Embed Size (px)
Citation preview

In the Name of God
1st Endodontic Workshop
Dental School,
Shahid Beheshti University of Medical Sciences
1

Refrences:
Pathways of the Pulp (Tenth ed)
Zohre Ahangari , D.D.S. ; M.S.c.: Associate Professor of Endodontics DepartmentDental School of ShahidBeheshti University of Medical Sciences
Omid Dianat, D.D.S ; M.S.c: Assistant Professor of Endodontics DepartmentDental School of ShahidBeheshti University of Medical Sciences
Nazanin Zargar ; D.D.S. ; M.S.c.: Assistant Professor of Endodontics DepartmentDental School of ShahidBeheshti University of Medical Sciences
2

Diagnosis and Treatment Planning
3

Diagnosis is the determination of the nature of a
diseased condition by careful investigation of its
symptoms and history
Definition
4

∗ Medical History Review
∗ Subjective History
∗ Objective Testing
∗ Analysis of data collected – Clinical diagnosis
∗ Plan of Action
Sequence of Events
5

Chief complaint
• In patient’s own words
▫ “My tooth hurts when I chew hard foods”
▫ “I can’t drink cold soda”
Subjective History
6

Pain History
7

Pain History
∗ Location
∗ Intensity
∗ Duration
∗ Stimulus
∗ Relief
∗ Spontaneity
Subjective History
8

Very poorly localized
∗ Intermittent
∗ Throbbing
∗ Intensified by heat, cold and sometimes chewing
∗ May be relieved by cold
∗ Usually severe
Pulpal Pain
9

Pulpal Pain
10

• May be well localized
• Deep pain
• Intensified by chewing
• Moderate to severe in intensity
Periradicular Pain
11

• May be well localized
• Intensified by chewing
• Moderate to severe in intensity
Periodontal Pain
12

Periradicular /Periodontal Pain
13

• Gives rise to tentative diagnosis
• Determines urgency of treatment
• Confirmed by examination and special tests
Subjective History
14

• Visual Examination
• Radiographs
• Percussion
• Palpation
• Mobility
• Thermal tests
Objective Testing
15

• Electric Pulp Test
• Periodontal probing
• Selective anesthesia
• Test cavity
• Transillumination
• Occlusion
Objective Testing
16

• Extra-oral examination
▫ Facial asymmetry
▫ Swelling
▫ Extra oral sinus tract
▫ TMJ
Visual Examination
17

Extra-oral Swelling
18

Visual Examination
Extra oral sinus tracts
associated with necrotic teeth
19

Intra-oral examination
∗Soft tissue lesions
∗Swelling
∗Redness
∗Sinus tract
Visual Examination
20

Acute apical abscess
Acute apical abscess
Incision and drainage
21

Visual Examination
A sinus tract should be traced
with a gutta-percha cone
22

Hard tissues
∗Caries
∗Large or defective restorations
∗Discolored/chipped teeth
Visual Examination
23

Discoloration
24

∗ Always take your own pre-operative radiograph
∗ Never make a diagnosis based on radiographic
evidence alone
Radiographs
25
• Consider taking a bitewing film of posterior teeth
• Note characteristic appearance of fractured root
Radiographs
26

Radiographs
Characteristic J-shaped or halo lesion associated with
fractured root
27

• A very significant test
• Always compare suspect tooth with adjacent and
contralateral teeth
• Tenderness indicates inflammation in the PDL
• Cause of inflammation may be pulpal or periodontal
Percussion Test
28

