Embed Size (px)
Citation preview
inthe
clinicin the clinic
Atrial FibrillationDiagnosis page ITC5-2
Treatment page ITC5-6
Practice Improvement page ITC5-14
CME Questions page ITC5-16
Section EditorsChristine Laine, MD, MPHDavid Goldmann, MD
Physician WriterDavid J. Callans, MD
The content of In the Clinic is drawn from the clinical information and education resources of the American College of Physicians (ACP), includingPIER (Physicians’ Information and Education Resource) and MKSAP (MedicalKnowledge and Self-Assessment Program). Annals of Internal Medicineeditors develop In the Clinic from these primary sources in collaboration withthe ACP’s Medical Education and Publishing Division and with the assistance of science writers and physician writers. Editorial consultants from PIER andMKSAP provide expert review of the content. Readers who are interested in these primary resources for more detail can consult http://pier.acponline.org and otherresources referenced in each issue of In the Clinic.
The information contained herein should never be used as a substitute for clinicaljudgment.
© 2008 American College of Physicians
®

Who is at risk for atrialfibrillation?Atrial fibrillation occurs in less than1% of individuals age 60 to 65years, but in 8% to 10% of thoseolder than 80 years. Prevalence ishigher in men than in women andhigher in whites than in blacks. Therisk for atrial fibrillation increaseswith the presence and severity ofunderlying heart failure and valvu-lar disease.
What symptoms and signs shouldcause clinicians to suspect atrialfibrillation?Many patients, particularly the eld-erly, are asymptomatic during atrialfibrillation. Other patients mayhave prominent symptoms, includ-ing palpitations, shortness ofbreath, exercise intolerance, ormalaise. When present, symptomsare generally greatest at diseaseonset, when episodes are typicallyparoxysmal, and tend to diminishover time or when the patternbecomes persistent. Symptoms dur-ing atrial fibrillation result fromelevation of ventricular rate (at restand exaggerated with exercise), theirregular nature of the ventricularrate, and the loss of atrial contribu-tion to cardiac output. Even patientswith severe symptoms during atrialfibrillation episodes often haveepisodes of silent atrial fibrillation aswell (4), which has important impli-cations for therapeutic strategies,especially anticoagulation.
On physical examination, the signs of atrial fibrillation include a
faster-than-expected heart rate(which is quite variable frompatient to patient), an irregularly(irregular in timing) irregular (interms of the amplitude of the pulse)peripheral pulse, as well as irregularheart sounds on auscultation.
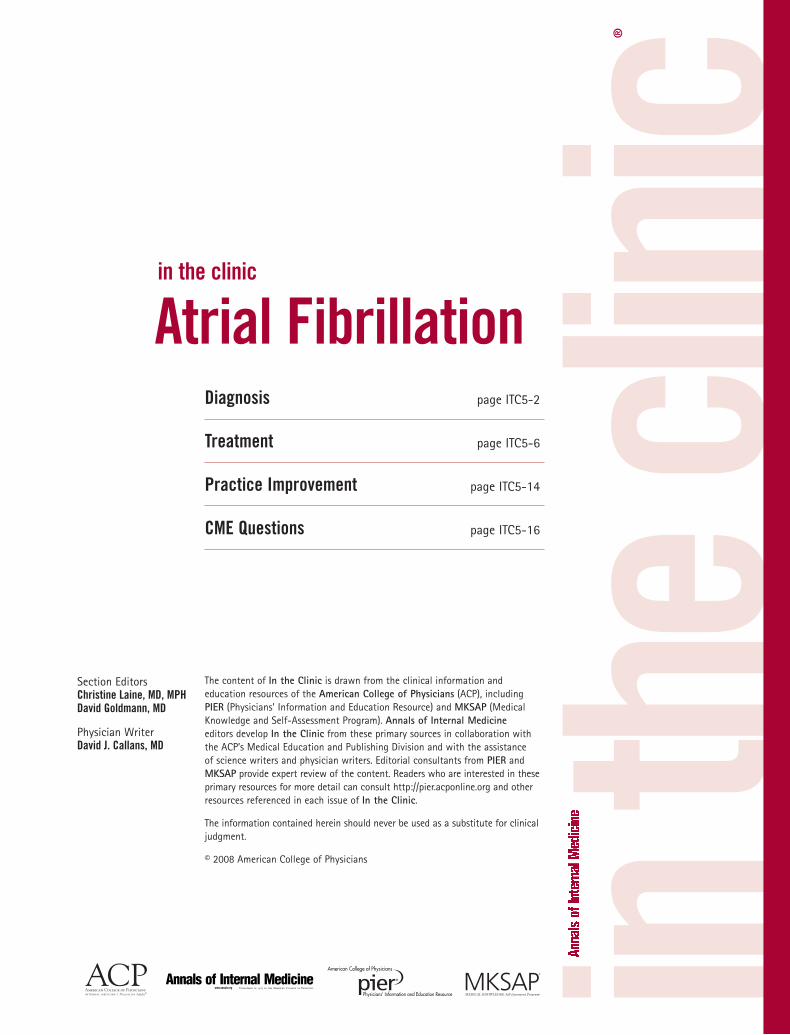
Is a single electrocardiogram(ECG) sufficient to diagnose orexclude atrial fibrillation?Figure 1 is an example of an ECGshowing atrial fibrillation. A singleECG is sufficient to diagnose atrialfibrillation if it is recorded duringan arrhythmia episode. However,atrial fibrillation is often paroxys-mal, so a single ECG showing nor-mal rhythm does not exclude thediagnosis. Longer-term monitoringcan be helpful when atrial fibrilla-tion is suspected but the ECG isnormal. In patients with dailyparoxysmal symptoms, 24- or 48-hour continuous Holter monitoringis usually sufficient to make thediagnosis. In patients with less-frequent symptoms, monitoringduring longer periods with electro-cardiographic loop recorders may be necessary for diagnosis. How-ever, even monitoring for periods aslong as a month can be nondiagnos-tic in patients with very infrequentepisodes. In addition, becausepatients trigger loop recorders torecord when symptoms occur, theserecorders are not helpful in detectingepisodes of asymptomatic arrhyth-mia. In some cases, a diagnosis ofatrial fibrillation occurs only afterseveral years of symptoms because ofthe nonspecific nature of symptoms
© 2008 American College of Physicians ITC5-2 In the Clinic Annals of Internal Medicine 4 November 2008
Atrial fibrillation, the most common clinically significant arrhythmia,occurs when a diffuse and chaotic pattern of electrical activity in theatria replaces the normal sinus mechanism, leading to deterioration of
mechanical function. Atrial fibrillation is a major cause of morbidity, mortal-ity, and health care expenditures, with a current prevalence of 2.3 millioncases in the United States and an estimated increase in prevalence to 15.9million by the year 2050 (1). Atrial fibrillation is associated with a 5-foldincreased risk for stroke and is estimated to cause 15% of all strokes (2).Independent of coexisting diseases, the presence of atrial fibrillation confers a2-fold increased risk for all-cause mortality (3).
Diagnosis
1. Miyasaka Y, BarnesME, Gersh BJ, et al.Secular trends in inci-dence of atrial fibrilla-tion in OlmstedCounty, Minnesota,1980 to 2000, andimplications on theprojections for futureprevalence. Circula-tion. 2006;114:119-25.[PMID: 16818816]
2. Hart RG, Benavente O,McBride R, Pearce LA.Antithrombotic ther-apy to prevent strokein patients with atrialfibrillation: a meta-analysis. Ann InternMed. 1999;131:492-501.[PMID: 10507957]
3. Benjamin EJ, Wolf PA,D’Agostino RB, et al.Impact of atrial fibril-lation on the risk ofdeath: the Framing-ham Heart Study. Cir-culation. 1998;98:946-52. [PMID: 9737513]
4. Page RL, WilkinsonWE, Clair WK, et al.Asymptomaticarrhythmias inpatients with symp-tomatic paroxysmalatrial fibrillation andparoxysmalsupraventriculartachycardia. Circula-tion. 1994;89:224-7.[PMID: 8281651]
© 2008 American College of PhysiciansITC5-3In the ClinicAnnals of Internal Medicine4 November 2008
and the occasionally long periodsbetween episodes in some patientsat the beginning of the diseaseprocess.
