Embed Size (px)
Citation preview


In the name of GOD

Abdominal Trauma &Abdominal Trauma &
hollow viscous injurhollow viscous injuryy

Abdominal injuries
• Solid organ injuries
• Hollow viscous injuries

Clinical findings
• Abdominal pain
• Guarding

Hollow viscous injuries
• Delay diagnosis (8-12 h)
– Hemorrhage
– Peritonitis
– Abdominal sepsis

Basic mechanisms of bowel and mesenteric injuries
• Shearing injuries caused by deceleration
• Crush injuries from direct impact
• Burst injuries from sudden increases in
intraluminal pressure

Site of injuries
• Small bowel
• Colon
• Duodenum
• Stomach

Imaging modalities
• Plain radiography
• Sonography
• CT scan

Plain radiography
• Chest X ray
• Abdominal radiography (supine &
upright)

Pneumoperitoan

Pneumoperitoan

Pneumoperitoan
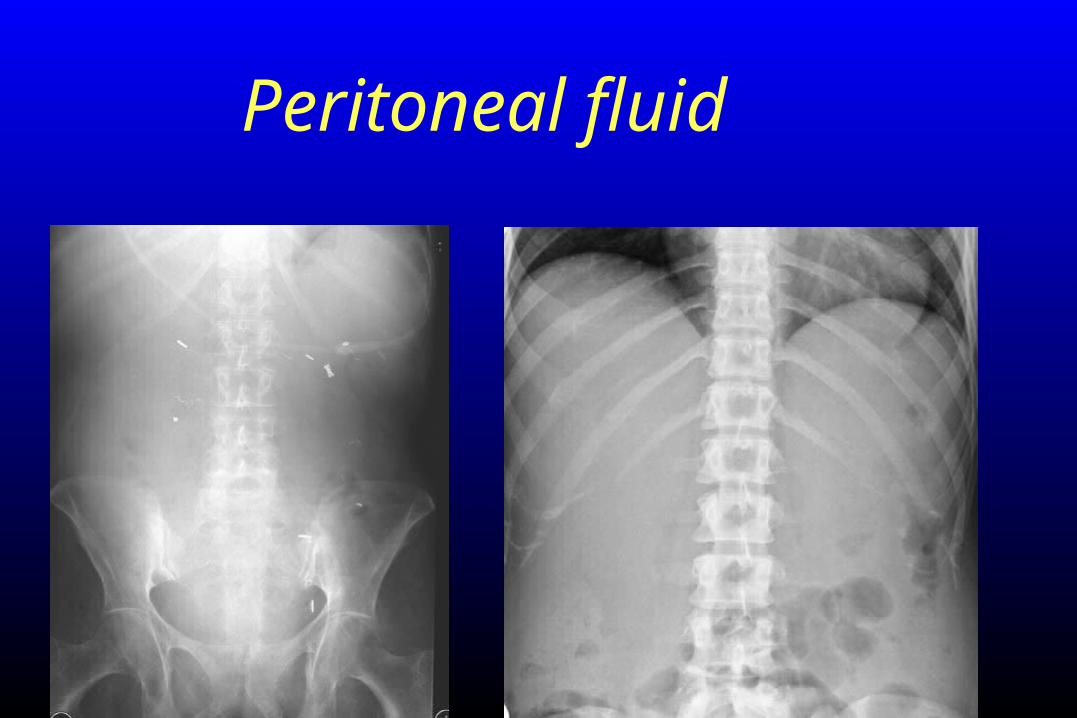
Peritoneal fluid

Ultrasound examination
• Free fluid
• Pneumoperitoneum
• Air in bowel wall
• Wall thickening of bowel loops

Pneumoperitoan

Pneumoperitoan

Air in Morrison’s pouch

Bowel loop hematoma

Bowel wall thickening, air bubble in its wall

CT Technique
• IV contrast (100-120 ml)• Portal venous phase (70 second delay)• Delay film (7 minute)• Oral contrast +/_• Rectal contrast +/_

CT signs of bowel loops injury
• Wall transection with focal discontinuity (spe:100%& sen:7%)
• Extraluminal oral contrast
• Pneumoperitoneum (20-75%)
• Pneumoretroperitoneum
• Focal wall thickening
• Abnormal wall enhancement
• Ill defined increased attenuation of mesentry
• Intra peritoneal fluid

