Embed Size (px)
Citation preview

IEEE Transactions on Nuclear Science, Vol. NS-29, No. 3, June 1982
IN VIVO DEFECTION OF THROMBI WITH INDIUM-lll-LABFTLED PLATELETS
David C. Price, Martin J. Lipton, Robert J. Lusby, Barry L. Engelstad,Ronald J. Stoney, Robert J. Prager, James A. Hartmeyer and Anne S. Holly
University of California School of MedicineSan Francisco, California 94143
SUMMARY
The use of Indium-ll-oxine labeled autologousplatelets has been explored in a dog-catheter model,as well as in a variety of clinical disorders in man.Newly forming experimental thrombi in dogs label wellduring the first 45-90 minutes, then lose both labeland thrombus mass in a manner consistent with fibrino-lysis. Thrcmbus weight is linearly related to In-lllactivity, so that in vivo scintigraphy will be a prac-tical method to evaluate various thrambotic stimuliand anti-thrombotic interventions experimentally.Preformed thrombus, however, labels poorly and cannotbe detected by imaging in this dog model. Initialclinical experience with a variety of arterial, venousand cardiac thrambotic states is reviewed, indicatingsome of the strengths and same of the potential weak-nesses of this new scintigraphic technique.
INTRODUCTION
Arteriosclerosis and Thrombosis
Almost all of the clinical complications of arter-iosclerosis leading to patient morbidity and mortalityinvolve intra-arterial thrombosis1,2 Thus, an ather-amatous plaque which thickens and then ruptures willpredispose to local platelet deposition and thrombusformation, ultimately becoming manifest by vessel occ-lusion and tissue infarction (myocardial infarction,stroke, etc.), or the breaking off of lesser pieces ofthrambus to produce emboli and consequent transientor permanent distal organ effects (transient ischemicattacks, recurrent minor strokes, etc.). Even theprocess of aneurysm formation which may ultimatelyresult in arterial rupture and hemorrhage is custom-arily accompanied by varying amounts of thrombosis inthe enlarging, irregular lumen of the affected artery.
Since cardiovascular and cerebrovascular diseasetogether account for approximately 47% of deaths in theadult American population (National Center for HealthStatistics, 1977), it would be of great value to haveavailable a non-invasive diagnostic test for the pres-ence and extent of in vivo thrcmbosis associated withthe degenerative vascular changes of arteriosclerosis.Other potential uses for in vivo thromboscintigraphywould inclide the detection of cardiac mural thrambi,which often result from previous myocardial infarcts,and/or aneurysms; the valvular lesions of subacutebacterial endocarditis which may also result in arter-ial emboli; the emboli and thrombi frequently associa-ted with prosthetic cardiac valves and prosthetic art-erial bypass grafts; and the venous thromboembolismarising fram deep venous thrombosis and frequentlyresulting in pulmonary emboli.
Indium-lll-Labeled Platelets
Attempts in the past to label and image thrombiin vivo have met with minimal success. Radioiodinatedfibrinogen, which converts to fibrin and is activelyincorporated into new thrambi, is catlmercially availa-ble only as Iodine-125-fibrinogen. Its use is restri-cted to the evaluation of superficial vessels becauseof the low energy of the I-125 gamna rays (35 keV) andthe characteristic x-rays of Tellurium (27 keV) emittedduring I-125 decay. In addition, energies this low
preclude effective imageability with the standardAnger scintillation camera. Although I-123-fibrinogenhas been explored as an imageable alternative,3 it isavailable only in certain research centers able tosynthesize the radiopharmaceutical, and is signific-antly limited in clinical utility by the 13 hour half-life of I-123.
The use of radiolabeled platelets for thrombuslocalization has been limited in the past by thetracers in established use. Chrcmium-51 attaches toplatelet proteins and does not appear to leave theplatelet significantly during its life span. For thisreason, much has been learned about the physiology andpathophysiology of platelet survival and thrombus for-mation in a variety of clinical conditions. However,the high energy gamma omission of Cr-51 (320 keV) issuboptimal for scintillation camera imging, and thelow isotope dose custonarily used along with a 9% abun-dance of the emitted gamna ray have all combined tomake in vivo imaging impractical. The other occasionalplatelet tracer in use, diisofluorophosphonate-P-32,is a beta emitter and therefore of no value for imag-ing.
