Embed Size (px)
Citation preview

In the name of God

endometriosis in adolescents
Dr Safoura Rouholamin


• A 20 y.o. woman presents to her gynecologist with a 4 year history of increasing lower abdominal pain with her menses. The pain begins on the first day of her menses and lasts 2-3 days. She also complains of lower back pain and nausea. Menarche occurred at the age of 13 and her menses occur every 28 days and last 5 days. Physical and pelvic exam are normal

CLINICAL MANIFESTATIONS
• both acyclic and cyclic pain (severe, progressive dysmenorrhea)
• Bowel symptoms (eg, rectal pain, constipation, painful defecation that may be cyclic, rectal bleeding)
• bladder symptoms (eg, dysuria, urgency, hematuria) are also common
• ovarian endometriomas and infertility are rare in adolescents

INITIAL EVALUATION
• The abdominal examination is usually normal.• On pelvic examination, adolescents rarely have
uterosacral nodularity, a common finding in adults with the disease, but pain in the cul-de-sac is common.
• Adnexal enlargement may be palpable if an endometrioma is present, but these masses are also rare in adolescents
• Wright KN, Laufer MR, Endometriomas in adolescents. Fertil Steril. 2010;94(4):1529.e7.

INITIAL EVALUATION
• Sonographic examination should be performed to augment a limited physical examination and identify/exclude causes of abdominopelvic pain other than endometriosis.

TRIAL OF MEDICAL THERAPY FOR DYSMENORRHEA
• Hormonal therapy, such as a cyclic low-dose combination estrogen/progestin oral contraceptive pill (OC), or progestin only therapy (oral, injectable, or implantable), should be given with the NSAIDs
• American College of Obstetricians and GynecologistsACOG Committee Opinion. Number 310, April 2005. Endometriosis in adolescentsObstet Gynecol. 2005;105(4):921

• If the pain does not resolve with NSAIDs and hormonal therapy, then further evaluation is necessary to determine whether endometriosis is the etiology of the pain.

PATIENTS WHO FAIL THERAPY FOR DYSMENORRHEA
• A definitive diagnosis should be established before administering further treatment to adolescents who have persistent pain after three to six months of hormonal therapy and NSAIDS for the treatment of dysmenorrhea
• Laparoscopy is the gold standard for diagnosis of endometriosis
• American College of Obstetricians and Gynecologists.ACOG Committee Opinion. Number 310, April 2005. Endometriosis in adolescentsObstet Gynecol. 2005;105(4):921

• We suggest that if her pain interferes with her daily life's activities or places her at a disadvantage in academics, sports, or social activities compared with others, then she should undergo laparoscopy for definitive diagnosis.

• At surgery, up to 70 percent of adolescents with chronic pelvic pain that has not responded to a trial of NSAIDs and cyclic OCs are found to have endometriosis
• • Laufer MR, Goitein L, Bush M, Cramer DW, Emans SJPrevalence of endometriosis in adolescent girls with
chronic pelvic pain not responding to conventional therapy. J Pediatr Adolesc Gynecol. 1997;10(4):199

Diagnostic (and therapeutic) laparoscopy
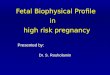
• red flame lesions were more common and powder burn lesions less common in adolescents than in adult patients
• This is consistent with the presumption that powder burn lesions represent older, more advanced implants.
• Clear and red lesions may be the more painful lesions of endometriosis
• Peritoneal windows or defects are also common in adolescents and should be recognized as diagnostic of endometriosis.

The top, middle, and bottom series are representative of red, white, and black implants, respectively

• If no evidence of endometriosis is identified, a posterior cul-de-sac biopsy to exclude the presence of microscopic disease should be performed and may identify lesions not visualized on laparoscopy.
• Nisolle M, Paindaveine B, Bourdon A, Berlière M, Casanas-Roux F, Donnez JHistologic study of peritoneal endometriosis in infertile women. Fertil Steril. 1990;53(6):984.

• ٍٍٍ���Experience at Children's Hospital, Boston, is that we find microscopic endometriosis in 3 percent of adolescent girls with chronic pelvic pain unresponsive to conventional therapy and with a visually normal pelvis
• Laufer MR, Goitein L, Bush M, Cramer DW, Emans SJPrevalence of endometriosis in adolescent girls with chronic pelvic pain not responding to conventional therapy. J Pediatr Adolesc Gynecol. 1997;10(4):199

Surgical treatment
• Electrocautery, endocoagulation, or laser ablation or resection of implants should be performed at the time of diagnostic laparoscopy
• Lysis of adhesions is also performed at the time of surgery.
• Cook AS, Rock JA The role of laparoscopy in the treatment of endometriosis. Fertil Steril. 1991;55(4):663.

• surgery alone is not adequate treatment for endometriosis as there can be microscopic residual disease that must be suppressed with medical therapy
• Symptoms will return within one year in approximately 50 percent of adult women who receive only surgical therapy
• Gambone JC, Mittman BS, Munro MG, Scialli AR, Winkel CA, Chronic Pelvic Pain/Endometriosis Working GroupConsensus statement for the management of chronic pelvic pain and endometriosis: proceedings of an expert-panel consensus process. Fertil Steril. 2002;78(5):961.

