Embed Size (px)
Citation preview
8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 1/17
Review Article
In vivo reectance-mode confocal microscopy in
clinical dermatology and cosmetology
S. Gonza lez*, and Y. Gilaberte-Calzada*Dermatology Service, Memorial Sloan Kettering Cancer Center, New York, NY, USA, Grupo Dermatologico, Madridand Dermatology Service, Hospital San Jorge, Av. Martı ´nez de Velasco 34, 22005 Huesca, Spain
Received 13 May 2007, Accepted 14 July 2007
Keywords: dermatology, cosmetology, in vivo confocal microscopy, non-invasive skin pathology
Synopsis
In vivo reectance confocal microscopy (RCM) is anon-invasive imaging tool that allows real-timevisualization of cells and structures in living skinwith near histological resolution. RCM has beenused for the assessment of benign and malignantlesions, showing great potential for applications inbasic skin research and clinical dermatology. RCMalso reveals dynamic changes in the skin over timeand in response to specic stimuli, like ultraviolet
exposure, which makes it a promising tool in cos-metology, as it allows repetitive sampling withoutbiopsy collection, causing no further damage tothe areas under investigation. This review summa-rizes the latest advances in RCM, and its applica-tions in the characterization of both normal andpathological skin.
Re sume ´
La microscopie confoncale en re ´ectance (RCM) estun outil de visualization non-invasif qui permetl’observation en temps re ´el des cellules et structuresde la peau vivante avec une re ´solution pratique-ment histologique. La RCM a e ´te utilise e pourl’observation des le´sions be nignes et malignes et amontre´ un fort potentiel pour les applications des
domaines de la recherche cutane ´e de base et en der-matologie clinique. La RMC est e ´galement capablede montrer des variations dynamiques dans la peauen fonction du temps et en re ´ponse a des stimulispeciques comme une exposition aux ultra-violets.Ceci fait de cette me thode un outil prometteur encosme tologie permettant des mesures re ´petitivessans pre levements de biopsies, c’est-a`-dire sansprovoquer de dommages aux zones de la peauetudie es. Cet article re sume les dernie`res avance´esconcernant le RCM et ses applications dans la
caracte´risation de la peau saine et pathologique.
Introduction
The ability to evaluate a skin lesion microscopi-cally in a non-invasive fashion has long been agoal for dermatologists and dermatopathologists.In the last several years, several techniques havebeen developed aimed to provide dynamic micro-scopic information about the skin to offer in vivodiagnosis and monitoring of disease evolution inreal time without morbidity. These technologiesinclude magnetic resonance [1], high frequency-ultrasonography [2], optical coherent tomography[3] and, more recently, reectance confocalmicroscopy (RCM) [4, 5].
Currently, i n vivo RCM has a wide range of applications, allowing real time non-invasivemicroscopic imaging with a resolution near that of conventional histology (1- l m lateral and 3- l maxial) when exploring cutaneous structuresbetween the stratum corneum and reticular dermis
Correspondence: Salvador Gonzalez, Dermatology Service,Memorial Sloan-Kettering Cancer Center, 160 East 53rdStreet, 2nd Floor, New York, NY 10022, USA.Tel.: +1 212 6100185; fax: +1 212 308 0530; e-mail:[email protected]
International Journal of Cosmetic Science , 2008, 30 , 1–17
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Socie ´te Francaise de Cosme´tologie 1

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 2/17
[6]. RCM is based on the collection of images fromlight reected by living tissue [7–10]. In 1995, Ra- jadhyaksha et al. [5] rst reported the foundationsof laser scanning RCM. Since then, improvementsin design and optimization of optical parameters
have improved image quality, reduced the size andimproved ergonomics of the imaging devices. Inrecent years, imaging techniques have improved,increasing the number of applications in dermatol-ogy, and a signicant number of skin conditionshave been objectively characterized.
Foundations of RCM
A confocal microscope consists of a light source, acondenser, an objective lens and a detector(Fig. 1). The light source illuminates a small three-dimensional spot within a sample, such as skin.This illuminated spot is then imaged onto thedetector through a small aperture (pinhole). The
small aperture allows only light that originatesfrom the focused illumination spot to be detected,whereas the light that originates away from thespot is reected [11]. The light source, the illumi-nated spot and the detection aperture are in opti-
cally conjugated focal locations and thisarrangement is called ‘confocal’. The illuminatedspot is then scanned horizontally over a 2-dimen-sional grid to obtain a horizontal microscopic sec-tion. This process is known as ‘optical sectioning’[7–10]. Adjustments can be made in the focallength of the beam, allowing the microscope toimage a series of horizontal planes stacked verti-cally, with and axial thickness of 2–5 l m(Table I). In this sense, the numerical aperture of the objective lens determines image resolution,which means that there is an inversely propor-tional relationship between high resolution imagesand small apertures (less light), and low resolutionthrough larger apertures (more light). Confocal
Out-of-focus plane
In-focus plane (object)
Out-of-focus plane
Pointlightsource
Condensderlens
Tissuesample
Objectivelens
Point detector–pinhole / aperuture
Figure 1 Diagram of a reectancemode confocal microscope. The dia-
gram depicts non-invasive imagingof a thin (focused) plane of skin.Back-scattered light is detected fromthe skin rather than transmitted lig-ht. The small aperture (pinhole) infront of the detector collects onlythe light in focus, while rejectinglight that is out of focus.
Table I Summary of basic principlesof reectance confocal microscopyand image interpretation
Wavelength of light source for 1- to 3- l msectioning in the epidermis
Visible 488–514 nm
3–5 l m in the deeper dermis Near-infrared 800–1064 nmObjective lens Magnication 30–100 ·
Numerical aperture 0.7–1.2Resolution Lateral 0.5–1.0 l mAxial 3.0–5.0 l mIllumination power up to 40 mWReal time confocal images are parallel to skin surfaceConfocal images of normal epidermis show honeycombed appearanceMelanin is the best endogenous contrast agent
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–172
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 3/17
images are obtained in greyscale. In this context,white represents total light reected and black rep-resents no reection at all. More light is reectedwhen the tissue contains structures of size similarto the wavelength of the light source [5, 6].
Reectance confocal microscopy systems use alaser as a light source. Best quality images areobtained with low power lasers (around 40 mW)and near-infrared wavelength (800–1064 nm).With an 830 nm diode laser, skin penetration isaround 400 l m [6]. Water immersion lenses areused as the refractive index of water (1.33) is closeto that of epidermis (1.34).
Skin movement may be a problem during in vivoimaging. To overcome this, a ring template skincontact device is used to reduce motion artefactsand to contain the immersion medium (water orultrasound gel) for the objective lens during imag-ing [6].
Basic principles for image interpreta-tion of the skin
Images obtained by RCM are en face (horizontal)images when compared with vertical sectionsobtained by routine histology. Whereas routinehistology requires tissue staining with exogenousdyes for diagnosis, confocal images are resolved ingreyscale. Confocal images are based on the pres-ence of ‘endogenous contrast’ [11], which is pro-
vided by microstructures such as melanin,haemoglobin or cellular organelles [5]. Therefore,structures are visualized based on the optical prop-erties such as the refraction index and the reec-tivity of the tissue under investigation [12, 13].
