Embed Size (px)
Citation preview

The Functional Significance of the First Thoracic Ganglionin Sympathectomy of the Upper Extremity in Man *
K. B. COLDWATER, PH.D., M.D.,* * W. F. ALEXANDER, PH.D.,J. W. Cox, M.D., PH.D.,j W. C. RANDALL, PH.D.tt
From the Veterans Administration Hospital and the Departments of Physiology and Anatomy,St. Louis University School of Medicine, St. Louis, Missouri
THE SPINAL LIMITS of origin of the sym-pathetic preganglionic fibers for the upperextremity have been reported to be fromthe levels of T2 to T7, or even as low asT9.2'6' 7,9,16 With a few notable excep-tions,10 11,12 most investigators have con-sidered the upper limit to be T2 in man,with but little emphasis upon the possibil-ity that Ti may contribute significantly tothe innervation of the arm and hand. Thesepreganglionic sympathetic fibers are saidto enter the sympathetic trunk and ascendto the inferior cervical ganglion, or ter-minate in the first and second thoracic gan-glia. Postganglionic fibers from the inferiorganglion (if present as a separate struc-ture) supply the C5 to C8 cervical nerveswhile postganglionic fibers from the Tiganglion innervate the 7th and 8th cervicaland first thoracic nerves.Smithwick 16 proposed a preganglionic
sympathectomy in which the second andthird thoracic ganglia are decentralizedand the second and third intercostal nervessectioned intradurally. This procedure wasbased upon the supposition that extirpa-tion of the inferior cervical as well as thefirst thoracic ganglion renders the bloodvessels of the extremity more sensitive tocirculating adrenalin. Modifications of this
* Submitted for publication Sept. 28, 1956.Formerly Chief Surgical Service VA Hospital,
St. Louis, Mo.+ USNR, U. S. Naval Hospital, San Diego,
Calif.ft Director, Department of Physiology, Stretch
School of Medicine, Loyola University, Chicago,Ill.
procedure have been proposed by manysurgeons. Some have even suggested thatremoval of only the second dorsal ganglionprovides adequate sympathectomy of theupper extremity.
Failure to achieve satisfactory resultsfrom sympathectomy of the upper extrem-ity would be puzzling indeed if the out-flow of its preganglionic fibers were limitedto the segments indicated above. We havetherefore extended our experience in thedirect electrical stimulation of the lumbarsympathetic trunk in man4"4 to the cer-vico-thoracic division and recorded thesudomotor responses to such stimulation onthe upper extremity and the anterior chestwall.
EXPOSURE AND STIMULATION OF THE TRUNK
The inferior portion of the stellate gan-glion together with the second through thefourth thoracic ganglia were exposed by amodification of the posterior surgical ap-proach, resecting the 2nd and 3rd proximalribs and transverse processes. A bipolarstimulating electrode was applied to the in-terganglionic segments starting betweenthe fourth and third ganglia and proceed-ing craniad. Individual rami between thespinal nerves and the ganglia were stim-ulated wherever possible. As each gan-glionic level was explored and stimulatedthe ganglion was decentralized by transec-tion of its connections and the stimulationprocedure repeated at the next higherlevel until the first four thoracic trunk seg-ments had been stimulated in continuity.
530
Volume 145 THORACIC GANGLIONumber 4
Whenever dissection revealed an intercon-necting ramus between the second and thefirst thoracic spinal nerves, this was gentlyelevated onto the electrode terminals andstimulated. The stimulus employed con-sisted of repetitive pulses delivered from asquare wave generator. The frequency ofstimulation varied from 10-60/sec. withan optimum in the lower range. Varyingvoltages from 0.5 to 10.0, with an optimumat 1.5 to 5.0, were used depending upon thesize of the trunk or ramus being stimulated.Pulse duration was varied from 2-15 withan optimum of 10 milliseconds. The totalduration of stimulation varied from 30 to60 seconds.
Sweating responses elicited by stimula-tion were recorded by the Iodine-Starch-Paper technic.14 One to two inch strips ofstarch-sized bond paper were wrappedaround the full circumference of the arm,proximal and distal forearm, and hand atthe level of the thenar and hypothenareminences. The finger pads were pressedon a strip of the paper. The observationalareas had been previously painted with a2 per cent alcoholic solution of iodine andallowed to dry. Responses of individualsweat glands were recorded as blue spots.The records are quantitative with respectto the number of functional glands per unitarea of skin surface.The cervico-thoracic sympathetic trunk
has been stimulated and removed from 13sides of a total of nine patients. The diseaseentities treated were Raynaud's phenomena,post-traumatic dystrophy, cervical rib, andcausalgia. The sympathetic surgery andstimulation was carried out under endo-tracheal anesthesia (Pentothal, nitrous ox-ide and oxygen). The sympathetic trunksremoved at operation were fixed in Forma-lin and saline and were serially sectionedfor fiber analysis. The results of fiber analy-sis and reconstruction of the fiber topog-raphy from the serial sections was thencorrelated with the results of the functionalresponses to stimulation.
