was discussed in
tems of working with disabled people to bbchallenge the injustices within al1 sectors of society,
working as part of the struggle to forge a more equitable structure" (International People's Health
Council, 1995, p. 127). The title of the conference report makes UPMRC's political focus explicit:
"The Concept of Health Undcr National Dcmocratic Struggle." A politicized CBR philosophy
serve- to re-orient the prc-existing perspective towards disability, and UPMRC saw CBR as

involving both service provision and action for social change, in order to meet both short- and long-
tenn disability needs .
5.2.4 Conflict and Deveio~ment - a Place for CBR
As was noted in Chapter Two, Anderson and Woodrow's Capacity and Vulnerabilities
Analysis has been widely cited and applied. With very practical implications, the Oxfam
Handbook for Development and Relief highlights sociaVorganizationa1 and motivationaVattitudinai
elements within their principles of response to emergcncy, and also goes as far as to Say:
Both relief and development should be more concemed with increasing local capacities and reducing vulnerabilities than with providing goods, serviccs or technical assistance. In fact goods, seMces etc should be provided only insofar as they support sustainable developmcnt by increasing local capacities and reducing vulnerabilities. (Eade & Williams, 1995, p. 834).
This Oxfam programming principlc not only articulates the CVA, but also parallels the Paleainian
principlc for health development during the Intifada, in which UPMRC and othcr health activists
promoted a "politicaUsocia1 health alternative" (Barghouthi & Giacaman, 1990, p. 8 1) that relied
on the strengths of votuntarism and health education, "in contrast to the potvcr of money,
equiprnent and buildings" (pp. 79-80). This principle echoes the findings of the current UPMRC
case study, which suggest a reduced emphasis on physical elements of CBK in prefercnce for
social and attitudinal ones,
Within the few welldocumcnted programmes of CBR within situations of conilict, a
community development focus is apparent. Peat et al. (1997) outline specific benefits resulting
frorn the integration of disability issues and CBR into a peace-building process, citing 'relief
development' as a policy principle which envisions building the capacity of local NGOs who
undertake CBR during conflict. O x h UK and Ireland provide in-depth selfevaiuative
documentation of their work with disabled children in Bosnia (Hastie, 1997). This Oxfam

casebook explores concrete issues for development and disability work under conflict conditions,
such as flexibiiity, ftnding and legal status, retention of stafF, insecurity and danger, and
communications and transport. More recentiy, Boyce's evaluation of a C BR programme in
Afghamstan details how rehabilitation service provision can be successfully integrated within
explicit development objectives and strategies, despite the obstacles and risks posed by war (Boyce,
1998). As yet, however, there is no evidence of the Capacities and Vulnerabilities Analysis being
applied to CBR programrning.
Remarkably, the Odarn experience in Bosnia echoes some of the findings of the current
Palestinian study, such as the opportunity presented for positive social change. Hastiç (1997)
quotes an Oxfam staff pcrson as saying, "It seems that it is not only possible to work on social
development projects in an unstable society, but also that unstable societies somctimes provide the
necessary conditions of shift and change to allow the adoption of new modcls, such ris the social
mode1 of disability." (p. 93). This was also obsewed in Lebanon, where the war had positive
results for disabiIity a\varcncss, for innovative projects such as CBR, and for coopcntive action
between disability professionals and people with disabilities (Abou Khali 1, 1997). In these cases,
international support to local groups \vas vital in prornoting social change, as was also scen in this
Palestinian CBR study.
Community based rehabilitôiion programmes have been classificd according to scveral
models (e.g., Kisanji, 1993: McColl & Paterson, 1995; see also Peat, 1997, pp. 48-7 l), and one is
a mode1 which articulates "CBR as part of cornmunity development" (Wu, 1997; sec also
Chaudhury et al., 1995, p. 177; Peat, 1997, p. 22). This parallels the definition of CBR as "a
strategy within cornmunity deve1opmcnt" stated jointly by the ILO, UNESCO and WHO (1994).
Coleridge (1993) makes an important contribution by locating CBR within a ethical and practical
discussion of disability in terms of concems for liberation and development. However, Coleridge
also daims that there is a muddied understanding of what CBR entails. Ambiguity and jargon are

demonstrated by the term 'CBR' itself, which "has tended to become synonpous with 'disability
work in development"' (p. 90). Indeed, though the issue of community development is increasingly
addresse. by CBR advmates, there appean to be confusion within CBR literature regarding what
it entails. Comrnunity development is often understd more nanowly as comrnunity participation
(participation being an important, closely related, but distinct issue) or with a Western bias as
personal empowement. Certainly it is essential to strengthen the capacities and diminish the
wlnerabilities of individuals, or the individual members of certain groups. Rehabilitation has
worked towards this goal within a medical model of disability. For CBR Anderson and
Woodrow's analysis is usehl for its focus on comrnuniîy level of analysis and intervention. It also
prompts CBR plannen O identiQ capacities and winerabilities beyond the physical.
5.3 Conclusion and Implications
1s CBR is an appropriate rchabilitation response under conditions of political violence?
This study suggests that it can be, if 'appropriateness' is understood in ternis of contribution to
community development. However, 1 suggest that CBR be chosen and irnplemented in those
situations with care. This Palestinian case study showved that CBR was afected both positively
and negatively by two distinct types of political violence, and that the individual elements of CBR
were affected in diffcrent ways. nie smdy also demonstrated the importance of contextual factors
that are beyond the sphere of the confiict. Therefore, if one believes that assistance should not
undermine cornmwlity development, it would be critical to assess several factors before endorsing a
CBR initiative in a region of conflict. These factors would include the comrnunity capacities and
vulnerabilities, the type of conflict, contextual factors such as culture, and whether certain elements
of CBR are to be priontizeâ in the particular project. The findings of this study indicate that,
where sociaUorganizational and attitudinaVmotivational capacities are high, a CBR programme
with a comrnunity development approach can be successfûlly developed.