Epidermis
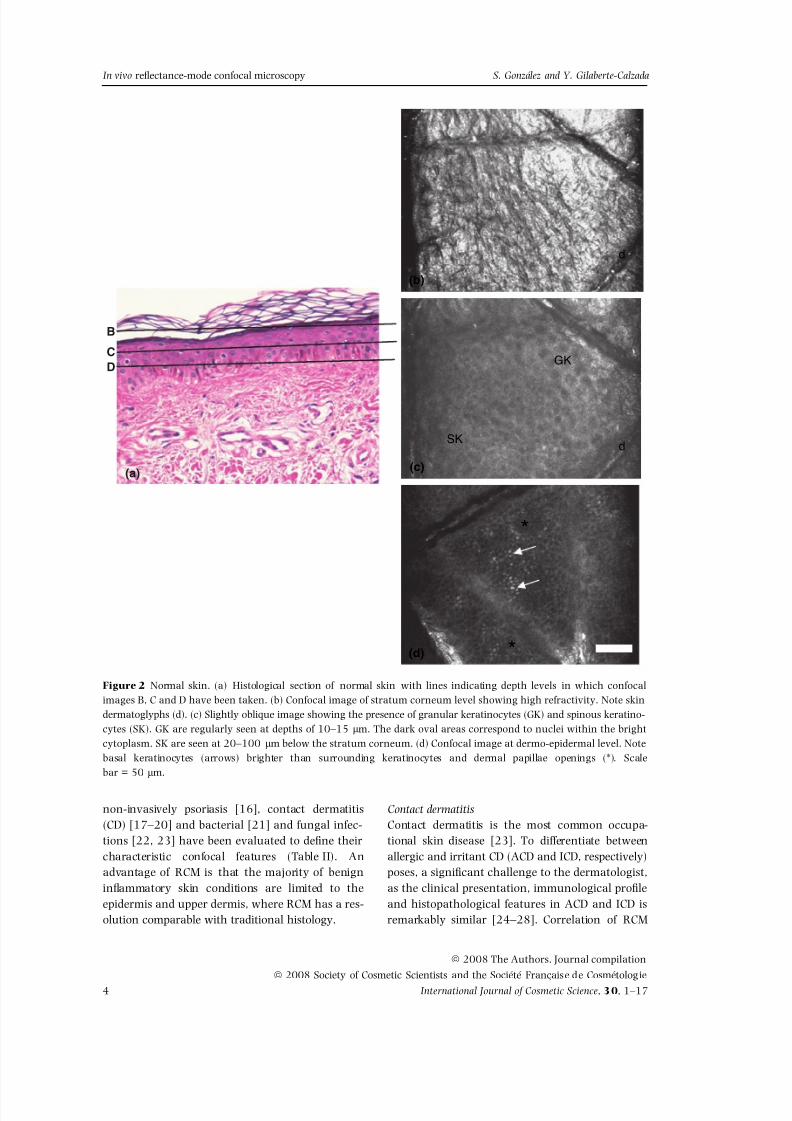
Imaging normal skin in real time usually takesplace from the surface and progressing deeper, thusmost supercial images correspond to the stratumcorneum (Fig. 2a). The stratum corneum producesthe rst image of the top surface of the skin becauseof backscattered light at the water-to-stratum cor-neum interface. Corneocytes are visualized as bril-liant polygonal shapes of 10- to 30- l m size, andgrouped in ‘islands’ separated by skin folds, whichappear very dark. The next layer (section) is thestratum granulosum, regularly distributed at adepth of 15–20 l m (Fig. 2b).The stratum granulo-sum keratinocytes are 20- to 25- l m size and theirnuclei show up as dark central oval structures sur-
rounded by a bright grainy cytoplasm. Underneaththe stratum corneum is the stratum spinosum,located 20- to 100- l m deep. It consists of a tight‘honeycomb pattern’ of keratinocytes (10- to 15- l msize) with well-demarcated cell borders (Fig. 2b).
Between 50- to 100- l m depth we can nd thedermo-epidermal junction. Basal keratinocytes aresmall (7–15 l m) and bright [6], due mostly to thepresence of melanin inside the cell (Fig. 2c). Themelanin in basal keratinocytes is typically arrangedin a supranuclear position, often referred to as ‘mel-anin caps’ or ‘umbrellas’, implying their protectivefunction. Melanocytes can be seen as bright, solitarynests at the dermo-epidermal junction, with round,oval, fusiform and dendritic shapes [14]. Differentbrightnesses correspond to endogenous variationamong skin phototypes and the anatomic location.Other cells that contain melanin are melanophageswhich can be distinguished in the supercial dermisas large, bright cells with ill-dened cytoplasmicborders, usually located around or near vessels.
Dermis
Dermal papillae are observed at the dermo-epider-mal junction as dark round areas surrounded byrings of bright circles of basal cells containinghighly reective melanin granules. Capillary loopsare located in the centre of dermal papillae asblack holes, often showing bright erythrocytes roll-
ing within them; based on their relative morpho-logies, sizes and numbers, these cells wereidentied as erythrocytes (6- to 9- l m diameter),leucocytes (6–30 l m) and platelets (2–5 l m).Below the dermo-epidermal junction, a network of collagen bres and bundles (1- l m and 5- to25- l m diameter, respectively) can be observedwithin the papillary dermis and supercial reticu-lar dermis. Eccrine ducts appear as bright centralhollow structures that spiral through the epidermisand dermis. Hair shafts with pilosebaceous unitscan be observed [6, 15], and appear as centralhollow structures with elliptical elongated cells atthe circumference, with a central white structurecorresponding to the hair shaft.
Use of RCM in clinical dermatology
RCM ndings of inammatory skin conditions
Reectance confocal microscopy has been used todescribe inammatory skin conditions in vivo and
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 3
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada
8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 4/17
non-invasively psoriasis [16], contact dermatitis(CD) [17–20] and bacterial [21] and fungal infec-tions [22, 23] have been evaluated to dene theircharacteristic confocal features (Table II). Anadvantage of RCM is that the majority of benigninammatory skin conditions are limited to theepidermis and upper dermis, where RCM has a res-olution comparable with traditional histology.
Contact dermatitisContact dermatitis is the most common occupa-tional skin disease [23]. To differentiate betweenallergic and irritant CD (ACD and ICD, respectively)poses, a signicant challenge to the dermatologist,as the clinical presentation, immunological proleand histopathological features in ACD and ICD isremarkably similar [24–28]. Correlation of RCM
B
CD
(c)
GK
SK d
(b)
d
(a)
(d) *
*
Figure 2 Normal skin. (a) Histological section of normal skin with lines indicating depth levels in which confocalimages B, C and D have been taken. (b) Confocal image of stratum corneum level showing high refractivity. Note skindermatoglyphs (d). (c) Slightly oblique image showing the presence of granular keratinocytes (GK) and spinous keratino-cytes (SK). GK are regularly seen at depths of 10–15 l m. The dark oval areas correspond to nuclei within the brightcytoplasm. SK are seen at 20–100 l m below the stratum corneum. (d) Confocal image at dermo-epidermal level. Notebasal keratinocytes (arrows) brighter than surrounding keratinocytes and dermal papillae openings (*). Scalebar = 50 l m.