POSTOPERATIVE MEDICAL TREATMENT
• The general consensus is that adolescents with histologically confirmed endometriosis should receive medical treatment after surgical ablation/resection until they have completed childbearing
• American College of Obstetricians and Gynecologists.ACOG Committee Opinion. Number 310, April 2005. Endometriosis in adolescentsObstet Gynecol. 2005;105(4):921

• The goal of medical therapy is to manage pain due to residual disease, allow the patient to function comfortably in her daily activities, and suppress disease progression, which could impair fertility.
• Long-term follow-up data in adolescents show that endometriosis that is surgically identified and destroyed and then followed by medical therapy tends not to progress
• Unger CA, Laufer MR. Progression of endometriosis in non-medically managed adolescents: a case seriesJ Pediatr Adolesc Gynecol. 2011;24(2):e21.

• The choice of treatment depends upon the severity of the patient's symptoms, the extent of disease, and compliance.
• combination hormonal therapy or GnRH agonists are usually used for first-line therapy.

• For adolescents with confirmed endometriosis, we offer both therapies to those ages 16 or over, but use only continuous combination hormonal therapy in those under 16 years of age out of concern about the effects of GnRH agonists on the formation of normal bones and bone density
• Lubianca JN, Gordon CM, Laufer MRAdd-back" therapy for endometriosis in adolescents. J Reprod Med. 1998;43(3):164.

Combination estrogen/progestins
• Combination therapy can be used to suppress menstruation and induce a “pseudo-pregnancy” state for suppression of endometriosis and endometriosis associated pain.

Progestins
• Progestins inhibit endometriotic tissue growth by causing initial decidualization and eventual atrophy.
• They also inhibit pituitary gonadotropin secretion and ovarian hormone production, resulting in a mildly hypoestrogenic state relative to normal.

Progestins
• The most commonly used progestational agents are:
• Norethindrone acetate (5 to 15 mg daily by mouth)
• Medroxyprogesterone acetate (30 to 50 mg daily by mouth)
• Depot medroxyprogesterone acetate (150 mg intramuscularly every one to three months)

GnRH agonists
• GnRH agonists can be prescribed for adolescents, with laparoscopically confirmed endometriosis, who are at least 16 years old.
• Our preference is depot leuprolideacetate (11.25 mg intramuscularly every three months); it is always given with add-back therapy.

GnRH agonists
• Generally, initial treatment with a GnRH agonist is continued for six months.
• Upon completion of this initial six-month course of GnRH agonist therapy, the patient must then choose a treatment course.

GnRH agonists
• She can return to a continuous combined hormonal contraceptive, as described above.
• If she is not able to tolerate continuous combination hormonal or progesterone only therapy, then long-term utilization of a GnRH agonist with add-back can be prescribed

GnRH agonists
• A baseline bone density assessment is obtained after the initial six to nine months of therapy and is then repeated every two years.
• If bone density remains stable, then the assessment is repeated every two years while the patient is receiving GnRH agonists

Add-back therapy
• Norethindrone acetate (5 mg daily) alone, • Conjugated estrogen (0.625 mg) plus either
norethindrone acetate (5 mg) or medroxyprogesterone acetate (5 mg daily)

Danazol
• Given the side effect profile, danazol would likely be poorly tolerated by adolescents, and thus is not utilized in the management of endometriosis in the adolescent population.

MANAGEMENT OF RECURRENT PAIN
• Endometriosis is a chronic and progressive disease, thus pain can recur despite therapy

MANAGEMENT OF RECURRENT PAIN
• Changing to a different treatment modality. • If girls less than 16 years of age have
persistent pain while taking continuous combination hormonal therapy, then utilization of GnRH agonists with add-back therapy may be needed.
• One course of six to nine months of therapy may be adequate, followed by return to combination continuous hormonal therapy

MANAGEMENT OF RECURRENT PAIN
• Prolonged utilization of a GnRH agonist with add-back therapy.
• We have treated patients with surgically diagnosed disease refractory to other medications with prolonged GnRH agonist treatment plus add-back for over 10 years.
• A baseline bone density evaluation should be obtained prior to starting retreatment with a GnRH agonist or if therapy is to be continued for over six to nine months

• If bone density is decreasing despite add-back therapy, then either surgical ablation/excision or continuous combination hormonal therapy are options.
• As noted above, the long-term utilization of a GnRH agonist with add-back therapy has not been studied in the adolescent population
• Lubianca JN, Gordon CM, Laufer MRAdd-back" therapy for endometriosis in adolescents. J Reprod Med. 1998;43(3):164.

• Pain that does not respond to aggressive medical therapy may be due to recurrent endometriosis, endometriomas, and/or pelvic adhesions from endometriosis or prior surgery.

• A repeat laparoscopic procedure should be considered in this clinical situation.
• If surgery is to be undertaken, then lysis of adhesions should be performed laparoscopically.
• All visible lesions of endometriosis should be cauterized, laser ablated, or resected. We utilize adhesion preventive agents laparoscopically following surgical lysis of adhesions.

Protocol for evaluation and treatment of adolescent pelvic pain/endometriosis