While a strength of Anderson and Woodrow's framework for developmental relief is that it
allows flexibility for many models of programme intervention, nonetheless, suppon for long-term
cornrnunity development remains a desird goal. If a CBR initiative thoroughly assesses, and then
maximizes capacities and reduces vulnerabiiities, then it will have the characteristics of a
community development approach. Othenvise, and certainly under conflict conditions, there
remains a high nsk of addressing only highly-visible imrnediate needs while undermining
community strengths. At the samc time, Anderson and Woodrow point to the importance of
disaggregating community groups (on the basis of gender, class and age, for example) when using
the CVA framework. It seems seIf-evident that a CBR programme be intended, above all, to
benefit people with disabilities. Therefore, a programme should explicitl y promotc their
development, and can evaluate itself for this goal.
This midy of the UPMRC CBR programme provides a unique and exernplary case
(Patton, 1990). This case study did not seck to compare the effectiveness of cornmunity-bascd
venus institutional initiatives in working towards goals of promoting disabled pcrsons'
development, of fostcring cornmunity development in general, or of reducing conflict. Within
disability and rchabiiitation ficlds, therc is growing reco~nition of thc necessity for coordinated
action on the pan of community-based groups with institutional and professional actors, each
exhibiting their oivn particular strengths, in ordcr to make maximum gains. Nonetheless, while a
rehabilitation initiative may be considercd to make appropriate responses to certain conditions, it
would be most enlightening for both community and institutional rchabilitation progranunes to be
critically evaluated by people with disabilities, in tems of their o m participation and needs.

REFERENCES
AlPPHR (Association of lsraeli and Palestinian Physicians for Human Rights). (1990). The condition of health services in thc Gaza Strip. Medicine and War. 6, 140-1 5 1.
Abou Khalil, 1. (1997, Apnl - lune). Catalyst for change. AHRTAG Hcalth Action, 18, 10.
Adams, M., & Bradbury, M. (1995). Conflict and development: Oraanisational adaptation in conflict Situations. Oxford: Oxfam UK and Ireland.
Agcrbak, L. (1 996). Brcaking the cycle of violence: Doing development in situations of conflict. in D. Eade (Scries Ed.) & S. Commins (Vol. Ed.), Oevelopment in Practice Readers. Development in statcs of war (chap. 3). Oxford: Oxfarn UK and ircland.
Ahlstrom, C. (1991). Casualties of conflict. Uppsala, Finland: Uppsala University, Dcpartment of Peace and Conflict Research.
Al-Haq. (1989). Punishinp - a nation: Human riehts violations durine the Palestinian Uprisine, -
Decernbcr 1987 - Deccmber 1988. Ramallah: Al-Haq.
Al-Haq. (1990). A Nation Undcr Seiae: Annual Rewrt on Human Riehts in the Occupied Palestinian Territories, 1989. Ramallah: Al-Haq.
Anderson, M. B. (1993). Development and the prevcntion of humanitarian emergcncies. In T. Weiss & L. Minear (Eds.), Humanitarianism across borders: Sustainine civilians in times of war. Boulder, CO, & London: Lynnc R e i ~ e r Publishers.
Anderson, M. B. (1 994a). Capacities and Vulnerabilities Analysis. In Oxfam Gendcr Training Manual. Osford: Osfarn LJK and Ireland.
Anderson, M. B. (1994b). lntcrnational assistance and conflict: An exploration of nceativc imoricts. Cambridge, MA: Thc Local Capacities for Peace Project.
Anderson, M. B. (1993). The es~cricnce of NGOs in conflict intervention: Problcms and proswcts. Cambridge, MA: The Local Capacities for Peace Projcct.
Anderson, M. B., & Woodrow, P. J. (1989). Risine from the ashes: Develoomcnt stratceies at times of disaster. Boulder, CO: Wcstview Press, & Paris: UNESCO Press.
Armenian, H. K. (1989). Perceptions frorn epidcmiologic research in an endcmic war. Social Science and Mcdicinc. 28(7), 643-647.
Aronson, G. (1990). tsrael. Palestinians and the Intifada: Creatinc facts on the West Bank. London: Kegan Paul International, L Washington DC: Instirute for Palestine Studies.
Amri, N. (Ed.). (1983). Occupation: lsrael over Palestine. Belmont, MA: Association of Arab American Graduates.