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–174
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 5/17
with conventional histopathology has unveiled dis-tinctive characteristics for ACD and ICD [17, 18,20]. Spongiosis is noted as intercellular brightness
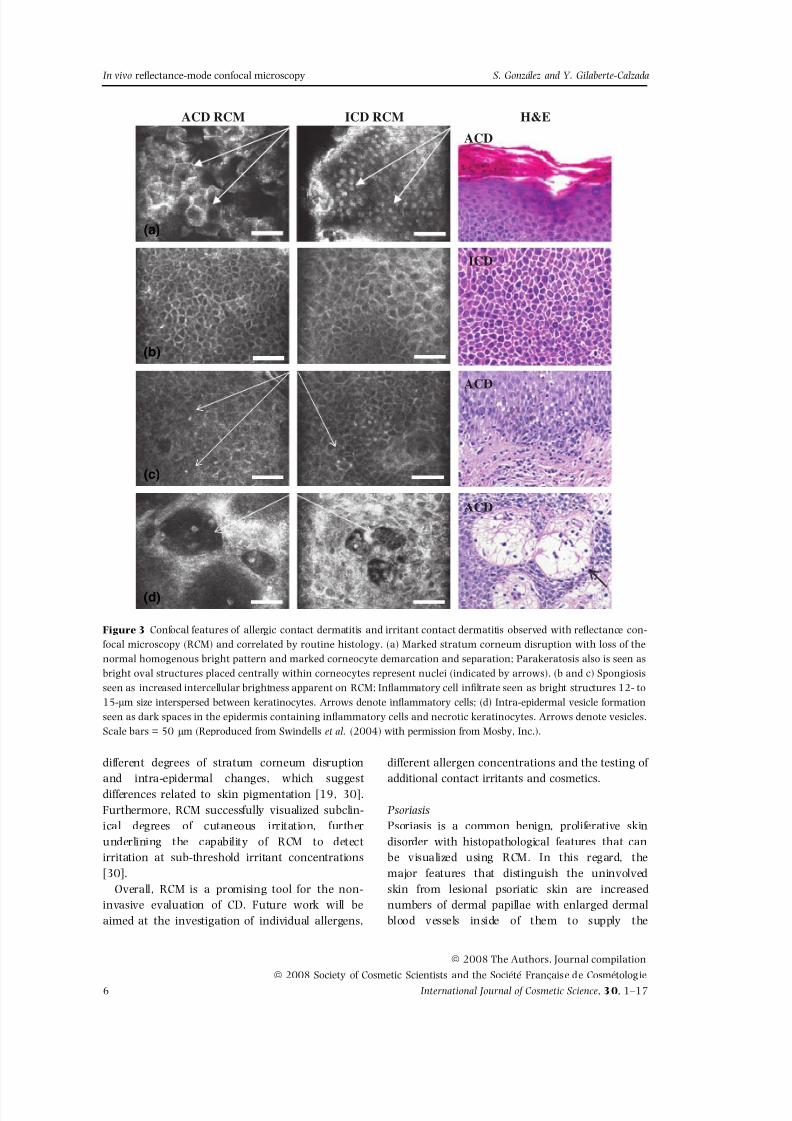
by RCM. The presence of epidermal inammatorycellular inltrate can be visualized as bright roundor oval structures 9- to 12- l m size interspersedbetween keratinocytes. Areas of necrotic epidermis,perivascular inammatory inltrate, and increasedsize and brightness of basal keratinocytes are alsoseen in both types of reaction. Whereas ACD pre-dominantly exhibits vesicle formation, inamma-tory inltrates and spongiosis [17, 20], ICD istypically associated to pronounced supercialchanges involving the stratum corneum, cleardemarcation and separation of individual corneo-cytes, and parakeratosis; it is possible to identifyparakeratotic nuclei and these appeared as bright(highly refractile) oval structures placed centrallywithin corneocytes (Fig. 3) [17, 20]. In these stud-ies, both ACD and ICD have demonstrated similardegrees of spongiosis. Preliminary data on the accu-racy of RCM in the diagnosis of ACD showed thatspongiosis and exocytosis in the spinous layer havehigh sensitivity and specicity with regard to patchtesting, indicating that RCM may add cellular level
information to the clinical interpretation of patchtests, thus potentially enhancing ACD diagnostic[29]. Furthermore, kinetic evolution of ACD and
ICD has been investigated by RCM, showing char-acteristic patterns. Firstly, the onset of disruptivechanges is generally much faster for ICD whencompared with ACD. The supercial changes in thestratum corneum are visible within few hours fol-lowing the application of the contact irritants,whereas stratum corneum alterations are generallyless prominent in acute ACD. Secondly, ACD exhib-its microvesicle formation, whereas ICD also fea-tures intra-epidermal necrosis [17, 20]. Finally,epidermal hyperproliferation associated with ICDreactions can be followed using RCM, and seems tobe a sensitive parameter for the activity of ICD reac-tions. Overall, ICD has a faster onset and resolutionthan the cutaneous changes in ACD.
Recently, investigations have also been aimedat the evaluation of ethnic variability in skinresponse to experimental contact irritants suchas sodium lauryl sulphate and common house-hold detergents such as ivory dishwashing liquid.Preliminary studies performed in Caucasian andAfrican-American volunteers have revealed
Table II Reectance confocal micro-scopy features of inammatorydermatosis
Skin lesion Features
Contact dermatitis SpongiosisAllergic Microvesicle formation
Inammatory inltrateIrri tant Pronounced supercial changes in s tratum corneum
Intra-epidermal necrosisProminent epidermal hyperproliferation and visible nucleoli
Psoriasis vulgaris Parakeratosis, acanthosis and papillomatosisThinning of the granular layerMunro’s microabscessesIncreased tortuosity of the dermal vasculature
Rosacea Increased diameters of the pilosebaceous ductsTortuous capillariesPerifollicular and perivascular inammatory inltrate
Pyogenic granuloma Increased number of dilated and tortuous blood vesselsPronounced spongiosisExocytosis
Cutaneous infections Onychomycosis Branched hyphae
Inammatory inltrateBacterial folliculitis Inltrating neutrophils in the subcorneal pustule
WartsCapillary dilatationMultiple highly refractile round structures (20–40 l m)
HerpesHyperkeratotic stratum corneumPleomorphic ballooned keratinocytesMultinucleated giant cells in a loose aggregate of keratinocytesInammatory cells and debris.
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 5
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada
8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 6/17
different degrees of stratum corneum disruptionand intra-epidermal changes, which suggestdifferences related to skin pigmentation [19, 30].Furthermore, RCM successfully visualized subclin-ical degrees of cutaneous irritation, furtherunderlining the capability of RCM to detectirritation at sub-threshold irritant concentrations[30].
Overall, RCM is a promising tool for the non-invasive evaluation of CD. Future work will beaimed at the investigation of individual allergens,
different allergen concentrations and the testing of additional contact irritants and cosmetics.
PsoriasisPsoriasis is a common benign, proliferative skindisorder with histopathological features that canbe visualized using RCM. In this regard, themajor features that distinguish the uninvolvedskin from lesional psoriatic skin are increasednumbers of dermal papillae with enlarged dermalblood vessels inside of them to supply the
(a)
ACD RCM ICD RCM H&E
ACD
ACD
ACD
ICD
(b)
(c)
(d)
Figure 3 Confocal features of allergic contact dermatitis and irritant contact dermatitis observed with reectance con-focal microscopy (RCM) and correlated by routine histology. (a) Marked stratum corneum disruption with loss of thenormal homogenous bright pattern and marked corneocyte demarcation and separation; Parakeratosis also is seen asbright oval structures placed centrally within corneocytes represent nuclei (indicated by arrows). (b and c) Spongiosisseen as increased intercellular brightness apparent on RCM; Inammatory cell inltrate seen as bright structures 12- to15- l m size interspersed between keratinocytes. Arrows denote inammatory cells; (d) Intra-epidermal vesicle formationseen as dark spaces in the epidermis containing inammatory cells and necrotic keratinocytes. Arrows denote vesicles.Scale bars = 50 l m (Reproduced from Swindells et al. (2004) with permission from Mosby, Inc.).
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–176
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 7/17
proliferative lesion with circulating erythrocytes[31]. Other features are: (i) retained nuclei withinthe corneocytes, seen as small dark areas (para-keratosis); (ii) clusters of polymorphonuclear leu-cocytes forming the Munro’s microabscesses,
visualized as highly refractile compared with thesurrounding keratinized background. It is easierto discriminate within the microabscess than inroutine histology; and (iii) thinning of the granu-lar layer (Fig. 4) [16].
dp
dp
(a)
(b)
B
(c)
C
A
Figure 4 Psoriatic lesion. Histologic section with bars indicating the depth levels in which confocal images A, B and Chave been obtained. (a) Confocal image of parakeratotic stratum corneum. Note arrows pointing out nuclei. (b) Confocalimage showing transverse section of Munro’s microabscess (arrow). (c) Confocal image at dermo-epidermal junctionshowing increased number density of dermal papillae (dp). Note tortuous blood vessels (arrows). Scale bar = 50 l m.
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 7
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 8/17
RosaceaAcne rosacea is a benign, inammatory skin disor-der of unknown aetiology with female preponder-ance. The disease typically presents on the face withdilated vasculature and acneiform inammatory
papules and pustules. RCM histopathology revealsincreased diameters of the pilosebaceous ducts, tor-tuous capillaries and a characteristic perifollicularand perivascular inammatory inltrate [21].
RCM ndings of cutaneous infections
Fungal infectionsDermatophyte infections including onychomycosisand tinea pedis, although common, can be difcultto diagnose. Diagnosis may be delayed when cul-ture is necessary because of the time required forthe hyphae to grow. RCM enables rapid real-timeidentication of branched hyphae, visualized as anetwork of long, dark, sometimes septated struc-tures. In vivo, they appear below the surface of thenail plate, but they can also be observed in vitro innail clippings or scrapings [22, 23]. RCM can beparticularly useful for tinea unguium, in whichthe high percentage of false negative results in themicrobiological tests makes the diagnosis difcult.
Bacterial folliculitisFolliculitis imaged with RCM can be diagnosed bydirect observation of a hair follicle surrounded by
a signicant number of small bright granular cells(neutrophils), which can be also found within thesubcorneal pustules. In addition, severe spongioticepidermis and capillary dilatation in the dermalpapillae can be observed [21].
Viral infectionsWarts have also been imaged with RCM. Thehyperkeratotic stratum corneum and the presenceof multiple highly refractile round structures mea-suring 20- to 40- l m size within the lesion allowsa rapid and conclusive diagnosis of common wart.These typical round structures may be keratohya-line granules or putative viral particles withininfected keratinocytes, based on their size (ourunpubl. data).