What is the role of history andphysical examination in patientswith atrial fibrillation?History and physical examinationcan help to determine the dura-tion of symptoms and potentialunderlying causes. Clinicians
should document history andphysical examination evidence ofhypertension, heart failure, mur-murs indicating structural heartdisease, or recent cardiac surgery.In addition, clinicians should lookfor signs and symptoms of non-cardiac causes of atrial fibrillation,including pulmonary disease;hyperthyroidism; use of caffeine or other stimulants; or use ofadrenergic drugs (such as those
Figure 1. Electrocardiogram showing atrial fibrillation with rapid ventricular rate.
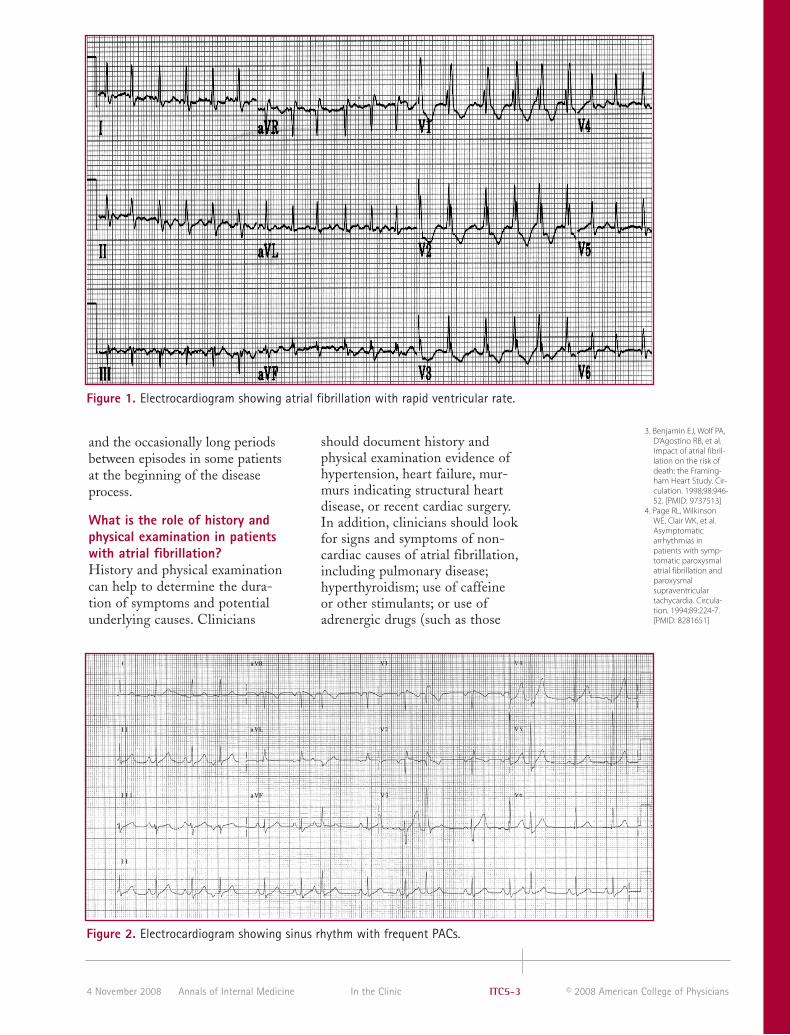
Figure 2. Electrocardiogram showing sinus rhythm with frequent PACs.

5. American College ofCardiology/AmericanHeart Association TaskForce on PracticeGuidelines.ACC/AHA/ESC 2006Guidelines for theManagement ofPatients with Atrial Fib-rillation: a report of theAmerican College ofCardiology/American Heart Asso-ciation Task Force onPractice Guidelinesand the EuropeanSociety of CardiologyCommittee for PracticeGuidelines (WritingCommittee to Revisethe 2001 Guidelinesfor the Managementof Patients With AtrialFibrillation): developedin collaboration withthe European HeartRhythm Associationand the Heart RhythmSociety. Circulation.2006;114:e257-354.[PMID: 16908781]
© 2008 American College of Physicians ITC5-4 In the Clinic Annals of Internal Medicine 4 November 2008
used to treat pulmonary disease) or alcohol.
What other electrocardiographicarrhythmias might cliniciansconfuse with atrial fibrillation?Other arrhythmias that are commonly confused with atrialfibrillation include sinus rhythmwith frequent premature atrial con-tractions (PACs), atrial tachycardia,and atrial flutter. The key electrocar-diographic components of atrial fib-rillation are the absence of discern-able P waves and an irregularventricular response without any pat-tern. When the diagnosis of atrialfibrillation is unclear, cliniciansshould obtain long rhythm stripswith multiple lead combinations toevaluate for irregular rhythms and P waves. Clinicians should look fordeformed T waves or ST segmentsfor evidence of P waves.
Sinus rhythm with frequent PACsis an irregular rhythm, but P wavesare present (Figure 2). Atrial tachy-cardia and atrial flutter have evi-dent atrial activation, but may beconducted to the ventricles in anirregular matter; even in this cir-cumstance, there is a pattern to the
irregular conduction (Figure 3).This is an important distinctionbecause catheter ablation is first-line therapy in many patients withatrial tachycardia and atrial flutter.
How should clinicians classifyatrial fibrillation according toduration and frequency?Although there is a great deal ofconfusion regarding this question,the convention is to describe atrialfibrillation by the qualifiers parox-ysmal, persistent, or permanent (5).“Paroxysmal” means that atrial fib-rillation episodes terminate withoutintervention within 7 days butoften in less than 24 hours. “Persis-tent” means that episodes lastlonger than 7 days or require inter-vention (such as cardioversion) torestore sinus rhythm. “Permanent”means that interventions to restoresinus rhythm have either failed orhave not been attempted. Thesequalifiers are not necessarily mutu-ally exclusive in a given patient, soclinicians should characterize thecurrent or most-usual pattern.
Traditionally, these distinctionshave been used to predict response to therapy. The response
Figure 3. Atrial flutter. Classic “saw-tooth” flutter waves are seen in all 12 leads, and the ventricularresponse is mostly regular. (There is a transient change from 2:1 to 4:1 atrioventricular conduction follow-ing the 12th QRS complex.)
Classification of AtrialFibrillationParoxysmal: Episodes
spontaneously terminatewithin 7 days
Persistent: Episodes last>7 days and requireintervention to restoresinus rhythm
Permanent: Interventionsto restore sinus rhythmhave either failed orhave not beenattempted

© 2008 American College of PhysiciansITC5-5In the ClinicAnnals of Internal Medicine4 November 2008
6. Brand FN, Abbott RD,Kannel WB, Wolf PA.Characteristics andprognosis of loneatrial fibrillation. 30-year follow-up in theFramingham Study.JAMA. 1985;254:3449-53. [PMID: 4068186]
7. Furberg CD, Psaty BM,Manolio TA, et al.Prevalence of atrialfibrillation in elderlysubjects (the Cardio-vascular HealthStudy). Am J Cardiol.1994;74:236-41.[PMID: 8037127]
to antiarrhythmic drug therapy isless favorable as the pattern goesfrom paroxysmal to persistent topermanent. There is no differencein the need for anticoagulation onthe basis of the pattern of atrialfibrillation.
What underlying cardiac andnoncardiac conditions shouldclinicians look for in patients with atrial fibrillation?Of patients with atrial fibrillation,80% have some component ofstructural heart disease, particularlyhypertensive heart disease, but alsocoronary disease, valvular heart dis-ease, or cardiomyopathies of anycause. Because the incidence ofatrial fibrillation is markedlyaffected by aging, age-related atrial
fibrosis is considered central to thearrhythmia’s pathogenesis. Somepatients have atrial fibrillation inthe absence of identifiable heartdisease, which is referred to as loneatrial fibrillation, but the usefulnessof this designation is a matter ofsome debate. Some experts believethat the designation “lone atrial
because it is difficult to excludestructural heart disease in olderpatients.
In 30 years of follow-up of 5209 partici-pants in the Framingham Study, 193 menand 183 women developed atrial fibrilla-tion. Of these, 32 men and 11 women hadno evidence of underlying heart disease.Matched comparisons between patientswith lone atrial fibrillation and control par-ticipants showed that individuals withatrial fibrillation had similar cardiac risk fac-tors but significantly higher rates of pre-existing nonspecific T- or ST-wave abnormal-ities, intraventricular block, and stroke (6).