The recent availability of Indium-lll-oxine forphysiologic labeling of platelets has opened up awhole new realm of in vivo platelet scintigraphy. Incontrast to Cr-51, In-lll has a short half-life of 2.8days as well as 183 imageable gamma emissions per 100disintegrations at energies of 173 and 247 keV, muchbetter suited to scintillation camera scintigraphy thanthe 320 keV Cr-51 garmma ray. McAfee and Thakur firstdemonstrated in 19764 that 8-hydroxyquinoline (oxine)could be used effectively as a lipophilic carrier tochelate In-lll and deliver it intracellularly intogranulocytes for physiological studies. The techniqueof labeling platelets with In-lll-oxine has then beenfurther refined by Thakur et al,5 Scheffel, McIntyreet al,6'7 Goodwin et al,8 and Heaton, Davis, Welch eta19 to the point where In-lll-oxine-labeled plateletsare now in routine use in a number of centers. Incre-asing experimental and clinical experience is now beg-inning to identify clinical thrombotic states in whichIn-lll-platelet scintigraphy is likely to prove of val-uable diagnostic benefit.
Our own initial experience with In-lll-plateletscintigraphy has been in a dog-catheter model whichhas allowed delineation of many of the factors influ-encing thrcmbus imageability. Scae of this work hasalready been published.10 More recently we have ext-ended the studies to a variety of clinical situationswhich will be illustrated.
METHODS
In-lll-Oxine Platelet Labeling
Platelet studies have been carried out to date inmore than 100 mongrel dogs, and in 45 adult humanshaving a variety of suspected or documented thrambo-tic disorders. These include recent myocardial infarc-tion with or without emboli, recent carotid endartere-ctcMY, thranbophlebitis with pulmonary omboli, etc..
Autologous platelets are separated from 45 cc of
0018-9499/82/0600-1191$00.75 41982 IEEE 1 191
blood by differential centrifugation and labeled withIn-lll-oxine in plasma or in ACD-saline by the tech-nique of Thakur et a15 as modified by Scheffel6 andHeaton9 for optimal platelet function and survival.In-lll-oxine is either purchased carmercially (Medi +Physics), or the In-lll is complexed to oxine in ourown laboratory using In-lll chloride and freshly sol-ubilized 8-hydroxyquinoline. The injected In-lll-platelet dose has varied fram 50-3001iCi. In all ani-mals and human studies, platelet survival is estima-ted fran daily whole blood samples, frequently withparallel samples centrifuged to separate and countthe platelet button.
Animal and Clinical Studies
Autologous canine platelets have been labeledand injected at various times before and after arter-ial angiographic catheter insertion. For predictablethrcnbus formation, a 5 ff polyethylene angiographiccatheter is introduced into a femoral artery and adv-anced under fluoroscopic control into one carotid.Catheters have been left in place for periods rangingfram 30 minutes to 24 hours. As described below,labeled platelets have been injected at various timesbefore and after catheter insertion to study the dif-ferential labeling between newly forming as opposedto preformed thranbus. Scintigraphic images are 5-10minutes in duration, depending on the level of acti-vity involved. In most instances, a medium energycollimator is used, and a summation image of bothIn-lll peaks is obtained. When only a single peak ispossible, the 173 keV peak is used. When a portablecamera must be used, the 173 keV peak with a high res-olution collimator gives excellent images. For quan-titative kinetic studies, 2-minute sequential imagesare stored in a DEC 11/10 or DEC 11/40 computer in a64 x 64 matrix, and region-of-interest curves arederived fran the stored data using standard Gamma-llsoftware. For standardization, a canputer-storedimage is also obtained of a calibrated In-lll sourcein a plexiglass phantam designed to simulate appropr-ate tissue absorption and scattering.
Clinical studies have been carried out similarly,with 5-15 minute double-peak images of the areas ofinterest, and usually a 24-hour whole body scan. Inthe human studies, imaging is continued daily for 72-96 hours whenever possible. Since the procedure isstill experimental, all studies are performed withinformed consent.
RESULTS
Animal Studies
Figure 1 illustrates a typical carotid catheterstudy, showing progressive In-lll-platelet uptake onthe catheter to a peak at 45-90 minutes, then decreasein catheter activity thereafter. The labeled plate-lets have been injected just prior to catheter inser-tion. Figure 2 is the caTputer-processed region-of-interest curve fram a similar study, demonstratingquantitatively a peak at 45 minutes with progressivefall-off thereafter.
Since the thrambosis associated with arterioscl-erosis derives fram subendothelial collagen exposurefollowing endothelial damage and denudation, in sev-
eral dogs a balloon catheter was introduced into afemoral artery, blown up, and pulled along the proxi-mal fenoral artery to create a specific area of denud-ed endothelium. This also demonstrated a distinctlypositive region of labeled platelet localization (Fig-ure 3, 4) having a kinetic pattern similar to theintra-arterial polyethylene angiographic catheters.Thus, the dog model has proved to be applicable both
to foreign surface thranbus induction and to the thro-mbosis of endothelial damage in a quantitatable manner.