Cutaneous herpes infections may be atypical andsevere, especially in immunocompromised individu-als. RCM has been proved to be a useful tool intheir diagnoses. Their main features are the pres-ence of pleomorphic big round cells with dark cyto-plasm, identied as ballooned keratinocytes, and
internal round bright structures corresponding tomultinucleated giant cells. Both types tend to formloose aggregates interspersed with round brightcells identied as inammatory cells moving withina black, uid medium. These ndings are identical
to those provided by conventional histology [32].
RCM ndings of skin neoplasms
Reectance confocal microscopy characterizationof neoplastic lesions is a major area for research,with the potential to aid in the non-invasive diag-nosis and management of a variety of skin can-cers. With the advent of newer less invasive ortopical therapies, it is desirable to use non-invasivediagnostic tools that enable accurate identicationof tumour subtypes and tumour margins, andresponse to treatment.
RCM of melanocytic lesionsPigmented lesions include different cellular constit-uents: melanocytes, pigmented keratinocytes andmelanophages. Using RCM, pigmented keratino-cytes appear as polygonal cohesive cells with brightgranular cytoplasms of varying intensity. Melano-cytes appear as bright round, oval, fusiform or den-dritic cells. They can be identied by their nestedgrowth pattern as aggregates of bright round tooval structures at the dermo-epidermal junction orin the supercial dermis. Melanocytes are also rec-
ognizable as single cells along the dermo-epidermal junction, usually separated from each other by avariable number of keratinocytes. Finally, melano-phages appear as large bright plump cells with ill-dened cytoplasmic borders, usually locatedaround or near vessels of the supercial dermis.
Melanocytic nevi
In nevi, both spinous and granular layers showno alteration, with normal patterns in a homoge-nous population of well-demarcated cells (Table III).A nevus itself is made of nevomelanocytes, ahomogenous population of small monomorphusround to oval bright refractive cells with centrallypositioned dark round nuclei [14, 33]. Dermalpapillae are uniformly distributed and circum-scribed by a rim of refractive monomorphous cells(edge papillae) that correspond to small melanocytesand melanin-rich keratinocytes, without any cyto-logical atypia. In junctional nevi, melanocytes areat the dermo-epidermal junction level [33–35]. On
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–178
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 9/17
the contrary, in compound and dermal nevi, theyare seen within the papillary and reticular dermis,
near the vessels. Sporadically, small brilliant den-drites in the epidermis can be observed.
Assessment of atypical nevi by dermoscopyreveals strikingly common features with commonnevi and melanoma, and occasionally the diagno-sis may be extremely difcult [34]. In atypicalnevi, the cell population is more heterogenous insize, shape and refractivity (different intensity inbrilliance) (Fig. 5 and Table III) [33–35]. However,cells tend to be round or oval as in common nevi,rather than dendritic as in melanoma. In general,atypia correlates with attenuated brightness in
most melanocytes, with isolated large bright epi-thelioid cells with peripheral nuclei, and cell nestscan be less demarcated [34, 35]. They also showfocal loss of keratinocyte demarcation within theepidermis overlying the lesion and bright granuleswithin the epidermis, probably representing mela-nin dust. Atypical nevi, especially on the face,may show destructuration at the dermo-epidermal
junction, and have non-homogenous dermal papil-lae with the absence of demarcation by refractive
cells (non-edge papillae ).
Melanoma
Reectance confocal microscopy allows the iden-tication of features characteristic of nevi andmelanoma. Pigmented melanomas and amelanoticmelanomas exhibit remarkably similar featureswhen assessed by RCM [33, 36–38]. Confocal fea-tures suspicious for melanoma are shown inTable III. These include structural changes in thespinous and granular layers, keratinocyte disar-
rangement and loss of intercellular demarcation(disruption of the ‘honeycomb pattern’) [33].Enlarged atypical cells with pleomorphic morphol-ogy, variable refractivity and angular nuclei maybe found in several layers of the epidermis (page-toid dissemination), and in the dermis (Fig. 6).Cells may be oval, stellate or fusiform, includ-ing coarse branching dendritic processes and
(a) (b)
Figure 5 Displastic lentiginous nevus. (a) Histologic section. The bars in image A show the depth level in which confo-cal image B has been obtained. (b) shows heterogeneous brightness with irregular distribution of dermal papillae. Der-mal papillae are surrounding by non-refractile rim of cells. Scale bar = 50 l m.
Table III Reectance confocal microscopy features of melanocytic skin tumours
Skin lesion Features
Melanocytic nevi Preserved honeycomb appearance of keratinocytes in the epidermis
Populations of monomorphous round to oval bright refractile cells withcentrally positioned nuclei in the basal layer (pigmented keratinocytes and melanocytes)
Regular and uniform dermal papillaeClusters of bright round cells in the dermis of compound nevi (nests)
Cutaneous melanoma Disarray of keratinocytes (loss of epidermal honeycomb appearance)Coarse branching dendritic structures in the epidermisSmall and irregular dermal papillaeBright grainy particles in the epidermisDermal cell clusters (nests) of different aspect when presentEnlarged round or dendritic highly refractive cells ascending in the
epidermis (pagetoid spread)
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 9
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 10/17
eccentrically placed large nuclei [33, 37, 39].Indistinguishable cell borders may be evident,which contributes to the abnormal epidermal mor-phology. In the basal layer, cells may be groupedresembling a dysplastic nevus or isolated. In thedermis, cerebriform cell clusters appear, includingthin refractive cell aggregates (poligonal orenlarged) surrounded by ‘melanin dust’ [34]. Mel-anoma also shares some of the features of dysplasticnevi. In this regard, dermal papillae are smaller,
more irregular and their borders are poorly denedwhen compared with common nevi. The architec-tural pattern is very asymmetrical in size and refrac-tivity. ‘Melanin dust’ is composed of coarse granules(1–3 l m) compared with atypical nevi, and is scat-tered along the epidermis. Linear dendrites arethicker and brighter than in healthy skin.
A useful advantage of RCM is that it enablesidentication of abnormal intra-epidermal melano-cytic proliferation, granules and dendritic struc-tures in clinically amelanotic melanomas [39].These features may be evident because of the pres-ence of melanosomes in the cytoplasm, which actas endogenous source of contrast because of theirsize (0.6–1.2 l m) and refractive index (1.70), and/or the presence of some melanin in pre-melano-somes [11, 36]. Apart from diagnosis, RCM hasshown good correlation to epiluminescence micros-copy during histological examination [40], andalso as a selective non-invasive tool to guide biopsycollection [37], pre-surgical mapping [38, 41] andmonitoring the response to treatment [38].
A limitation for the use of RCM in melanomadiagnosis is an imaging depth. Lesion depth hasbeen shown to be a very important prognosticfactor in patients diagnosed with melanoma.Available instruments can image to a depth of 200–350 l m, but the presence of refractive struc-tures in the dermis, such as inammatory cellsand collagen bundles, may decrease contrast anddifcult melanocyte visualization [38]. Thus,although RCM has been shown useful for the
differential diagnosis of intra-epidermal processes,little or no information about dermal cells andstructures can be obtained, limiting its use for theassessment of deeper lesions.
RCM of non-melanocitic skin tumours
Actinic keratosis
The main features of actinic keratosis assessed byin vivo RCM include irregular hyperkeratosis in thestratum corneum. In addition, the stratum granu-losum is almost identical to that of normal skin,with dark nuclei, contrasted against the brightrefractile cytoplasm of the keratinocytes. Whereasnuclei in the stratum spinosum and stratumbasale vary in shape, size and haphazard orienta-tion, these ndings correspond to nuclear enlarge-ment with pleomorphism in a pattern consistentwith architectural disarray, which does notinvolve the full thickness of the epidermis usuallyseen in conventional histology (Fig. 7) (Table IV)
B
C
(b) (c)
*
*
(a)
*
Figure 6 Supercial spreading melanoma. (a) Histology section with bars indicating the depth level in which confocalimages B and C have been obtained. (b) Confocal image shows the presence of atypical melanocytes and dendrites(arrows) ascending in the epidermis (pagetoid spread), within a background of marked loss of keratinocyte demarcation(*). (c) Confocal image shows the presence of non-refractile rims around dermal papillae openings (non-edge papillae, *).Also, enlarge (atypical) melanocytes are observed (arrows). Scale bar: 50 l m .
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–1710
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 11/17
[42]. Observation of dysplastic features in the fullskin thickness on RCM is suggestive of squamouscell carcinoma.