Aston, D. G. (1992). Cambodia: A pro~osal for the rchabilitation of the disabled. Unpublislied manuscript.
Atshan, L. (1997). Disability and gender at a cross-roads: A Palestinian perspective. In L. Abu- Habib (Ed.), Gender and Disabilitv: Wornen's exoeriences in the Middle East @p. 53- 59). Oxford: Oxfam UK and Ireland.
Ballantyne, S. (1 988). Ph~siothenpv fkt-findina visii. West Bank and Gaza S trip. Limassol, Cypnis: Middle East Council of Churches.
Barghouthi, M. (1994). Palestinian NGOs and their role in buildine a civil societv. Jerusalem: UPMRC.
Barghouthi, M., & Daibes, 1. (1993). Infiastructure and health services in the West Bank: Guidelines for health care plannina (The West Bank rural PHC survev). Ramallah, West Bank: Health Developrnent Information Project.
Barghouthi, M., & Ciacaman, R. (1 990). The Emergence of an Infrastnicturc of Resistance: The Case of Hcalth. In J. Nassar & R. Heacock (Eds.), Intifada: Palestine at the crossroads @p. 73-87). Birzeit, West Bank: Birzeit University, & New York: Praeger Publishers.
Barghouthi, M., & Giacaman, R. (1991, March). The irn~act of lsraeli oolicv on health conditions in the lsraeli Occu~icd Territories dunnpthe War in the Gulf. Birzcit, West Bank: Birzcit University Community Hcalth Unit.
Barton, A. H. (1969). Cornmunities in disaster: A Socioloaical analpis of collective stress situations. New York: Doublcday & Co.
Bellisari, A. (1991). Health and medical care in the Occu~ied Temtories. (Special report 110.2) Washington, DC: Center for Poiicy Analysis on Palestine.
Benvenisti, M. (1984). The West Bank Data Proiecr: A Survev of Israel's ijolicies. Washington, DC: Amencan Enterprise Institute for Public Policy Research.
Black, M. (1993). Collapsing health care in Serbia and Montenegro. British Mcdical Journal. 307, 1135-1 137.
Boyce, W. (1998). Mid-term ~erfonnancc evaluation of the Comprehcnsive Disabled Afghan's Proeramrne. Peshawar, Pakistan: UNDPNNOPS.
Boyce, W., & Ballantyne, S. (1997, Aupst - September). Community based rehabilitation in areas of amed conflict. In Proceedings of the 8th World Conmess of the International Rehabilitation Medicine Association (IRMA VI11). moto Jaoan. Bologna, Italy: Monduzzi Editore S.P.A.
Boyce, W., & Weera, S. (1998). lssues of disabilitv assessrnent in war zones. In, 1998 Bonn Symposium on Culture and Disability (In press).

Brazzclli, M. (1 995). Rehabilitation needs in Palestine: A survey in the West Bank. Phvsiothera~v Theorv and Practice, 1 1,5 1-53.
Bruun, F. J. (1995). Hero, beggar, or spom star: Negotiating the identity of the disabled person in Nicaragua. In B. Ingstad % S. R. Whyte (Eds.), Disability and Culture @p. 196-209). Berkeley, CA: University of Calfornia Press.
Bryce, J . W., Walker, N., Ghorayeb, F., & Kanj, M. (1 989). Life experiences, response styles and mental hcalth among rnothers and children in Beimt, Lebanon. Social Science and Medicine. 28(7), 685-695.
Bush, K. D. (1996). Beyond bungee cord hurnanitarianism: Towards a developmcntal agenda for peacebuilding. Canadian Joumal of Develo~ment Studies [Special Issuc J.
CNCR (Central National Cornmittee for Rehabilitation). (1992). Guidelines for the national rehabilitation policv in the West Bank and Gaza. Jenisalem: Author.
COPEDU. (1989). The effects of torture and political repression in a sample of Chilcan families. Social Science and Medicine. 28(7), 735-740.
Cairns, E. (1997). A safer future: Reducing the human cost of war. Oxford: Oxfarn UK and Ireland.
Carballo, M.., Simic, S., % Zcric, D. (1996). Health in coumies tom by conflict: Lessons from Sarajevo. Lancct. 348,872-874.
Carey, P. (1990). War of the mines. The Tndeoendent Magazine, 30-38.
Centcr for Policy Analysis on Palestine. (1992). Facts and Figures about thc Palestinians. (Information Paper No. 1). Washington, DC: Author.
Chaudhury, G., Menon-Sen. K., & Zinkin, P. (1995). Disability Programmes in thc Cornmunit).. In P. Zinkin & H. McConachie (Eds.), Disabled Children and Develooine Countries (pp. 152- 182). London: MacKeith Press.
Coleridge, P. (1993). Disabilitv. libention and develooment. Oxford: Oxfm UK and Ireland.
Commins, S. (Vol. Ed.). (1996). Development in states of war. In D. Eade (Series Ed.) Deveio~ment in Practice Readers. Osford: Osfarn UK and lreland
Coupland, R., & Korver, A. (199 1). Injuries from antipersonnel mines: The expcrîence of the International Committeç of the Red Cross. British Medical Joumal. 303, 1509 - 15 12.
Craissati, D. (1996, March). Social movements and dcrnocracy in Palestine: Politicization of society or civilization of politics? ORIENT - German Joumal for Politics and Economics of the Middle East, 37(1), 1 11-136.
Cnsp, J. (1989). Disabled refugees: Coming out of the shadows. W H C R ReFueees. 66, 19-22.