In-ill-Platelet Correlation with Newly Forming ThranbusIn 24 dogs, the carotid catheter was introduced
shortly after labeled platelet injection, then wasexcised at varying times up to three hours later tosee if the late loss of In-lll activity in Figure 2was the result of thranbus dissolution or tracer lossfran the thronbus due to platelet lysis. It is wellknown in veterinarian hematology that the dog has aparticularly active and easily activated fibrinolyticsystem, so that the former postulate seemed more like-ly. This in fact proved true, as seen in Figure 5,indicating that thrcnbus mass showed the same patternof 45-90 minute peak and subsequent fall-off as didthe In-lll activity. In fact, correlation betweenthronbus weight and In-lll was quite good (Figure 6),indicating that at least for newly forming thracbus,the in vivo In-lll-platelet method is an accurate indi-cator of thranbus size.
In-lll-Platelet Correlation with Preformed ThronbusIn almost all clinical situations of medical imp-
ortance, the patient presents with preformed thrcnbusalready in existence and producing clinical manifesta-tions. Thus, it would be essential to know if prefor-med thranbus has the same ability to concentrate radi-olabeled platelets as does newly forming thrambus.This would seem unlikely, as continuing thranbus grow-th occurs only at the surface of existing thrombus,and therefore In-lll-platelet uptake is likely toreflect only minor surface exchange. A series of exp-eriments was carried out in which the carotid catheterwas left in place for 2 or 24 hours prior to In-lll-platelet injection, and the catheter was excised after1 hour of imaging to determine peak clot weight andIn-lll activity. As indicated in Table I, there was asignificant drop in thranbus weight at 2 hours whichrecovered by 24 hours. In-lll-platelet uptake fellprogressively at the 2 and 24 hour times, and in noinstances were these catheters visualizable by scinti-graphy. Thus, these studies document that preformedthranbus has much less labeled platelet uptake thannewly forming thranbus, resulting in camplete loss ofimageability, a fact that will represent a great disad-vantage in trying to utilize the imaging techniqueclinically.
In phantam studies, we have found that an In-111point source in simulated tissue background must be atleast 0.2-0.3 pCi in the carotid location to be detect-able by scintigraphy. For a thrcnbus of significantmass (i.e. larger than a point source), this minimumimageable tracer will need to be even greater in magni-tude, as will also be true for deeper locations. Sincethe human tracer dose is limited to approximately 300pCi of In-lll to keep spleen radiation dose below 8rads, a minimum of 0.1% of the circulating plateletmass will have to deposit in a thranbus to be visuali-zed, approximately 1.5 x 106 platelets.
CLINICAL STUDIES
Normals
Figure 7 illustrates the whole body distributionof In-lll-platelets in a normal adult. Of irmportanceis the fact that there is considerable splenic poolingand a lesser degree of hepatic pooling, with cardiacand major vessel outlines also evident. Normal plate-let disappearance half-time, calculated by least squ-ares fit of a single exponential plot fran whole bloodactivity, is greater than 100 hours.
1192
Arterial Thrambosis
Figure 8 illustrates positive labeling in theabdominal aorta of a young man with embryonal cellcarcinama of the testis, presenting with retroperito-neal metastases which had grown through the aorticwall and had caused intra-aortic thrambosis, At sur-gery, a large clot was removed which contained 3.51Ci In-lll.
Figure 9 illustrates positive labeling at thefemoral artery insertion site of an angiographic cath-eter from recent catheterization. Although there isprominent platelet deposition at the insertion site,the vessel remained patent, and no evidence of distalemboli was noted in that extremity.
Arteriosclerosis and Carotid Endarterectamy
Carotid endarterectamy is a frequent surgicalprocedure carried out to open the narrowed carotidlumen frequently found in older patients with carotidarteriosclerosis. Since collagen in the subendothe-lial layers is a known initiator of platelet adhesionand thrombus formation, it would be reasonable toexpect to visualize labeled platelet deposition insuch patients. Whether active platelet uptake wouldbe a brief phencmenon or one lasting several days orweeks is not presently known. An additional potentialapplication of In-lll-platelet scintigraphy in suchpatients might be to identify those patients at highrisk for excessive carotid thrombus formation result-ing in occlusion or embolization, perl-ps identifiableby abnormally increased platelet deposition.