Squamous cell carcinoma
The shallow penetration of the RCM illuminatingwavelengths prevents accurate visualization atthe dermo-epidermal junction, particularly inhyperkeratotic lesions. This makes differential diag-nosis between supercially invasive SCC and SCCin situ unfeasible because of lack of adequatevisual assessment at the dermo-epidermal junction.Confocal features suggestive of SCC are full thick-ness architectural disarray and nuclear enlarge-ment with pleomorphism observed from the basallayer to the stratum granulosum (Table IV). Otherfeatures suggestive of SCC, such as vascularpatterns and keratin pearls, need further investiga-tion.
Basal cell carcinoma
Reectance confocal microscopy morphologicalcharacteristics of basal cell carcinoma (BCC) havebeen well dened (Table IV) [43, 44], and include:(i) the presence of pleomorphism and architectural
disorder of the overlying epidermis, indicative of actinic damage or the presence of the tumour; (ii)the presence of islands of refractive tumour cellswith elongated monomorphic basaloid nuclei, asso-ciated with intervening areas of low refractility,
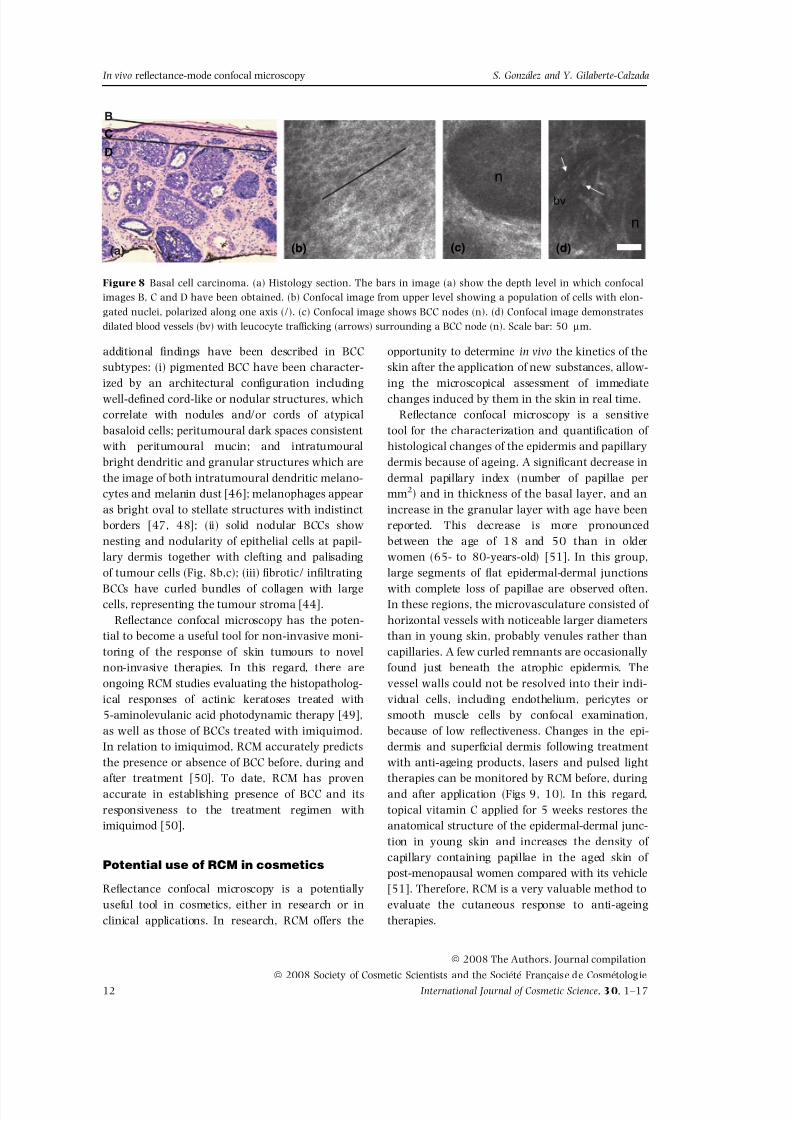
which might correspond to the mucinous stroma(Fig. 8); (iii) nuclei of tumour cells that are polar-ized along the same axis of orientation, disruptingthe normal honeycomb pattern of the epidermisand the dermal papillae architecture; (iv) increaseddermal vasculature with prominent dilatation andtortuosity of blood vessels; and (v) trafcking of leucocytes is easily identied as bright, highlyrefractile round cells along the endothelial lining(Fig. 8C). A retrospective, multicentric study of 152 patients has shown that the presence of atleast two of these criteria has a sensitivity of 100% for the diagnosis of BCC [45]. As the num-ber of criteria present for a lesion was greater, thespecicity increased, so when at least four criteriawere present, the specicity was 95.7%, giving thebest concordance between high sensitivity andhigh specicity. The most sensitive and specic cri-terion was the presence of polarized nuclei (91.6%and 97%, respectively), which is consistent withhistological ndings as palisading is one of themost remarkable characteristics of BCC. Specic
(a) (b)
Figure 7 Actinic keratosis. (a) His-tology section showing the depth
level of confocal image. (b) Confocalimage shows en face confocal imagewith keratinocyte disarray-epidermalpleomorphism. Scale bar: 50 l m.
Table IV Reectance confocal microscopy features of non-melanocytic skin tumours
Skin lesion Features
Actinic keratosis Irregular hyperkeratosisEpidermal nuclear enlargement and pleomorphismArchitectural disarray limited to lower portion of epidermis
Squamous cell carcinoma Nuclear enlargement with pleomorphism
Full thickness architectural disarray of epidermisBasal cell carcinoma Islands of tumour cells with monomorphic elongated basaloid nuclei
Polarization of tumour cell nuclei along the same spatial axis throughout epidermisProminent inammatory inltrate admixed or closely apposed with tumour cellsIncreased dermal vasculature with tortuous dilated blood vessels and
leucocyte accumulation and rolling along endothelial liningPlemorphism and architectural disorder of overlying epidermis.
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 11
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada
8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 12/17
additional ndings have been described in BCCsubtypes: (i) pigmented BCC have been character-ized by an architectural conguration includingwell-dened cord-like or nodular structures, whichcorrelate with nodules and/or cords of atypicalbasaloid cells; peritumoural dark spaces consistentwith peritumoural mucin; and intratumouralbright dendritic and granular structures which arethe image of both intratumoural dendritic melano-cytes and melanin dust [46]; melanophages appearas bright oval to stellate structures with indistinctborders [47, 48]; (ii) solid nodular BCCs shownesting and nodularity of epithelial cells at papil-lary dermis together with clefting and palisadingof tumour cells (Fig. 8b,c); (iii) brotic/ inltrating
BCCs have curled bundles of collagen with largecells, representing the tumour stroma [44].
Reectance confocal microscopy has the poten-tial to become a useful tool for non-invasive moni-toring of the response of skin tumours to novelnon-invasive therapies. In this regard, there areongoing RCM studies evaluating the histopatholog-ical responses of actinic keratoses treated with5-aminolevulanic acid photodynamic therapy [49],as well as those of BCCs treated with imiquimod.In relation to imiquimod, RCM accurately predictsthe presence or absence of BCC before, during andafter treatment [50]. To date, RCM has provenaccurate in establishing presence of BCC and itsresponsiveness to the treatment regimen withimiquimod [50].
Potential use of RCM in cosmetics
Reectance confocal microscopy is a potentiallyuseful tool in cosmetics, either in research or inclinical applications. In research, RCM offers the
opportunity to determine in vivo the kinetics of theskin after the application of new substances, allow-ing the microscopical assessment of immediatechanges induced by them in the skin in real time.