Despouy, L. (1991). Human riehts and disability. UN Economic and Social Council, Commission on Human Rights, Subcommission on Prevention of Discrimination and Protection of Minorities, 43rd session, Paper no. E/CN.4/Sub.2/199 113 1.
Eade, D., & Williams, S. (Eds.). (1995). The Oxfam handbook of develooment and relief (Vol. 1). Oxford: Oxfam UK and Ireland.
FAFO (Institute for Applied Social Science, Nonvay). (1994). Palestinian socicty in Gaza. West Bank and Arab Jerusalem: Summarv of a survw of living conditions. Toyen, Nonvay: Author.
Forsby, A. S. (1 995, February). CBR in practice: a personal report from the West Bank and Gaza Strip. NU: Nvtt orn U-landshalsovard (News on Health Care in Developinn - Countries). 9, 37-40.
Gaff, A. (1994). The human riehts of ~ersons with disabilities. h a l l a h : Al-Haq.
Garbarino, J., Kostelny, K., & Dubrow, N. (1 99 1). Palestinians in revolt: Children of the Intifada. In 1. Garbarino, K. Kostelny, & N. Dubrow (Eds.). No Place To Be A Child: Growing UP in a War Zone (pp. 101-129). Toronto, Lexington: Lexington Books.
Garfield, R. ( 1989). War-rclatcd changes in health and health services in Nicaragua. Social Science and Mcdicine. 28(7), 669-676.
Giacaman, R. (1984). Plannine for health in Occuoied Palestine. Birzeit, West Bank: Birzeit University Cornmunity Hcalth Unit.
Giacaman, R. (1991). The disabled in the vill3ge of Nahalin. Bethlehem, West Bank: Caritas Baby Hospital Rural Health Tarn.
Giacaman, R. (1993). Disabilitv and rehabilitation needs in the Gaza Strio: A survel! report on Bureii and al-Shati rcfuecc camps. Gaza City: G u National Cornmittee for Rehabilitation, & Diakonia, Sweden.
Giacaman R., & Daibes, 1. (1989, October). Towards the formulation of a rehabilitation oolicv: Disabilitv in the West Bank. Birzeit, West Bank: Birzeit University Community H d t h Unit.
Giacaman, R., & Haramy, G. (1996). A audy of 19 Palestinian communities in the southem district of the West Bank. with special rcfcrence to the necds of Dcrsons with disabilities. West Bank: The Southcm Regional Cornmittee for Rehabilitation.
Gibson, K. (1989). Childrcn in Political Violence. Social Science and Medicine. 28(7), 659667.
Gilgun, J.F. (1994, My). A Case for Case Studies in Social Work Research. Social Work. 39(4), 371.380.

Godfiey, N., & Kalache, A. (1989). Health needs of older adults displaced to Sudan by \var and famine: Questioning current targeting practices in health relief. Social Science and Medicine, 28(7), 707-7 13.
Graham-Brown, S. (1983). The economic consequences of the Occupation. In N. Amri (Ed.), Occuoation: Israel over Palestine @p. 167-222). Belmont, MA: Association of Arab Anieiican Graduates.
Habibi, G. (1994, June). A alance at the situation of disabled children. Paper prcsented at the International Year ofthe Family Confcrence on the UN Convention on the Rights of the Child (Stronger Children - Stronger Families), University of Victoria, British Columbia.
H a m y , G. (1993). CBR challenge in the Occupicd Territones. AHRTAG CBR News. 14.4-5.
H a m y , G., Parson U., 8: Giacaman, R. (1995, October). A studv of 23 Palestinian villages in the central district of the West Bank. with s~ecial reference to the nceds of ~ersons with disabilities. West Bank: The Central Regional Cornmittee for Rehabiiitation.
Hastie, R. (1997). Disabled children in a societv at war: A casebook from Bosnia. Oxford: Oxfam UK and Ireland.
Heiberg, M., & Ovensen, G. (1994). Palestinian scietv in Gaza. West Bank and Arab Jerusalem: A survev of living conditions. Toyen, Nonvay: FAFO (Institute for Applicd Social Science).
Hclander, E. (1992). Preiudicc and die ni^. New York: United Nations Devcloprnent Programme, Division for Global and Intemgional Programs.
Hclander, E. (1993). What is in a definition? AHRTAG CBRNews. 13,3.
Hclandcr, E., Mendis, P., Nelson, G., & Goerdt, A. (1989). Training in the communitv for people with disabilitics. Gcneva: World Health Organization.
Hiltermann, J. R. (1 991). Behind the Intifada: Labor and rvomcn's movements in the Occuoied Temtorics. Princeton NJ: Princeton University Press.
ICACBR (International Centre for the Advancement of Community Based Rchabilitatioa). (1 993, September). CBR: The Debate. ICACBR Update. 1.2,3.
ICACBR. (1996, December). Communitv bascd rchabilitation ~roiect in Bosnia-Herze~ovina: Final report. Quecn's University, Kinsston, ON: ICACBR & The World Health Organization.
ILO, UNESCO, & WHO. (1994). Communiw-based rehabilitation: For and with peoole with disabilities. (Joint position paper.) Gcneva: Authon.
International People's Health Council. (1995). The conccDt of health under national dernacratic stm& lerusalem: UPMRC.