)N IN SYMPATHECTOMY 531RESULTS
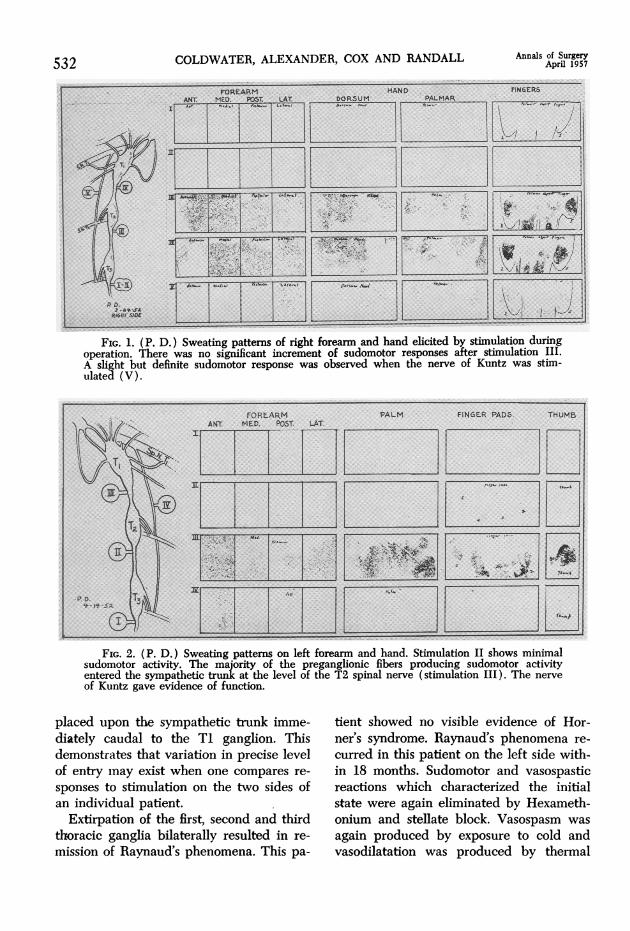
Stimulation of the interganglionic seg-ments caudal to the third thoracic gan-glion consistently failed to elicit significantsweating responses on the upper extremity.Figure 1 illustrates the complete absenceof response on the hand or forearm whenthe electrodes were applied immediatelycaudal to the third thoracic ganglion. Asecond period of stimulation at the samesite confirmed these results. Movement ofthe electrodes to a position immediatelycaudal to the T2 ganglion resulted in arelatively profuse sweating response oneach of the areas under observation andessentially similar results were obtainedupon stimulation between the T2 and theTi ganglia. A fifth stimulation was appliedto the interconecting ramus (the Nerve ofKuntz) between the second and the firstthoracic nerves. A slight but very definiteresponse to this stimulation emphasizes thepossible significance of this pathway forsympathetic fibers passing to the periphery.However, its stimulation does not invari-ably elicit a sweating response in all pa-tients.These observations indicate that prac-
tically the entire preganglionic innervationof sweat glands on the hand and forearmof this patient entered the trunk from thelevel of T3 via the communicating ramusfrom the third thoracic nerve. The failureto demonstrate any significant change insweating pattern elicited by stimulationnumber IV, Figure 1, indicates that fiberswere neither added to nor subtracted fromthose excited in the previous stimulation.Similar studies carried out during the re-moval of the upper thoracic trunk from theopposite side of the same patient are illus-trated in Figure 2. Here it is apparentthat the significant entry of preganglionicfibers was at a level one segment higher,i.e., the communicating ramus of the T2spinal nerve. Marked sweating was elicitedonly when the stimulating electrodes were
COLDWATER, ALEXANDER, COX AND RANDALL Annals of SurgeryApril 1957
FIG. 1. (P. D.) Sweating patterns of right forearm and hand elicited by stimulation duringoperation. There was no significant increment of sudomotor responses after stimulation III.A slight but definite sudomotor response was observed when the nerve of Kuntz was stim-ulated (V).