Reectance confocal microscopy is a sensitivetool for the characterization and quantication of histological changes of the epidermis and papillarydermis because of ageing. A signicant decrease indermal papillary index (number of papillae permm 2 ) and in thickness of the basal layer, and anincrease in the granular layer with age have beenreported. This decrease is more pronouncedbetween the age of 18 and 50 than in olderwomen (65- to 80-years-old) [51]. In this group,large segments of at epidermal-dermal junctions
with complete loss of papillae are observed often.In these regions, the microvasculature consisted of horizontal vessels with noticeable larger diametersthan in young skin, probably venules rather thancapillaries. A few curled remnants are occasionallyfound just beneath the atrophic epidermis. Thevessel walls could not be resolved into their indi-vidual cells, including endothelium, pericytes orsmooth muscle cells by confocal examination,because of low reectiveness. Changes in the epi-dermis and supercial dermis following treatmentwith anti-ageing products, lasers and pulsed lighttherapies can be monitored by RCM before, duringand after application (Figs 9, 10). In this regard,topical vitamin C applied for 5 weeks restores theanatomical structure of the epidermal-dermal junc-tion in young skin and increases the density of capillary containing papillae in the aged skin of post-menopausal women compared with its vehicle[51]. Therefore, RCM is a very valuable method toevaluate the cutaneous response to anti-ageingtherapies.
bv
n
n
(c)(b)
BC
D
(d)(a)
Figure 8 Basal cell carcinoma. (a) Histology section. The bars in image (a) show the depth level in which confocalimages B, C and D have been obtained. (b) Confocal image from upper level showing a population of cells with elon-gated nuclei, polarized along one axis (/). (c) Confocal image shows BCC nodes (n). (d) Confocal image demonstratesdilated blood vessels (bv) with leucocyte trafcking (arrows) surrounding a BCC node (n). Scale bar: 50 l m.
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–1712
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 13/17
Comedogenecity has long been a concern in thedevelopment of cosmetic and personal care prod-ucts. The hairless rhino mouse has extensivelybeen used for comedone studies because its skin
contains many horn-lled utriculi also known aspseudocomedones. These pseudocomedones appearin RCM as circular or oval structures lled with ahighly refractive substance – keratin and collagen – and enclosed by loosely arranged dermis [52].The skin effect of retinoic acid has been observedby RCM in these animals. Removal of follicularplugs from pseudocomedones and transformationinto normal follicular structures in a dose-relatedmanner were observed. Sebaceous duct develop-ment was registered by RCM, changes perfectlycorrelated with conventional histology. Addition-ally, small comedones, presenting as follicularplugs within the epidermis and small pustules atand below the dermo-epidermal junction, havebeen detected in RCM images of patients with acne(Fig. 11). Therefore, RCM is a useful tool forin vivo morphological and quantitative evaluationof skin comedones over time and can be usedeither for studying the comedogenecity of acosmetic product or for monitoring the treatmentof comedones.
Reectance confocal microscopy greatlyenhances assessment of dynamic pigmentarychanges in human or animal skin over time andin response to specic stimuli such as ultraviolet
radiation exposure [53, 54]. A study in pigmentedguinea pigs has shown that after 4 days of irradia-tion, when only faint erythema and no clinicaltanning was yet visible, RCM could already detectpigmentary changes, as follows: (i) melanocytes,visible as bright dendritic cells, have bigger cellbodies; (ii) the stratum spinosum, composed of small polygonal cells with dark nuclei and abrighter ring of cytoplasm is less bright because of epidermal hyperplasia; (iii) a dened cellular layeremerged showing keratinocytes in different degreesof melanization and cells with the size of spinouscells belong to the stratum spinosum; and (iv)many dendrites viewed in cross-section appearedas small bright dots showing increased dendricityof melanocytes. RCM images after 3 weeks afterstarting irradiation, when skin has clinically visi-ble tanning, show: (i) melanocytes are increased insize and number and pigmented keratinocytes of the stratum spinosum can be seen next to them;the stratum spinosum consists out of pigment-loaded keratinocytes, but in some cells the nucleus
(a) (b)
Figure 9 Normal dermis. Confocalimages taken at upper reticular der-
mis level of a subject volunteer of 41 years old (a) compared withanother of 84 years old (b). Scalebar: 50 l m (courtesy: C. Alessi,Lucid Inc., NY, USA).
ProminentDermatoglyphs
DermatoglyphsThinner
(a) (b)
Figure 10 Sun-exposed skin. Super-cial confocal images (approximately30- l m depth) of photodamaged skinat baseline (a) and at 1 month of tre-atment (b). Note thinner dermato-glyphs after treatment. Scale bar:50 l m (courtesy: C. Alessi, LucidInc., NY, USA).
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 13
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 14/17
can still be seen as a dark round center [54]. RCMhas also been used to evaluate in vivo dose andtime-dependent skin changes in humans followingsolar-simulated irradiation and to correlate themwith other non-invasive techniques such as optical
coherence tomography [55]. The authors demon-strated denite optical coherence tomography andRCM ndings obtained from UV exposed skinincluding increase epidermis thickness (hyperprolif-eration and acanthosis), reduction in dermalreectivity (dermal oedema), increase in brightnessof the basal layer (pigmentation), and increase invessel diameter within the dermal papillae (vasodi-latation). In conclusion, RCM seems to be a veryuseful tool in photobiology research including sun-screen tests [53, 54]. Additionally, this tool alsohas been used to analyze depigmenting agents[56]. In the context of skin photoageing, solarlentigines occurring in sun-damaged skin of olderadults also have been analyzed by RCM [57](Fig. 12). RCM can be an accurate in vivo method
for assessing their response to cosmetic approachesnot only for evaluating pigmentation degree, butalso for monitoring their morphological changes athigh resolution.
Finally, RCM can be used to tattoo-related skin
alterations [58]. Massive subepidermal deposits of dense, clustered pigment granules up to about3-mm size correspond to black tattoos, with themore scarce and diffuse deposits corresponding tored, blue and green tattoos. Diffuse pigment gran-ules tended to accumulate in the outer dermisunderneath the level of the basement membranezone. Therefore, RCM could be a useful techniquefor pre-evaluation of tattoos before laser removal,helping to predict their clinical outcome.
Limitations of RCM
The main limitation of RCM is its penetration indermis, which nowadays reaches a maximumdepth of 350–400 l m. This prevents imaging of
(a) (b)
Figure 11 Comedo cyst. Confocalimages (a and b) at different depthlevels of a comedo cyst. Scale bar:50 l m (courtesy: C. Alessi, LucidInc., NY, USA).
(a) (b)
Figure 12 Solar Lentigo. Reectance confocal images were collected from a solar lentigo located on the hand of a 60-year-old volunteer. They were taken at 43 l m (spinous compartment, (a)) and 97 l m (dermo-epidermal level, (b)) belowthe stratum corneum. At dermo-epidermal papillae, the presence of polymorphous dermal papillae with polycyclic con-tours is noted. Eccrine duct (encircled) appears as a spiraling structure showing less refractivity and a donut shape atdermal epidermal level. Scale bar: 50 l m (courtesy: L. Declercq and C. Polleiet, Este ´e Lauder Companies, Oevel,Belgium).
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–1714
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 15/17
structures located in the deep dermis, especially incases of hyperpigmented or hyperkeratotic lesions,as, in these cases, there is strong contrast attenua-tion because of absorption and scattering of lightgoing through those structures. The presence of
refractive structures in the dermis, such as inam-matory cells and collagen bundles, may alsodecrease contrast and difcult melanocyte visual-ization.This might be improved by assayingdifferent immersion media and illuminationsources.
The current contact device can be unwieldy anddifcult to use on a non-at surface. A portableprototype RCM has recently been developed thatwill further miniaturize the microscope to producea more manageable or hand-held device possiblyusing bre optics. This would make it much moreuser-friendly and practical. Finally, work is ongo-ing to facilitate the creation of vertical and3-dimensional sections, which would vastlyincrease the potential of RCM.
Summary and conclusions
Reectance confocal microscopy has the potentialto reduce the need for invasive biopsies by facilitat-ing in vivo diagnosis of both benign and malignantlypigmented and non-pigmented lesions. Unfortu-nately, a major limitation to this technology is theimaging depth, especially in hyperkeratotic lesions,
largely because of attenuation of the intensity,which is secondary to light absorption and scatter-ing. Further improvements regarding increasing theRCM power and depth of optical penetration, andusing optimal immersion media with good diffusionproperties may help address this issue.
Reectance confocal microscopy presentsresearchers with the opportunity to perform non-invasive evaluation of skin lesions with histologicaldetail. It may be employed as a guide for perform-ing biopsies, by helping to determine areas exhibit-ing suspicious features of malignancy andreducing sampling error [37]. Furthermore, it maybe used as an adjunct to Mohs surgery and ther-apy [59–61] by mapping out the margins orextent of involvement prior to excision or othertherapies. RCM can be repeated indenitely, andtherefore can be used to monitor progression orresolution of lesions through time. In this regard,RCM may be valuable to examine the histopatho-logical response of tumours to therapy. Progressivenormalization of architecture in lesions of AK trea-
ted with photodynamic therapy has been observedunder RCM monitoring, and it has also beenemployed to conrm complete clearance of AKand BCC and resulting inammatory response totopical imiquimod. Finally, RCM is also a powerful
tool in cosmetics not only in research, but also tomonitor histological changes after cosmetic treat-ments in a non-invasive way.