In a population-based, longitudinal studyof risk factors for coronary artery diseaseand stroke in 5201 men and women age≥65 years, 4.8% of women and 6.2% ofmen had atrial fibrillation at baseline.Prevalence was 9.1% in patients with clini-cal cardiovascular disease, 4.6% in patientswith evidence of subclinical but no clinicalcardiovascular disease, and only 1.6% inpatients with neither clinical nor subclini-cal cardiovascular disease. The low preva-lence of atrial fibrillation in the absence of clinical and subclinical cardiovasculardisease calls into question the clinical use-fulness of the designation “lone atrial fibrillation,” particularly in the elderly (7).
Acute illnesses that may be associ-ated with new-onset atrial fibrilla-tion include acute myocardialinfarction, pulmonary embolism,and thyrotoxicosis. Atrial fibrilla-tion is common after cardiac orthoracic surgery, but may also occurin reaction to another major sur-gery or severe illness. Atrial fibrilla-tion has an increased incidence insleep apnea and obesity; however,treatment of these conditions doesnot seem to affect the subsequentprogression of arrhythmia.
fibrillation” should be restricted topatients younger than 60 years of age
What laboratory studies shouldclinicians obtain in patients withatrial fibrillation?On initial presentation of atrial fib-rillation, clinicians should measuresensitive thyroid-stimulating hor-mone to exclude hyperthyroidism,serum electrolytes, and renal andhepatic function to evaluate risk fortoxicity to specific drugs. Trans-thoracic echocardiogram is generally helpful to evaluate the presence of structural heart disease, but is specifically able to evaluate left atrial size, valvular heart disease, pericardial disease, and left ventric-ular hypertrophy, which are associated with responsiveness to antiarrhythmic therapy. Trans-esophageal echocardiogram is indicated to exclude atrial clot when transthoracic images are inadequate or when cardioversion is planned in a patient who has been anticoag-ulated for less than 3 weeks. In selected patients, tests to evaluate specific disease processes that may be causative in acute episodes of atrial fibrillation, such as pulmonary embolism, acute myocardial infarc-tion, or acute heart failure, may also be appropriate. Clinicians should test stool for occult blood before initiation of anticoagulation.

© 2008 American College of Physicians ITC5-6 In the Clinic Annals of Internal Medicine 4 November 2008
8. Naito M, David D,Michelson EL, et al.The hemodynamicconsequences of car-diac arrhythmias:evaluation of the rel-ative roles of abnor-mal atrioventricularsequencing, irregular-ity of ventricularrhythm and atrial fib-rillation in a caninemodel. Am Heart J.1983;106:284-91.[PMID: 6869209]
9. Risk factors for strokeand efficacy ofantithrombotic ther-apy in atrial fibrilla-tion. Analysis ofpooled data from fiverandomized con-trolled trials. ArchIntern Med.1994;154:1449-57.[PMID: 8018000]
10. Hart RG, ShermanDG, Easton JD,Cairns JA. Preventionof stroke in patientswith nonvalvularatrial fibrillation.Neurology.1998;51:674-81.[PMID: 9748009]
11. Redfield MM, KayGN, Jenkins LS, et al.Tachycardia-relatedcardiomyopathy: acommon cause ofventricular dysfunc-tion in patients withatrial fibrillationreferred for atrioven-tricular ablation.Mayo Clin Proc.2000;75:790-5.[PMID: 10943231]
12. Atrial Fibrillation Fol-low-up Investigationof Rhythm Manage-ment (AFFIRM)Investigators. A com-parison of rate con-trol and rhythm con-trol in patients withatrial fibrillation. NEngl J Med.2002;347:1825-33.[PMID: 12466506]
Treatment
Diagnosis... Atrial fibrillation is the most common clinically significant arrhythmia,and prevalence increases with advancing age. Typical symptoms include palpita-tions, shortness of breath, and exercise intolerance. However, some patients
What are the complications ofatrial fibrillation and how cantherapy decrease the risk forthese events?There are 3 reasons to prescribetherapy for atrial fibrillation: toreduce symptoms, to preventthromboembolism, and to reducethe risk for tachycardia-relatedmyocardiopathy.
Although atrial fibrillation is notalways symptomatic, when presentit can be disabling for somepatients. Symptoms are usuallycaused by inappropriately rapidventricular rates or the irregularityof the ventricular response duringatrial fibrillation (8). Rhythm con-trol (restoring and maintainingsinus rhythm) and rate control(controlling heart rate responsewithout attempts to restore andmaintain sinus rhythm) can bothhelp to reduce symptoms.
The average annual risk for arterialthromboembolism is 5% in patientswith nonvalvular atrial fibrillation,and the risk for stroke is higher in
patients older than age 75 (9). Bothestablished risk factors for throm-boembolism and specific features ofatrial fibrillation modulate strokerisk (6). Left-atrial thrombi cause75% of strokes in patients withatrial fibrillation (10). Antithrom-botic therapy reduces stroke risk.
The other pathologic consequence ofatrial fibrillation is tachycardia-related cardiomyopathy (11). Drugtherapy to control rate or rhythm canreduce the risk for this complication.
What are the relative benefits ofrate control versus rhythm controlin patients with atrial fibrillation?High-quality clinical trials suggestthat rhythm control does notimprove mortality, stroke rates,hospitalization rates, or quality oflife compared with rate control formost patients with atrial fibrillation(12–14). Rate control is easier toaccomplish and prevents exposureto potentially harmful antiarrhyth-mic agents. On the other hand,rhythm control may be useful inselected patients with severe atrial
exercise. The mechanism of alco-hol-precipitated atrial fibrillationis unclear, but may be related toincreases in circulating catechola-mines, changes in conduction timeand refractory periods in themyocardium, and increases invagal tone.
Vagal forms of atrial fibrillationusually occur in men age 40 to 50years who have no structural heartdisease. Symptoms often occur atnight, at rest, or after alcohol use.Adrenergic forms of atrial fibrilla-tion occur during waking hourspreceded by emotional stress or
report only general malaise, and many patients are asymptomatic. Electrocardio-gram recordings during episodes are the only way to confirm the diagnosis. If thediagnosis is suspected and ECG is normal, longer-term monitoring with a Holtermonitor or loop recorder can be helpful. Initial assessment should include labora-tory tests (electrolytes, thyroid-stimulating hormone, and renal and hepatic func-tion) to rule out underlying disorders or contraindications to therapies, and
CLINICAL BOTTOM LINE
echocardiogram to look for structural heart disease.

fibrillation symptoms (before orafter failure of rate control) or inyounger patients without structuralheart disease.
The AFFIRM (Atrial Fibrillation Follow-upInvestigation of Rhythm Management)trial included 4060 patients with atrial fib-rillation who had at least 1 risk factor forstroke. The mean age was 69 years, andstructural heart disease, aside from hyper-tension, was unusual. All-cause mortalityat 5 years was 25.9% in the rate-controlgroup and 26.7% in the rhythm-controlgroup (P = 0.080). Important observationsfrom the trial are that patients with appar-ently successful rhythm control still need tocontinue anticoagulation because of per-sistent stroke risk, and that patients whowere able to maintain sinus rhythm had asurvival advantage that was almost bal-anced by the disadvantage imposed byantiarrhythmic drug therapy (15).
A more recent trial extended these observa-tions to outpatients with severe heart failureby randomly assigning 1376 patients withatrial fibrillation, left ventricular ejectionfraction of ≤35%, and heart failure symp-toms to rate control versus rhythm control.Over 37 months, 27% of the rhythm-control group and 25% of the rate-controlgroup died from cardiovascular causes (P = 0.6). There was no improvement in all-cause mortality, stroke, heart failure, orneed for hospitalization in the rhythm-control group (16).