To date we have studied 11 patients injected withIn-lll-platelets 1-2 hours after completion of carotidendarterectcmy (Table 2). All patients have demon-strated positive labeling of the endarterectamizedcarotid (Figure 10), varying rather widely in theintensity of labeling. Thus, early platelet deposi-tion is a substantial part of the initial healingprocess in such a de-endothelialized carotid. In 3patients the opposite carotid had been operated onone week before, and none of these patients showed apositive image on that side (Table 2, Figure 11).This would suggest that the period of active plateletdeposition is short, certainly less than one week.Of the 6 opposite carotids which had significant art-eriosclerotic disease, none of the lesions were visu-alizable by scintigraphy (Table 2, Figure 12). Theselatter results are in contradiction to the publishedexperience of Davis et alll who found In-lll plateletsto have a 61% sensitivity for detecting carotid arter-iosclerosis. Clearly, small lesions will be more dif-ficult to identify than large ones, and new lesionsactively accumulating platelets will be more readilydetected than old thrambi or re-endothelialized les-ions which are thronbogenically quiescent.
Cardiac Mural Thrombi
One important camplication of myocardial infarc-tion is that the damaged ventricular wall may predis-pose to intraventricular mural thraonbus formation,thus leading to risk of arterial embolization (tobrain, kidneys, etc.). Such mural thrombi may alsooccur in ventricular aneurysms which generally origi-nate from prior myocardial infarcts. Ultrasound hasproven only moderately sensitive in identifying suchthrcmbi (Ezekowitz et al'2) and the utility of cardiacCr scanning is still being explored. In two recentlypublished studies with In-lll-platelets, Ezekowitz etaI12 and Stratton et a113 have reported an accumulatedexperience in 27 patients with left ventricular thrmn-bi and 46 patients without. The sensitivity of thetechnique was 67%, with a specificity of 98%, suggest-
ing that In-lll-platelets will be extremely helpfulin evaluation for mural thrombi. In spite of thisencouraging experience, we have to date failed todentify any of the first three left ventricular thro-mbi so far available for study. Once again, consider-able further experience fram several laboratories willbe essential.
Venous Thrombosis
Our experience with venous thrombosis to date hasbeen quite limited. In 2 patients with recent pulmon-ary emboli, thoracic imaging was negative, althoughboth patients were receiving heparin. In one of thepatients in wham deep pelvic veins were suspected tobe the source of emboli, the In-lll-platelet studyin fact demonstrated a strikingly positive left basil-ic vein with normal lower extremities (Figure 13).The patient was undergoing chronic renal dialysis,and had a thrombosed arterio-venous shunt as well asa functioning shunt-in the left arm.
Renal Transplantation
Microscopic thrombosis and hemorrhage is a prom-inent microvascular feature of acute renal transplantrejection. We have studied 4 renal transplants todate, and have seen significant In-lll-platelet dep-osition in all 3 patients undergoing acute rejection(Figure 14). Since the finding is scmewhat predict-able, it remains to be seen whether a clinically use-ful application of the observation can be established.Others have similarly described renal transplant lab-eling during acute rejection.14
CONCLUSION
The recent availability of In-lll-platelet label-ing, using 8-hydroxyquinoline (oxine) as the isotopiccarrier, has initiated considerable interest in a widevariety of potential diagnostic applications in man.Since most of the medical presentations of arterio-sclerosis relate to thrombus formation with vascularocclusion or embolization, it is likely that this newimaging technique will have significant impact on car-diovascular and cerebrovascular morbidity as well asmortality. The necessity for continuing active plate-let deposition for thrcmbus imageability will, however,impose distinct limitations as to which thromboticconditions will be detectable in vivo. Increasingclinical experience over the next several years willdetermine the ultimate place of In-lll-platelet thro-mboscintigraphy as a routine procedure amongst thebattery of diagnostic procedures presently available.
ACKNCWLEDGEMENTS
Tfhis work has been supported in part by the Nat-ional Heart, Lung and Blood Institute of the PublicHealth Service (Grant Number R01 HL 23414) as well asthe Louis R. Lurie Foundation and the American HeartAssociation (California Affiliate). Dr. Lipton issupported by a Research Career Development AwardNumber 5 K04 - HL 00360.
REFERENCES
1. Kinlough-Rathbone RL and Mustard JF: Atherosclero-sis. Current Concepts. An J Surg 141:638-643,1981.
2. Fuster V and Chesebro JH: Antithranbotic Therapy:Role of Platelet-Inhibitor Drugs. 1. CurrentConcepts of Thranbogenesis: Role of Platelets.Mayo Clin Proc 56:102-112, 1981.
3. DeNardo SJ and DeNardo GL: Iodine-123-FibrinogenScintigraphy. Sem Nuc Med 7:245-251, 1977.
1193
4. McAfee JG and Thakur ML: Survey of RadioactiveAgents for In Vitro Labeling of Phagocytic Leu-kocytes. 1. Soluble Agents. J Nuc Med 17:480-487, 1976.
5. Thakur ML, Welch MJ, Joist JH and Colenan RE:Indium-ill Labeled Platelets: Studies on Prepa-ration and Evaluation of In Vitro and In VivoFunctions. Thran Res 9:345-357, 1976.