Acknowledgements
This work has been partially supported by a grantfrom the Spanish Ministry of Health (FISS,PI060499).
References
1. Markisz, J.A. and Aquilia, M.G. Technical Magnetic res-onance Imaging . Appleton & Lange, Standford (1996).
2. Mansotti, L. Basic principles and advanced technicalaspects of ultrasound imaging. In: Physics and Engi-neering of Medical Imaging (Guzzardi, R., ed.), pp.263–317. Springer, the Netherlands (1987).
3. Tearney, G.T., Brezinski, M.E., Southern, J.F., Bouma,B.E., Hee, M.R. and Fujimoto, J.G. Determination of the refractive index of highly scattering human tis-sue by optical coherence tomography. Opt. Lett . 20 ,2258–2260 (1995).
4. New, K.C., Petroll, W.M., Boyde, A. et al. In vivoimaging of human teeth and skin using real-timeconfocal microscopy. Scanning 13 , 369–372 (1991).
5. Rajadhyaksha, M., Grossman, M., Esterowitz, D.,Webb, R.H. and Anderson, R.R. In vivo confocalscanning laser microscopy of human skin: melaninprovides strong contrast. J. Invest. Dermatol. 104 ,946–952 (1995).
6. Rajadhyaksha, M., Gonza ´lez, S., Zavislan, J., Ander-son, R.R. and Webb, R.H. In vivo confocal scanninglaser microscopy of human skin II: advances ininstrumentation and comparison to histology. J. Invest. Dermatol. 113 , 293–303 (1999).
7. Wilson, T. Confocal Microscopy . Academic Press, SanDiego (1990).
8. Pawley, J.B. Handbook of Biological Confocal Micros-copy. 2nd ed. Plenum Press, New York (1995).
9. Webb, R.H. Confocal optical microscopy. Rep. Prog.Phys. 59 , 427–471 (1996).
10. Webb, R.H. Theoretical Basis of confocal microscopy.Methods Enzymol. 307 , 3–20 (1999).
11. Rajadhyaksha, M., Gonzalez, S. and Zavislan, J.M.Detectability of contrast agents for confocal reec-tance imaging of skin and microcirculation. J. Bio-med. Opt. 9 , 323–331 (2004).
12. Carlsson, K. The inuence of specimen refractiveindex, detector signal integration, and non-uniform
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de CosmetologieInternational Journal of Cosmetic Science , 30 , 1–17 15
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada
8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 16/17
scan speed on the imaging properties in confocalmicroscopy. J. Microsc. 163 , 167–178 (1991).
13. Wan, D.S., Rajadhyaksha, M. and Webb, R.H. Analy-sis of spherical aberration of a water immersionobjective: application to specimens with refractiveindices 1.33-1.40. J. Microsc. 197 , 274–284 (2000).
14. Busan, K.J., Charles, C., Lee, G. and Halpern, A.C.Morphologic features of melanocytes, pigmentedkeratinocytes, and melanophages by in vivo confocalscanning laser microscopy. Mod. Pathol. 14 , 862– 868 (2001).
15. Rajadhyaksha, M., Anderson, R.R. and Webb, R.H.Video-rate confocal scanning laser microscope for imag-ing human tissues in vivo. Appl. Opt. 38 , 1–12 (1999).
16. Gonzalez, S., Rajakhyaksha, M., Rubinstein, G. andAnderson, R.R. Characterization of psoriasis in vivoby reectance confocal microscopy. J. Med. 30 , 337– 356 (1999).
17. Astner, S., Gonzalez, E., Cheung, A.C., Rius-Diaz, F.,
Doukas, A.G., William, F. and Gonzalez, S. Non-inva-sive evaluation of the kinetics of allergic and irritantcontact dermatitis. J. Invest. Dermatol. 124 , 351–359(2005).
18. Gonzalez, S., Gonzalez, E., White, W.M., Rajadhyak-sha, M. and Anderson, R.R. Allergic contact dermati-tis: correlation of in vivo confocal imaging to routinehistology. J. Am. Acad. Dermatol. 40 , 708–713 (1999).
19. Hicks, S.P., Swindells, K.J., Middelkamp-Hup, M.A.,Sifakis, M.A., Gonzalez, E. and Gonzalez, S. Confocalhistopathology of irritant contact dermatitis in vivoand the impact of skin color (black vs white). J. Am.Acad. Dermatol. 48 , 727–734 (2003).
20. Swindells, K., Burnett, N, Rius-Diaz, F, Gonzalez, E.,Mihm, M.C. and Gonzalez, S. Reectance confocalmicroscopy may differentiate acute allergic and irri-tant contact dermatitis in vivo. J. Am. Acad. Dermatol.50 , 220–228 (2004).
21. Gonza lez, S., Rajadhyaksha, M., Gonza ´lez-Serva, A.,White, W.M. and Anderson, R.R. Confocal reec-tance imaging of folliculitis in vivo. Correlation of confocal imaging to routine histology. J. Cut. Pathol.26 , 201–205 (1999).
22. Hongcharu, W., Dwyer, P., Gonza ´lez, S. and Anderson,R.R.Conrmation of onychomychosis by confocal micro-scopy. J. Am. Acad. Dermatol. 42 , 214–216 (2000).
23. Markus, R., Huzaira, M., Anderson, R.R. and Gon-
zalez, S. A better KOH prep? In vivo diagnosis of tineawith confocal microscopy. Arch. Dermatol. 137 ,1076–1078 (2001).
24. Mathias, C.G. The cost of occupational skin disease.Arch. Dermatol. 121 , 332–334 (1985).
25. Brasch, J., Burgard, J. and Sterry, W. Common path-ogenetic pathways in allergic and irritant contactdermatitis. J. Invest. Dermatol. 98 , 166–170 (1992).
26. Willis, C.M., Young, E, Brandon, D.R. and Wilkinson, J.D. Immunopathological and ultrastructural ndings
in human allergic and irritant contact dermatitis. Br. J. Dermatol. 115 , 305–316 (1986).
27. Scheynius, A., Fischer, T., Forsum, U. and Klareskog,L. Phenotypic characterization in situ of inamma-tory cells in allergic and irritant contact dermatitis inman. Clin. Exp. Immunol. 55 , 81–90 (1984).
28. Flier, J., Boorsma, D.M., Bruynzeel, D.P. et al. TheCXCR3 activating chemokines IP-10, Mig, and IP-9are expressed in allergic but not in irritant patch testreactions. J. Invest. Dermatol. 113 , 574–578 (1999).
29. Astner, S., Gonzalez, E., Cheung, A., Rius-Diaz, F.and Gonzalez, S. Pilot study on the sensitivity andspecicity of in vivo reectance confocal microscopyin the diagnosis of allergic contact dermatitis. J. Am.Acad. Dermatol. . 53 , 986–992 (2005) .
30. Astner, S., Burnett, N., Rius-Diaz, F., Doukas, A.G.,Gonzalez, S. and Gonzalez, E. Irritant contact dermati-tis induced by a common household irritant: a non-invasive evaluation of ethnic variability in skin
response. J. Am. Acad. Dermatol. 54 , 458–465 (2006).31. Gonzalez, S., Rajadhyaksha, M. and Anderson, R.R.
Non-invasive (real-time) imaging of histologic mar-gin of a proliferative skin lesion in vivo. J. Invest. Der-matol. 111 , 538–539 (1998).
32. Goldgeier, M., Fox, C.A. and Muhlbauer, J.E. Immedi-ate non-invasive diagnosis of herpes virus by confo-cal scanning laser microscopy. J. Am. Acad. Dermatol.46 , 783–785 (2002).
33. Langley, R.G.B., Rajadhyaksha, M., Dwyer, P.J.,Sober, A.J., Flotte, T.J. and Anderson, R.R. Confocalscanning laser microscopy of benign and malignantmelanocytic skin lesions in vivo. J. Am. Acad. Derma-tol. 45 , 365–376 (2001).
34. Pellacani, G., Cesinaro, A.M. and Seidenari, S. In vivoassessment of melanocytic nests in nevi and melano-mas by reectance confocal microscopy. Mod. Pathol.18 , 469–474 (2005).