What drugs should cliniciansconsider for rate control inpatients with rapid atrialfibrillation?Clinicians should consider drugtherapy to control ventricular ratein all patients with atrial fibrilla-tion. Criteria for rate control varywith patient age, but cliniciansshould generally target therapy toachieve target heart rates of 60 to 80beats per minute at rest and between90 to 115 beats per minute duringmoderate exercise (17). Agents thataffect atrioventricular nodal conduc-tion and are recommended as first-line therapy in this setting includeβ-blockers and nondihydropyridinecalcium-channel antagonists (Table1). Amiodarone and digoxin alsoblock the atrioventricular node, butare not recommended as first-line
© 2008 American College of PhysiciansITC5-7In the ClinicAnnals of Internal Medicine4 November 2008
13. STAF Investigators.Randomized trial ofrate-control versusrhythm-control inpersistent atrial fibril-lation: the Strategiesof Treatment ofAtrial Fibrillation(STAF) study. J AmColl Cardiol.2003;41:1690-6.[PMID: 12767648]
14. Hohnloser SH, KuckKH, Lilienthal J.Rhythm or rate con-trol in atrial fibrilla-tion—-Pharmaco-logical Interventionin Atrial Fibrillation(PIAF): a randomisedtrial. Lancet.2000;356:1789-94.[PMID: 11117910]
15. AFFIRM Investiga-tors. Relationshipsbetween sinusrhythm, treatment,and survival in theAtrial Fibrillation Fol-low-Up Investigationof Rhythm Manage-ment (AFFIRM)Study. Circulation.2004;109:1509-13.[PMID: 15007003]
16. Atrial Fibrillation andCongestive HeartFailure Investigators.Rhythm control ver-sus rate control foratrial fibrillation andheart failure. N EnglJ Med.2008;358:2667-77.[PMID: 18565859]
17. American College ofCardiology/Ameri-can Heart Associa-tion Task Force onPractice Guidelines.ACC/AHA/ESC 2006Guidelines for theManagement ofPatients with AtrialFibrillation. Circula-tion. 2006;114:e257-354.[PMID: 16908781]
18. Roy D, Talajic M,Dorian P, et al. Amio-darone to preventrecurrence of atrialfibrillation. CanadianTrial of Atrial Fibrilla-tion Investigators. NEngl J Med.2000;342:913-20.[PMID: 10738049]
monotherapy for rate control (17).Digitalis is not helpful in reducingheart rate with exercise. Addition-ally, monotherapy with digitalis isunlikely to control rate in patientswith heart failure and high sympa-thetic activity.
Amiodarone is occasionally used toreduce ventricular response duringcontinued atrial fibrillation if otheragents have failed. This practice ismore difficult to justify because oftoxicities associated with amio-darone and the trial evidence thatrhythm control is no better thanrate control.
When should clinicians considerantiarrhythmic drugs in thetreatment of atrial fibrillation?Rhythm-control therapy is nolonger the preferred strategy inmost patients with atrial fibrilla-tion. However, the major trialscomparing rate control withrhythm control did not includeyounger patients or patients withhighly symptomatic atrial fibrilla-tion. Consequently, it is reasonableto consider rhythm control in thesepatient subgroups, either primarilyor when symptoms persist despiterate control. Rhythm control isoften favored for the first episode ofsymptomatic atrial fibrillation, par-ticularly in young patients becausemany maintain sinus rhythm for aperiod after pharmacologic car-dioversion without continued anti-arrhythmic drug treatment. Anti-arrhythmic drugs have been shownto have modest effects comparedwith placebo in prolonging time torecurrent atrial fibrillation (Table 1),but rather than the complete ab-sence of atrial fibrillation episodes,antiarrhythmic drug therapy is gen-erally judged to be effective if itreduces episodes and symptoms.
The Canadian Trial of Atrial Fibrillationrandomly assigned 403 patients to amio-darone, sotalol, or propafenone and foundthat after mean follow-up of 16 months,recurrence of atrial fibrillation was 35%during amiodarone and 63% duringsotalol or propafenone therapy (18).

© 2008 American College of Physicians ITC5-8 In the Clinic Annals of Internal Medicine 4 November 2008
Table 1. Drug Therapy for Rate and Rhythm Control in Atrial FibrillationAgent Mechanism of Action Dosage Benefits Side Effects Notes
Rate-Controlling Agentsß-BlockersMetoprolol Selective ß
1-adrenergic– 5 mg IV every 5 min, Convenient IV Bradycardia, hypotension,
receptor blocking agent up to 15 mg 50–100 administration in NPO heart block, mg PO twice daily patients, rapid onset of bronchospasm (less
action, dependable AV frequently than nonselectivenodal blockade ß-blockers), worsening of CHF
Propranolol Nonselective ß-adrenergic– 1–8 mg IV (1 mg every Inexpensive, commonly Bradycardia, hypotension,receptor blocking agent 2 min). 10–120 mg PO available heart block, bronchospasm,
3 times daily; long- worsening of CHFacting preparation: 80–320 mg PO once daily
Esmolol Short-acting IV ß1
0.05–0.2 mg/kg per Short-acting, titratable Bradycardia, hypotension, Occasionally selective adrenergic min IV on or off with very rapid heart block, bronchospasm inconsistent effect inreceptor-blocking agent half-life (less frequent) high-catecholamine
statesPindolol Nonselective ß-adrenergic– 2.5–20 mg PO 2 to 3 Less bradycardia, less Bradycardia, hypotension, Less propensity for
receptor blocking agent times daily bronchospasm heart block heart block than with intrinsic sympatho- other ß-blockersmimetic activity
Atenolol Selective ß1-adrenergic– 5 mg IV over 5 min, Does not cross blood– Bradycardia, hypotension,
receptor blocking agent repeat in 10 min. brain barrier, fewer heart block25–100 mg PO once CNS side effectsdaily
Nadolol Nonselective ß-adrenergic– 20–120 mg once daily Lower incidence of Bradycardia, hypotension, Oral form onlyreceptor blocking agent crossing of blood–brain heart block
barrier, fewer CNS side effects
Calcium-channel blockersVerapamil Calcium-channel blocking 5–20 mg in 5-mg Consistent AV nodal Hypotension, heart block, Do not use in the
agent increments IV every blockade direct myocardial depression Wolff–Parkinson–30 min, or 0.005 mg/kg White syndromeper min infusion. 120–360 mg PO daily, in divided doses or in the slow-release form
Diltiazem Calcium-channel blocking 0.25–0.35 mg/kg IV Consistent AV nodal Hypotension, heart block, less Do not use in the agent followed by 5–15 mg/h. blockade myocardial depression Wolff–Parkinson–
120–360 mg PO daily White syndromeas slow release
Cardiac glycosideDigoxin Na+-K+ pump inhibitor, 0.75–1.5 mg PO or IV Particularly useful for Heart block, digoxin- First-line therapy
increases intracellular in 3–4 divided doses rate control in CHF. associated arrhythmias; only in patients with calcium over 12–24 h. dosage adjustment required decreased left-
Maintenance dose: in renal impairment ventricular systolic 0.125 mg PO or IV to function. Not useful0.5 mg daily for rate control with
exercise. Not usefulfor conversion of AF oraflutter to NSR.
Antiarrhythmic agentsClass IaProcainamide Prolongs conduction 1–2 g q 12 h (shorter- Convenient IV dosing Not recommended because Need to follow drug
and slows repolarization acting oral preparations available with of frequent side effects, levels and QT interval by blocking inward Na+ are no longer available) maintenance infusion, including hypotension, for toxicity, adjust flux and conversion to PO nausea, vomiting, dose in patients with
tablets, very effective lupus-like syndrome, QT renal insufficiency, at converting AF to prolongation, and Not for use in patients NSR arrhythmia with severe LV
dysfunction.Quinidine Prolongs conduction and 324–648 mg PO Relatively effective in Proarrhythmia, nausea, Not recommended gluconate slows repolarization. every 8–12 h converting AF to NSR vomiting, diarrhea, because of frequent
Blocks fast inward Na+ but may take several QT prolongation side effects. Follow channel. days to achieve NSR drug levels and QT
because of PO dosing interval for toxicity.Adjust dose in patientswith renal insuffi-ciency. Oral agent only

© 2008 American College of PhysiciansITC5-9In the ClinicAnnals of Internal Medicine4 November 2008
Table 1. Drug Therapy for Rate and Rhythm Control in Atrial Fibrillation (continued)Agent Mechanism of Action Dosage Benefits Side Effects Notes
Disopyramide Similar electrophysiologic 150 mg PO every Can be useful in QT prolongation (not PR Rarely used in current properties to procainamide 6–8 h, or 150–300 mg patients with or QRS), torsades de era of antiarrhythmic and quinidine twice a day hypertension and pointes, heart block therapy. Oral agent
normal LV function only, negativeinotropic properties.