6. Scheffel U, McIntyre PA, Evatt B, Dvornicky JAJr, Natarajan TK, Bolling DR and Murphy EA:Evaluation of Indium-lll as a New High PhotonYield Gamna-Enitting "Physiological" PlateletLabel. The Johns Hcpkins Med J 140:285-293,1977.
7. Scheffel U, Tsan M-F and McIntyre PA: Labelingof Human Platelets with { 1 1In} 8-Hydroxyquino-line. J Nuc Med 20:524-531, 1979.
8. Goodwin DA, Bushberg JT, Doherty PW, Liptm MJ,Conley FK, Diamanti CI and Meares CF: Indium-111-Labeled Autologous Platelets for Location ofVascular Thrcmbi in Humans. J Nucl Med 19:626-634, 1978.
9. Heaton WA, Davis HH, Welch MJ, Mathias CJ, JoistJH, Sherman IA and Siegel BA: Indium-ill: ANew Radionuclide Label for Studying Human Plate-let Kinetics. Brit J Haenatol 42:613-622, 1979.
10. Price DC, Hartneyer JA, Prager r and Lipton MJ:Evaluation of In Vivo Thranbus Formation in DogsUsing Indium-lll-Oxine-Labeled Autologous Platel-ets. In Indium-lll Labeled Neutrophils, Platelets,and Lyrphocytes. Thakur ML and Gottschalk A eds.Trivir Publishing Ccnpany, New York, 1980, ppl83-186.
11. Davis HH, Siegel BA, Sherman IA, Heaton WA,Naidich TIP, Joist JH and Welch mJ: ScintigraphicDetection of Carotid Atherosclerosis with Indium-111-Labeled Autologous Platelets. Circulation61:982-988, 1980.
12. Ezekewitz MD, Ieonard JC, Snith EO, Allen EW andTaylor FB: Identification of Left VentricularThrarbi in Man Using Indium-lll-Labeled Autolog-ous Platelets. A Preliminary Report. Circula-tion 63:803-810, 1981.