FIG. 2. (P. D.) Sweating patterns on left forearm and hand. Stimulation II shows minimalsudomotor activity. The majority of the preganglionic fibers producing sudomotor activityentered the sympathetic trunk at the level of the T2 spinal nerve (stimulation III). The nerveof Kuntz gave evidence of function.
placed upon the sympathetic trunk imme-diately caudal to the Ti ganglion. Thisdemonstrates that variation in precise levelof entry may exist when one compares re-
sponses to stimulation on the two sides ofan individual patient.
Extirpation of the first, second and thirdthoracic ganglia bilaterally resulted in re-
mission of Raynaud's phenomena. This pa-
tient showed no visible evidence of Hor-ner's syndrome. Raynaud's phenomena re-
curred in this patient on the left side with-in 18 months. Sudomotor and vasospasticreactions which characterized the initialstate were again eliminated by Hexameth-onium and stellate block. Vasospasm was
again produced by exposure to cold andvasodilatation was produced by therrnal
532
Volume 145Number 4
THORACIC GANGLION IN SYMPATHECTOMY
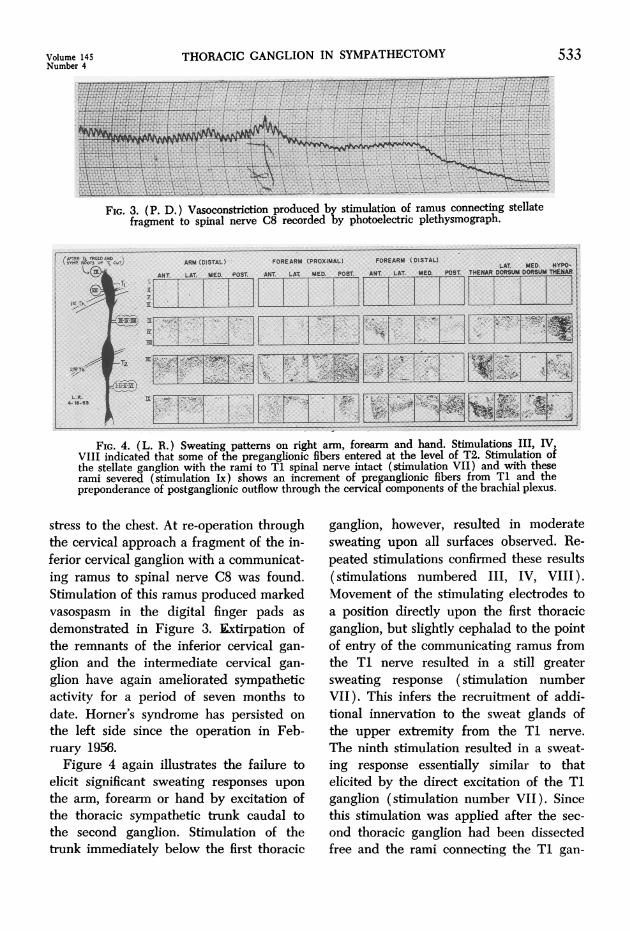
FIG. 3. (P. D.) Vasoconstriction produced by stimulation of ramus connecting stellatefragment to spinal nerve C8 recorded by photoelectric plethysmograph.
FIG. 4. (L. R.) Sweating patterns on right arm, forearm and hand. Stimulations III, IV,VIII indicated that some of the preganghonic fibers entered at the level of T2. Stimulation ofthe stellate ganglion with the rami to Ti spinal nerve intact (stimulation VII) and with theserami severed (stimulation Ix) shows an increment of preganglionic fibers from Ti and thepreponderance of postganglionic outflow through the cervical components of the brachial plexus.
stress to the chest. At re-operation throughthe cervical approach a fragment of the in-ferior cervical ganglion with a communicat-ing ramus to spinal nerve C8 was found.Stimulation of this ramus produced markedvasospasm in the digital finger pads as
demonstrated in Figure 3. Extirpation ofthe remnants of the inferior cervical gan-
glion and the intermediate cervical gan-
glion have again ameliorated sympatheticactivity for a period of seven months todate. Horner's syndrome has persisted on
the left side since the operation in Feb-ruary 1956.