Percussion Test
Vertical percussion Horizontal percussion29
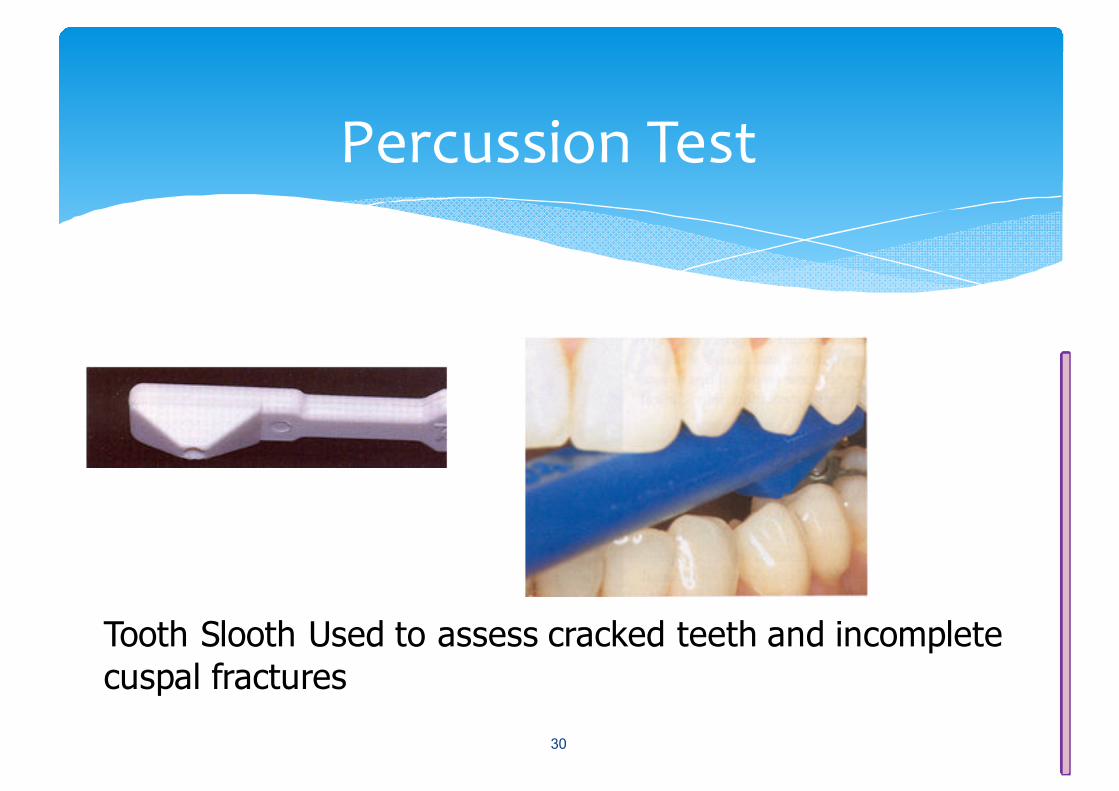
Percussion Test
Tooth Slooth Used to assess cracked teeth and incomplete
cuspal fractures
30

• Extraoral
▫ To detect swollen or tender lymph nodes
• Intraoral
▫ May detect early periapical tenderness
▫ Identifies soft tissue swelling
▫ Must compare with other areas
Palpation Test
31

Palpation
32

• Reflects the extent of inflammation in the PDL
• Compare with adjacent and contralateral teeth
• There are many causes of mobility besides pulpal inflammation
extending into the PDL
Mobility
33