13. Stratton JR, Ritchie JL, Hamilton GW, Ha ermeis-ter KE and Harker IA: Left Ventricular Thranbi:In Vivo Detection by Indium-lll Platelet Imagingand Two Dimensional Echocardiography. Am JCardiol 47:874-881, 1981.
14. Kolbe H, Sinzinger H, Angelburger P and LeithnerCH: Frueherkennung von Abstossungs reaktionenmit 1 1Indium-Oxin Markierten Thranbozyten-Radiol Diagn 21:821-824, 1980.
ABIE 1
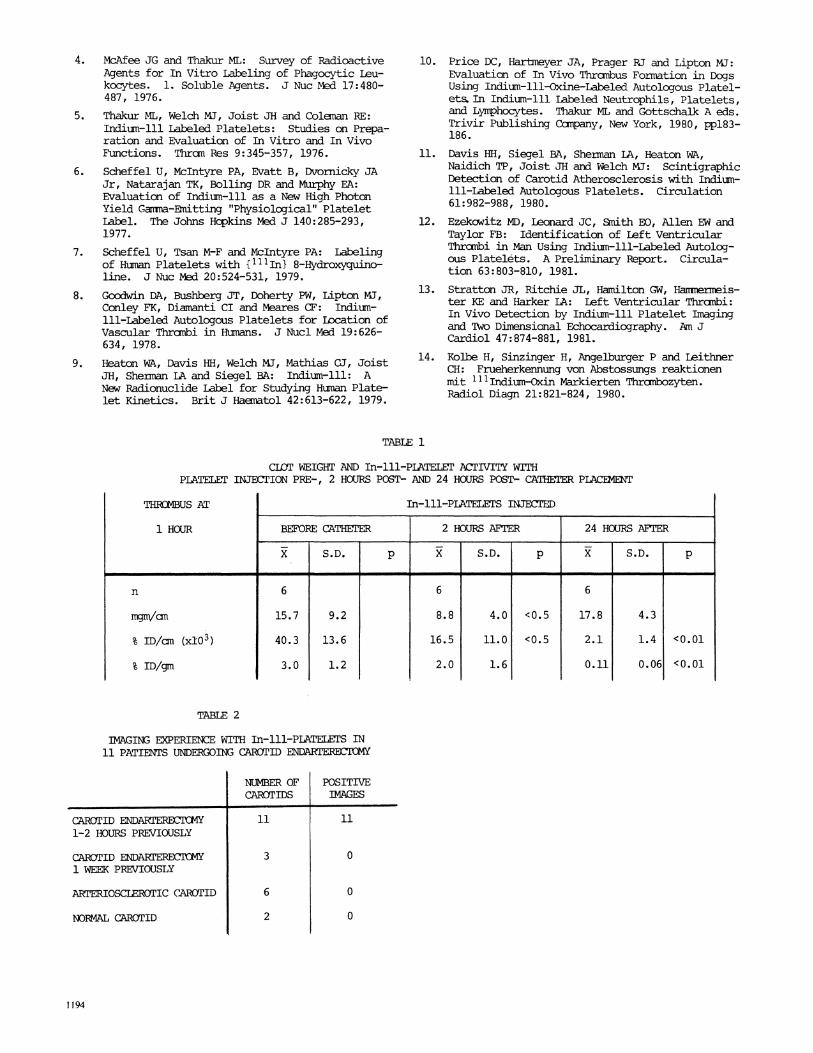
CLOT WEIGHT AND In-ill-PIATELET ACTITY WITHPLATEL INTEBCION PRE-, 2 HOURS POST- AND 24 HOURS POST- CATHEER PLACEMENT
THROMBUS AT
1 HOUR
n
mmanVa
% ID/cm (x10 3)
% ID/gm
In-111-PLATELETS INJECTE
BEFORE CATHETER 2 HOURS AFTER 24 HOURS AFTER, ,I Igl
S.D. p S.D. p
I - I , - I- -I
6
15.7
40.3
3.0
9.2
13.6
1.2
6
8.8
16.5
2.0
4.0
11.0
1.6
<0.5
<0.5
TABLE 2
IMGING EXPERIENCE WITH In-lll-PlATELETS IN11 PATIENTS UNDERGOING CAROTID ENDARTERB2CTY
CAROTID ENDARTERECTCMY1-2 HOURS PREVIOUSLY
CAROTID ENDAIPERECICM1 WEEK PREVIO(JSLY
ARTERIOSCLEROTIC CAROTID
NORMAL CAROTID
NUMBER OFCAROTIDS
I11
3
6
2
1194
S.D. p
6
17.8
2.1
0.11
4.3
1.4
0.06
<0.01
<0.01
POSITIVEIMAGES
11
0
0
0
DAMAGWD INDOTHELIUM
~~~~~~-.
30 60 90 120 150 9a0 2 0
MINUTES
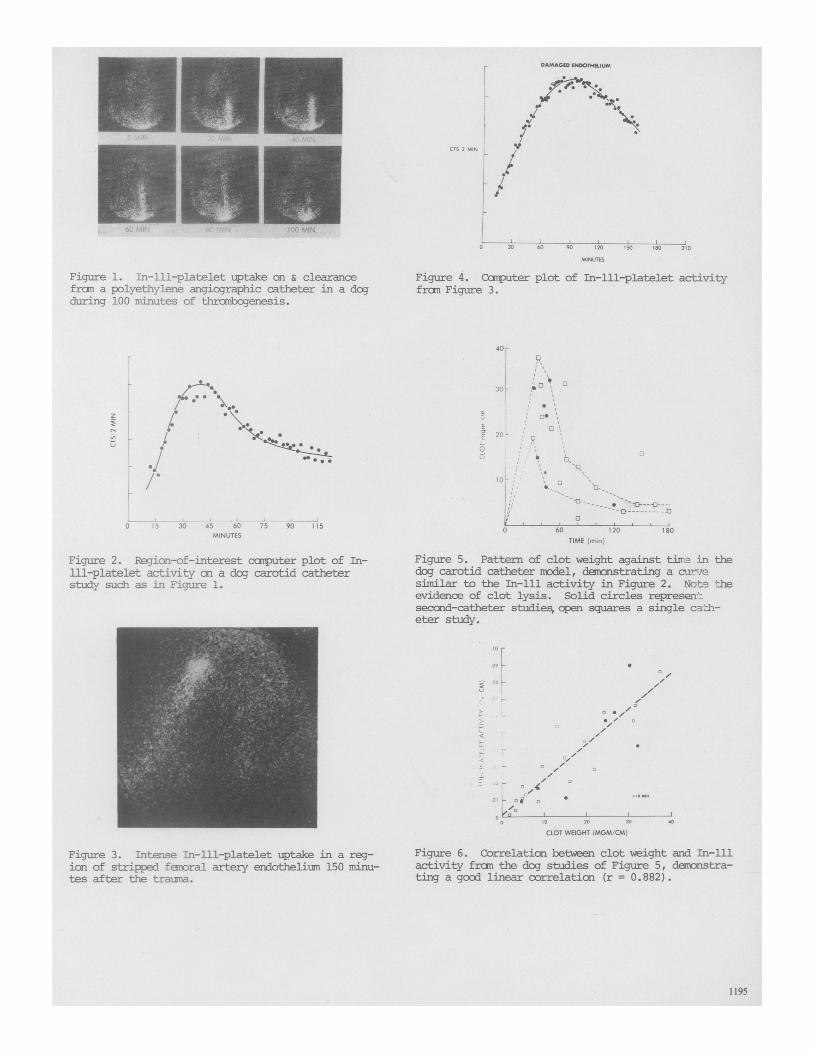
Figure 1. In-lll-platelet uptake an & clearancefran a polyethylene angiographic catheter in a dogduring 100 minutes of thranbogenesis.