Ityavyar, D.A., & Ogba, L.O. (1989). Violence, conflict and health in Afnca. Social Science and Medicine. 28(7), 649-657.
Jarrar, A., & Giacaman, R. (1994, August). A studv of 22 Palestinian villaees in the Jenin district, uith special reference to the needs of persons with disabilities. West Bank: Northern Regional Cornmittee for Rehabilitation.
Jenson, G. M. (1989). Qualitative rnethods in physicai therapy research: A form of disciplinai inquiry. Phvsical Thera~v. 69(6), 76-84.
Khamis, V. (1992-93). Fa'iliayat mu'assassaat a-iathil al-falastiniya li mu'aaqi al-intifada (Eff'çctiveness of the rehabilitation institutions for the Intifada disabled). Bethlehem Universitv Journal. 1 1-1 2,87-97.
Kisanji, J. (1995, January - April). Understanding CBR Models. AHRTAG CBR News. 19,4.
Krammer, W. (1990, Junc). Medical studv on the Phvsiothera~v Emeraencv Proeramme. Gaza S t r i ~ . Gaza: üNICEF/UNRWA.
Krefting, L. ( 199 1). Rigor in qualitative rescarch: The assessrnent of tnishvorthincss. Amencan Journal of Occupational Thera~ 45(3), 2 14-222.
Lockman, Z., & Beinin, j. (Eds.). (1 989). Intifada: The Palestinian Uprisine apainst lsraeli Occupation. Boston MA: South End Press, MERIP.
Lundgren, R.I., & Lang, R. (1989). niere is no sea, only fish': Effects of Unitcd States policy on the hcalth of the displaccd in El Salvador. Social Science and Medicine 28(7), 697-706.
MacGrory, R. (1996, May). General Union of Disabled Palestinians. RamaIlah: GUDP.
Machel, G. (1996). Impact of armcd conflict on children. UNICEF wcb page, http://~~wwnicef.org/graca, I April 1999.
Macrac, I., & Zwi, A. (1994, January). When the \var is over: Spcculations on the relieffdevelopment transition and its implications for the health sector - The case of Unanda. ~ a i e r submined for pesentat& to the 4th International Research & Advisory Panel Confcrcncc, Rcfugec Studies Programme, Somerville Cokge, Osford.
Marshall, C., Rossman, G. (1989). Desimine Qualitative Research. Newbury Park: Sage.
Mash'd, J. (1 990). Knowledge. attitude and pnctice of the carers of children with disabilities in the West Bank (Palestinel Unpublishcd master's thesis, Institute of Child Health, University of London, England.
Mash'al, J. (199 1, April). Caring for disabled childrcn in the West Bank and Gaza Strip. AHRTAG CBR News, 8, 4-5.
Mash'al, J. (1993). The communitv based rehabilitation Droeramme of the Union of Palestinian Medical Relief Comniittecs, West Bank and Gaza S t r i ~ . Jerusalem: UPMRC.

McColl, M. A., & Paterson, I.A. (1995). Critical dimensions of cornrnunitv-based rchabilitation: Develo~mcnt of a descn~tive framework for CBR. Kingston, ON: Queen's University School of Rehabilitation Therapy & ICACBR.
Mendis, P. (1996, April-May). Communitv-based rehabilitation KBR) aroeram. West Bank and Gaza Strip: Report of an evaluation mission.
Miles, M. B., & Hubcrman, A. M. (1984). Analvzinn qualitative data: A sourcebook for new rnethods. Beverly Hills: Sage.
Minear, L., & Weiss, T. G. (1993). Humanitarian action in times of war: A handbook for practitionen. Boulder & London: Lynne Reinnef Publishers.
Mooney, T. L. (Ed.). (1 995). The challenge of develo~ment within conflict zones. Pans: Dcvelopment Centre of the Organization for Economic Cooperation and Dcvcloprnent (OECD).
Nassar, I. R., & Heacock, R. (Eds). (1990). Intifada: Palestine at the crossroads. Bineit, West Bank: Birzeit University, & New York: Praeger Publishers.
Nixon, A. (1990). The status of Palestinian children durine the Uprisine in the Occu~ied Territories: Child Dcath and In-iury. Radda Bamen (Swedish Save the Children).
PASSIA (Palestinian Acadcmic Socicty for the Study of International Affairs). (1 999, Apnl). Wcb page, http://w~~nv.passia.ordpalcstine facts/chronology/O chronology.htm.
Palestinian Central Burcau of Statistics. (1997, January). The hcalth survev in the Wcst Bank and Gaza Strio: Main findings. RamalIah, Palcstinc: Author.
Palestinian Central Bureau of Statistics. (1 999, April) http://wn~~v.pcbs.org/englishlphc~97/popu.h~
Patton, M. Q. (1990). Oualitative cvaluation and research methods (2nd cd.). Newbury Park: Sage.
Peat, M. (199 1). Community based rchabilitation: Developmcnt and stmcture. In Community based rehabilitation: lntemational oers~cctives. Kingston, ON: Quccn's University, & Bombay, lndia: Scth G. S. Mcdical College.
Peat, M. (1997). Comrnunitv bascd rchabilitation. London: W.B. Saundcrs.
Peat, M., Koros, M., Boyce, W., Edrnonds, LJ, Smith, J., Ballantqne, S. (1997). Community based rehabilitation: A pcacc buildinc o~oortunih?. Quecn's University, Kingston, ON: ICACBR.
Pereîz, D. (1 990). Intifada: The Palest inian Uorising . Boulder, CO: Westview Press.
Physicians for Human Rights. (1988). The casualties of the conflict: Medical care and hurnan riehts in the West Bank and Gaza S t r i ~ . Somerville, MA: Author.