Class IcFlecainide Blocks Na+ channels 2 mg/kg, IV*. 50–150 Efficacy in paroxysmal Aflutter or atrial tachycardia Not for use in
(and fast Na+ current) mg PO every 12 h. AF with structurally with rapid ventricular patients withAlso, single loading normal hearts response but not with acute structurally abnormal doses of 300 mg are single loading doses. VT heartsefficacious in and VF in diseased heartsconversion of recent onset AF.
Propafenone Blocks myocardial 2 mg/kg, IV*. 150–300 Efficacy in paroxysmal Aflutter or atrial tachycardia Antiarrhythmic and Na+ channels mg PO every 8 h. Also, and sustained AF with rapid ventricular response, weak calcium channel
single loading doses of but not with acute single and ß-blocking 600 mg are efficacious loading doses properties. Not for in conversion of recent use with structuralonset AF. heart disease.
C. Class IIIIbutilide Prolongs action potential 1 mg IV over 10 min. Efficacy in acute and Polymorphic VT (torsades de In some centers, only
duration (and atrial and May be repeated once rapid conversion of AF pointes) occurred in 8.3% used in the ventricular refractoriness) if necessary. to NSR of patients in a clinical trial electrophysiology by blocking rapid (most with LV dysfunction), laboratory. May also component of delayed QT prolongation be used to facilitate rectifier potassium current unsuccessful direct-
current cardioversion. Amiodarone Blocks Na+ channels 5–7 mg/kg IV up to Safest agent for use Bradycardia, QT prolongation, Can be used in the
(affinity for inactivated 1500 mg per 24 h. in patients with hyperthyroidism, lung toxicity, Wolff–Parkinson–channels). Noncompetitive 400–800 mg PO daily, structural heart disease, argyria (blue discoloration White syndrome. ß- and ß-receptor for 3–4 wk, followed good efficacy in of skin) with chronic useinhibitor. by 100–400 mg PO maintaining NSR
daily chronicallySotalol Nonselective ß
1- and 80–240 mg PO every Similar efficacy to Fatigue, depression, ß-blocking properties,
ß2-blocking agent, 12 h quinidine, but fewer bradycardia, torsades de but some positive
prolongs action adverse effects. Better pointes, CHF inotropic activity. potential duration rate control because of Lethal arrhythmias
ß-blocking properties. possible. Adjust dosein patients with renalinsufficiency. Initiateon telemetry.
Dofetilide Blocks rapid component 500 µg twice daily More effective than QT prolongation, torsades Must be strictly dosed of the delayed rectifier quinidine in conversion de pointes (2%–4% risk). according to renal potassium current (IK�), to and maintenance of function, body size, prolonging refractoriness NSR. and age. Contra-without slowing conduction indicated in patients
with creatinine clearance <20 mL/min. Initiate on telemetry.
AF = atrial fibrillation; AV = atrioventricular; CHF = congestive heart failure; CNS = central nervous system; IV = intraventricular; LV = left ventricular;NPO = nil per os; NSR = normal sinus rhythm; PO = orally; VF = ventricular fibrillation; VT = ventricular tachycardia.
disease because of an increase inmortality (19). In patients withoutheart disease, the side effects aredue to unwanted sodium-channelblockade in other organ systems,such as the gastrointestinal tract(resulting in anorexia or esophagealreflux) and the central nervous sys-tem. Other class I drugs, such asquinidine and procainamide, are nolonger used because of their fre-quent noncardiac side effects.
Antiarrhythmic drugs other thanamiodarone are generally have equal efficacy, so susceptibility toside effects should guide choicefrom among them (Table 1). Drugsthat block cardiac sodium channels(class I effect), such as flecainideand propafenone, are useful inpatients without coronary heart dis-ease or advanced left-ventriculardysfunction. Trial data do not sup-port their use in patients with heart
19. The Cardiac Arrhyth-mia SuppressionTrial (CAST) Investi-gators. Preliminaryreport: effect ofencainide and fle-cainide on mortalityin a randomized trialof arrhythmia sup-pression aftermyocardial infarc-tion. N Engl J Med.1989;321:406-12.[PMID: 2473403]

© 2008 American College of Physicians ITC5-10 In the Clinic Annals of Internal Medicine 4 November 2008
Drugs that block potassium chan-nels (class III effects), such assotalol and dofetilide, have a poten-tial to prolong the QT interval andcause torsades de pointes.
Amiodarone can be used inpatients with advanced structuralheart disease. However, amiodaronecan cause permanent end organtoxicity (liver, lungs) that is dose-and duration-dependent. Otherside effects include thyroid dys-function (hypothyroidism, hyper-thyroidism), sun sensitivity, andocular symptoms.
Some nonantiarrhythmic drugs,such as angiotensin-convertingenzyme inhibitors and statins, havebeen demonstrated (albeit primarilyin patients with heart failure) toreduce the incidence of atrial fibril-lation, presumably because ofantifibrotic effects (20).
Before pharmacologic cardioversionof atrial fibrillation present formore than 48 hours, patientsshould first receive adequate ther-apy for rate control and anticoagu-lation. In addition, serum potas-sium level should be greater than4.0 mmol/L, serum magnesiumlevel should be greater than 1.0mmol/L, and ionized calcium levelsshould be greater than 0.5 mmol/L[2.0 mg/dL]. In most cases, phar-macologic cardioversion should beperformed in a monitored hospitalsetting to permit adequate assess-ment of the degree of rate control,bradycardia, proarrhythmic affectsof antiarrhythmic agents, and otheradverse effects (21).
When is anticoagulation indicatedfor patients with atrialfibrillation?A meta-analysis (9) of 5 high-quality randomized trials (22–26)supports the use of antithrombotictherapy for appropriate patientswith nonvalvular atrial fibrillation.
Anticoagulation is indicated forpatients with atrial fibrillation
20. CHARM Investiga-tors. Prevention ofatrial fibrillation inpatients with symp-tomatic chronicheart failure by can-desartan in the Can-desartan in Heartfailure: Assessmentof Reduction in Mor-tality and morbidity(CHARM) program.Am Heart J.2006;152:86-92.[PMID: 16838426]
21. Maisel WH, KuntzKM, Reimold SC, etal. Risk of initiatingantiarrhythmic drugtherapy for atrial fib-rillation in patientsadmitted to a uni-versity hospital. AnnIntern Med.1997;127:281-4.[PMID: 9265427]
22. Stroke Prevention inAtrial FibrillationStudy. Final results.Circulation.1991;84:527-39.[PMID: 1860198]
23. Petersen P, BoysenG, Godtfredsen J, etal. Placebo-con-trolled, randomisedtrial of warfarin andaspirin for preven-tion of thromboem-bolic complicationsin chronic atrial fib-rillation. The Copen-hagen AFASAKstudy. Lancet.1989;1:175-9.[PMID: 2563096]
24. Connolly SJ, Lau-pacis A, Gent M, etal. Canadian AtrialFibrillation Anticoag-ulation (CAFA) Study.J Am Coll Cardiol.1991;18:349-55.[PMID: 1856403]
25. Ezekowitz MD,Bridgers SL, JamesKE, et al. Warfarin inthe prevention ofstroke associatedwith nonrheumaticatrial fibrillation. Vet-erans Affairs StrokePrevention in Non-rheumatic Atrial Fib-rillation Investiga-tors. N Engl J Med.1992;327:1406-12.[PMID: 1406859]
26. The Boston AreaAnticoagulation Trialfor Atrial FibrillationInvestigators. Theeffect of low-dosewarfarin on the riskof stroke in patientswith nonrheumaticatrial fibrillation. NEngl J Med.1990;323:1505-11.[PMID: 2233931]
27. Stroke Prevention inAtrial FibrillationInvestigators.Lessons from theStroke Prevention inAtrial Fibrillation tri-als. Ann Intern Med.2003;138:831-8.[PMID: 12755555]
when the risk for thromboem-bolism exceeds the risk for anticoagulation-associated bleeding(17). About one third of patientswith atrial fibrillation have a lowrisk for thromboembolism, onethird have a high risk, and onethird have a moderate risk (27).
In addition to established risk fac-tors for thromboembolism, specificfeatures of atrial fibrillation andunderlying disease also modulatethromboembolism risk. Patientswith reversible causes of atrial fib-rillation and those with structurallynormal hearts are less likely to havepersistent or recurrent episodes andmay be at a lower risk for throm-boembolism than patients withoutthese features. However, cliniciansshould keep in mind that the rateof stroke in patients with nonvalvu-lar atrial fibrillation and at least 1risk factor exceeds that of hemor-rhage from chronic anticoagulation.