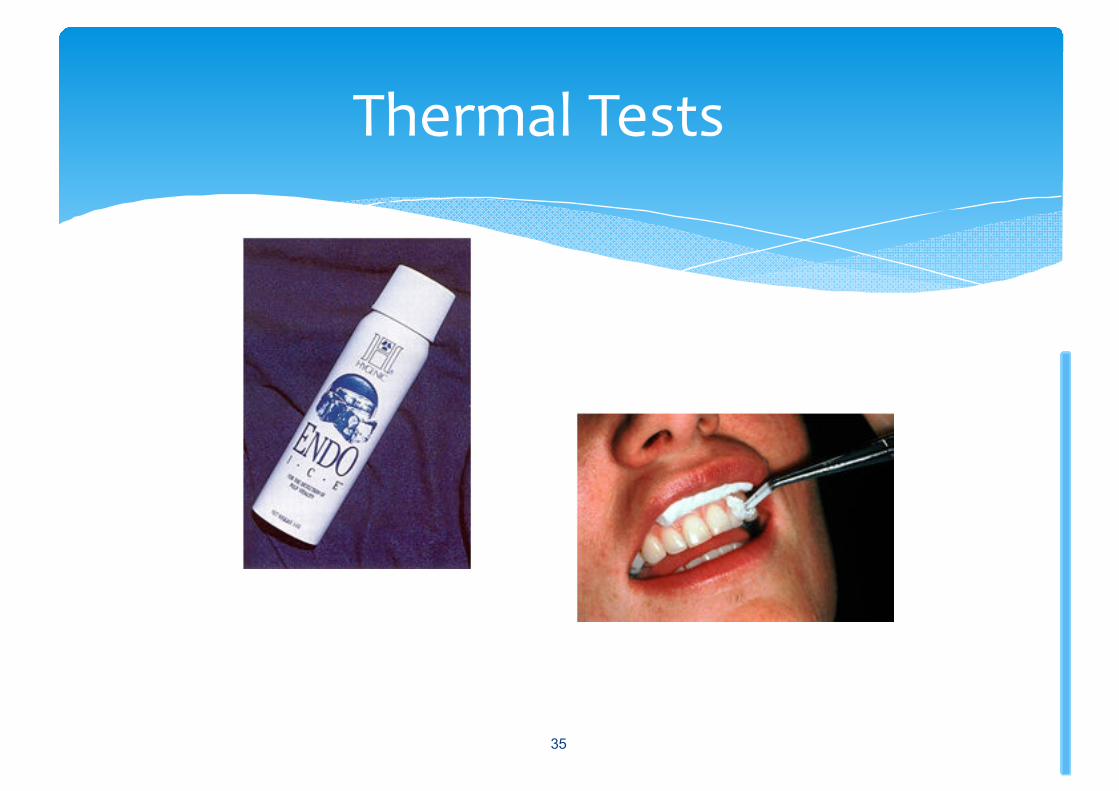
• Cold always used
• Heat rarely used
• Compare reaction with adjacent and contralateral
teeth
• Refractory period of at least 10 minutes before pulp
can be retested accurately
Thermal Tests
34
Thermal Tests
35

Thermal Tests
Ice stick
CO2 Snow
36

∗ Isolate area with cotton rolls
∗ Dry teeth to be tested
∗ Ask patient to:
∗ “Raise hand on feeling cold”
∗ “Lower hand when cold feeling goes away”
∗ Record:
∗ + or – sensitivity to cold
∗ Time until cold sensitivity was felt
∗ Time that cold sensitivity lingered
Thermal Tests
37

Classic Responses to Thermal (cold) Testing:
• Normal Pulp: Moderate transient pain
• Reversible Pulpitis: Sharp pain; subsides quickly
• Irreversible pulpitis: Pain lingers
• Necrosis: No response
(Note false positive and false negative responses common)
Thermal Tests
38

• A direct test of nerve elements of pulpal tissue
• Vitality versus non-vitality only – not whether vital pulp
is normal or inflamed
• In multi-rooted teeth, where one canal is vital – tooth
usually tests vital
• False positives and false negatives may occur
Electric Pulp Test
39

False positive reading:
∗ Electrode contact with metal restoration or gingiva
∗ Patient anxiety
∗ Liquefaction necrosis
∗ Failure to isolate and dry teeth prior to testing
Electric Pulp Test
40

Electric Pulp Test
41

False negative reading:
• Patient is heavily premedicated
• Inadequate contact between electrode and enamel
• Recently traumatized tooth
• Recently erupted tooth with open apex
• Partial necrosis
Electric Pulp Test
42

Electric Pulp Testing
43

• Periodontal probing pocket depths must be measured and
recorded
• A significant pocket, in the absence of periodontal disease
may indicate root fracture
• Poor periodontal prognosis may be a contraindication to root
canal therapy
Periodontal Examination
44

Periodontal Examination
45

Periodontal Examination
An isolated deep pocket may indicate a root fracture46

Selective Anesthesia
• May help to identify the possible
source of pain
• Ability to anesthetize a single tooth
has been questioned
47

∗ Initiation of cavity preparation without anesthesia
∗ Test of last resort
Test Cavity
48

∗ Helps to identify vertical crown fracture
∗ Produces light and dark shadows at fracture site
Transillumination
49

Transillumination
A crack will block and reflect the light when transilluminated
50

∗ Hyperocclusion – a possible cause of percussion sensitivity
Occlusion
51

∗ Analyze the data gathered via:
∗ History
∗ Examination
∗ Special tests
∗ Arrive at a clinical (not histologic) diagnosis:
∗ Pulpal diagnosis
∗ Periapical diagnosis
Analysis
52