Figure 4 again illustrates the failure toelicit significant sweating responses upon
the arm, forearm or hand by excitation ofthe thoracic sympathetic trunk caudal tothe second ganglion. Stimulation of thetrunk immediately below the first thoracic
ganglion, however, resulted in moderatesweating upon all surfaces observed. Re-peated stimulations confirmed these results(stimulations numbered III, IV, VIII).Movement of the stimulating electrodes toa position directly upon the first thoracicganglion, but slightly cephalad to the pointof entry of the communicating ramus fromthe TI nerve resulted in a still greatersweating response (stimulation numberVII). This infers the recruitment of addi-tional innervation to the sweat glands ofthe upper extremity from the Ti nerve.
The ninth stimulation resulted in a sweat-ing response essentially similar to thatelicited by the direct excitation of the Tiganglion (stimulation number VII). Sincethis stimulation was applied after the sec-
ond thoracic ganglion had been dissectedfree and the rami connecting the TI gan-
533
COLDWATER, ALEXANDER, COX AND RANDALL Annals of SurgeryApril 19S7
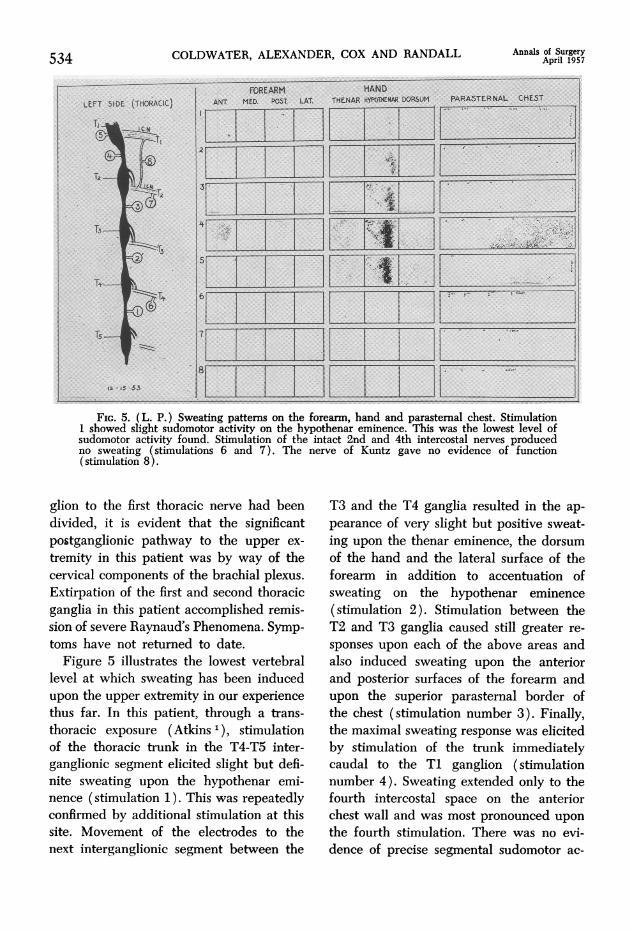
Fir. 5. (L. P.) Sweating patterns on the foreann, hand and parasternal chest. Stimulation1 showed slight sudomotor activity on the hypothenar eminence. This was the lowest level ofsudomotor activity found. Stimulation of the intact 2nd and 4th intercostal nerves producedno sweating (stimulations 6 and 7). The nerve of Kuntz gave no evidence of function(stimulation 8).
glion to the first thoracic nerve had beendivided, it is evident that the significantpostganglionic pathway to the upper ex-
tremity in this patient was by way of thecervical components of the brachial plexus.Extirpation of the first and second thoracicganglia in this patient accomplished remis-sion of severe Raynaud's Phenomena. Symp-toms have not returned to date.