Hemoperitoan

focal segment of thickened jejunumassociated stranding of the small bowel mesentery

segment of thickened jejunum and hemoperitoneum

wall thickening in a segment of jejunum

segment of thickened and poorly enhancing small bowel

Mesenteric fat stranding

Other causes of pneumoperitoneum
• Bladder rupture with an indwelling Foley catheter
• Massive pneumothorax
• Barotrauma
• Benign pneumoperitoneum
• Peritoneal lavage
• Pseudopneumoperitoneum (air between abdominal wall and parietal peritoneum)

Pneumoperitoneum and pseudopneumoperitoneum

Diffuse bowel wall thickening
• Fluid over load– Liver inhomogeneous enhancement(nutmeg appearance)– Periportal edema
• Hypoperfusion complex(shock bowel)– Flat IVC– Increased enhancement of adrenal gland– Retroperitoneal edema



Diffuse thickening and hyperenhancementof the loops due to aggressive resuscitation with
intravenous fluids




Duodenal injuries
• More secondary to penetrating injuries and less likely due to blunt trauma
• CT findings: wall thickening, discontinuity, contrast extravasation, fluid adjacent to the duodenum and pancreatic head and retroperitoneum air or fluid

Duodenal wall thickeningand extensive hemoperitoneum

Colonic injuries
• Wall transection with focal discontinuity• Contrast extravasation • Pneumoperitoneum• Pneumoretroperitoneum • Focal wall thickening• Abnormal wall enhancement• Ill defined increased attenuation of mesentry• Intra peritoneal fluid

Transverse colonic wall thickening
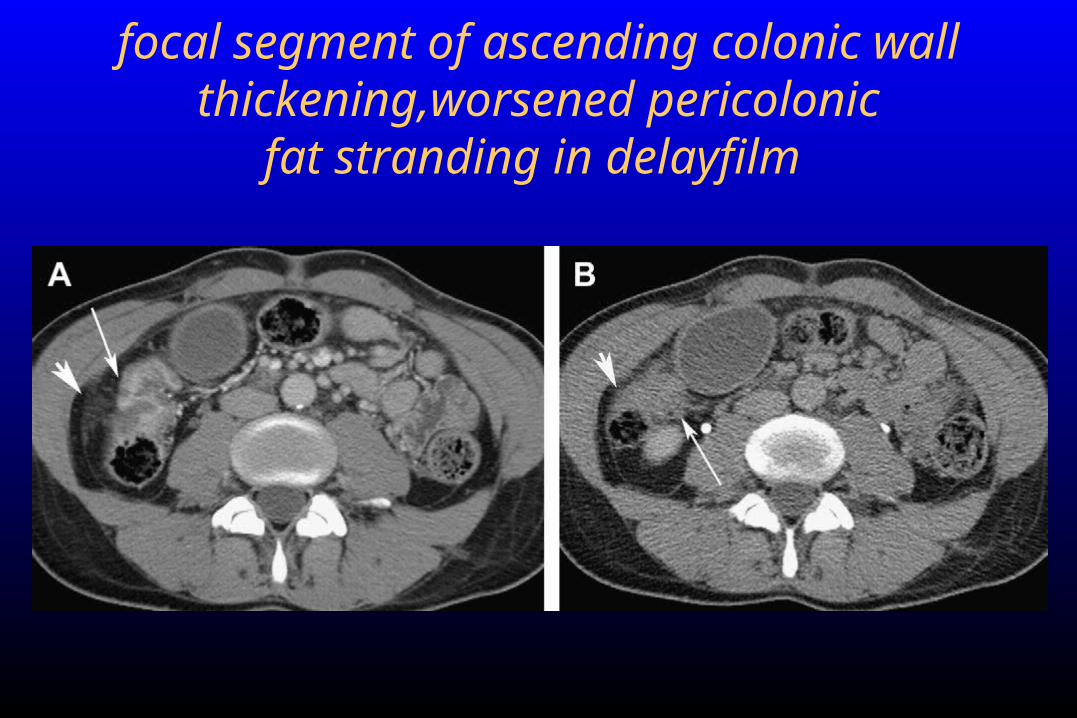
focal segment of ascending colonic wall thickening,worsened pericolonic
fat stranding in delayfilm