I
bf;
30 45 60 75 90 115MINUTES
Figure 2. Region-of-interest carputer plot of In-ill-platelet activity an a dog carotid catheterstudy such as in Figure 1.
Figure 4. Coiputer plot of In-lll-platelet activityfran Figure 3.
40F
30 o III
E ,I 0
320 - o
U
a20o; io
E
0 60 120 180TIME (min)
Figure 5. Pattern of clot weight against tixro in thedog carotid catheter model, demanstrating a cuaresimilar to the In-lll activity in Figure 2. Note theevidenoe of clot lysis. Solid circles represen-secand-catheter studies,coen squares a single ca.h-eter study.
0 r
09
I0 20 30
CLOT WEIGHT (MGM/CM)
Figure 3. Intense In-lll-platelet uptake in a reg-ian of stripped femoral artery endothelium 150 minu-tes after the trauma.
Figure 6. Correlatian between clot weight and In-lllactivity from the dog studies of Figure 5, demonstra-ting a good linear correlaticn (r = 0.882).
1195
CTS 2 MIl
z
j_iI
L0o 1 5
11
. .'/41,
. .1 .
uk
. o "2
o
0
0
,ir .
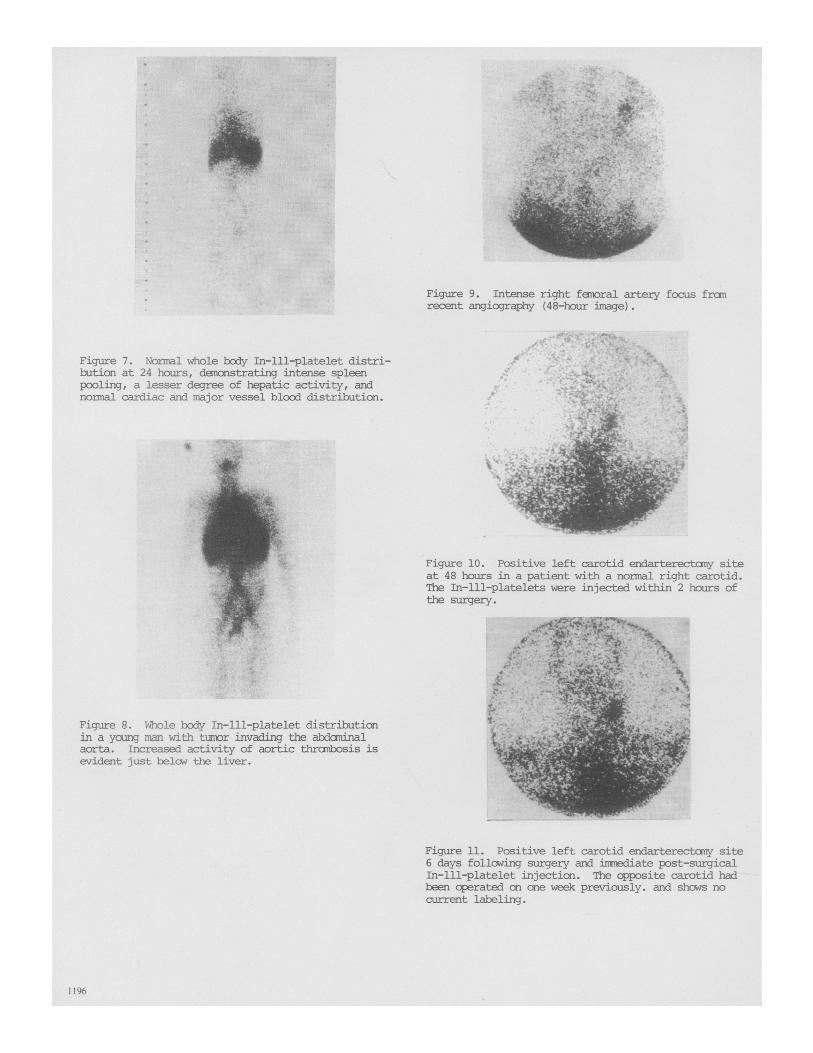
Figure 9. Intense right femoral artery focus franrecent angiography (48-hour image).