RUUNICEF. (1 989-90). Community-based rehabilitation: A ten ycar review. One in Ten, 8(14), 9(1-2). -
RI/UNICEF. ( t 99 A). Effects of armed conflict on women and children: Relief and rchabihtion in war situations. One in Ten. 1 O(2-3).
Rankin, W. (1991). Growing up in hatred. Journal of Pediatnc Nursine. 6(1), 60-6 1.
Rautio J., Paavolainen P. (1988). Afghan war wvoundcd: Experience with 200 cases. Journal of Trauma. 28(4), 523-525.
Richman, N. (1995). Violcnce and disabled children. In P. Zinkin & H. McConachie (Eds.). Disabled children and developinn countries @p. 203-2 13). London: MacKeith Press.
Rigby, A. (1 99 1, Sumner). Coping wvith the "epidemic of violence7': The struggle over health care in the Intifada. Journal of Palestine Studies. 20(4), 86-98
Roy, S. (1 995). The Grva S t r i ~ : The ~olitical economv of dedeveloprnent. Washington DC: Institute for Palestine Studies.
Ruff, T., & Ward, J. (199 1). The Middle East War - A medical perspective. The Medical Joumal of Australia. 55,3942.
Saleh, S. A. (1 990). The effects of Isneli Occupation on the econorny of the West Byik and Gaza Strip. In J. R. Nassar & R. Heacock (Eds.), Intifada: Palestine at the Crossroads (pp. 37-5 1). Birzeit, West Bank: Birzcit University, & New York: Pneger Publishers.
Salem, M. O. (1990, October). Stinma and the origin of disabih: The case of the Palcstinians. Unpublishcd master's thesis, Sociology Dcpartment, Faculty of Economics and Social Sciences, University of Manchester, England.
Saicrn, M. O. (1992). A documentation of the ewerienct: of sehreanization arnanp ~hvs i cdk disabled aalçstinians. Birzeit, West Bank: Birzcit University Cornmunity Hcalth Unit.
Schaller, J. G., & Nightingale, E. 0. (1 992). Childrcn and childhds: Hidden casualties of war and civil unrest. JAMA. 268(5), 642-644.
Siegel, D., Baron, R., & Epstein, P. (1985, lune). The epidemiology of aggression: Health consequences of cvar in Nicaragua. The Lancer. 8440, 1492- 1493.
Smith, C. (1987). Hcalth develooment in the Gaza Strio: A case for the suppon of local nrouus. Birzeit, West Bank: Birzeit University Community Health Unit.
Stake, R. (1995). The an of case studv research. Newbury Park: Sage.
Taraki, L. (1990). n i e development of political consciousness among palestinians in the Occupied Territories, 1967-1987. In J. R. Nassar & R. Heacock (Eds.), Intifada: Palestine at the crossroads (pp. 53-71). Birzeit, West Bank: Bineit University, & New York: Praeger Publishers.

Tesch, R. (1990). Qualitative research: Analwis hges and software tools. New York: Falmer Press.
Toole, M., Galson, S., & Brady, W. (1993). Are war and public health compatible? Lancet. 341, 1193-1 196.
UN (United Nations). ( 1 989). Convention on the rights of the child. Ottawa: Human Rights Directorate, Depariment of Multiculturalism and Citizenship, Governmcnt of Canada.
LTNDP (United Nations Development Program). (1994). Human develooment report. New York, Oxford: Oxford University Press.
WNHCR (United Nations High Commission for Refugees). (1992). UNHCR yi~c l ines on assistance to disabled refiiaees. Gcneva: Author.
UNICEF (United Nations Children's Fund). (1986a). Overview: Children in especiallv dificult circumstances. Executivc Board, 1986 Session, Paper No. EACEF/ l986L.6
UNICEF. (1986b). Children in situations of armcd conflict. Executive Board, 1986 Session, Papcr No. EACEF/1986/CRP.2
UNICEF. (1 990). Childrcn in Espccially DiEcult Circumstances. In Children and devdo~ment in the 1990s: A UNICEF sourcebook (Part Sis). New York: Osford University Press.
UNICEF. (199 1). The state of the world's children 1990. New York: Oxford University Press. (p.
UNICEF. (1994). Anti-ocrsonncl land-mines: A scouree on childrcn. New York: WICEF House.
UNICEF. (1 996). Thc state of the world's children 1996. New York: Osford University Press
UNCTAD (United Nations Conference on Trade and Developmrnt). (1993). Prospects for sustaincd dcveio~mcnt of the Palcstinian economv in the West Bank and thc Gaza S t r i ~ . UNCTAD/DSD/SEU/Z 27 September 1993.
UNRWA (United Nations Relief and Works Agcncy for Palestinian Rehgccs). (1 992, May). Comrnunitv rehabifitation Drocrammes for disablcd Palestine rcfusecs. Rcport and Recornrnendations of üNRWA/NGO Confercnce, Amman, Jordan.
UPMRC (Union of Palcstinian Mediwl Relief Cornmittees). (1987, August). An overview of health conditions and serviccs in thc Israeli Occu~ied Temtories. Jerusalcm: Author.
UPMRC. (1988). The Uprisine: Conseauences for health and Palestinian reseonse. Jerusalem: Author.
UPMRC. (1992). 1992 Re~ort. Jerusalem: Author.
UPMRC. (1994). n i f l health care develo~mcnt 1974 - 1994. Jenisalem: Author.