Risk factors for thromboembolismhave been identified in the StrokePrevention in Atrial Fibrillationtrial (9). Patients younger than age65 years with nonvalvular atrial fib-rillation and no risk factors have anannual stroke risk of about 0.5%,whereas patients older than 65years with no risk factors have arisk of about 1%. This latter figureapproximates the risk for majorbleeding while on warfarin with aninternational normalized ratio(INR) of 2.0 to 3.0 (28, 29). Themean annual rate of major bleedingin the major anticoagulation trialson warfarin therapy was 1.2%.
Because of the delicate balancebetween risk and benefit, indiceshave been developed to assesswhich patients with atrial fibrilla-tion are at sufficient risk for stroketo warrant anticoagulation therapy.The most popular of these is theCHADS
2score (30, 31) (Table 2).
Table 3 presents recommendationsfor therapy based on this score.

© 2008 American College of PhysiciansITC5-11In the ClinicAnnals of Internal Medicine4 November 2008
A 2007 meta-analysis of 29 trials including28 044 participants characterized the effi-cacy and safety of antithrombotic agentsfor stroke prevention in patients who haveatrial fibrillation. Compared with controlparticipants, adjusted-dose warfarin (6 tri-als, 2900 participants) and antiplateletagents (8 trials, 4876 participants) reducedstroke by 64% (95% CI, 49% to 74%) and22% (CI, 6% to 35%), respectively. Adjusted-dose warfarin was substantially more effi-cacious than antiplatelet therapy (relativerisk reduction, 39% [CI, 22% to 52%]) (12 trials, 12 963 participants). Absolute in-creases in major extracranial hemorrhagewere small (0.3% per year) (32).
Some data indicate that risk factor–adjusted incidence of ischemicstroke and major bleeding is currently considerably less thanthat reflected in the previouslydescribed trials. The consensus isthat this is related to improvedtherapy for hypertension (33).Less-encouraging recent data haveindicated that the rate of majorbleeding is high in the elderly (34).
What regimens should cliniciansuse to anticoagulate patients withatrial fibrillation?Adjusted-dose warfarin to an INRof 2.0 to 3.0 is the first choice foranticoagulation of patients withatrial fibrillation. Certain patientswith prosthetic valves in additionto atrial fibrillation should have
28. Jung F, DiMarco JP.Treatment strategiesfor atrial fibrillation.Am J Med.1998;104:272-86.[PMID: 9552091]
29. Zabalgoitia M,Halperin JL, PearceLA, et al. Trans-esophageal echocar-diographic corre-lates of clinical riskof thromboem-bolism in nonvalvu-lar atrial fibrillation.Stroke Prevention inAtrial Fibrillation IIIInvestigators. J AmColl Cardiol.1998;31:1622-6.[PMID: 9626843]
30. Gage BF, WatermanAD, Shannon W, etal. Validation of clini-cal classificationschemes for predict-ing stroke: resultsfrom the NationalRegistry of Atrial Fib-rillation. JAMA.2001;285:2864-70.[PMID: 11401607]
31. van Walraven C, HartRG, Wells GA, et al. Aclinical predictionrule to identifypatients with atrialfibrillation and a lowrisk for stroke whiletaking aspirin. ArchIntern Med.2003;163:936-43.[PMID: 12719203]
32. Hart RG, Pearce LA,Aguilar MI. Meta-analysis: antithrom-botic therapy to pre-vent stroke inpatients who havenonvalvular atrial fib-rillation. Ann InternMed. 2007;146:857-67. [PMID: 17577005]
Table 2. Stroke Risk in Patients with Nonvalvular Atrial Fibrillation Not Treatedwith Anticoagulation According to CHADS
2Index*
CHADS2
Risk Criteria Score
Past stroke or TIA 2Age >75 y 1Hypertension 1Diabetes mellitus 1Heart failure 1
Patients (n= 1733) Adjusted Stroke Rate (%/y)†
(95% CI) CHADS2
Score
120 1.9 (1.2 to 2.0) 0463 2.8 (2.0 to 3.8) 1523 4.0 (3.1 to 5.1) 2337 5.9 (4.6 to 7.3) 3220 8.5 (6.3 to 11.1) 465 12.5 (8.2 to 17.5) 55 18.2 (10.5 to 27.4) 6
CHADS2
= Cardiac Failure, Hypertension, Age, Diabetes, and Stroke (Doubled); TIA = transientischemic attack.* Reproduced from reference 5 with permission from the American Heart Association.† The adjusted stroke rate was derived from multivariate analysis assuming no aspirin usage.Data from from references 30, 31.
Table 3. Antithrombotic Therapy for Patients with Atrial Fibrillation* Risk Category Recommended Therapy
No risk factors Aspirin, 81–325 mg daily1 moderate risk factor Aspirin, 81–325 mg daily or
warfarin (INR, 2.0–3.0, target 2.5)Any high risk factor or Warfarin (INR, 2.0–3.0, target 2.5)*more than 1 moderate risk factor
Less-Validated or Weaker Moderate Risk Factors High Risk FactorsRisk Factors
Female sex Age ≥75 y Previous stroke, TIA, or embolismAge 65–74 y Hypertension Mitral stenosisCoronary artery disease Heart failure Prosthetic heart valve†
Thyrotoxicosis LV ejection fraction 35% or less, diabetes mellitus
INR = international normalized ratio; LV = left ventricular; TIA = transient ischemic attack.* Reproduced from reference 5 with permission from the American Heart Association.† If mechanical valve, target INR >2.5.
warfarin titrated to an INR of 2.5to 3.5. In patients without addi-tional stroke risk factors (previousstroke or transient ischemic attack,age >75 years, hypertension, dia-betes, heart failure) or who havecontraindications to full anticoagu-lation, aspirin 325 mg/d can beused as alternative thromboem-bolism prophylaxis.
The effect of aspirin is controver-sial, but is probably present and less dramatic than that of warfarin(35). A recent trial demonstratedthat aspirin plus clopidogrel was

clearly inferior to adjusted-dosewarfarin (36).
Institution of warfarin withoutloading doses or concurrent heparinis sufficient in lower-risk patients,whereas patients at high risk forthromboembolism should be hospi-talized for immediate anticoagula-tion with unfractionated heparinbefore target levels of oral anticoag-ulation are reached. There are limiteddata on the use of low-molecular-weight heparin in this setting.
Patients with atrial fibrillation last-ing more than 48 hours or thosewith intracardiac thrombus shouldreceive anticoagulation with war-farin before cardioversion and forat least 4 weeks afterward.
Clinicians should consider chronicanticoagulation in patients who areat high risk for recurrent atrial fib-rillation, have asymptomatic atrialfibrillation, have evidence of intrac-ardiac thrombus, or have known
Warfarin has a narrow therapeuticwindow, and its metabolism isaffected by many drug and dietaryinteractions, requiring frequentINR monitoring and dosageadjustment. These limitations ofwarfarin have prompted a searchfor alternative anticoagulants. Atrial showed ximelagatran not tobe a suitable alternative to war-farin (37). Investigational studiesto develop other oral anticoagu-lants (direct thrombin inhibitors,factor Xa inhibitors) are inprogress, but there are no currentalternatives to warfarin.
When should clinicians considerimmediate cardioversion inpatients with atrial fibrillation?Prompt cardioversion should beconsidered for new-onset atrial
33. Hart RG, Tonarelli SB,Pearce LA. Avoidingcentral nervous sys-tem bleeding duringantithrombotic ther-apy: recent data andideas. Stroke.2005;36:1588-93.[PMID: 15947271]
34. Hylek EM, Evans-Molina C, Shea C, etal. Major hemor-rhage and tolerabil-ity of warfarin in thefirst year of therapyamong elderlypatients with atrialfibrillation. Circula-tion. 2007;115:2689-96. [PMID: 17515465]
35. The SPAF III WritingCommittee for theStroke Prevention inAtrial FibrillationInvestigators.Patients with nonva-lvular atrial fibrilla-tion at low risk ofstroke during treat-ment with aspirin:Stroke Prevention inAtrial Fibrillation IIIStudy. JAMA.1998;279:1273-7.[PMID: 9565007]
36. ACTIVE WritingGroup of the ACTIVEInvestigators. Clopi-dogrel plus aspirinversus oral anticoag-ulation for atrial fib-rillation in the Atrialfibrillation Clopido-grel Trial with Irbe-sartan for preventionof Vascular Events(ACTIVE W): a ran-domised controlledtrial. Lancet.2006;367:1903-12.[PMID: 16765759]
© 2008 American College of Physicians ITC5-12 In the Clinic Annals of Internal Medicine 4 November 2008
fibrillation when it is clear that theduration of the arrhythmia is lessthan 48 hours (as might be the casewhen atrial fibrillation onset occursin a hospitalized patient on cardiacmonitoring) and the patient is not athigh risk for stroke. Immediate car-dioversion, if successful, could obvi-ate the need for anticoagulation.