Figure 5 illustrates the lowest vertebrallevel at which sweating has been inducedupon the upper extremity in our experiencethus far. In this patient, through a trans-thoracic exposure (Atkins 1), stimulationof the thoracic trunk in the T4-T5 inter-ganglionic segment elicited slight but defi-nite sweating upon the hypothenar emi-nence (stimulation 1). This was repeatedlyconfirmed by additional stimulation at thissite. Movement of the electrodes to thenext interganglionic segment between the
T3 and the T4 ganglia resulted in the ap-
pearance of very slight but positive sweat-ing upon the thenar eminence, the dorsumof the hand and the lateral surface of theforearm in addition to accentuation ofsweating on the hypothenar eminence(stimulation 2). Stimulation between theT2 and T3 ganglia caused still greater re-
sponses upon each of the above areas andalso induced sweating upon the anteriorand posterior surfaces of the forearm andupon the superior parasternal border ofthe chest (stimulation number 3). Finally,the maximal sweating response was elicitedby stimulation of the trunk immediatelycaudal to the Ti ganglion (stimulationnumber 4). Sweating extended only to thefourth intercostal space on the anteriorchest wall and was most pronounced upon
the fourth stimulation. There was no evi-dence of precise segmental sudomotor ac-
534
THORACIC GANGLION IN SYMPATHECTOMY 535
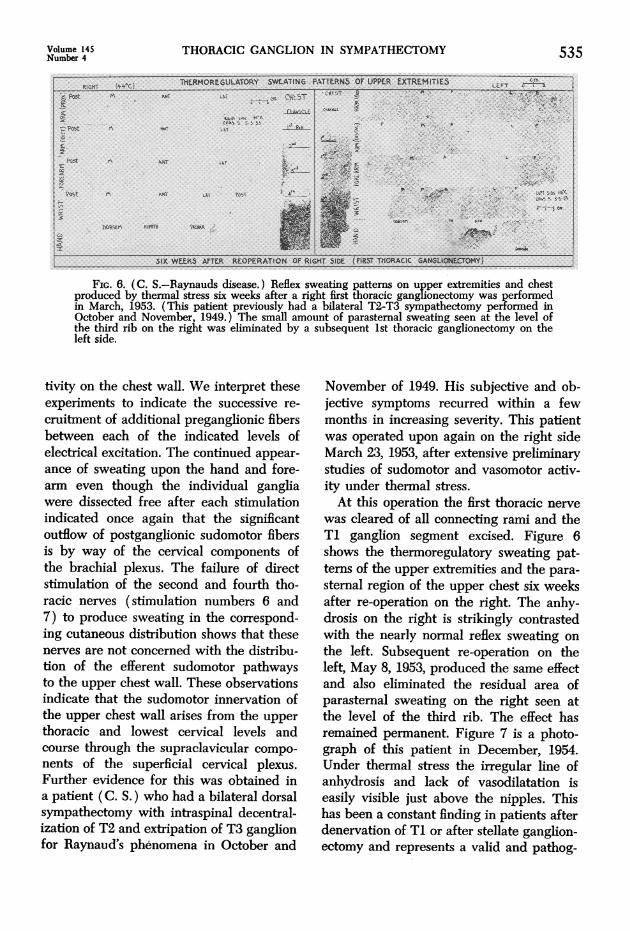
FIG. 6. (C. S.-Raynauds disease.) Reflex sweating patterns on upper extremities and chestproduced by thermal stress six weeks after a right first thoracic ganglionectomy was performedin March, 1953. (This patient previously had a bilateral T2-T3 sympathectomy performed inOctober and November, 1949.) The small amount of parasternal sweating seen at the level ofthe third rib on the right was eliminated by a subsequent 1st thoracic ganglionectomy on theleft side.
tivity on the chest wall. We interpret theseexperiments to indicate the successive re-
cruitment of additional preganglionic fibersbetween each of the indicated levels ofelectrical excitation. The continued appear-ance of sweating upon the hand and fore-arm even though the individual gangliawere dissected free after each stimulationindicated once again that the significantoutflow of postganglionic sudomotor fibersis by way of the cervical components ofthe brachial plexus. The failure of directstimulation of the second and fourth tho-racic nerves (stimulation numbers 6 and7) to produce sweating in the correspond-ing cutaneous distribution shows that thesenerves are not concerned with the distribu-tion of the efferent sudomotor pathwaysto the upper chest wall. These observationsindicate that the sudomotor innervation ofthe upper chest wall arises from the upper
thoracic and lowest cervical levels andcourse through the supraclavicular compo-
nents of the superficial cervical plexus.Further evidence for this was obtained ina patient (C. S.) who had a bilateral dorsalsympathectomy with intraspinal decentral-ization of T2 and extripation of T3 ganglionfor Raynaud's phenomena in October and