United Nations Comrnittee on the Exercisç o f the InaIienable Rights of the Palestinian People. (1990). The oneins and evolution of the Palestinian oroblern 19 17- 1988. New York: United Nations.
Vandam, S. (1989, September). Survev o f phvsiothera~v services in the West Bank. Brussels: Medecins Sans Frontiers.
Verhceff, T. (1 989). Phvsiotheraov Gaza and West Bank: Januarv 1 992. International Comrnittee of the Red Cross.
von Kotze, A., & Holloway, A. (1996). Reducine nsk: Participatorv leamins activitics for disaster mitkation in Southem AFnca. International Federation of Red Cross and Rcd Crescent Societies & Dcpartment of Adult and Community Education, University of Natal.
WHO (World Health Organization) Expert Cornmittee on Disability Prevention and Rchabilitation. (198 1). Disability prevention and rehabilitation. WHO Technical Rer101-t Series. 668, 7- 37.
Weiss, T., & Mincar, L. (Eds.). (1993). Humanitarianism across borders: Sustahine civilians in times of war. Boulder & London: Lynne Reinner Publishcrs.
Werncr, D. (1987). Disablcd villave children. Palo Alto, California: The Hesperian Foundation. (p. 14).
Wemer, D. (1990a). Staning in a village - where to bcgin? AHRTAG CBR News. 7,698.
Werner, D. (1 990b). Visit to Angola: Where civilians arc disablcd as a stntcgy of low intensity conflict. Disabilitv Studies Quartcrlv, 10(2), 36-39.
World Bank. (1993). Developine the Occu~ied Territones: An investment in pcace - Vol. 2: The Economv. Washington DC: Author.
Wu, G. (1997). Let thcm have CBR: Adeauacv of comrnunitv-based rehabilitation (CERI as resoonsc to disabili~ in develooinp countrics. Unpublishcd bachclor's paper, Queen's Univenitv, Kingston, ON.
Yin, R. K. (1984). Case studv rescarch: Desien and methods. Beverly Hills: Sage.
Zwi, A., & Ugalde, A. (1989). To~vards an epidemiology of political violcnce in the Third World. Social Scicnce and Medicine 28(7), 63 3-642.
Zwi, A. and Ugalde, A. (1991). Political violence in the Third World: a public hcalth issue. Health Policv and Plannina 6(3), 203-2 17.

APPENDIX 1.
CAPACITIES AND VULNERABILITIES ANALYSIS
(adapted fiom: Anderson and Woodrow, 1989; Anderson, 1994a)
The CVA framework distinguishes h e e realms of capacities and vulnerabilities. These are:
Physicd / Material: these include features of the land, climate and environment, people's health, skills and labour, infrastmcture, bousing, technologies, water and food supply, physical technologies, capital and other assets.
Social 1 Organizationd: this refers to the social fàbric of a population or group, and includes stnictures like fàmilia and kinship groups such as clans, social and political organizations, and synm>s for diaributing goods and services. It therefore includes forma1 and informal system through which people get things done, such as making decisions, establishing leadership, or organizing various social and economic activities.
Motivationai / Attitudinal: these include cultural and psychological factors that may be based on religion, history, and expectations. It reflects how the community views ifself, including its beliefs, motivations, and sense of empowerment or dependency.
The three realms of vulnerabilities and capacities are represented in the matrix. n i e analysis always refers to factors at the community level, rather than at the individual level. The intemal lines in the matrix are dotted because the categories overlap and there is constant interaction among them.
Vulnerabilities Capacities
What productive resources, skills, and hazards exist?
Social / Organizational
What are the relations and organization among people?
Motivational / Attitudinal
How does the community view its ability to create change?

APPEND lx II.
INTERVIEW QUESTION GUIDE
Questions were based on a set of eight 'elements' in CBR developed for this study.
Note to respondents: the ternis "Occupation" and "Uprising" refer to the conditions of confiict in which you lived and worked (for example, curfcws or strikes, violence, threats).
Romoting posif ive community attitudes towards disability and people with disabiliries What have been the gcneral attitudes (and behaviours) totvards disabled people?
positive / negative / charitable ... * how did the Occupation / Uprising affect these?
To what degrec has this program influenced attitudes towards disability? * how 1 why not? * reasons for effectiveness / little effectiveness?
Romoting in tepration of people ivith disa bilities with in society How do you think thc Occupation / Uprising affected people with disabilities in being fully active and involved within society?
no cffcct / made easier / made more dificult? To what degrec has this prognnl enabled pcople with disabilitics to takc part in society?
how / why not? * rcasons for cffectiveness / little effcctivcness?
Tramferring rchabili~a f ion kn oivlcdge and skills (trainin@ In gencral, to what degree are pcople with disabilities and their familics becoming educatcd, and lcarning the skiils to takc care of thcmselves?
* how / why not? * did the Occupation i Uprising affect this? How?
How has this proçram woked ro educate and teach self-lirlp skills? rçasons for effectivcncss / little effectiveness?
Roviding particim~nt-rlirected rehabilitation services To what dcgree have people with disabilities and their families havc bccn involvcd with making decisions about this program's rehabilitation services, so that scrvices are based upon their ow expressed needs?
* how / why not? how did the Occupation / Uprising affect this?
Implcrnenthg the programme ivith cornmunit 11 nartici~ation To what degree has the community bccn involvcd with this program in: making decisions, running the program, taking responsibility? (decision-mnking. implementation, itcco~rntcrbiliry)
how / why not? how did the Occupation / Upnsing affect this?