Most patients with atrial fibrilla-tion do not require immediatepharmacologic or electrical car-dioversion, but it may be appro-priate in selected patients withdecompensated heart failure,severe angina or acute infarction,hypotension, or high risk for acutestroke. Patients with atrial fibrilla-tion and the Wolff–Parkinson–White syndrome can haveextremely rapid atrioventricularconduction during atrial fibrilla-tion mediated by the accessorypathway, which is a potentiallylife-threatening condition thatrequires urgent cardioversion.
When should clinicians consideratrioventricular nodal catheterablation, device therapy, orsurgical techniques in patientswith atrial fibrillation?Nonpharmacologic therapy foratrial fibrillation should be consid-ered after failure or intolerance torate-control or rhythm-controltherapy. Nonpharmacologic thera-peutic options include catheter orsurgical atrioventricular nodal abla-tion and pacing.
Atrioventricular nodal catheterablation is used in situations wherepharmacologic rate control cannotbe achieved, usually because ofintolerance to medications. Thisoccurs most frequently in patientswith advanced heart failure orobstructive pulmonary disease (limiting β-blocker usage) or elderly patients. Atrioventricularnodal ablation is highly effective(38) but requires pacemaker inser-tion, which introduces the risk forproducing progressive left ventricu-lar dysfunction secondary to
risk factors for thromboembolism(age >65 years, recent heart failure,left-ventricular dysfunction onechocardiogram, past thrombo-embolism, diabetes mellitus, hyper-tension, or left atrial enlargement).

37. Kaul S, Diamond GA,Weintraub WS. Trialsand tribulations ofnon-inferiority: theximelagatran experi-ence. J Am Coll Car-diol. 2005;46:1986-95. [PMID: 16325029]
38. Wood MA, Brown-Mahoney C, Kay GN,Ellenbogen KA. Clini-cal outcomes afterablation and pacingtherapy for atrial fib-rillation : a meta-analysis. Circulation.2000;101:1138-44.[PMID: 10715260]
39. Packer DL, Asir-vatham S, MungerTM. Progress in non-pharmacologic ther-apy of atrial fibrilla-tion. J CardiovascElectrophysiol.2003;14:S296-309.[PMID: 15005218]
© 2008 American College of PhysiciansITC5-13In the ClinicAnnals of Internal Medicine4 November 2008
pacing. Catheter ablation of atrialfibrillation has been shown to beeffective in preventing recurrentsymptomatic atrial fibrillation inhighly selected patients (39).Recent guideline statements haveacknowledged that it may be rea-sonable to provide this therapy forhighly symptomatic patients withparoxysmal atrial fibrillation inwhom an attempt at antiarrhythmicdrug therapy has failed. This rela-tively aggressive approach may prevent progressive atrial fibrilla-tion–related morbidity (residualrisk for stroke, risk for medicationside effects), but the impact of this therapeutic strategy on mortal-ity has not been demonstrated.Innovative minimally invasive sur-gical ablation of atrial fibrillation is also available at highly special-ized centers.
Pacing therapy without atrioven-tricular nodal ablation has verylittle effect on atrial fibrillationburden, but may be helpful inpatients with paroxysmal atrial fib-rillation who have symptomaticbradycardia (often caused by sideeffects of atrial fibrillation pharma-cologic therapy).
How should clinicians monitorpatients with atrial fibrillation?Although there are few studies toinform the appropriate frequency offollow-up for patients with atrialfibrillation, clinical consensus is that
patients with atrial fibrillation shouldhave regular follow-up to assesssymptoms and clinical effectivenessof therapy. For many patients, anti-coagulation monitoring drives thefrequency of follow-up. Cliniciansshould assess rate control by askingabout such symptoms as palpitations,easy fatigability, and dyspnea onexertion. Examination should assessresting and exercise heart rates fortargets of 60 to 80 beats per minuteand 90 to 115 beats per minute,respectively. Patients in whomrhythm control is chosen should bemonitored for symptoms suggestiveof atrial fibrillation. Sporadic asymp-tomatic episodes of atrial fibrillationon therapy are not important and donot need to be monitored for. How-ever, patients who do not improve onrhythm-control drugs should bechanged to less-toxic rate-controlagents. Routine blood tests to evalu-ate for side effects of antiarrhythmictherapy are not essential, except inthe case of amiodarone, whichrequires liver and thyroid functionstudies every 6 months and chestradiography every year.
Which patients with newlydiagnosed atrial fibrillation shouldclinicians consider hospitalizing?Although atrial fibrillation is usu-ally managed in outpatient settings,clinicians should consider hospital-izing patients with atrial fibrillationwhen management requires closemonitoring for safety (see Box).
Situations in Which Patientswith Atrial Fibrillation MayRequire Hospitalization• Uncertain or unstable underly-
ing arrhythmia• Acute myocardial infarction,
altered mental status, decom-pensated heart failure, orhypotension
• Intolerable symptoms despitehemodynamic stability
• Elective cardioversion (if moni-tored outpatient setting is notavailable)
• Acute anticoagulation if very-high risk for stroke
• Telemetry monitoring duringinitiation of certain drugs
• Procedures such as cardiaccatheterization, electrophysio-logic studies, pacemakers,implantable defibrillators, orcatheter or surgical ablation
Treatment... Treatment goals for atrial fibrillation include preventing stroke,reducing symptoms, and preventing tachycardia-related cardiomyopathy. The use ofanticoagulants (aspirin or warfarin) is guided by risk classifications, such as theCHADS
2score. Several randomized trials have demonstrated no general advantage to
rhythm control over rate control. Rate control with calcium-channel antagonists orβ-blockers to keep heart rate at 60 to 80 beats per minute at rest and 90 to 115beats per minute during exercise should be the first-line therapy. Rhythm control,which has greater adverse effects than rate control, may be reasonable in individualpatients who do not respond to rate control. Atrial and atrioventricular nodal abla-tion therapy may be appropriate for selected patients with highly symptomatic atrialfibrillation despite pharmacologic therapy.
CLINICAL BOTTOM LINE
© 2008 American College of Physicians ITC5-14 In the Clinic Annals of Internal Medicine 4 November 2008
40. Snow V, Weiss KB,LeFevre M, et al.Management ofnewly detectedatrial fibrillation: aclinical practiceguideline from theAmerican Academyof Family Physiciansand the AmericanCollege of Physi-cians. Ann InternMed. 2003;139:1009-17. [PMID: 14678921]
PracticeImprovement Do U.S. stakeholders consider
management of patients with atrialfibrillation when evaluating thequality of care physicians deliver?The Centers for Medicare & Med-icaid Services (CMS) has issuedspecifications for 74 measures thatmake up the 2008 Physician QualityReporting Initiative (PQRI). Ofthese 74 measures, none directlymeasures the quality of atrial fibrilla-tion therapy. However, one of thestroke measures does relate to atrialfibrillation. This measure examinesthe percentage of patients age 18years or older with a diagnosis ofischemic stroke or transient ischemicattack and documented permanent,persistent, or paroxysmal atrial fibril-lation who were prescribed an anti-coagulant at discharge.
What do professionalorganizations recommend with regard to the management of patients with atrial fibrillation?The material presented in thisreview is consistent with the 2006guidelines developed by a consen-sus panel of the American HeartAssociation, American College ofCardiology, and the EuropeanSociety of Cardiology (17). In2003, the American College ofPhysicians and the AmericanAcademy of Family Physiciansreleased a guideline on atrial fibril-lation management (40). Bothguideline statements stress antico-agulation in appropriately selectedpatients and the nonsuperiority of the rhythm-control strategy.The AHA/ACC/ESC guidelineemphasizes the cardiology perspec-tive, whereas the ACP/AAFPfocuses on the primary care perspective.
inthe
c linicTool Kit
in the clinic
Atrial Fibrillation
PIER Moduleswww.pier.acponline.orgAccess PIER module on atrial fibrillation for updated, evidence-based informationdesigned for rapid access at the point of care.