35. Pellacani, G., Cesinaro, A.M., Longo, C., Grana, C.and Seidenari, S. Microscopic in vivo description of cellular architecture of dermascopic pigment networkin nevi and melanomas. Arch. Dermatol. 141 , 147– 154 (2005).
36. Busam, K.J., Hester, K., Charles, C., Sachs, D.L., An-tonescu, C.R., Gonzalez, S and Halpern, A.C. Detec-tion of clinically amelanotic malignant melanomaand assessment of its margins by in vivo confocal
scanning laser microscopy. Arch. Dermatol. 137 ,923–929 (2001).37. Tannous, Z.S., Mihm, M.C., Flotte, T.J. and Gonzalez,
S. In vivo examination of lentigo maligna and malig-nant melanoma in situ, lentigo maligna type bynear-infrared reectance confocal microscopy: com-parison of in vivo confocal images with histologic sec-tions. J. Am. Acad. Dermatol. 46 , 260–263 (2002).
38. Curiel-Lewandrowski, C., Williams, C.M., Swindells,K.J., Tahan, S.R., Astner, S, Frankenthaler, R.A. and
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
International Journal of Cosmetic Science , 30 , 1–1716
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada

8/12/2019 In Vivo Reflectance-mode Confocal Microscopy in Clinical Dermatology and Cosmetology
http://slidepdf.com/reader/full/in-vivo-reflectance-mode-confocal-microscopy-in-clinical-dermatology-and-cosmetology 17/17
Gonzalez, S. Use of in vivo confocal microscopy inmalignant melanoma: an aid in diagnosis and assess-ment of surgical and nonsurgical therapeutic approa-ches. Arch. Dermatol. 140 , 1127–1132 (2004).
39. Busam, K.J., Charles, C., Lohmann, C.M., Marghoob,A., Goldgeier, M. and Halpern, A.C. Detection of in-traepidermal malignant melanoma in vivo by confo-cal scanning laser microscopy. Melanoma Res. 12 ,349–355 (2002).
40. Scope, A., Benvenuto-Andrade, C., Agero, A.C., Halp-ern, A.C., Gonzalez, S. and Marghhob, A.A. Precisedermoscopy to reectance confocal microscopy corre-lation of melanocytic neoplasms. Arch. Dermatol.143 , 727–734 (2007).
41. Chen, C., Elias, M., Busam, K., Rajadhyaksha, M.and Marghoob, A.A. Multi-modal in vivo opticalimaging, including confocal microscopy, facilitatepre-surgical margin mapping for clinically complexlentigo maligna melanoma. Br. J. Dermatol. 153 ,
1031–1036 (2005).42. Agasshi, D., Anderson, R.R. and Gonza ´lez, S. Confo-
cal, laser microscopic imaging of actinic keratoses invivo: a preliminary report. J. Am. Acad. Dermatol. 43 ,42–48 (2000).
43. Gonza´lez, S. and Tannous, Z. Real-time in vivo confo-cal reectance microscopy of basal cell carcinoma. J.Am. Acad. Dermatol. 47 , 869–874 (2002).
44. Sauermann, K., Gambichler, T., Wilmert, M., Rotter-dam, S., Stucker, M., Altmeyer, P. and Hoffmann, K.Investigation of basal cell carcinoma [correction of carcionoma] by confocal laser scanning microscopyin vivo. Skin Res. Technol. 8 , 141–147 (2002).
45. Nori, S., Rius-Diaz, F., Cuevas, J., Goldgeier, M., Jaen,P., Torres, A. and Gonzalez, S. Sensitivity and specic-ity of reectance-mode confocal microscopy for in vivodiagnosis of basal cell carcinoma: a multicenter study. J. Am. Acad. Dermatol. 51 , 923–930 (2004).
46. Agero, A.L.C., Busam, K.J., Benvenuto-Andrade, C.,et al. Reectance confocal microscopy of pigmentedbasal cell cancers in vivo. J. Am. Acad. Dermatol. 54 ,638–643 (2006).
47. Ruocco, E., Argenziano, G., Pellacani, G. and Seide-nari, S. Noninvasive imaging of skin tumors. Derma-tol. Surg. 30 , 301–310 (2004).
48. Charles, C.A., Marghoob, A.A., Busam, K.J., Clark-Loeser, L. and Halpern, A.C. Melanoma or pigmented
basal cell carcinoma: a clinical-pathologic correlationwith dermoscopy, in vivo confocal scanning lasermicroscopy, and routine histology. Skin Res. Technol.8 , 282–287 (2002).
49. Goldgeier, M., Fox, C.A., Zavislan, J.M., Harris, D. andGonzalez, S. Noninvasive imaging, treatment, andmicroscopic conrmation of clearance of basal cell car-cinoma. Dermatol. Surg. 29 , 205–210 (2003).
50. Torres, A., Niemeyer, A., Berkes, B. et al. 5% imiqui-mod cream and reectance-mode confocal micros-
copy as adjunct modalities to Mohs micrographicsurgery for treatment of Basal cell carcinoma. Derma-tol. Surg. 30 , 1462–1469 (2004).
51. Sauermann, K., Jaspers, S., Koop, Y. and Wenck, H.Topically applied vitamin C increases the density of dermal papillae in aged human skin. BMC Dermatol .29 , 13 (2004).
52. Nakano, K., Kiyokane, K., Benveneuto-Andrade, C.and Gonza lez, S. Real-time refrelctance confocalmicroscopy, a noninvasive tool for in vivo quantita-tive evaluation of comedolysis in the rhino mousemodel. Skin Pharmacol. Physiol. 20 , 29–36 (2007).
53. Yamashita, T., Kuwahara, T., Gonzalez, S. and Ta-kahashi, M. Non-invasive visualization of melaninand melanocytes by reectance-mode confocalmicroscopy. J. Invest. Dermatol. 124 , 235–240(2005).
54. Middelkamp-Hup, M.A., Park, H.Y., Lee, J., Gilchrest,B.A. and Gonzalez, S. Detection of UV-induced pig-
mentary and epidermal changes over time using invivo reectance confocal microscopy. J. Invest. Derma-tol. , 126 , 402–407 (2006).
55. Gambichler, T., Huyn, J., Tomi, N.S. et al. A compar-ative pilot study on ultraviolet-induced skin changesassessed by noninvasive imaging techniques in vivo.Photochem. Photobiol. 82 , 1103–1107 (2006).
56. Park, H.Y., Lee, J., Gonzalez, S., Middelkamp-Hup,M.A., Kapasi, S., Peterson, S. and Gilchrest, B.A.Topical application of a protein kinase C inhibitorreduces skin and hair pigmentation. J. Invest. Derma-tol. 122 , 159–166 (2004).
57. Pollifiet, C., Hellmans, H., Corstjens, H., Vanderover,G., Cummins, P., Declercq, L. and Maes, D. Increasedproliferation associated in vivo skin uorescenceanddeformation of the rete ridges pattern are commonfeatures of solar lentigines J. Invest. Dermatol. 127 ,s154 (2007).
58. O’goshi, K., Suihko, C. and Serup, J. In vivo imagingof intradermal tattoos by confocal scanning lasermicroscopy. Skin Res. Technol. 12 , 94–98 (2006).
59. Rajadhyaksha, M., Menaker, G., Flotte, T., Dwyer,P.J. and Gonzalez, S. Confocal examination of non-melanoma cancers in thick skin excisions to poten-tially guide Mohs micrographic surgery withoutfrozen histopathology. J. Invest. Dermatol. 117 ,1137–1143 (2001).
60. Chung, V.Q., Dwyer, P.J., Nehal, K.S., Rajadhyaksha,M., Menaker, G.M., Charles, C. and Jiang, S.B. Use of ex vivo confocal scanning laser microscopy duringMohs surgery for nonmelanoma skin cancers. Derma-tol. Surg. 30 , 1470–1478 (2004).
61. Tannous, Z., Torres, W. and Gonzalez, S. In vivo real-time confocal reectance microscopy: a noninvasiveguide for Mohs micrographic surgery facilitated byaluminum chloride, an excellent contrast enhancer.Dermatol. Surg. 29 , 839–846 (2003).
ª 2008 The Authors. Journal compilationª 2008 Society of Cosmetic Scientists and the Societe Francaise de Cosmetologie
In vivo reectance-mode confocal microscopy S. Gonzalez and Y. Gilaberte-Calzada