November of 1949. His subjective and ob-jective symptoms recurred within a fewmonths in increasing severity. This patientwas operated upon again on the right sideMarch 23, 1953, after extensive preliminarystudies of sudomotor and vasomotor activ-ity under thermal stress.At this operation the first thoracic nerve
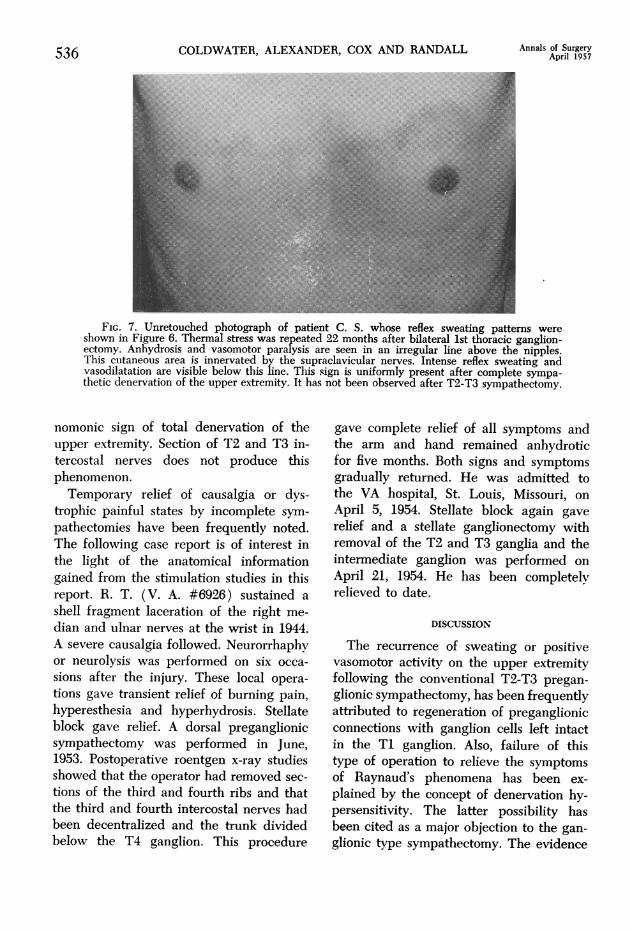
was cleared of all connecting rami and theTi ganglion segment excised. Figure 6shows the thermoregulatory sweating pat-terns of the upper extremities and the para-sternal region of the upper chest six weeksafter re-operation on the right. The anhy-drosis on the right is strikingly contrastedwith the nearly normal reflex sweating onthe left. Subsequent re-operation on theleft, May 8, 1953, produced the same effectand also eliminated the residual area ofparasternal sweating on the right seen atthe level of the third rib. The effect hasremained permanent. Figure 7 is a photo-graph of this patient in December, 1954.Under thermal stress the irregular line ofanhydrosis and lack of vasodilatation iseasily visible just above the nipples. Thishas been a constant finding in patients afterdenervation of TI or after stellate ganglion-ectomy and represents a valid and pathog-
Volume 145Number 4
COLDWATER, ALEXANDER, COX AND RANDALL Annals of SurgeryApril 1957
FIG. 7. Unretouched photograph of patient C. S. whose reflex sweating pattems wereshown in Figure 6. Thermal stress was repeated 22 months after bilateral 1st thoracic ganglion-ectomy. Anhydrosis and vasomotor paralysis are seen in an irregular line above the nipples.This cutaneous area is innervated by the supraclavicular nerves. Intense reflex sweating andvasodilatation are visible below this line. This sign is uniformly present after complete sympa-thetic denervation of the upper extremity. It has not been observed after T2-T3 sympathectomy.
nomonic sign of total denervation of theupper extremity. Section of T2 and T3 in-tercostal nerves does not produce thisphenomenon.Temporary relief of causalgia or dys-
trophic painful states by incomplete sym-pathectomies have been frequently noted.The following case report is of interest inthe light of the anatomical informationgained from the stimulation studies in thisreport. R. T. (V. A. #6926) sustained a
shell fragment laceration of the right me-
dian and ulnar nerves at the wrist in 1944.A severe causalgia followed. Neurorrhaphyor neurolysis was performed on six occa-
sions after the injury. These local opera-
tions gave transient relief of burning pain,hyperesthesia and hyperhydrosis. Stellateblock gave relief. A dorsal preganglionicsympathectomy was performed in June,1953. Postoperative roentgen x-ray studiesshowed that the operator had removed sec-
tions of the third and fourth ribs and thatthe third and fourth intercostal nerves hadbeen decentralized and the trunk dividedbelow the T4 ganglion. This procedure
gave complete relief of all symptoms andthe arm and hand remained anhydroticfor five months. Both signs and symptomsgradually returned. He was admitted tothe VA hospital, St. Louis, Missouri, on
April 5, 1954. Stellate block again gaverelief and a stellate ganglionectomy withremoval of the T2 and T3 ganglia and theintermediate ganglion was performed on
April 21, 1954. He has been completelyrelieved to date.