Quality Measurespier.acponline.org/qualitym/prv.htmlAccess the PIER Quality Measure Tool, which links newly developed quality measuresissued by the Ambulatory Quality Alliance and the Physician Quality Improvement QAAlliance and CMS’s Physician Quality Reporting Initiative program to administrativecriteria for each measure and provides clinical guidance to help implement the measuresand improve quality of care.
Patient Informationwww.annals.intheclinic/toolsDownload copies of the Patient Information sheet that appears on the following page forduplication and distribution to your patients.
Anticoagulation Flow Sheetwww.acponline.org/running_practice/quality_improvement/projects/cfpi/doc_anticoag.pdfDownload a copy of a flow sheet to help manage patients on warfarin.
Guidelineswww.americanheart.org/downloadable/heart/222_ja20017993p_1.pdfAccess the American Heart Association, American College of Cardiology, and EuropeanSociety of Cardiology joint 2006 guidelines for the management of patients with atrialfibrillation.www.annals.org/cgi/reprint/139/12/1009.pdfAccess the American College of Physicians/American Academy of Family Physicians2003 guidelines for the management of newly detected atrial fibrillation.
WHAT YOU SHOULD KNOWABOUT ATRIAL FIBRILLATION
In the ClinicAnnals of Internal Medicine
annals.org
Atrial fibrillation is an irregular and some-times very fast heart beat. Atrial fibrilla-tion can come and go or be constant. It ismore common in older people than inyounger people and in people with heartconditions.
Atrial fibrillation can lead to 3 bad healthoutcomes:
• Symptoms that can make a personunable to do their usual activities.
• Over the long term, a very fast heartbeat can damage heart muscle.
• Atrial fibrillation can cause strokewhen blood clots form in the heart andtravel to the brain.
How would I know if I have atrial fibrillation?
• Many people with atrial fibrillationhave no symptoms and don’t knowthat they have it.
• When people have symptoms, theyinclude palpitations (pounding in the chest), shortness of breath, or tiredness.
• Your doctor may see atrial fibrillationon an electrocardiogram (ECG) if anepisode occurs during the test.
• If you have symptoms that could beatrial fibrillation but your ECG is nor-mal, your doctor may send you for atest that records your heartbeat whileyou go about your usual activities.
• If you have atrial fibrillation, your doc-tor may do an echocardiogram to lookfor heart problems. Echocardiogramsuse sound waves to take pictures ofthe heart.
What is the treatment?
• Many patients with atrial fibrillationneed to be on drugs to prevent stroke.Some people need only aspirin. Othersneed to take the blood thinner warfarin.
• Treatment also sometimes includesdrugs to slow the heart rate down ormake it more regular.
• Less often, treatment with catheters,surgery, and pacemakers is needed.
• Atrial fibrillation treatment can havedangerous side effects. It is importantto follow instructions and see yourdoctor regularly.
Web Sites with Good Information
MedlinePlus: www.nlm.nih.gov/medlineplus/tutorials/atrialfibrillation/htm/_no_50_no_0.htm
Heart Rhythm Society:www.hrspatients.org/patients/heart_disorders/atrial_fibrillation/default.asp
American Heart Association: circ.ahajournals.org/cgi/content/full/117/20/e340 Pa
tien
t In
form
atio
n

© 2008 American College of Physicians In the Clinic Annals of Internal Medicine
CME Questions
A 70-year-old woman with type 2 dia-betes mellitus is evaluated for dyspneaand fatigue. She has a history of atrialfibrillation that has resulted in thesesymptoms in the past. She has had suc-cessful cardioversions, most recentlyabout 2 years ago. She has hypertensioncontrolled with medication. She also hasmild left-ventricular dysfunction relatedto coronary artery disease and history ofmyocardial infarction. Her current med-ications include atenolol, lisinopril,aspirin, atorvastatin, and insulin.
Physical examination demonstrates anirregularly irregular rhythm with a heartrate of 78 beats per minute. Blood pres-sure is 130/80 mm Hg. The cardio-vascular and pulmonary examinationsare otherwise unremarkable.
What medication should this patientreceive before cardioversion?
A. Aspirin and dipyridamoleB. WarfarinC. ClopidogrelD. No additional medication is
needed
A 70-year-old woman reports mildeffort intolerance over the last severalmonths but has continued her usualactivities. She has a history of hyperten-sion that is well controlled with diuretictherapy. Findings on physical examina-tion and electrocardiography are consis-tent with atrial fibrillation, with a ven-tricular rate of 100 beats per minute,but were otherwise normal. Echocardio-gram shows a left-ventricular ejectionfraction of 55%, with left atrial enlarge-ment, mild mitral annular calcification,and mild mitral regurgitation. She hasno history of stroke or ulcer disease.
Which of the following would be themost appropriate therapy for thispatient?
A. Aspirin and a β-blocker B. Aspirin and amiodarone C. Aspirin and digoxin D. Warfarin and a β-blocker E. Warfarin and amlodipine
A 61-year-old man with a history ofmyocardial infarction, paroxysmal atrialfibrillation, ischemic cardiomyopathy,and heart failure presents for furthermanagement. He underwent percuta-neous revascularization 4 years ago. He has not had chest pain and he hadundergone an exercise scintigraphicstudy 2 months ago without stress-induced ischemia. His left-ventricularejection fraction was estimated to be35%. He has had NYHA class II symp-toms with mild dyspnea on moderateexertion. He had multiple episodes ofatrial fibrillation starting 4 years ago.His last recurrence of atrial fibrillationwas 4 months ago. At that time he wasstarted on anticoagulation with warfarinand amiodarone. He has been toleratinghis medications well. He has had no palpitations in the past 4 months. He isbeing treated with lisinopril, 20 mg/d,carvedilol, 25 mg/d, digoxin, 0.125 mg/d,atorvastatin, 10 mg/d, amiodarone, 200mg/d, and warfarin, 5 mg/d. His INR hasranged from 2.1 to 2.7. His electro-cardiogram on this visit shows normalsinus rhythm and evidence of a pastanterior myocardial infarction. A 24-hour Holter monitor performed last week showed no evidence of atrialfibrillation and occasional prematureventricular contractions.
Which of the following treatmentoptions would you recommend?
A. Discontinue warfarin, continueamiodarone
B. Discontinue amiodarone, startprocainamide
C. Discontinue amiodarone andwarfarin
D. Continue amiodarone andwarfarin
E. Refer patient for atrial fibrillationablation
Which one of the following statementsabout atrial fibrillation is correct?
A. Lone atrial fibrillation is acommon cause of atrialfibrillation.
B. Atrial fibrillation is more commonin older women than in older men.
C. Anticoagulation is not indicatedin patients who havenonrheumatic heart disease andatrial fibrillation.
D. Many patients who have atrialfibrillation do not requireantiarrhythmic therapy.
E. Atrial fibrillation is a serious andcommon problem in patients whohave the Wolff–Parkinson–Whitesyndrome.
A 67-year-old woman is admitted to theemergency room because of suddenonset of chest pain and rapid pulse. Shehas no history of similar occurrences.Physical examination reveals a palediaphoretic woman in moderate respira-tory distress. Her blood pressure is pal-pable at 75 mm Hg systolic. Lungs showbibasilar crackles. There is no jugularvenous distention and heart sounds aredistant with a variable S1. A 12-leadelectrocardiogram is shown.
What is the appropriate immediatetherapy?
A. Rapid infusion of 250 mL ofnormal saline
B. Diltiazem, 20 mg intravenously,followed by 10 mg/h infusion
C. Digoxin, 0.50 mg intravenouslyD. Direct-current cardioversionE. Procainamide, 500 mg
intravenously over 20 min
Questions are largely from the ACP’s Medical Knowledge Self-Assessment Program (MKSAP). Go to www.annals.org/intheclinic/ to obtain up to 1.5 CME credits, to view explanations for correct answers, or to purchase the complete MKSAP program.
1. 3.
2.
4 November 2008ITC5-16
5.
4.




