Sign mesenteric trauma
• Mesenteric hematoma
• Intraperitoneal extravasation of intravenous contrast
• Abrupt termination of mesenteric vessels
• Unequivocal irregularity of the wall of mesenteric vessels
• Increased attenuation of the mesentery

small focal hematoma in the root of the mesentery

Mesenteric hematoma

Mesenteric hematoma

Mesenteric bleeding

Focal collection of high attenuation fluid is seen in the root of the mesentery

abnormally positioned in the right hemiabdomen , with subtle stranding of the corresponding mesentery due to
traumatic internal hernia

Anorectal injury
• Mortality rate three times more than colonic injury
• Associated with pelvic fracture
• concomitant with bladder, urethral and vascular injuries
• Divided into intraperitoneal and extraperitoneal

Extraluminal air is seen in the
presacralspace
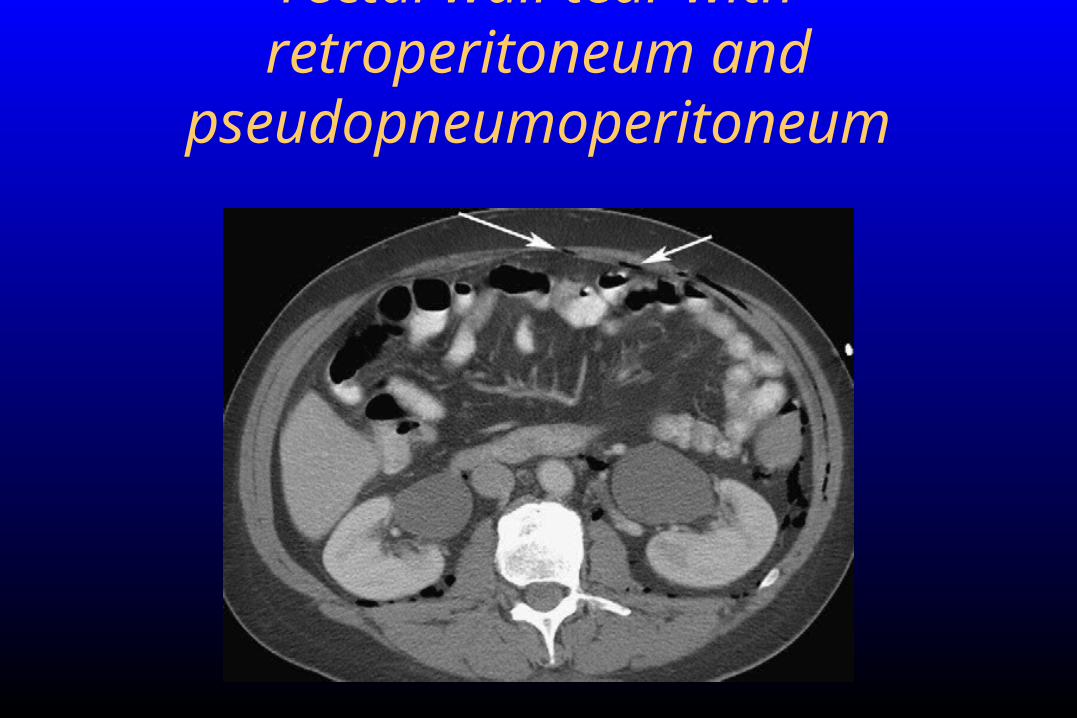
rectal wall tear with retroperitoneum and pseudopneumoperitoneum

Injury of mesentery and mesenteric vessels
• Extravasation of IV contrast
• Mesentric hematoma
• Mesentric infiltration
• Beading or abrupt termination of mesentric vessels
• Mesentric rent with internal hernia

Mesenteric hematoma

Mesenteric tear

Causes of retroperitoneal air
• Colonic perforation (ascending and descending)
• Duodenal injuries
• Pneumothorax
• Pneumomediastinum

Pneumoperitoneum and pseudopneumoperitoneum

Free peritoneal fluid
• Most common finding (most sensitive)
• Absence of free fluid excludes surgical important injury
• The attenuation is highest in the vicinity of the injured organ (sentinel clot)
• Localized fluid (triangle sign)
• Attenuation of hemoperitoan is high (>30-40) , simple fluid H.U is about 13

Lesser sac hematoma

Sentinel clot sign

Sentinel clot sign

hemoperitoneum (mean attenuation, 39 HU) due to small hepatic laceration

A small amount free pelvic fluid with mean attenuation of the8 HU

Thank you