Figure 7. Normal whole bcdy In-1ll-platelet distri-bution at 24 hours, demonstrating intense spleenpooling, a lesser degree of hepatic activity, andnonnal cardiac and major vessel blood distribution.
Figure 10. Positive left carotid endarterectamy siteat 48 hours in a patient with a normal right carotid.The In-1ll-platelets were injected within 2 hours ofthe surgery.
Figure 8. Whole body In-ll-platelet distributimnin a young man with tunmr invading the abdominalaorta. Increased activity of aortic thrombosis isevident just below the liver.
Figure 11. Positive left carotid endarterectnomy site6 days following surgery and immediate post-surgicalIn-lll-platelet injection. The cpposite carotid hadbeen operated on one week previously. and shows nocurrent labeling.
1196
r
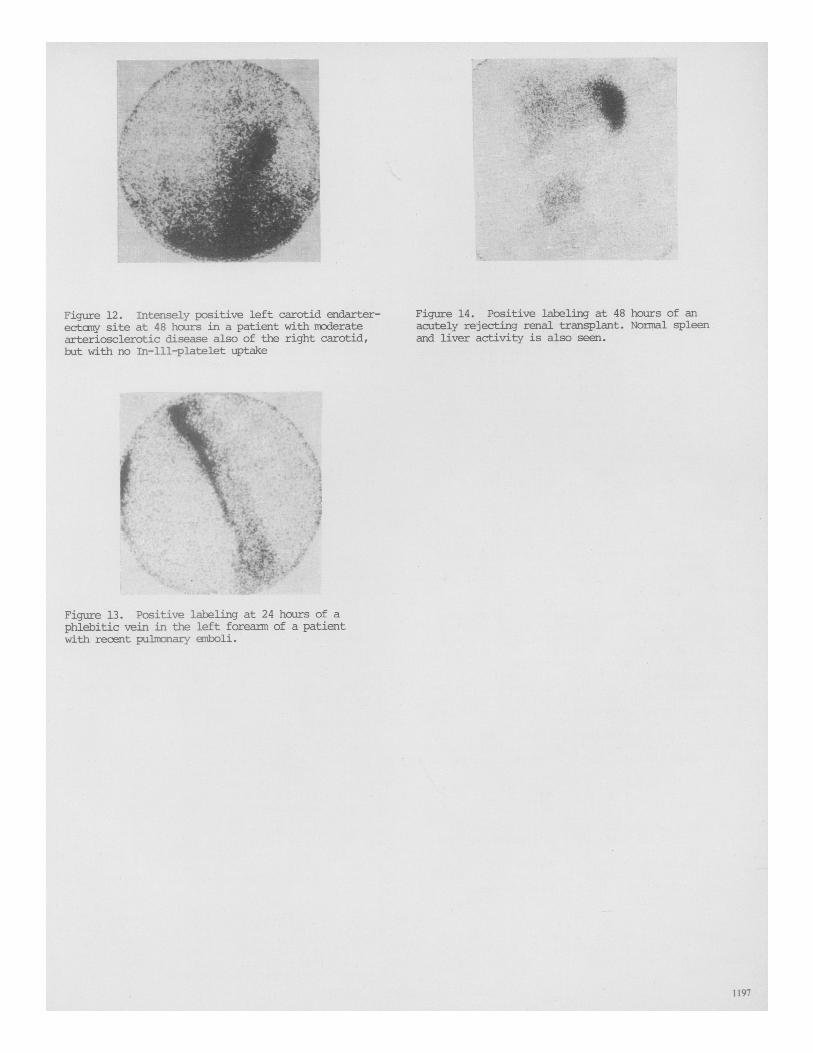
Figure 12. Intensely positive left carotid endarter-ectcmy site at 48 hours in a patient with moderatearteriosclerotic disease also of the right carotid,but with no In-lll-platelet uptake
Figure 14. Positive labeling at 48 hours of anacutely rejecting renal transplant. Normal spleenand liver activity is also seen.
- ,i ,f,&4 .\;
; . ,4;.F .. sb, ,, x >_h & S UD nz;.:'S,'t.^.;''s' @6X. C:*
WE'S nNJ. 00NEw Ai: 4 Say AVet,+0C3S^ a 4*CllX--;0: <+tvaft E
w > ; .'-.SEWS,. q. iVS ! >'0+ X t vti 0
i.;1 E L:Vs.E aD1-
t ! st '$ S.t\^s. 3 FDiA -s ;.^ X^,, W:; 1E' >V;S !.r. tv
Figure 13. Positive labeling at 24 hours of aphlebitic vein in the left forearm of a patientwith recent pulnmnary emboli.
1197
7)",,4 I





