• Normal
• Reversible pulpitis
• Irreversible pulpitis
• Necrosis
• Previous endodontic treatment
Possible Pulpal Diagnoses
53

Normal Pulp
∗ Symptoms None
∗ Radiograph No periapical change
∗ Pulp tests Responds normally
∗ Periapical tests Not tender to percussion or palpation
54

Reversible Pulpitis
∗ Symptoms May have thermal sensitivity
∗ Radiograph No periapical change
∗ Pulp tests Responds – sensitivity not lingering
∗ Periapical tests Not tender to percussion or palpation
55

Irreversible Pulpitis
• Symptoms May have spontaneous pain
• Radiograph No periapical change
• Pulp Tests Pain that lingers
• Periapical tests Generally not tender to Percussion or palpation
56
Necrotic Pulp
∗ Symptoms No thermal sensitivity
∗ Radiograph Dependent on periapical status
∗ Pulp tests No response
∗ Periapical tests Dependent on Periapical status
57

• Normal
• Acute apical periodontitis
• Chronic apical periodontitis
• Chronic apical periodontitis with symptoms
• Acute apical abscess
• Chronic apical abscess
• Condensing osteitis
Possible Periapical Diagnoses
58

Normal Periapex
∗ Symptoms None
∗ Radiograph No periapical change
∗ Pulp tests Responds normally
∗ Periapical tests Not tender to percussion or palpation
59

Acute Apical Periodontitis
∗ Symptoms Pain on pressure
∗ Radiograph No periapical change
∗ Pulp tests +/- depending on pulp status
∗ Periapical tests Tender to percussion and/or palpation
High restorations, traumatic occlusion, orthodontic treatment, cracked teeth, vertical root fractures, periodontal disease and maxillary sinusitis may also produce this response
60

Chronic Apical Periodontitis
∗ Symptoms None
∗ Radiograph Periapical radiolucency
∗ Pulp tests No response
∗ Periapical tests Not tender to percussion or palpation
61

• Symptoms Pain on pressure
• Radiograph Periapical radiolucency
• Pulp tests No response
• Periapical tests Tender to percussion and/or palpation
Chronic Apical Periodontitis with symptoms
62

Acute Apical Abscess
∗ Symptoms Swelling and severe pain
∗ Radiograph +/- periapical radiolucency
∗ Pulp tests No response
∗ Periapical tests Tender to percussion and palpation
63

Chronic apical abscess
∗ Symptoms Draining sinus – usually no pain
∗ Radiograph Periapical radiolucency
∗ Pulp tests No response
∗ Periapical tests Not tender to percussion or palpation
64

Condensing Osteitis
∗ Symptoms Variable
∗ Radiograph Increased bone density
∗ Pulp tests Dependent on pulp status
∗ Periapical tests +/- tenderness to percussion and palpation
65

• Treatment decisions are based on:
▫ Pulpal diagnosis
▫ Periapical diagnosis
▫ Restorability of tooth
▫ Periodontal considerations
▫ Difficulty of case
▫ Financial considerations
Treatment Planning
66

Two major decisions:
• Is root canal therapy indicated?
• Should I carry out this treatment myself or should I refer
the case?
Treatment Planning
67

• Patient considerations
• Objective clinical findings
• Additional conditions
Factors that add risk to Endodontic Cases
68

∗ Medical history
∗ Local anesthetic considerations
∗ Personal factors and general considerations
Patient Considerations
69

• Diagnosis
• Radiographic findings
• Pulpal space
• Root morphology
• Apical morphology
• Malpositioned teeth
Objective Clinical Findings
70

• Restorability
• Existing restoration
• Fractured tooth
• Resorptions
• Endo-perio lesions
• Trauma
• Previous endodontic treatment
• Perforations
Additional Conditions
71

• Rate the risk presented by each factor as:
▫ Average – 1
▫ High – 2
▫ Extreme – 3
• A case with all average ratings should be fairly straightforward
AAE Case Difficulty Assessment Form
72

AAE Case Difficulty Assessment Form
73

∗ If one or more factors present high or extreme risk, one must plan how to manage this extra risk prior to initiating treatment
AAE Case Difficulty Assessment Form
74

75

76

77