DISCUSSION
The recurrence of sweating or positivevasomotor activity on the upper extremityfollowing the conventional T2-T3 pregan-glionic sympathectomy, has been frequentlyattributed to regeneration of preganglionicconnections with ganglion cells left intactin the Ti ganglion. Also, failure of thistype of operation to relieve the symptomsof Raynaud's phenomena has been ex-
plained by the concept of denervation hy-persensitivity. The latter possibility hasbeen cited as a major objection to the gan-glionic type sympathectomy. The evidence
536
THORACIC GANGLION IN SYMPATHECTOMY
refuting these concepts has been reviewedby Ray.'5 Further data adding to this evi-dence has been reported by Cooper, Will-man and Hertzman.5 In light of the resultsof direct stimulation of the sympathetictrunk in man reported here, it is our con-viction that neither regeneration or dener-vation sensitivity is the cause of failure.We believe that incomplete denervationaccounts for the residue of functional re-sponse and therapeutic failure. A case ispresented in which an admittedly inade-quate operation (third and fourth dorsalpreganglionic sympathectomy) has pro-duced complete remission of causalgia withvasomotor and sudomotor paralysis for aperiod of five months. Recurrence of painand resumption of sympathetic activityhave been permanently suppressed by totalganglionectomy of the upper extremity.We are fully in accord with the conclu-
sion of Ray 15 that the first thoracic con-
nections should be severed and that thesimplest approach to such denervationsis the stellate ganglionectomy which maybe easily extended caudalward to includethe second and third thoracic ganglia andcraniad to include the intermediate cervicalganglion. This extension into the chestmakes it possible to disconnect the nerve
of Kuntz and other accessory pathwayswhich have been demonstrated by stim-ulation studies to carry fibers of functionalimportance to the upper extremity. Addi-tional evidence for this has recently beenput forth by Palumbo,'3 Bridges and Yahr,3and by Hoffman.8Although all but one of these 13 pro-
cedures have been done through Smith-wick's dorsal approach extended to includethe second and third proximal ribs andtransverse processes, this approach is diffi-cult and its morbidity is high. A significantnumber of patients have not developed a
permanent Homer's syndrome (Palumbo 13 )when the inferior cervical ganglionic com-
ponent of the stellate is spared. The cilio-spinal reflex has returned in a few weeks.
We have used the peraxillary approach ofAtkins 1 in one of this series (Fig. 5) andseveral subsequent patients. Excellent ex-
posure is obtained and the operation grad-uates from the "keyhole" type. Morbidityis significantly reduced when comparedwith the dorsal approach. This operationresecting ganglia Ti or the inferior portionof the stellate, T2, T3, and the nerve ofKuntz has given us remission of Raynaud'sdisease of 2 to 3 years duration with no
evidence of sudomotor or vasospastic ac-
tivity. Stellate ganglionectomy with resec-tion of the intermediate cervical, T2, andT3 ganglia has been adopted for post-trau-matic painful states. We believe that theassurance of total afferent and efferentdenervation to the upper extremity andprompt and more nearly certain rehabilita-tion of the patient is more important thanthe minor disability of the inevitable Hor-ner's syndrome.
Direct stimulation of one of the upperintercostal nerves should give evidence ofsudomotor activity throughout the area of-its cutaneous distribution if it carries fibersof this nature. We have not found this tobe true. It is only after the removal of theTi ganglion or the caudal portion of thestellate ganglion that we have found anhy-drosis to be apparent on the upper chestwall. This gives conclusive evidence thatefferent sudomotor fibers to the upper chestwall traverse the supraclavicular nerves.
Complete denervation of the upper extrem-ity must be associated with anhydrosis ofthe upper chest. If this sign is not presentafter sympathectomy and signs and symp-toms have recurred, a re-operation withmore radical gainglionectomy is warranted.T2 and T3 denervation do not affect sweat-ing on the chest.
SUMMARY
1. Stimulation of the sympathetic trunkin man indicates that in addition to thefibers from T2 and T3, Ti contributes sig-nificantly to the innervation of the sweat
Volume 145Number 4 537
538 COLDWATER, ALEXANDER, COX AND RANDALL Annals of Surgery
glands of the upper extremity in the major-ity of patients.
2. The entrance of preganglionic sudo-motor fibers for the upper extremity belowthe level of T4 is rare.
3. The absence of strict segmental rela-tionship between sweating patterns on theupper extremity and chest wall during di-rect electrical stimulation of the thoracicsympathetic trunk and the thoracic spinalnerves shows that the supraclavicularnerves rather than the intercostal nervesare the peripheral pathway for sudomotorfibers to the upper chest.