$ Erliibiting a model of partnershin among people with dimbilliies, families, the community, and reh ttbilitation personnel To what degree have people with disabilities, their families, the communitv, and rehabilitation workers cooperated and worked together as partners?
how / why not? how did the Occupation 1 Upnsing affect this?
Usimg locaIIpmade rehabilifation aids and equipment (iechnnlom) To what degree were local matenals and workers used to make rehabilitation equipmentfaids?
+ how / why not? how ddi the Occupation 1 Uprising affect this?
b Participating in a referral nehvork luith specialists and institutions, fior professions/ and tech nical reh u b i h t i o n supporî To what dcgrce did the communig program coordinatc with, and refer to, an outside network of professiomls and institutions for treamienil trainingkquipment?
* how / why not? how did the Occupation / Uprising affect this?
also: Would you like to add any othcr elcments of Cornrnunity Based Rehabilitation bat may not havc been mcntioncd?
Overall, do you feel that Cornmunity Bascd Rehabilitation works well in the conditions of the Occupation and Uprising?
OTHER DATA COLLECTION:
Document rcview, and intcrvicws with representatives of the UPMRC, elaborated upon: i) the history of the UPMRC rehabilitation programme ii) thc structure of the programme iii) programme mandate and act ivities iv) obstacles and programme strategies v) programme rcsources and support

APPENDIX III.
DATA ANALYSIS TOOLS
1. Process Diagram
Conditions CBR elements
occ
Int Train C- efficcts
upon
Programme responses

2. Sample Codes
Background back.cult back. reg back.prof back.att
Conditions cond. occ
cond.occ.miladmin cond.occ.popdis cond.occ.adminbam cond.occ. policies cond.occ.milact
cond.int cond.int.non-v cond.int.viol cond.int.injured cont.int.support
Work work. rep work.res
Int int.effects int.effects. rep int.efficcts.int int.responses
Contextual or background factors culture regionuf & comrnunity characteristics profesionulization / insfifutionalizaiion' of disability attitudes rowards disability
Conditions of political violence Occupation (conditions of repression) military administration population dislocation administrative barriers policies of control and punishment military actions Inti fada (conditions of rais f ance) non-violent communiîy resistance violent resislance actions inrifada-injured internafionaf support
EfJects of conditions on dailv activities of CBR W S E'ects of occupu fion Eflecis of inttjada
CBR Elerncnt: prornoting +ve uttitiides Eflccts a/conditions on elernent of artirudes Eflccts of ocaipotion Efïcts of inrifada CBR program responscs
CBi? Elment: integration Efecn of conditions on elemcnr of integration Effccrs of ocnipotion Effccts of inrifada CBR program responses
... [Train ... Serv ... Comm ... Pa R... Tech ... Refl
Activities CBR program aclhlities

3. Matrix summarizing findings and noting processes
1 . attitudes
1 2. integration
1 3. training 4. bencficianes
direct services
5 . community involvement
6. partnership
17. technology
OCCUPATION CONDITIONS, UPRISMG CONDITIONS, having : having : negativc effects Positive effects Ncgative effects poSitive effects
1
i IS, r
KEY:
OCCüP ATION Conditions UPRISMG Conditions
A... Miiitary administration P.. . Policics of occupation
and punishment M... Military actions B... Administrative barriers
W.. . Violent resistancc CR.. . Non-violent comrnunity resistance 1.. . Intifada-injurcd S . . International support
@rackets) indicate a less sipificant effiect
arong indication of relationship (Occupation -ve I Intifada +ve)
[/ moderate indication of relaiionrhip
-1 no indication of relatiowhip

APPENDTX IV.
INFORMATION AND CONSENT FORM
TlTLE OF PROJECT: Community B a d Rehabilitation Under Conditions of Political Violence - A Case Study of the Union of Palestinian Medical Relief Committees
RESEARCHER: Sandra Ballantyne BSc.(PT), MSc candidate Queen's University, Kingston, Cana& O1 1-6 13-545-6 103
ACADEMIC ADMSOR: Professor Will Boyce School of Rehabilitation Therapy, Queen's University O1 1-613-545-6726
Dircctor of School of Rehabilitation Therapy: Dr. Malcolm Peat 0 1 1-6 13-545-6 1 O4
You are being asked to participate in a research project to descnbe the community bascd rehabilitation program of the Union of Palestinian Medical Relief Committees (UPMRC). The purpose of this study is to understand how community based rehabilitation is provideâ in circumstances of political violence. nie researcher will read through this consent form with you, and answer any questions you rnay have.
You will be interviewed by the researcher one or bvo times, each interview lasting approximately one and a half hours. During these i n t c ~ e w s you will be asked questions about how the conditions of the Uprising affectcd rehabilitation of people with disabilities, and how the UPMRC program worked undcr these conditions. The interviews will be tapcd, and these tapes will not be shared with anyone else. The rcscarcher will type thcse conversations for use, and thcn the tapes will be erased. The wvrinen pages of the interviews will be kept without your name attached. The information will be kept in a locked location, and only the researcher will have access. The final report, wvith anonymous quotations, \ d l be sent to the UPMRC at the end of the snidy, and everyonc wvho was interviewed will be notified that the report is available.
This study will not be of direct benefit to you, but others in situations like yours may benefit fiom your description of your experiences. Due to political sensitivities, you rnay be at some risk, as information about activities during the Uprising will be shared. If you decide not to continue with the study, you may stop at any time.
1 have read and understand this consent form. 1 have been given time to consider it, and get advice. By signing this form, 1, , agree to participate in this study. 1 understand the information may be published, but that my name will not be associated with the research. I understand that 1 rnay choose to not answr any specific question, and 1 may withdraw at any the . Al1 of my questions have been answered to my satisfaction. 1 will receive a copy of this consent f o m for my information.
participant \r i tness researcher date








![Conceptual Modeling Tips and Common Mistakes - Jarrar · [11] Mustafa Jarrar: Towards Methodological Principles For Ontology Engineering. PhD Thesis. Vrije Universiteit Brussel. (May2005)](https://img.pdfslide.net/doc/110x75/5f10d2147e708231d44af9a2/conceptual-modeling-tips-and-common-mistakes-11-mustafa-jarrar-towards-methodological.jpg)