4. Anhydrosis of the upper chest is aclinical sign of complete sympathetic dener-vation of the upper extremity, and occursonly after resection of the Ti ganglion orthe caudal portion of the stellate ganglion.Persistent sweating of this region is indica-tive of incomplete sympathectomy.
5. Our studies show that incompletesympathectomy may produce extendedtemporary paralysis of the pathologicalsensory effects and the sympathetic inner-vation. Return of sweating is not due toregeneration and hypersensitivity.
6. The peraxillary approach for upperextremity sympathectomy is our choice invasospastic disorders of the arm and hand.Preservation of the inferior cervical gan-glion (stellate) may spare the patient thedisfigurement of the Horner's syndrome.
7. Stellate ganglionectomy with removalof the intermediate cervical and T2 and T3ganglia is our choice of operation in post-traumatic painful states and where vaso-spastic disorder is associated with thescalenus syndrome.
BIBLIOGRAPHY
1. Atkins, H. J. B.: Peraxillary Approach to theStellate and Upper Thoracic SympatheticGanglia. Lancet, 2: 1152, 1949.
2. Atlas, L. N.: The Role of the Second ThoracicSpinal Segment in the Preganglionic Sym-pathetic Innervation of the Human Hand-
Surgical Implications. Surgery, 114: 456,1941.
3. Bridges, T. J. and M. D. Yahr: Digital Vaso-motor Responses Following Nerve RootStimulation. Arch. Neurol. and Psychiat.,74: 534, 1955.
4. Coldwater, K. B., J. W. Cox, W. C. Randall,W. F. Alexander and A. B. Hertzman:Sweating Patterns and Vascular Responsesin the Lower Extremity of Man Elicited byStimulation of the Sympathetic Trunk. Sur-gical Forum, American College of Surgeons.Philadelphia and London, W. B. Saunders& Co., pp. 716 (see pp. 486-492), 1953.
5. Cooper, T., V. L. Willman and A. B. Hertz-man: Vascular Reactivity to EpinephrineFollowing Sympathectomy. Fed. Proc., 15:40, 1956.
6. Gask, G. E. and J. P. Ross: Surgery of theSympathetic Nervous System. Philadelphia,William Wood & Co., 2nd Ed., 1937.
7. Goetz, R. H. and J. A. S. Marr: The Impor-tance of the Second Thoracic Ganglion forSympathetic Supply of the Upper Extremitywith a Description of Two New Approachesfor its Removal in Cases of Vascular Disease.Clin. Proc., 3: 102, 1944.
8. Hoffman, H. H.: An Analysis of the Sympa-thetic Trunk and Rami in the Cervical andUpper Thoracic Region in Man. (Acceptedfor Publication in Annals of Surgery.)
9. Hyndman,-O. R. and J. Wolkin: Sympathec-tomy of the Upper Extremity. Evidence ThatOnly the Second Dorsal Ganglion Need beRemoved for Complete Sympathectomy.Arch. Surg., 45: 145, 1942.
10. Kuntz, A., W. F. Alexander and C. L. Fur-colo: Complete Sympathetic Denervation ofthe Upper Extremity. Ann. Surg., 107: 25,1938.
11. Kuntz, A. and J. B. Dillon: PreganglionicComponents of the First Thoracic Nerve.Arch. Surg., 44: 772, 1942.
12. Netsky, M. G.: Studies on Sweat Secretion inMan. 1. Innervation of the Sweat Glands ofthe Upper Extremity; Newer Methods ofStudying Sweating. Arch. Neurol. and Psy-chiat., 60: 279, 1948.
13. Palumbo, L. T.: Anterior Transthoracic Ap-proach for Upper Thoracic Sympathectomy.Arch. Surg., 72: 659, 1956.
14. Randall, W. C., J. W. Cox, W. F. Alexanderand K. B. Coldwater: Direct Stimulation ofthe Sympathetic Outflows in Man. J. Ap-plied Physiology, 7: 688, 1953.
Volume 145 THORACIC GANGLION IN SYMPATHECTOMY 539Number 4
15. Ray, B. S.: Sympathectomy of the Upper Ex-tremity; Evaluation of Surgical Methods. J.Neurosurg., 10: 624, 1953.
16. Smithwick, R. H.: Modified Dorsal Sympathec-tomy for Vascular Spasm (Raynaud's Dis-
ease) of the Upper Extremity; A preliminaryreport. Ann. Surg., 104: 339, 1936.
17. White, J. C. and R. H. Smithwick: The Auto-nomic Nervous System. New York, The Mac-millan Co., 2nd Ed., 1941.
()p